
Generalized Joint Hypermobility and Injuries: A Prospective Cohort Study of 185 Pre-Professional Contemporary Dancers

Abstract
1. Introduction
2. Methods
2.1. Participants and Procedures
2.2. Generalized Joint Hypermobility
2.3. Injury Registration
2.4. Injury Definitions
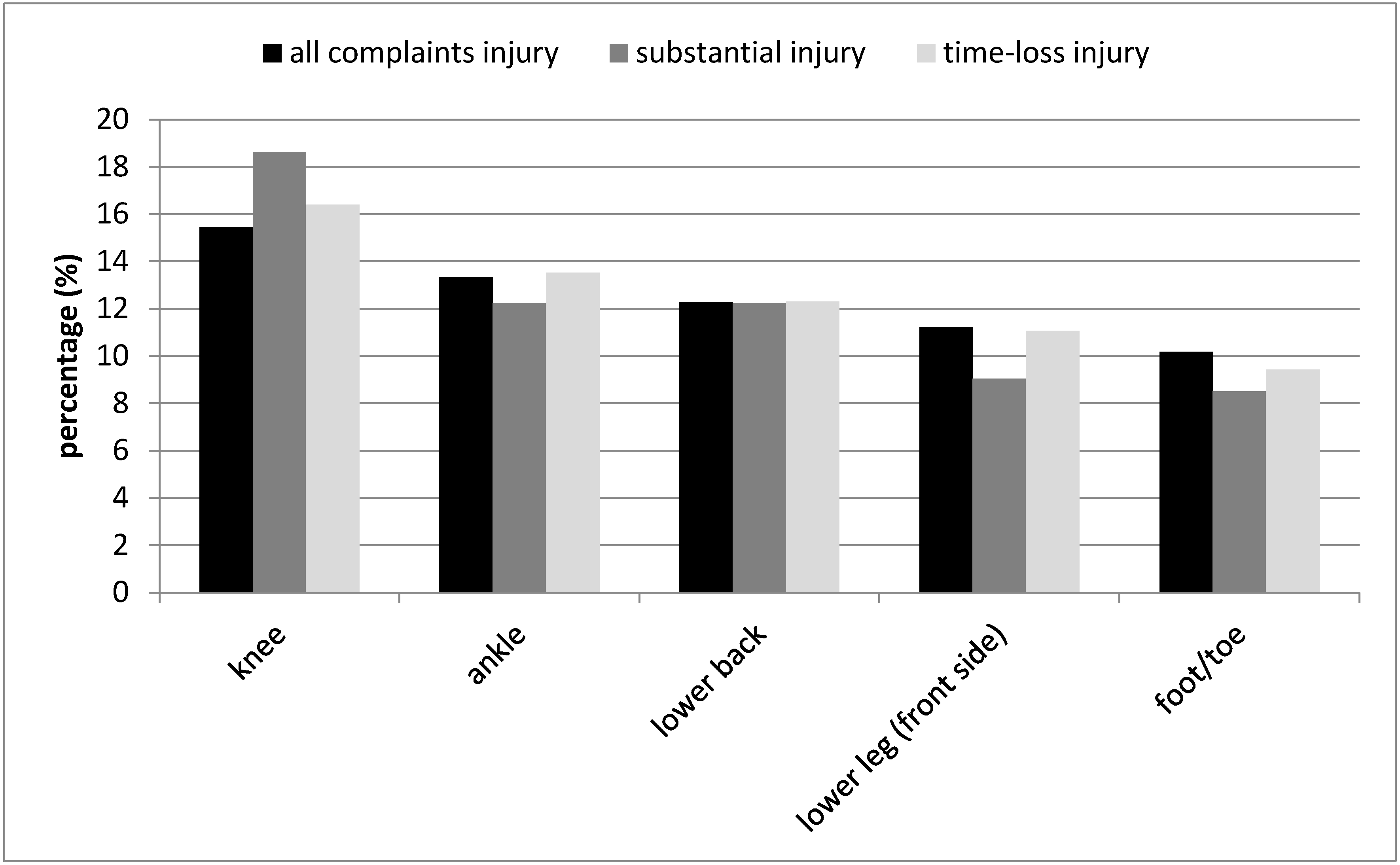
- All complaints injury: any physical complaint resulting in a severity score higher than zero on the OSTRC questionnaire irrespective of the need for medical attention or time loss from dance activities [23].
