
Recommendations for Diagnosis and Treatment of Lumbosacral Radicular Pain: A Systematic Review of Clinical Practice Guidelines

Abstract
1. Introduction
2. Methods
2.1. Review Registration and Reporting
2.2. Literature Search
2.3. Guidelines Selection
2.4. Quality Assessment
2.5. Data Extraction and Synthesis
- a.
- Consistent recommendations: from the guidelines including recommendation for a specific approach, the majority (≥80%) indicate as ‘should do’, ‘could do’, ‘do not do’, or ‘uncertain’, but without conflicting recommendations across guidelines. Conflicting recommendations are present when at least one ‘should do’ or ‘could do’, and at least one ‘do not do’ is applied for the same recommendation in different guidelines.
- b.
- Common recommendations: from the guidelines including recommendation for a specific approach, most (between 50% and 80%) indicate as ‘should do’, ‘could do’, ‘do not do’, or ‘uncertain’, but with no conflicting recommendations across guidelines.
- c.
- Inconsistent recommendations: a recommendation for one approach indicates ‘should do’ or ‘could do’, and another recommendation for the same approach indicates ‘do not do’ or ‘uncertain’, both recommendations issued by different guidelines; the same applies if a recommendation for an approach is ‘uncertain’, and another recommendation for the same approach is ‘do not do’.
3. Results
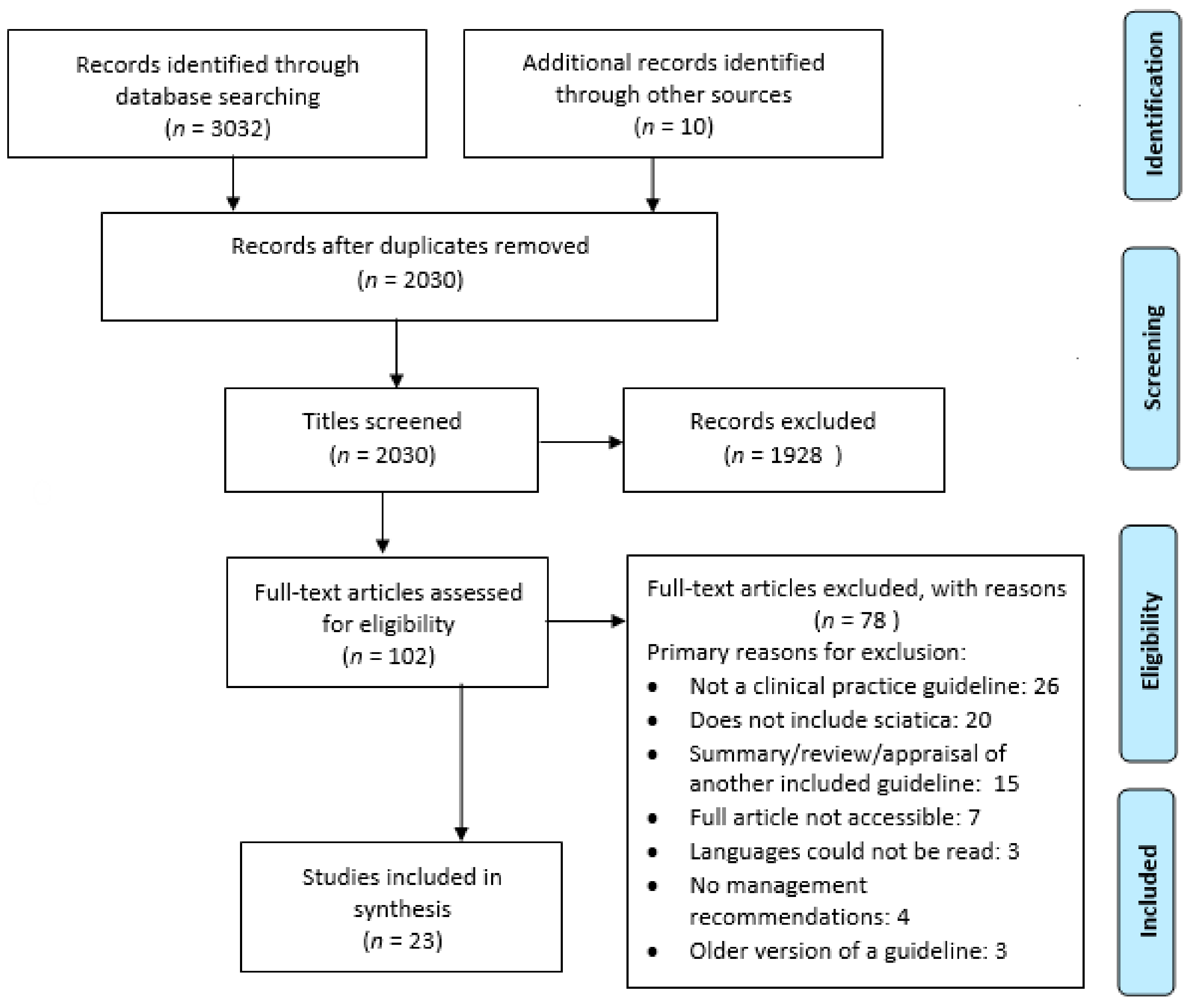
3.1. Guidelines Selection
3.2. Quality Assessment and Inter-Rater Agreement
3.3. Recommendations for Diagnosis
3.3.1. Physical Examination
3.3.2. Diagnostics
3.4. Guideline Recommendations for Treatment
3.4.1. Non-Invasive Treatments
3.4.2. Pharmacological Interventions
3.4.3. Invasive Treatments and Referral
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- “Guideline*”.ab,ti.
