
Discordance between Body-Mass Index and Body Adiposity Index in the Classification of Weight Status of Elderly Patients with Stable Coronary Artery Disease

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Anthropometric Measurements
2.2. Bioimpedance Analysis (BImpA)
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
6. Study Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lavie, C.J.; De Schutter, A.; Parto, P.; Jahangir, E.; Kokkinos, P.; Ortega, F.B.; Arena, R.; Milani, R.V. Obesity and Prevalence of Cardiovascular Diseases and Prognosis-The Obesity Paradox Updated. Prog. Cardiovasc. Dis. 2016, 58, 537–547. [Google Scholar] [CrossRef]
- Hubert, H.B.; Feinleib, M.; McNamara, P.M.; Castelli, W.P. Obesity as an independent risk factor for cardiovascular disease: A 26-year fol-low-up of participants in the Framingham Heart Study. Circulation 1983, 67, 968–977. [Google Scholar] [CrossRef]
- Whitlock, G.; Lewington, S.; Sherliker, P.; Clarke, R.; Emberson, J.; Halsey, J.; Qizilbash, N.; Collins, R.; Peto, R. Body-mass index and cause-specific mortality in 900 000 adults: Collaborative analyses of 57 prospective studies. Lancet 2009, 373, 1083–1096. [Google Scholar] [CrossRef]
- Libby, P.; Buring, J.E.; Badimon, L.; Hansson, G.K.; Deanfield, J.; Bittencourt, M.S.; Tokgozoglu, L.; Lewis, E.F. Atherosclerosis. Nat. Rev. Dis. Primers 2019, 5, 56. [Google Scholar] [CrossRef] [PubMed]
- Peeters, A.; Barendregt, J.J.; Willekens, F.; Mackenbach, J.P.; Al Mamun, A.; Bonneux, L. Obesity in adulthood and its consequences for life expectancy: A life-table analysis. Ann. Intern. Med. 2003, 138, 24–32. [Google Scholar] [CrossRef]
- Akin, I.; Nienaber, C.A. “Obesity paradox” in coronary artery disease. World J. Cardiol. 2015, 7, 603–608. [Google Scholar] [CrossRef] [PubMed]
- Eyuboglu, M. Controversial points in the obesity paradox in patients with coronary artery disease. Atherosclerosis 2018, 275, 453–454. [Google Scholar] [CrossRef] [PubMed]
- Cornier, M.A.; Despres, J.P.; Davis, N.; Grossniklaus, D.A.; Klein, S.; Lamarche, B.; Lopez-Jimenez, F.; Rao, G.; St-Onge, M.P.; Towfighi, A.; et al. Assessing adiposity: A scientific statement from the American Heart Association. Circulation 2011, 124, 1996–2019. [Google Scholar] [CrossRef]
- Andreoli, A.; Scalzo, G.; Masala, S.; Tarantino, U.; Guglielmi, G. Body composition assessment by dual-energy X-ray absorptiometry (DXA). Radiol. Med. 2009, 114, 286–300. [Google Scholar] [CrossRef]