- Substantial injury: any physical complaint resulting in a severity score higher than zero on the OSTRC questionnaire irrespective of the need for medical attention and resulting in problems leading to moderate or severe reductions (value ≥13 on question 2 or 3 of the OSTRC) in training volume or moderate or severe reductions in performance or complete inability to participate in dance [23].
- Time-loss injury: any physical complaint resulting in a severity score higher than zero on the OSTRC questionnaire and resulting in a dancer not being able to complete a class, rehearsal, or performance or a subsequent class, rehearsal, or performance for one or more days beyond the day of onset [24].
2.5. Statistical Analysis
3. Results
3.1. Participants
3.2. Generalized Joint Hypermobility
3.3. Injuries
3.4. Risk Factors
4. Discussion
Strengths and Limitations of the Study
5. Conclusions and Implications for Practice
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Caine, D.; Goodwin, B.J.; Caine, C.G.; Bergeron, G. Epidemiological Review of Injury in Pre-Professional Ballet Dancers. J. Dance Med. Sci. 2015, 19, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Bowerman, E.A.; Whatman, C.; Harris, N.; Bradshaw, E. A review of the risk factors for lower extremity overuse injuries in young elite female ballet dancers. J. Dance Med. Sci. 2015, 19, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Kenny, S.J.; Whittaker, J.L.; Emery, C.A. Risk factors for musculoskeletal injury in preprofessional dancers: A systematic review. Br. J. Sports Med. 2016, 50, 997–1003. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.; Reid, D.; Cadwell, J.; Palmer, P. Injury Incidence, Dance Exposure and the Use of the Movement Competency Screen (Mcs) to Identify Variables Associated with Injury in Full-Time Pre-Professional Dancers. Int. J. Sports Phys. Ther. 2017, 12, 352–370. [Google Scholar]
- van Winden, D.; Van Rijn, R.M.; Richardson, A.; Savelsbergh, G.J.P.; Oudejans, R.R.D.; Stubbe, J.H. Detailed injury epidemiology in contemporary dance: A 1-year prospective study of 134 students. BMJ Open Sport Exerc. Med. 2019, 5, e000453. [Google Scholar] [CrossRef] [PubMed]
- Finch, C. A new framework for research leading to sports injury prevention. J. Sci. Med. Sport 2006, 9, 3–9, discussion 10. [Google Scholar] [CrossRef]
- van Mechelen, W.; Hlobil, H.; Kemper, H.C. Incidence, severity, aetiology and prevention of sports injuries. A review of concepts. Sports Med. 1992, 14, 82–99. [Google Scholar] [CrossRef]
- Beighton, P.; Solomon, L.; Soskolne, C.L. Articular mobility in an African population. Ann. Rheum. Dis. 1973, 32, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Grahame, R.; Jenkins, J.M. Joint hypermobility—Asset or liability? A study of joint mobility in ballet dancers. Ann. Rheum. Dis. 1972, 31, 109–111. [Google Scholar] [CrossRef] [PubMed]
- Day, H.; Koutedakis, Y.; Wyon, M.A. Hypermobility and dance: A review. Int. J. Sports Med. 2011, 32, 485–489. [Google Scholar] [CrossRef]
- Armstrong, R. The Beighton Score and Injury in Dancers: A Prospective Cohort Study. J. Sport Rehabil. 2019, 29, 563–571. [Google Scholar] [CrossRef] [PubMed]
- McCormack, M. Teaching the Hypermobile Dancer. IADMS Bull. Teach. 2010, 2, 5–8. [Google Scholar]
- Ruemper, A.; Watkins, K. Correlations Between General Joint Hypermobility and Joint Hypermobility Syndrome and Injury in Contemporary Dance Students. J. Dance Med. Sci. 2012, 16, 161–166. [Google Scholar] [PubMed]
- Scheper, M.C.; de Vries, J.E.; de Vos, R.; Verbunt, J.; Nollet, F.; Engelbert, R.H. Generalized joint hypermobility in professional dancers: A sign of talent or vulnerability? Rheumatology 2013, 52, 651–658. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.O.; Davies, L.; de Medici, A.; Hakim, A.; Haddad, F.; Macgregor, A. Prevalence and profile of musculoskeletal injuries in ballet dancers: A systematic review and meta-analysis. Phys. Ther. Sport 2016, 19, 50–56. [Google Scholar] [CrossRef]