- Exp Guideline/or exp Practice Guideline/;
- Clinical practice guideline.ab,ti.
- 1 or 2 or 3;
- Back disorder*.tw,kf.;
- Dorsalgia.tw,kf.;
- Exp Back Pain/;
- (Backache* or back ache*).tw,kf.;
- ((Lumb* or back) adj3 pain).tw,kf.;
- Coccyx.tw,kf.;
- Coccydynia.tw,kf.;
- Sciatic*.tw,kf.;
- Exp sciatic neuropathy/;
- Spondylosis.tw,kf.;
- Lumbago.tw,kf.;
- Ischialgia.tw,kf.;
- (Discitis or diskitis).tw,kf.;
- ((Disc* or disk*) adj3 degenerat*).tw,kf.;
- ((Disc* or disk*) adj3 prolapse*).tw,kf.;
- ((Disc* or disk*) adj3 herniat*).tw,kf.
- Intervertebral Disc/;
- Exp Intervertebral Disk Displacement/;
- Exp Intervertebral Disc Degeneration/;
- Lumbar Vertebrae/;
- Nerve Compression Syndromes/;
- Spinal Osteophytosis/;
- Radiculopathy/;
- Polyradiculopathy/;
- Radicul*.tw,kf.;
- polyradicul*.tw,kf.;
- arachnoiditis.tw,kf.;
- exp Spinal Nerve Roots/;
- or/5–32
- 4 and 33
Appendix B

{kind=link}
| Recommendation Classification | Definition | Examples of Terminology Used in Guidelines |
|---|---|---|
| Should do | Strong recommendations based on strong evidence | Offer, should occur, provide, always do, give, use, apply, (strongly) endorsed, endorsed, must be considered, should be considered, provide, promote and facilitate, important to do, carried out, primary choice, must be done, usually appropriate |
| Could do | When a recommendation could be ‘Considered’ | May include, recommend, practitioner might, suggest, may be used, advice, give, may be considered, conditional recommendation, evaluate, can be evaluated, can be tried, may be appropriate, suggested, should be carefully considered |
| Do not do | When a recommendation should not be offered | Should refrain from, do not routinely offer, not appropriate, should not, do not give, do not use, do not, not indicated, do not start |
| Uncertain | Inconclusive recommendation | ‘We are unable to recommend for or against’, inconclusive evidence, uncertain, no basis for recommending, Insufficient evidence to make a recommendation for or against |
References
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef]
- Freburger, J.K.; Holmes, G.M.; Agans, R.P.; Jackman, A.M.; Darter, J.D.; Wallace, A.S.; Castel, L.D.; Kalsbeek, W.D.; Carey, T.S. The Rising Prevalence of Chronic Low Back Pain. Arch. Intern. Med. 2009, 169, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Hoy, D.; March, L.; Brooks, P.; Woolf, A.; Blyth, F.; Vos, T.; Buchbinder, R. Measuring the global burden of low back pain. Best Pr. Res. Clin. Rheumatol. 2010, 24, 155–165. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, N.E.; Ward, S.P. Low Back Pain: What Have Clinical Guidelines Ever Done for Us? J. Orthop. Sports Phys. Ther. 2018, 48, 54–57. [Google Scholar] [CrossRef]
- Disease, G.B.D.; Injury, I.; Prevalence, C. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: A systematic analy-sis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar]
- Hoy, D.; Bain, C.; Williams, G.; March, L.; Brooks, P.; Blyth, F.; Woolf, A.; Vos, T.; Buchbinder, R. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012, 64, 2028–2037. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.C.; Konstantinou, K.; Egbewale, B.E.; Dunn, K.M.; Lewis, M.; Van Der Windt, D. Clinical Outcomes Among Low Back Pain Consulters With Referred Leg Pain in Primary Care. Spine 2011, 36, 2168–2175. [Google Scholar] [CrossRef]
- Merskey, H.; Bogduk, N. Classification of Chronic Pain: Descriptions of Chronic Pain Syndromes and Definitions of Pain Terms; IASP Press: Seattle, WA, USA, 1994. [Google Scholar]
- Lin, C.-W.; Verwoerd, A.J.H.; Maher, C.; Verhagen, A.; Pinto, R.; Luijsterburg, P.A.J.; Hancock, M. How is radiating leg pain defined in randomized controlled trials of conservative treatments in primary care? A systematic review. Eur. J. Pain 2014, 18, 455–464. [Google Scholar] [CrossRef]
- Hider, S.L.; Whitehurst, D.G.T.; Thomas, E.; Foster, N.E. Pain location matters: The impact of leg pain on health care use, work disability and quality of life in patients with low back pain. Eur. Spine J. 2014, 24, 444–451. [Google Scholar] [CrossRef] [PubMed]
- Konstantinou, K.; Hider, S.L.; Jordan, J.L.; Lewis, M.; Dunn, K.M.; Hay, E.M. The impact of low back-related leg pain on outcomes as compared with low back pain alone: A systematic review of the literature. Clin. J. Pain. 2013, 29, 644–654. [Google Scholar] [CrossRef]