- Flegal, K.M.; Shepherd, J.A.; Looker, A.C.; Graubard, B.I.; Borrud, L.G.; Ogden, C.L.; Harris, T.B.; Everhart, J.E.; Schenker, N. Comparisons of percentage body fat, body mass index, waist circumference, and waist-stature ratio in adults. Am. J. Clin. Nutr. 2009, 89, 500–508. [Google Scholar] [CrossRef]
- Romero-Corral, A.; Somers, V.K.; Sierra-Johnson, J.; Jensen, M.D.; Thomas, R.J.; Squires, R.W.; Allison, T.G.; Korinek, J.; Lopez-Jimenez, F. Diagnostic performance of body mass index to detect obesity in patients with coronary artery disease. Eur. Heart J. 2007, 28, 2087–2093. [Google Scholar] [CrossRef] [PubMed]
- De Schutter, A.; Lavie, C.J.; Arce, K.; Menendez, S.G.; Milani, R.V. Correlation and discrepancies between obesity by body mass index and body fat in patients with coronary heart disease. J. Cardiopulm. Rehabil. Prev. 2013, 33, 77–83. [Google Scholar] [CrossRef]
- Gill, L.E.; Bartels, S.J.; Batsis, J.A. Weight Management in Older Adults. Curr. Obes. Rep. 2015, 4, 379–388. [Google Scholar] [CrossRef]
- Bergman, R.N.; Stefanovski, D.; Buchanan, T.A.; Sumner, A.E.; Reynolds, J.C.; Sebring, N.G.; Xiang, A.H.; Watanabe, R.M. A better index of body adiposity. Obesity (Silver Spring) 2011, 19, 1083–1089. [Google Scholar] [CrossRef] [PubMed]
- Yesil, E.; Kose, B.; Ozdemir, M. Is Body Adiposity Index a Better and Easily Applicable Measure for Determination of Body Fat? J. Am. Coll. Nutr. 2020, 1–6. [Google Scholar] [CrossRef]
- Lam, B.C.; Lim, S.C.; Wong, M.T.; Shum, E.; Ho, C.Y.; Bosco, J.I.; Chen, C.; Koh, G.C. A method comparison study to validate a novel param-eter of obesity, the body adiposity index, in Chinese subjects. Obesity (Silver Spring) 2013, 21, E634–E639. [Google Scholar] [CrossRef] [PubMed]
- Poirier, P.; Giles, T.D.; Bray, G.A.; Hong, Y.; Stern, J.S.; Pi-Sunyer, F.X.; Eckel, R.H. Obesity and cardiovascular disease: Pathophysiology, evaluation, and effect of weight loss. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 968–976. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.U.; Khan, M.U.; Riaz, H.; Raggi, P.; Valavoor, S.; Khan, M.Z.; Kolodziejczak, M.; Khan, M.S.; Krupica, T.; Alkhouli, M.; et al. Meta-analysis of the Relation of Body Mass Index to Cardiovascular Outcomes in Patients Receiving Intensive Low-Density Lipoprotein Choles-terol Lowering Therapy. Am. J. Cardiol. 2020, 125, 727–734. [Google Scholar] [CrossRef]