- Bronner, S.; Bauer, N.G. Risk factors for musculoskeletal injury in elite pre-professional modern dancers: A prospective cohort prognostic study. Phys. Ther. Sport 2018, 31, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Biernacki, J.L.; Stracciolini, A.; Fraser, J.; Miceli, L.J.; Sugimoto, D. Risk Factors for Lower-Extremity Injuries in Female Ballet Dancers. Clin. J. Sports Med. 2018. [Google Scholar] [CrossRef]
- van Seters, C.; van Rijn, R.M.; van Middelkoop, M.; Stubbe, J.H. Risk Factors for Lower-Extremity Injuries Among Contemporary Dance Students. Clin. J. Sport Med. 2020, 30, 60–66. [Google Scholar] [CrossRef]
- van Winden, D.; van Rijn, R.M.; Savelsbergh, G.J.P.; Oudejans, R.R.D.; Stubbe, J.H. Limited Coping Skills, Young Age, and High BMI Are Risk Factors for Injuries in Contemporary Dance: A 1-Year Prospective Study. Front. Psychol. 2020, 11, 1452. [Google Scholar] [CrossRef]
- Clarsen, B.; Myklebust, G.; Bahr, R. Development and validation of a new method for the registration of overuse injuries in sports injury epidemiology: The Oslo Sports Trauma Research Centre (OSTRC) overuse injury questionnaire. Br. J. Sports Med. 2013, 47, 495–502. [Google Scholar] [CrossRef]
- Fuller, C.W.; Ekstrand, J.; Junge, A.; Andersen, T.E.; Bahr, R.; Dvorak, J.; Hagglund, M.; McCrory, P.; Meeuwisse, W.H. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Scand. J. Med. Sci. Sports 2006, 16, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Stubbe, J.H.; Richardson, A.; van Rijn, R.M. Prospective cohort study on injuries and health problems among circus arts students. BMJ Open Sport Exerc. Med. 2018, 4, e000327. [Google Scholar] [CrossRef] [PubMed]
- Clarsen, B.; Ronsen, O.; Myklebust, G.; Florenes, T.W.; Bahr, R. The Oslo Sports Trauma Research Center questionnaire on health problems: A new approach to prospective monitoring of illness and injury in elite athletes. Br. J. Sports Med. 2014, 48, 754–760. [Google Scholar] [CrossRef] [PubMed]
- Kenny, S.J.; Palacios-Derflingher, L.; Whittaker, J.L.; Emery, C.A. The Influence of Injury Definition on Injury Burden in Preprofessional Ballet and Contemporary Dancers. J. Orthop. Sports Phys. Ther. 2018, 48, 185–193. [Google Scholar] [CrossRef]
- Stewart, D.R.; Burden, S.B. Does generalised ligamentous laxity increase seasonal incidence of injuries in male first division club rugby players? Br. J. Sports Med. 2004, 38, 457–460. [Google Scholar] [CrossRef]
- Chan, C.; Hopper, L.; Zhang, F.; Pacey, V.; Nicholson, L.L. The prevalence of generalized and syndromic hypermobility in elite Australian dancers. Phys. Ther. Sport 2018, 32, 15–21. [Google Scholar] [CrossRef]
- Field, A. Discovering Statistics Using SPSS; Sage Publications: London, UK, 2009. [Google Scholar]
- Longworth, B.; Fary, R.; Hopper, D. Prevalence and predictors of adolescent idiopathic scoliosis in adolescent ballet dancers. Arch. Phys. Med. Rehabil. 2014, 95, 1725–1730. [Google Scholar] [CrossRef]
- Roussel, N.A.; Nijs, J.; Mottram, S.; Van Moorsel, A.; Truijen, S.; Stassijns, G. Altered lumbopelvic movement control but not generalized joint hypermobility is associated with increased injury in dancers. A prospective study. Man. Ther. 2009, 14, 630–635. [Google Scholar] [CrossRef]
- Peduzzi, P.; Concato, J.; Kemper, E.; Holford, T.R.; Feinstein, A.R. A simulation study of the number of events per variable in logistic regression analysis. J. Clin. Epidemiol. 1996, 49, 1373–1379. [Google Scholar] [CrossRef]
- Welsh, T.; Ambegaonkar, J.; Mainwaring, L. Research in the Dance Sciences; University Press of Florida: Gainesville, FL, USA, in press.