- van Tulder, M.W.; Koes, B.W.; Bouter, L.M. A cost-of-illness study of back pain in The Netherlands. Pain 1995, 62, 233–240. [Google Scholar] [CrossRef]
- Oliveira, C.B.; Maher, C.G.; Pinto, R.Z.; Traeger, A.C.; Lin, C.-W.C.; Chenot, J.-F.; Van Tulder, M.; Koes, B.W. Clinical practice guidelines for the management of non-specific low back pain in primary care: An updated overview. Eur. Spine J. 2018, 27, 2791–2803. [Google Scholar] [CrossRef]
- Bouwmeester, W.; van Enst, A.; van Tulder, M. Quality of low back pain guidelines improved. Spine 2009, 34, 2562–2567. [Google Scholar] [CrossRef] [PubMed]
- Koes, B.W.; van Tulder, M.; Lin, C.W.; Macedo, L.G.; McAuley, J.; Maher, C. An updated overview of clinical guide-lines for the management of non-specific low back pain in primary care. Eur. Spine J. 2010, 19, 2075–2094. [Google Scholar] [CrossRef] [PubMed]
- Koes, B.W.; van Tulder, M.W.; Ostelo, R.; Kim Burton, A.; Waddell, G. Clinical guidelines for the management of low back pain in primary care: An international comparison. Spine 2001, 26, 2504–2513. [Google Scholar] [CrossRef]
- Pillastrini, P.; Gardenghi, I.; Bonetti, F.; Capra, F.; Guccione, A.; Mugnai, R.; Violante, F.S. An updated overview of clinical guidelines for chronic low back pain management in primary care. Jt. Bone Spine 2012, 79, 176–185. [Google Scholar] [CrossRef]
- Meroni, R.; Piscitelli, D.; Ravasio, C.; Vanti, C.; Bertozzi, L.; de Vito, G.; Perin, C.; Guccione, A.A.; Cerri, C.G.; Pillastrini, P. Evidence for managing chronic low back pain in primary care: A re-view of recommendations from high-quality clinical practice guidelines. Disabil. Rehabil. 2021, 43, 1029–1043. [Google Scholar] [CrossRef]
- The AGREE Next Steps Consortium. Appraisal of Guidelines for Research & Evaluation (AGREE) II Manual. 2009. Available online: http://www.agreetrust.org/wp-content/uploads/2013/06/AGREE_II_Users_Manual_and_23-item_Instrument_ENGLISH.pdf (accessed on 14 May 2009).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Ripple, A.S. Expert googling: Best practices and advanced strategies for using google in health sciences li-braries. Med. Ref. Serv. Q. 2006, 25, 97–107. [Google Scholar] [CrossRef]
- Brouwers, M.C.; Kho, M.; Browman, G.P.; Burgers, J.S.; Cluzeau, F.; Feder, G.; Fervers, B.; Graham, I.D.; Grimshaw, J.; Hanna, S.E.; et al. AGREE II: Advancing guideline development, reporting and evaluation in health care. Can. Med. Assoc. J. 2010, 182, E839–E842. [Google Scholar] [CrossRef]
- Uzeloto, J.S.; Moseley, A.M.; Elkins, M.R.; Franco, M.R.; Pinto, R.Z.; Freire, A.P.C.F.; Ramos, E.M.C. The quality of clinical practice guidelines for chronic respiratory diseases and the reliability of the AGREE II: An observational study. Physiotherapy 2017, 103, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Zens, T.J.; Cartmill, R.; Muldowney, B.L.; Fernandes-Taylor, S.; Nichol, P.; Kohler, J.E. Practice Variation in Umbili-cal Hernia Repair Demonstrates a Need for Best Practice Guidelines. J. Pediatr. 2019, 206, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Cicchetti, D.V. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol. Assess. 1994, 6, 284. [Google Scholar] [CrossRef]
- Yan, J.; Min, J.; Zhou, B. Diagnosis of pheochromocytoma: A clinical practice guideline appraisal using AGREE II instrument. J. Eval. Clin. Pract. 2012, 19, 626–632. [Google Scholar] [CrossRef] [PubMed]
- Lin, I.; Wiles, L.; Waller, R.; Goucke, R.; Nagree, Y.; Gibberd, M.; Straker, L.; Maher, C.G.; O’Sullivan, P.P.B. What does best practice care for musculoskeletal pain look like? Eleven consistent recommendations from high-quality clinical practice guidelines: Systematic review. Br. J. Sports Med. 2020, 54, 79–86. [Google Scholar] [CrossRef] [PubMed]
- American College of Occupational and Environmental Medicine. Low Back Disorders; Reed Group Ltd.: Broomfield, CO, USA, 2016. [Google Scholar]
- Chou, R.; Qaseem, A.; Owens, D.K.; Shekelle, P. Diagnostic Imaging for Low Back Pain: Advice for High-Value Health Care From the American College of Physicians. Ann. Intern. Med. 2011, 154, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Chou, R.; Qaseem, A.; Snow, V.; Casey, D.; Cross, J.T., Jr.; Shekelle, P.; Owens, D.K. Diagnosis and treatment of low back pain: A joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann. Intern. Med. 2007, 147, 478–491. [Google Scholar] [CrossRef]