- Korzonek-Szlacheta, I.; Hudzik, B.; Nowak, J.; Szkodzinski, J.; Gasior, M.; Zubelewicz-Szkodzinska, B. Mean platelet volume is associated with serum 25-hydroxyvitamin D concentrations in patients with stable coronary artery disease. Heart Vessel. 2018, 33, 1275–1281. [Google Scholar] [CrossRef]
- National Research Council (US) Committee on Diet and Health. Diet and Health: Implications for Reducing Chronic Disease Risk; National Academies Press (US): Washington, DC, USA, 1989. [Google Scholar]
- Gallagher, D.; Heymsfield, S.B.; Heo, M.; Jebb, S.A.; Murgatroyd, P.R.; Sakamoto, Y. Healthy percentage body fat ranges: An approach for developing guidelines based on body mass index. Am. J. Clin. Nutr. 2000, 72, 694–701. [Google Scholar] [CrossRef]
- Houtkooper, L.B.; Lohman, T.G.; Going, S.B.; Howell, W.H. Why bioelectrical impedance analysis should be used for estimating adiposity. Am. J. Clin. Nutr. 1996, 64, 436S–448S. [Google Scholar] [CrossRef]
- Willett, K.; Jiang, R.; Lenart, E.; Spiegelman, D.; Willett, W. Comparison of bioelectrical impedance and BMI in predicting obesity-related medical conditions. Obesity (Silver Spring) 2006, 14, 480–490. [Google Scholar] [CrossRef]
- Kyle, U.G.; Genton, L.; Karsegard, L.; Slosman, D.O.; Pichard, C. Single prediction equation for bioelectrical impedance analysis in adults aged 20--94 years. Nutrition 2001, 17, 248–253. [Google Scholar] [CrossRef]
- Ignacio de Ulibarri, J.; Gonzalez-Madrono, A.; de Villar, N.G.; Gonzalez, P.; Gonzalez, B.; Mancha, A.; Rodriguez, F.; Fernandez, G. CONUT: A tool for controlling nutritional status. First validation in a hospital population. Nutr. Hosp. 2005, 20, 38–45. [Google Scholar]
- Muller, M.J.; Lagerpusch, M.; Enderle, J.; Schautz, B.; Heller, M.; Bosy-Westphal, A. Beyond the body mass index: Tracking body composi-tion in the pathogenesis of obesity and the metabolic syndrome. Obes. Rev. 2012, 13 (Suppl. S2), 6–13. [Google Scholar] [CrossRef]
- Batsis, J.A.; Mackenzie, T.A.; Bartels, S.J.; Sahakyan, K.R.; Somers, V.K.; Lopez-Jimenez, F. Diagnostic accuracy of body mass index to iden-tify obesity in older adults: NHANES 1999-2004. Int. J. Obes. (Lond) 2016, 40, 761–767. [Google Scholar] [CrossRef]
- Villareal, D.T.; Apovian, C.M.; Kushner, R.F.; Klein, S. Obesity in older adults: Technical review and position statement of the American So-ciety for Nutrition and NAASO, The Obesity Society. Am. J. Clin. Nutr. 2005, 82, 923–934. [Google Scholar] [CrossRef]