- Clarsen, B.; Bahr, R.; Myklebust, G.; Andersson, S.H.; Docking, S.I.; Drew, M.; Finch, C.F.; Fortington, L.V.; Harøy, J.; Khan, K.M.; et al. Improved reporting of overuse injuries and health problems in sport: An update of the Oslo Sport Trauma Research Center questionnaires. Br. J. Sports Med. 2020, 54, 390–396. [Google Scholar] [CrossRef] [PubMed]
- Bahr, R. Why screening tests to predict injury do not work-and probably never will …: A critical review. Br. J. Sports Med. 2016, 50, 776–780. [Google Scholar] [CrossRef]


{kind=link}
| Total Population (N = 185) | Dance (n = 117) | Dance Teacher (n = 68) | |
|---|---|---|---|
| Sex (female) | 127 (68.6%) | 63 (53.8%) | 64 (94.1%) |
| Age (years) | 19.1 ± 1.3 | 18.8 ± 0.9 | 19.4 ± 1.9 |
| Previous long-lasting injury (yes) # | 60 (33.3%) | 29 (25.9%) | 31 (45.6%) |
| Generalized joint hypermobility * | |||
| Beighton score | 2.8 ± 2.3 | 3.2 ± 2.5 | 2.2 ± 2.0 |
| Not hypermobile (0–3) Hypermobile (4–6) Extreme hypermobile (7–9) | 129 (70.9%) 25 (13.7%) 28 (15.4%) | 76 (65.5%) 17 (14.7%) 23 (19.8%) | 53 (80.3%) 8 (12.1%) 5 (7.6%) |
| Not hypermobile (0–3) Hypermobile (4–9) | 129 (70.9%) 53 (29.1%) | 76 (65.5%) 40 (34.5%) | 53 (80.3%) 13 (19.7%) |
| Not hypermobile (0–5) Hypermobile (6–9) | 154 (84.6%) 28 (15.4%) | 93 (80.2%) 23 (19.8%) | 61 (92.4%) 5 (7.6%) |
| Non-Injured (n = 60) | Injured (n = 125) | Univariate Analysis OR (95% CI) | Multivariate Analysis OR (95% CI) | ||||
|---|---|---|---|---|---|---|---|
| Sex (female) | 44 (73.3%) | 83 (66.4%) | 0.72 (0.36–1.42) | 0.75 (0.33–1.70) | 0.65 (0.29–1.49) | 0.67 (0.30–1.53) | 0.71 (0.32–1.56) |
| Age (years) | 19.0 ± 1.15 | 19.1 ± 1.43 | 1.08 (0.85–1.39) | 1.04 (0.80–1.35) | 1.04 (0.80–1.35) | 1.04 (0.80–1.35) | 1.04 (0.80–1.35) |
| Educational Program | |||||||
| Bachelor dance Bachelor dance teacher | 37 (61.7%) 23 (38.3%) | 80 (64.0%) 45 (36.0%) | Ref. 0.91 (0.48–1.71) | Ref. 0.84 (0.37–1.88) | Ref. 0.93 (0.42–2.06) | Ref. 0.94 (0.42–2.07) | Ref. 0.88 (0.40–1.92) |
| Previous long-lasting injury (yes) # | 12 (20.3%) | 48 (39.7%) | 2.58 (1.24–5.35) | 2.74 (1.26–5.94) | 2.69 (1.24–5.82) | 2.60 (1.21–5.59) | 2.68 (1.24–5.81) |
| Generalized joint hypermobility * | |||||||
| Beighton score (0–9) | 2.95 ± 2.23 | 2.78 ± 2.40 | 0.97 (0.85–1.11) | 0.96 (0.82–1.12) | |||