- Patel, N.D.; Broderick, D.F.; Burns, J.; Deshmukh, T.K.; Fries, I.B.; Harvey, H.B.; Holly, L.; Hunt, C.H.; Jagadeesan, B.D.; Kennedy, T.A.; et al. ACR Appropriateness Criteria Low Back Pain. J. Am. Coll. Radiol. 2016, 13, 1069–1078. [Google Scholar] [CrossRef]
- Chou, R.; Loeser, J.D.; Owens, D.K.; Rosenquist, R.W.; Atlas, S.J.; Baisden, J.; Carragee, E.J.; Grabois, M.; Murphy, D.R.; Resnick, D.K.; et al. Interventional Therapies, Surgery, and Interdisciplinary Rehabilitation for Low Back Pain. Spine 2009, 34, 1066–1077. [Google Scholar] [CrossRef]
- Delitto, A.; George, S.Z.; Van Dillen, L.; Whitman, J.M.; Sowa, G.; Shekelle, P.; Denninger, T.R.; Godges, J.J. Low back pain. J. Orthop. Sports Phys. Ther. 2012, 42, A1–A57. [Google Scholar] [CrossRef]
- Manchikanti, L.; Abdi, S.; Atluri, S.; Benyamin, R.M.; Boswell, M.V.; Buenaventura, R.M.; Bryce, D.A.; Burks, P.A.; Caraway, D.L.; Calodney, A.K.; et al. An update of comprehensive evidence-based guidelines for interven-tional techniques in chronic spinal pain. Part II: Guidance and recommendations. Pain Physician 2013, 16, S49–S283. [Google Scholar] [PubMed]
- Bussières, A.E.; Stewart, G.; Al-Zoubi, F.; Decina, P.; Descarreaux, M.; Haskett, D.; Hincapié, C.; Pagé, I.; Passmore, S.; Srbely, J.; et al. Spinal manipulative therapy and other conservative treatments for low back pain: A guideline from the Canadian Chiropractic Guideline Initiative [with consumer summary]. J. Manip. Physiol. Ther. 2018, 41, 265–293. [Google Scholar] [CrossRef] [PubMed]
- Colorado Division of Workers Compensation USDoH, Human Services PHSAfHR, Quality. Low Back Pain–Medical Treatment Guidelines. 2014. Available online: https://www.colorado.gov/pacific/sites/default/files/Rule_XVII_Exhibit_A.pdf (accessed on 10 March 2014).
- Airaksinen, O.; Brox, J.I.; Cedraschi, C.; Hildebrandt, J.; Klaber-Moffett, J.; Kovacs, F.; Mannion, A.F.; Reis, S.; Staal, J.B.; Ursin, H.; et al. European guidelines for the management of chronic non-specific low back pain [with consumer summary]. Eur. Spine J. 2006, 15, S192–S300. [Google Scholar] [CrossRef] [PubMed]
- Thorson, D.; Campbell, R.; Massey, M.; Mueller, B.; McCathie, B.; Richards, H.; Peterson, S.; Kramer, C.; Ginkel, T.; Dvorkin, J.; et al. Adult Acute and Subacute Low Back Pain, 16th ed.; Institute for Clinical Systems Improvement (ICSI): Bloomington, MN, USA, 2018. [Google Scholar]
- Negrini, S.; Giovannoni, S.; Minozzi, S.; Barneschi, G.; Bonaiuti, D.; Bussotti, A.; D’Arienzo, M.; Di Lorenzo, N.; Mannoni, A.; Mattioli, S.; et al. Diagnostic therapeutic flow-charts for low back pain patients: The Italian clinical guidelines. Eur. Med. 2006, 42, 151–170. [Google Scholar]
- van Wambeke, P.; Desomer, A.; Ailliet, L.; Berquin, A.; Demoulin, C.; Depreitere, B.; Dewachter, J.; Dolphens, M.; Forget, P.; Fraselle, V.; et al. Low Back Pain and Radicular Pain: Evaluation and Management; Good Clinical Practice (GCP), KCE Reports 287. D/2017/10.273/36; Belgian Health Care Knowledge Centre (KCE): Brussels, Belgium, 2017. [Google Scholar]
- Jun, J.H.; Cha, Y.; Lee, J.A.; Choi, J.; Choi, T.-Y.; Park, W.; Chung, W.; Shin, B.-C.; Lee, M.S. Korean medicine clinical practice guideline for lumbar herniated intervertebral disc in adults: An evidence based approach. Eur. J. Integr. Med. 2017, 9, 18–26. [Google Scholar] [CrossRef]
- Kreiner, D.S.; Hwang, S.W.; Easa, J.E.; Resnick, D.K.; Baisden, J.L.; Bess, S.; Cho, C.H.; DePalma, M.J.; Dougherty, P.; Fernand, R.; et al. An evidence-based clinical guideline for the diagnosis and treatment of lumbar disc herniation with radiculopathy. Spine J. 2014, 14, 180–191. [Google Scholar] [CrossRef] [PubMed]
- Danish Health Authority. National Clinical Guideline for the Nonsurgical Treatment of Recent Onset Lumbar Nerve Root Compression (Lumbar Radiculopathy). 2016. Available online: https://www.sst.dk/da/udgivelser/2016/~/media/B9D3E068233A4F7E95F7A1492EBC4484.ashx (accessed on 6 June 2016).
- Laerum, E.; Dullerud, R.; Kirkesola, G.; Nygaard, Ø.P.; Skouen, J.S.; Stig, L.-C.; Werner, E. The Norwegian Back Pain Network. Acute Low Back Pain: Interdisciplinary Clinical Guidelines. 2007. Available online: https://chiro.org/Low_Back_Pain/FULL/Acute_Low_Back_Pain_Interdisciplinary.pdf (accessed on 20 June 2016).
- Nederlands Huisartsen Genootschap Workgroup. Standaard Lumbosacraal Radiculair Syndroom. 2015. Available online: https://www.henw.org/artikelen/nhg-standaard-lumbosacraal-radiculair-syndroom-tweede-herziening (accessed on 6 September 2018).