- Dehghan, M.; Merchant, A.T. Is bioelectrical impedance accurate for use in large epidemiological studies? Nutr. J. 2008, 7, 26. [Google Scholar] [CrossRef]
- Barreira, T.V.; Harrington, D.M.; Staiano, A.E.; Heymsfield, S.B.; Katzmarzyk, P.T. Body adiposity index, body mass index, and body fat in white and black adults. JAMA 2011, 306, 828–830. [Google Scholar] [CrossRef]
- Bennasar-Veny, M.; Lopez-Gonzalez, A.A.; Tauler, P.; Cespedes, M.L.; Vicente-Herrero, T.; Yanez, A.; Tomas-Salva, M.; Aguilo, A. Body ad-iposity index and cardiovascular health risk factors in Caucasians: A comparison with the body mass index and others. PLoS ONE 2013, 8, e63999. [Google Scholar] [CrossRef]
- Johnson, W.; Chumlea, W.C.; Czerwinski, S.A.; Demerath, E.W. Concordance of the recently published body adiposity index with meas-ured body fat percent in European-American adults. Obesity (Silver Spring) 2012, 20, 900–903. [Google Scholar] [CrossRef] [PubMed]
- Bernhard, A.B.; Scabim, V.M.; Serafim, M.P.; Gadducci, A.V.; Santo, M.A.; de Cleva, R. Modified body adiposity index for body fat estima-tion in severe obesity. J. Hum. Nutr. Diet. 2017, 30, 177–184. [Google Scholar] [CrossRef]
- Geliebter, A.; Atalayer, D.; Flancbaum, L.; Gibson, C.D. Comparison of body adiposity index (BAI) and BMI with estimations of % body fat in clinically severe obese women. Obesity (Silver Spring) 2013, 21, 493–498. [Google Scholar] [CrossRef]
- Kuhn, P.C.; Vieira Filho, J.P.; Franco, L.; Dal Fabbro, A.; Franco, L.J.; Moises, R.S. Evaluation of body adiposity index (BAI) to estimate per-cent body fat in an indigenous population. Clin. Nutr. 2014, 33, 287–290. [Google Scholar] [CrossRef]
- Zhao, D.; Li, Y.; Zheng, L.; Yu, K. Brief communication: Body mass index, body adiposity index, and percent body fat in Asians. Am. J. Phys. Anthropol. 2013, 152, 294–299. [Google Scholar] [CrossRef]
- Zhang, Z.Q.; Liu, Y.H.; Xu, Y.; Dai, X.W.; Ling, W.H.; Su, Y.X.; Chen, Y.M. The validity of the body adiposity index in predicting percentage body fat and cardiovascular risk factors among Chinese. Clin. Endocrinol. (Oxf) 2014, 81, 356–362. [Google Scholar] [CrossRef]
- Gujral, U.P.; Vittinghoff, E.; Mongraw-Chaffin, M.; Vaidya, D.; Kandula, N.R.; Allison, M.; Carr, J.; Liu, K.; Narayan, K.M.V.; Kanaya, A.M. Cardiometabolic Abnormalities Among Normal-Weight Persons From Five Racial/Ethnic Groups in the United States: A Cross-sectional Analysis of Two Cohort Studies. Ann. Intern. Med. 2017, 166, 628–636. [Google Scholar] [CrossRef]