| Not hypermobile (0–3) Hypermobile (4–6) Extreme hypermobile (7–9) | 41 (71.9%) 7 (12.3%) 9 (15.8%) | 88 (70.4%) 18 (14.4%) 19 (15.2%) | Ref. 1.20 (0.46–3.09) 0.98 (0.41–2.36) | Ref. 1.42 (0.51–3.90) 0.94 (0.35–2.49) | |||
| Not hypermobile (0–3) Hypermobile (4–9) | 41 (71.9%) 16 (28.1%) | 88 (70.4%) 37 (29.6%) | Ref. 1.08 (0.54–2.16) | Ref. 1.15 (0.53–2.49) | |||
| Not hypermobile (0–5) Hypermobile (6–9) | 48 (84.2%) 9 (15.8%) | 106 (84.8%) 19 (15.2%) | Ref. 0.96 (0.40–2.27) | Ref. 0.87 (0.34–2.27) | |||
| Nagelkerke R2 | 0.059 | 0.060 | 0.057 | 0.057 | |||
| Non-Injured (n = 105) | Injured (n = 80) | Univariate Analysis OR (95% CI) | Multivariate Analysis OR (95% CI) | ||||
|---|---|---|---|---|---|---|---|
| Sex (female) | 69 (65.7%) | 58 (72.5%) | 1.38 (0.73–2.60) | 1.14 (0.52–2.50) | 0.97 (0.44–2.15) | 1.01 (0.46–2.21) | 1.04 (0.49–2.22) |
| Age (years) | 19.04 ± 1.27 | 19.08 ± 1.44 | 1.02 (0.82–1.27) | 0.95 (0.75−1.20) | 0.95 (0.75–1.20) | 0.95 (0.75–1.20) | 0.95 (0.75–1.20) |
| Educational Program | |||||||
| Bachelor dance Bachelor dance teacher | 73 (69.5%) 32 (30.5%) | 44 (55.0%) 36 (45.0%) | Ref. 1.87 (1.02–3.42) | Ref. 1.57 (0.73–3.39) | Ref. 1.78 (0.83–3.82) | Ref. 1.79 (0.84–3.83) | Ref. 1.70 (0.81–3.58) |
| Previous long-lasting injury (yes) # | 23 (22.3%) | 37 (48.1%) | 3.22 (1.69–6.13) | 2.96 (1.50–5.84) | 2.85 (1.45–5.61) | 2.76 (1.42–5.37) | 2.84 (1.45–5.59) |
| Generalized joint hypermobility * | |||||||
| Beighton score (0–9) | 2.92 ± 2.38 | 2.71 ± 2.31 | 0.96 (0.85–1.09) | 0.94 (0.81–1.08) | |||
| Not hypermobile (0–3) Hypermobile (4–6) Extreme hypermobile (7–9) | 73 (71.6%) 13 (12.7%) 16 (15.7%) | 56 (70.0%) 12 (15.0%) 12 (15.0%) | Ref. 1.20 (0.51–2.84) 0.98 (0.43–2.23) | Ref. 1.33 (0.51–3.43) 0.90 (0.35–2.27) | |||
| Not hypermobile (0–3) Hypermobile (4–9) | 73 (71.6%) 29 (28.4%) | 56 (70.0%) 24 (30.0%) | Ref. 1.08 (0.57–2.05) | Ref. 1.08 (0.52–2.25) | |||
| Not hypermobile (0–5) Hypermobile (6–9) | 86 (84.3%) 16 (15.7%) | 68 (85.0%) 12 (15.0%) | Ref. 0.95 (0.42–2.14) | Ref. 0.84 (0.34–2.10) | |||
| Nagelkerke R2 | 0.115 | 0.113 | 0.110 | 0.110 | |||
| Non-Injured (n = 84) | Injured (n = 101) | Univariate Analysis OR (95% CI) | Multivariate Analysis OR (95% CI) | ||||
|---|---|---|---|---|---|---|---|
| Sex (female) | 60 (71.4%) | 67 (66.3%) | 0.79 (0.42–1.48) | 0.65 (0.30–1.39) | 0.60 (0.28–1.31) | 0.60 (0.28–1.31) | 0.62 (0.29–1.30) |