- UK NGC. Evidence Review for Pharmacological Management of Sciatica: Low Back Pain and Sciatica in over 16s: Assessment and Management: Evidence Review A. 2020. Available online: https://pubmed.ncbi.nlm.nih.gov/33090751/ (accessed on 20 March 2021).
- Philippine Academy of Rehabilitation Medicine. Clinical Practice Guidelines on the Diagnosis and Management of Low Back. 2011. Available online: http://www.ncbi.nlm.nih.gov/books/nbk562934/ (accessed on 7 February 2021).
- Low Back Pain Working Group Toward Optimized Practice. Evidence-Informed Primary Care Management of Low Back Pain. 2017. Available online: https://parm.org.ph/pdf/lbp.pdf (accessed on 20 January 2021).
- The University of Michigan Health System. Acute Low Back Pain. 2010. Available online: http://www.med.umich.edu/1info/FHP/practiceguides/back/back.pdf (accessed on 9 October 2020).
- Treatment of Low Back Pain Work Group Department of Veterans Affairs DoD. VA/DoD clinical practice guideline for diagnosis and treatment of low back pain (version 2.0). J. Gen. Intern. Med. 2019, 34, 2620–2629. [Google Scholar] [CrossRef]
- Doniselli, F.M.; Zanardo, M.; Manfrè, L.; Papini, G.D.E.; Rovira, A.; Sardanelli, F.; Sconfienza, L.C.; Arana, E. A critical appraisal of the quality of low back pain practice guide-lines using the AGREE II tool and comparison with previous evaluations: A EuroAIM initiative. Eur. Spine J. 2018, 27, 2781–2790. [Google Scholar] [CrossRef] [PubMed]
- Schünemann, H.J.; Wiercioch, W.; Brozek, J.; Etxeandia-Ikobaltzeta, I.; Mustafa, R.A.; Manja, V.; Brignardello-Petersen, R.; Neumann, I.; Falavigna, M.; Alhazzani, W.; et al. GRADE Evidence to Decision (EtD) frameworks for adoption, adaptation, and de novo development of trustworthy recommendations: GRADE-ADOLOPMENT. J. Clin. Epidemiol. 2017, 81, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Harstall, C.; Taenzer, P.; Angus, D.K.; Moga, C.; Schuller, T.; Scott, N.A. Creating a multidisciplinary low back pain guideline: Anatomy of a guideline adaptation process. J. Eval. Clin. Pract. 2011, 17, 693–704. [Google Scholar] [CrossRef] [PubMed]
- van der Windt, D.A.; Simons, E.; Riphagen, I.I.; Ammendolia, C.; Verhagen, A.P.; Laslett, M.; Devillé, W.; Deyo, R.A.; Bouter, L.M.; de Vet, H.C.; et al. Physical examination for lumbar radiculopathy due to disc herniation in patients with low-back pain. Cochrane Database Syst. Rev. 2010, CD007431. [Google Scholar] [CrossRef] [PubMed]
- Majlesi, J.; Togay, H.; Ünalan, H.; Toprak, S. The Sensitivity and Specificity of the Slump and the Straight Leg Raising Tests in Patients With Lumbar Disc Herniation. JCR J. Clin. Rheumatol. 2008, 14, 87–91. [Google Scholar] [CrossRef]
- Ostelo, R.W. Physiotherapy management of sciatica. J. Physiother. 2020, 66, 83–88. [Google Scholar] [CrossRef]
- Pinto, R.Z.; Verwoerd, A.J.H.; Koes, B.W. Which pain medications are effective for sciatica (radicular leg pain)? BMJ 2017, 359, j4248. [Google Scholar] [CrossRef] [PubMed]
- Williams, C.M.; Maher, C.G.; Latimer, J.; McLachlan, A.; Hancock, M.J.; O Day, R.; Lin, C.-W.C. Efficacy of paracetamol for acute low-back pain: A double-blind, randomised controlled trial. Lancet 2014, 384, 1586–1596. [Google Scholar] [CrossRef]
- Rasmussen-Barr, E.; Held, U.; Grooten, W.J.; Roelofs, P.D.; Koes, B.W.; Van Tulder, M.W.; Wertli, M. Non-steroidal anti-inflammatory drugs for sciatica. Cochrane Database Syst. Rev. 2016, 10, CD012382. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, C.B.; Maher, C.G.; Ferreira, M.L.; Hancock, M.J.; Oliveira, V.C.; McLachlan, A.J.; Koes, B.W.; Ferreira, P.H.; Cohen, S.P.; Pinto, R.Z. Epidural corticosteroid injections for lumbosacral radicular pain. Cochrane Database Syst. Rev. 2020, CD013577. [Google Scholar] [CrossRef] [PubMed]
- Shallwani, S.M.; King, J.; Thomas, R.; Thevenot, O.; De Angelis, G.; Aburub, A.S.; Brosseau, L. Methodological quality of clinical practice guidelines with physical ac-tivity recommendations for people diagnosed with cancer: A systematic critical appraisal using the AGREE II tool. PLoS ONE 2019, 14, e0214846. [Google Scholar] [CrossRef]
- Smith, C.A.M.; Toupin-April, K.; Jutai, J.W.; Duffy, C.M.; Rahman, P.; Cavallo, S.; Brosseau, L. A Systematic Critical Appraisal of Clinical Practice Guidelines in Juvenile Idiopathic Arthritis Using the Appraisal of Guidelines for Research and Evaluation II (AGREE II) Instrument. PLoS ONE 2015, 10, e0137180. [Google Scholar] [CrossRef]