- Camina Martin, M.A.; de Mateo Silleras, B.; Redondo del Rio, M.P. Body composition analysis in older adults with dementia. Anthropome-try and bioelectrical impedance analysis: A critical review. Eur. J. Clin. Nutr. 2014, 68, 1228–1233. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Weight Status | Age ≥ 60 Years | |
|---|---|---|
| Men | Women | |
| Underweight | <13% | <25% |
| Normal weight | 13–25% | 25–38% |
| Overweight | 26–31% | 39–43% |
| Obesity | >31% | >43% |
| Sex, men n (%) | 52 (30.8%) |
| Age (years) | 75 (70–84) |
| Prior myocardial infarction n (%) | 30 (18.0) |
| Heart failure n (%) | 73 (43.2%) |
| Atrial fibrillation n (%) | 28 (16.7) |
| Hyperlipidemia n (%) | 39 (23.1) |
| Diabetes mellitus n (%) | 63 (37.3) |
| Hypertension n (%) | 154 (91.1) |
| Leucocytes (103/mm3) | 6.5 (5.2–8.4) |
| Erythrocytes (106/mm3) | 4.2 (3.9–4.5) |
| Hemoglobin (g/dL) | 12.5 (12.7–13.4) |
| Hematocrit (%) | 38 (36–40) |
| Platelets (103/mm3) | 215 (171–262) |
| Total cholesterol (mmol/L) | 4.4 (3.6–5.3) |
| HDL cholesterol (mmol/L) | 1.3 (1.1–1.7) |
| LDL cholesterol (mmol/L) | 2.6 (1.7–3.2) |
| Triglycerides (mmol/L) | 1.1 (0.9–1.4) |
| Serum creatinine (μmol/L) | 75 (65–91) |
| eGFR (mL/min/1.73 m2) | 76 (61–89) |
| Aspartate aminotransferase (AST) (U/L) | 18 (15–21) |
| Alanine aminotransferase (ALT) (U/L) | 15 (11–20) |
| Bilirubin (mmol/L) | 10.7 (8.5–14.7) |
| Total protein (g/L) | 60.0 (56.2–65.3) |
| Albumin (mg/mL) | 36 (34–40) |
| CONUT score | 2 (1–3) |
| Weight (kg) | 70 (61–79) |
| Height (m) | 1.68 (1.58–1.75) |
| BMI | 27.6 (24.3–31.3) |
| BAI | 34.6 (29.0–42.1) |
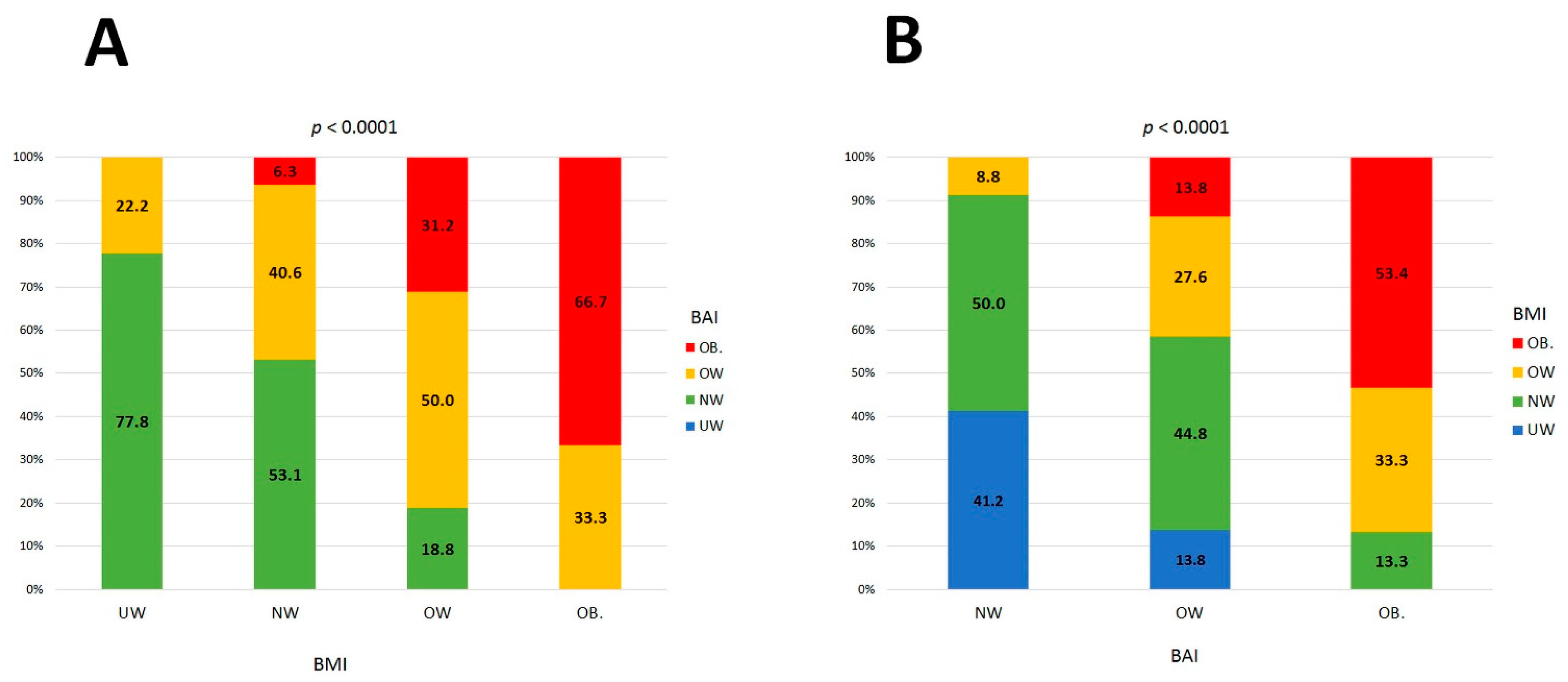
| Weight status by BMI | |
| 39 (23.1) |
| 69 (41.0) |
| 35 (20.7) |
| 26 (15.2) |
| Weight status by BAI | |
| 0 (0) |
| 74 (43.8) |
| 63 (37.3) |
| 32 (18.9) |
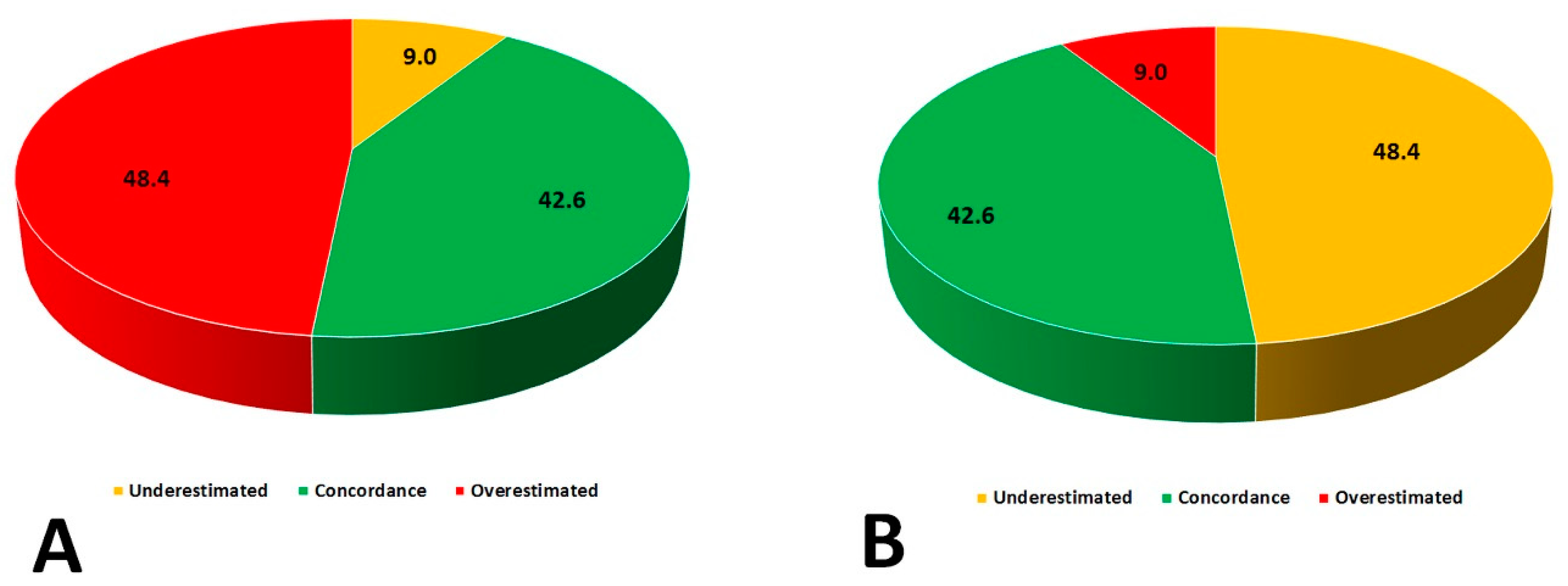
| Concordant classification of weight status by both BMI and BAI, n (%) | 72 (42.6) |
| Hip circumference (cm) | 104 (97–112) |
| Waist circumference (cm) | 103 (90–114) |
| Mid-upper arm circumference (cm) | 28 (26–31) |
| Calf circumference (cm) | 34 (32–37) |
| Waist-to-hip ratio | 0.97 (0.90–1.00) |
| Waist-to-height ratio | 0.64 (0.56–0.73) |
| Fat percentage (%) | 33.6 (26.3–42.3) |
| Fat mass (kg) | 22.8 (16.3–32.6) |