| Age (years) | 18.94 ± 1.10 | 19.15 ± 1.51 | 1.13 (0.90–1.42) | 1.05 (0.82–1.35) | 1.05 (0.82–1.35) | 1.05 (0.82–1.35) | 1.05 (0.82–1.35) |
| Educational Program | |||||||
| Bachelor dance Bachelor dance teacher | 57 (67.9%) 27 (32.1%) | 60 (59.4%) 41 (40.6%) | Ref. 1.44 (0.79–2.65) | Ref. 1.46 (0.68 −3.15) | Ref. 1.57 (0.73–3.36) | Ref. 1.57 (0.73–3.36) | Ref. 1.54 (0.73–3.26) |
| Previous long-lasting injury (yes) # | 17 (20.5%) | 43 (44.3%) | 3.09 (1.59–6.02) | 3.04 (1.50–6.15) | 2.95 (1.46–5.94) | 2.94 (1.47–5.89) | 2.94 (1.46–5.93) |
| Generalized joint hypermobility * | |||||||
| Beighton score (0–9) | 2.94 ± 2.29 | 2.74 ± 2.39 | 0.97 (0.85–1.09) | 0.97 (0.84–1.13) | |||
| Not hypermobile (0–3) Hypermobile (4–6) Extreme hypermobile (7–9) | 57 (70.4%) 12 (14.8%) 12 (14.8%) | 72 (71.3%) 13 (12.9%) 16 (15.8%) | Ref. 0.86 (0.36–2.02) 1.06 (0.46–2.41) | Ref. 1.10 (0.43–2.83) 1.09 (0.43–2.75) | |||
| Not hypermobile (0–3) Hypermobile (4–9) | 57 (70.4%) 24 (29.6%) | 72 (71.3%) 29 (28.7%) | Ref. 0.96 (0.50–1.82) | Ref. 1.09 (0.53–2.27) | |||
| Not hypermobile (0–5) Hypermobile (6–9) | 69 (85.2%) 12 (14.8%) | 85 (84.2%) 16 (15.8%) | Ref. 1.08 (0.48–2.44) | Ref. 1.07 (0.43–2.64) | |||
| Nagelkerke R2 | 0.099 | 0.098 | 0.098 | 0.098 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Rijn, R.M.; Stubbe, J.H. Generalized Joint Hypermobility and Injuries: A Prospective Cohort Study of 185 Pre-Professional Contemporary Dancers. J. Clin. Med. 2021, 10, 1007. https://doi.org/10.3390/jcm10051007
van Rijn RM, Stubbe JH. Generalized Joint Hypermobility and Injuries: A Prospective Cohort Study of 185 Pre-Professional Contemporary Dancers. Journal of Clinical Medicine. 2021; 10(5):1007. https://doi.org/10.3390/jcm10051007
Chicago/Turabian Stylevan Rijn, Rogier M., and Janine H. Stubbe. 2021. "Generalized Joint Hypermobility and Injuries: A Prospective Cohort Study of 185 Pre-Professional Contemporary Dancers" Journal of Clinical Medicine 10, no. 5: 1007. https://doi.org/10.3390/jcm10051007
APA Stylevan Rijn, R. M., & Stubbe, J. H. (2021). Generalized Joint Hypermobility and Injuries: A Prospective Cohort Study of 185 Pre-Professional Contemporary Dancers. Journal of Clinical Medicine, 10(5), 1007. https://doi.org/10.3390/jcm10051007