- Brosseau, L.; Rahman, P.; Toupin-April, K.; Poitras, S.; King, J.; De Angelis, G.; Loew, L.; Casimiro, L.; Paterson, G.; McEwan, J. A systematic critical appraisal for non-pharmacological management of osteoarthritis using the appraisal of guidelines research and evalua-tion II instrument. PLoS ONE 2014, 9, e82986. [Google Scholar]

| Title Guideline | Year | Country | Professional Bodies/ Abbreviation |
|---|---|---|---|
| Low back disorders | 2016 | USA | American College of Occupational and Environmental Medicine (ACOEM [28]) |
| Diagnostic Imaging for Low Back Pain: Advice for High-Value Health Care From the American College of Physicians | 2011 | USA | American College of Physicians (ACP [29]) |
| Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society | 2007 | USA | American College of Physicians and the American Pain Society (ACP-APS [30]) |
| ACR Appropriateness Criteria Low Back Pain | 2016 | USA | American College of Radiology (ACR [31]) |
| Interventional Therapies, Surgery, and Interdisciplinary Rehabilitation for Low Back Pain | 2009 | USA | American Pain Society (APS [32]) |
| Low Back Pain: Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability, and Health from the Orthopedic Section of the American Physical Therapy Association | 2012 | USA | Orthopedic Section of the American Physical Therapy Association (APTA [33]) |
| An Update of Comprehensive Evidence-Based Guidelines for Interventional Techniques in Chronic Spinal Pain. Part II: Guidance and Recommendations | 2013 | USA | American Society of Interventional Pain Physicians (ASIPP [34]) |
| Spinal Manipulative Therapy and Other Conservative Treatments for Low Back Pain: A Guideline From the Canadian Chiropractic Guideline Initiative | 2018 | Canada | Canadian Chiropractic Guideline Initiative (CCGI [35]) |
| Low Back Pain medical Treatment Guidelines | 2014 | USA | Department of Labor and Employment, Division of Worker’s Compensation (DLE-DWC [36]) |
| European guidelines for the management of chronic non-specific low back pain | 2004 | Europe | European Commission, Research Directorate-General, department of Policy, Coordination and Strategy (EG [37]) |
| Adult Acute and Subacute Low Back Pain Diagnosis Algorithm | 2018 | USA | Institute for Clinical Systems Improvement (ICSI [38]) |
| Diagnostic therapeutic flow-charts for low back pain patients: the Italian clinical guideline | 2006 | Italy | Italian Health Ministry-Care and Research Institute Fondazione Don Carlo Gnocchi ONLUS of Milan (IHM [39]) |
| Low back pain and radicular pain: assessment and management | 2017 | Belgian | Belgian Health Care Knowledge Center (KCE [40]) |
| Korean medicine clinical practice guideline for lumbar herniated intervertebral disc in adults | 2017 | Korea | The Korea Institute of Oriental Medicine (KIOM [41]) |
| Clinical Guideline for the Diagnosis and Treatment of Lumbar Disc Herniation with Radiculopathy | 2012 | USA | North American Spine Society (NASS [42]) |
| National Clinical Guideline: interventions for recent onset lumbar radiculopathy | 2016 | Denmark | National Board of Health (Denmark) (NBHD [43]) |
| Acute low back pain Interdisciplinary clinical guidelines | 2007 | Norway | The Norwegian Back Pain Network and an interdisciplinary working group (NBPN [44]) |
| NHG-Standaard Lumbosacraal radiculair syndroom | 2015 | Netherlands | Dutch General Practitioners Society (NHG [45]) |
| Low back pain and sciatica in over 16s: assessment and management | 2016 | UK | National Institute for Health and Care Excellence (NICE [46]) |
| Clinical Practice Guidelines on the Diagnosis and Management of LBP | 2011 | Philippines | Philippine Academy of Rehabilitation Medicine PARM [47]) |
| Evidence-Informed Primary Care Management of Low Back Pain | 2015 | Canada | Institute of Health Economics Toward Optimized Practice (TOP [48]) |
| Acute Low Back Pain | 2010 | USA | The University of Michigan Health System (UMHS [49]) |
| VA/Do clinical practice guideline for diagnosis and treatment of low back pain | 2017 | USA | Department of Veterans Affairs and Department of Defense (Va/Dod [50]) |
| Guideline | AGREE Domains | |||||||
|---|---|---|---|---|---|---|---|---|
| Guideline * | Scope and Purpose, % | Stakeholder Involvement, % | Rigor of Development, % | Clarity of Presentation, % | Applicability, % | Editorial Independence, % | Overall Assessment, % | Quality |