| Lean mass (kg) | 42.8 (38.9–61.7) |
| Muscle mass (kg) | 40.6 (36.9–49.1) |
| Total body water percentage (%) | 29.7 (26.2–37.0) |
| Total body water percentage (kg) | 43.8 (39.6–50.7) |
| BAI Weight Status | |||||||
|---|---|---|---|---|---|---|---|
| BMI cutoff | AUC (95%CI) | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | p | |
| Normal weight | ≤27 | 0.88 (0.78–0.94) | 85 | 79 | 76 | 87 | <0.0001 |
| Overweight | >25.7 | 0.61 (0.51–0.72) | 83 | 51 | 50 | 83 | 0.05 |
| Obesity | >28.7 | 0.93 (0.85–0.97) | 100 | 71 | 45 | 100 | <0.0001 |
| BMI weight status | |||||||
| BAI cutoff | AUC (95%CI) | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | p | |
| Underweight | <33.1 | 0.78 (0.68–0.87) | 78 | 72 | 45 | 91 | <0.0001 |
| Normal weight | <43.5 | 0.60 (0.48–0.70) | 100 | 28 | 49 | 100 | 0.13 |
| Overweight | >37 | 0.62 (0.50–0.73) | 62 | 69 | 34 | 88 | 0.11 |
| Obesity | >42 | 0.92 (0,82–0,97) | 92 | 88 | 61 | 98 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hudzik, B.; Nowak, J.; Szkodzinski, J.; Danikiewicz, A.; Korzonek-Szlacheta, I.; Zubelewicz-Szkodzińska, B. Discordance between Body-Mass Index and Body Adiposity Index in the Classification of Weight Status of Elderly Patients with Stable Coronary Artery Disease. J. Clin. Med. 2021, 10, 943. https://doi.org/10.3390/jcm10050943
Hudzik B, Nowak J, Szkodzinski J, Danikiewicz A, Korzonek-Szlacheta I, Zubelewicz-Szkodzińska B. Discordance between Body-Mass Index and Body Adiposity Index in the Classification of Weight Status of Elderly Patients with Stable Coronary Artery Disease. Journal of Clinical Medicine. 2021; 10(5):943. https://doi.org/10.3390/jcm10050943
Chicago/Turabian StyleHudzik, Bartosz, Justyna Nowak, Janusz Szkodzinski, Aleksander Danikiewicz, Ilona Korzonek-Szlacheta, and Barbara Zubelewicz-Szkodzińska. 2021. "Discordance between Body-Mass Index and Body Adiposity Index in the Classification of Weight Status of Elderly Patients with Stable Coronary Artery Disease" Journal of Clinical Medicine 10, no. 5: 943. https://doi.org/10.3390/jcm10050943
APA StyleHudzik, B., Nowak, J., Szkodzinski, J., Danikiewicz, A., Korzonek-Szlacheta, I., & Zubelewicz-Szkodzińska, B. (2021). Discordance between Body-Mass Index and Body Adiposity Index in the Classification of Weight Status of Elderly Patients with Stable Coronary Artery Disease. Journal of Clinical Medicine, 10(5), 943. https://doi.org/10.3390/jcm10050943