| ACOEM | 58 | 44 | 50 | 100 | 23 | 92 | 61 | Low |
| ACP | 86 | 36 | 11 | 83 | 46 | 100 | 60 | Average |
| ACP-APS | 97 | 47 | 76 | 94 | 46 | 96 | 76 | Average |
| ACR | 14 | 17 | 81 | 67 | 0 | 17 | 33 | Low |
| APS | 100 | 67 | 94 | 94 | 60 | 96 | 85 | High |
| APTA | 81 | 47 | 72 | 89 | 0 | 0 | 48 | Average |
| ASIPP | 83 | 64 | 72 | 67 | 29 | 96 | 68 | High |
| CCGI | 92 | 72 | 74 | 58 | 33 | 67 | 66 | Average |
| DLE-DWC | 17 | 11 | 0 | 72 | 2 | 0 | 17 | Low |
| EG | 72 | 64 | 70 | 92 | 33 | 38 | 61 | Average |
| ICSI | 83 | 69 | 76 | 92 | 60 | 92 | 79 | High |
| IHM | 61 | 58 | 68 | 83 | 50 | 25 | 58 | Average |
| KCE | 97 | 75 | 88 | 86 | 77 | 100 | 87 | High |
| KIOM | 78 | 28 | 76 | 81 | 6 | 83 | 59 | Average |
| NASS | 83 | 61 | 75 | 78 | 17 | 92 | 68 | High |
| NBHD | 86 | 47 | 91 | 97 | 60 | 96 | 80 | High |
| NBPN | 89 | 83 | 83 | 94 | 29 | 100 | 80 | High |
| NHG | 83 | 56 | 58 | 89 | 25 | 33 | 57 | Low |
| NICE | 97 | 94 | 95 | 97 | 71 | 100 | 92 | High |
| PRAM | 72 | 25 | 31 | 81 | 38 | 0 | 41 | Low |
| TOP | 94 | 78 | 84 | 94 | 73 | 96 | 87 | High |
| UMHS | 56 | 25 | 57 | 94 | 6 | 92 | 55 | Low |
| VA/Dod | 94 | 92 | 77 | 83 | 44 | 67 | 76 | High |
| Mean | 77 | 55 | 68 | 85 | 36 | 69 | 65 | |
| Domain | ICC * (95% CI) |
|---|---|
| Scope and purpose | 0.847 (0.631 to 0.936) |
| Stakeholder involvement | 0.820 (0.2563 to 0.926) |
| Rigor of development | 0.858 (0.636 to 0.943) |
| Clarity of presentation | 0.549 (-0.044 to 0.811) |
| Applicability | 0.874 (0.695 to 0.948) |
| Editorial independence | 0.901 (0.762 to 0.959) |
| Overall rating | 0.785 (0.493 to 0.910) |
| Physical Examination | Guideline * | Consistency | Clinical Inference |
|---|---|---|---|
| Femoral stretch test | NASS | Inconsistent | None |
| NBPN | |||
| PARM | |||
| Straight leg test | NASS | Consistent | Should do |
| PARM | |||
| IHM | |||
| NHG | |||
| ACP-APS | |||
| NBPN | |||
| Crossed straight leg test | NASS | Consistent | Should do |
| PARM | |||
| IHM | |||
| NHG | |||
| NBPN | |||
| Muscle testing | NASS | Common/consistent | Should/Could do |
| PARM | |||
| IHM | |||
| NHG | |||
| ACP-APS | |||
| NBPN | |||
| Sensory testing | NASS | Common | Could do |
| PARM | |||
| IHM | |||
| ACP-APS | |||
| NBPN | |||
| Reflex tests (ankle and knee tendon) | PARM | Inconsistent | None |
| NBPN | |||
| ACP-APS | |||
| NASS | |||
| Mapping pain distribution | PARM | Consistent | Should do |
| IHM | |||
| Slump test | PARM | Inconsistent | None |
| NASS | |||
| Wasserman test | PARM | Consistent | Could do |
| IHM | |||
| Gait | PARM | Consistent | Should do |
| IHM | |||
| Agreement of signs and symptoms | PARM | Consistent | Should do |
| IHM | |||
| Diagnostics | |||
| Imaging | |||
| Routinely offering imaging in primary care or absent of red flags | KCE ICSI NICE ACOEM CCGI ACR NBPN | Consistent | Do not do |
| Computed Tomography (CT)/ Magnetic resonance imaging (MRI) routinely in first 4–6 weeks | ICSI | Consistent | Do not do |
| ACOEM | |||
| NHG | |||
| PRSM | |||
| IHM NBPN | |||
| CT when history and physical examination findings consistent with disc herniation, after 4–6 weeks of low back pain if surgery is considered, severe or progressive neurologic signs and symptoms present | NASS VA/Dod TOP PRAM ACOEM IHM ACP-APS NBPN ACR | Consistent | Should do |
| MRI when history and physical examination findings consistent with disc herniation, radiculopathy persists after six weeks, if surgery is considered, severe or progressive neurologic signs and symptoms present, where an epidural glucocorticosteroid injection is being considered | NASS VA/DoD TOP NBHD EG PRAM ACOEM IHM ACP-APS UMHS NBPN ACR ACP | Common | Should do |
| Others | |||
| EMG | EG PRAM ACOEM IHM UMHS | Inconsistent | None |
| Sensory nerve somatosensory evoked potentials (SEP) | NASS DLE-DWC | Inconsistent | None |
| Discography | ACOEM | Inconsistent | None |
| DLE-DWC | |||
| Diagnostic medial branch block | APS | Inconsistent | None |
| ACOEM |
| Non-Invasive Interventions | Guideline * | Consistency | Clinical Inference |
|---|---|---|---|
| Bed rest | ACOEM | Inconsistent | None |
| PARM | |||
| IHM | |||
| NHG | |||
| NBPN | |||
| Physical activity | NBHD | Common | Should do |
| PARM | |||
| IHM | |||
| ACP-APS | |||
| NICE | |||
| NHG | |||
| NBPN | |||
| Educational care | NICE | Consistent | Should do |
| ICSI | |||
| NHG | |||
| ACP-APS NBPN | |||
| Multidisciplinary approach/rehabilitation program/Psychological therapy | NICE | Common | Could do |
| KCE | |||
| UMHS | |||
| NBPN | |||
| Alternative medicine | |||
| Acupuncture | ICSI | Inconsistent | None |
| PARM | |||
| ACOEM | |||
| IHM | |||
| NICE | |||
| KIOM NBPN | |||
| Manual therapies | |||
| Traction | NASS | Inconsistent | None |
| KCE | |||
| PRAM | |||
| ACOEM | |||
| DLE-DWC | |||
| NICE | |||
| NBPN | |||
| APTA | |||
| Manipulation/mobilisation/soft-tissue techniques | NASS | Inconsistent | None |
| KCE | |||
| ICSI | |||
| NBHD | |||
| PARM | |||
| ACOEM | |||
| DLE-DWC | |||
| IHM | |||
| NICE | |||
| NHG | |||
| CCGI | |||
| NBPN | |||
| APTA | |||
| Massage | PRAM | Inconsistent | None |
| ACOEM | |||
| IHM NBPN | |||
| Devices | NICE | Consistent | Do not do |
| (e.g., belts, corset, foot orthotics etc.) | KCE | ||
| ACOEM | |||
| NBPN | |||
| Exercise/physical therapies | NASS | Consistent | Could do |
| KCE | |||
| ACOEM | |||
| NBHD | |||
| CCGI | |||
| NBPN | |||
| APTA | |||
| Electrotherapies | |||
| TENS/PENS/interferential therapy | NICE | Consistent | Do not do |
| KCE | |||
| PRAM | |||
| ACOEM | |||
| IHM NBPN | |||
| Therapeutic ultrasound | KCE | Inconsistent | None |
| PARM | |||
| NICE | |||
| Heat/cold/infrared therapies | ICSI | Inconsistent | None |
| PRAM | |||
| UMHS | |||
| ACOEM | |||
| Pharmacological interventions | |||
| Paracetamol | KCE | Inconsistent | None |
| PARM | |||
| ACOEM | |||
| IHM | |||
| UMHS | |||
| NHG | |||
| NBPN | |||
| Non-steroidal anti-inflammatory drugs (NSAIDs) | KCE | Inconsistent | None |
| ICSI | |||
| PARM | |||
| ACOEM | |||
| IHM | |||
| NHG | |||
| NBPN | |||
| Opioids | NICE | Inconsistent | None |
| KCE | |||
| PARM | |||
| IHM | |||
| NHG NBPN | |||
| Paracetamol + opioids | IHM | Inconsistent | None |
| NHG | |||
| NBPN | |||
| Anti-epilepticum | KCE | Inconsistent | None |
| VA/Dod | |||
| PARM | |||
| ACOEM | |||
| NASS | |||
| NICE | |||
| NHG | |||
| Muscle relaxants | KCE | Inconsistent | None |
| ICSI | |||
| PARM | |||
| ACOEM | |||
| IHM | |||
| NHG | |||
| NBPN | |||
| Antidepressants | NASS | Inconsistent | None |
| NICE | |||
| KCE | |||
| ACOEM | |||
| NHG | |||
| Corticosteroids | VA/Dod | Inconsistent | None |
| PARM | |||
| ACOEM | |||
| DLE-DWC | |||
| NHG | |||
| ACP-APS | |||
| Antibiotics | KCE | Inconsistent | None |
| ACOEM | |||
| Cannabis | NICE | Consistent | Do not do |
| NHG | |||
| Invasive Treatments | |||
| Surgery | NASS | Common | Could do |
| APS | |||
| NHG | |||
| DLE-DWC | |||
| IHM | |||
| ACOEM NBPN | |||
| Injection therapies | |||
| Epidural injections | NICE | Inconsistent | None |
| NASS | |||
| KCE | |||
| VA/Dod | |||
| ICSI | |||
| NBHD | |||
| PRAM | |||
| ACOEM | |||
| ACP | |||
| NHG | |||
| NBPN | |||
| APS | |||
| Referral | PRAM | Consistent | Should do |
| IHM | |||
| NHG |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khorami, A.K.; Oliveira, C.B.; Maher, C.G.; Bindels, P.J.E.; Machado, G.C.; Pinto, R.Z.; Koes, B.W.; Chiarotto, A. Recommendations for Diagnosis and Treatment of Lumbosacral Radicular Pain: A Systematic Review of Clinical Practice Guidelines. J. Clin. Med. 2021, 10, 2482. https://doi.org/10.3390/jcm10112482
Khorami AK, Oliveira CB, Maher CG, Bindels PJE, Machado GC, Pinto RZ, Koes BW, Chiarotto A. Recommendations for Diagnosis and Treatment of Lumbosacral Radicular Pain: A Systematic Review of Clinical Practice Guidelines. Journal of Clinical Medicine. 2021; 10(11):2482. https://doi.org/10.3390/jcm10112482
Chicago/Turabian StyleKhorami, Ahmad Khoshal, Crystian B. Oliveira, Christopher G. Maher, Patrick J. E. Bindels, Gustavo C. Machado, Rafael Z. Pinto, Bart W. Koes, and Alessandro Chiarotto. 2021. "Recommendations for Diagnosis and Treatment of Lumbosacral Radicular Pain: A Systematic Review of Clinical Practice Guidelines" Journal of Clinical Medicine 10, no. 11: 2482. https://doi.org/10.3390/jcm10112482
APA StyleKhorami, A. K., Oliveira, C. B., Maher, C. G., Bindels, P. J. E., Machado, G. C., Pinto, R. Z., Koes, B. W., & Chiarotto, A. (2021). Recommendations for Diagnosis and Treatment of Lumbosacral Radicular Pain: A Systematic Review of Clinical Practice Guidelines. Journal of Clinical Medicine, 10(11), 2482. https://doi.org/10.3390/jcm10112482