
Assessment of Lymph Node Involvement with PET-CT in Advanced Epithelial Ovarian Cancer. A FRANCOGYN Group Study

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Main Objective and Main Outcome Measure
2.3. Inclusion Criteria
2.4. Collected Data
2.5. Statistical Analysis
3. Results
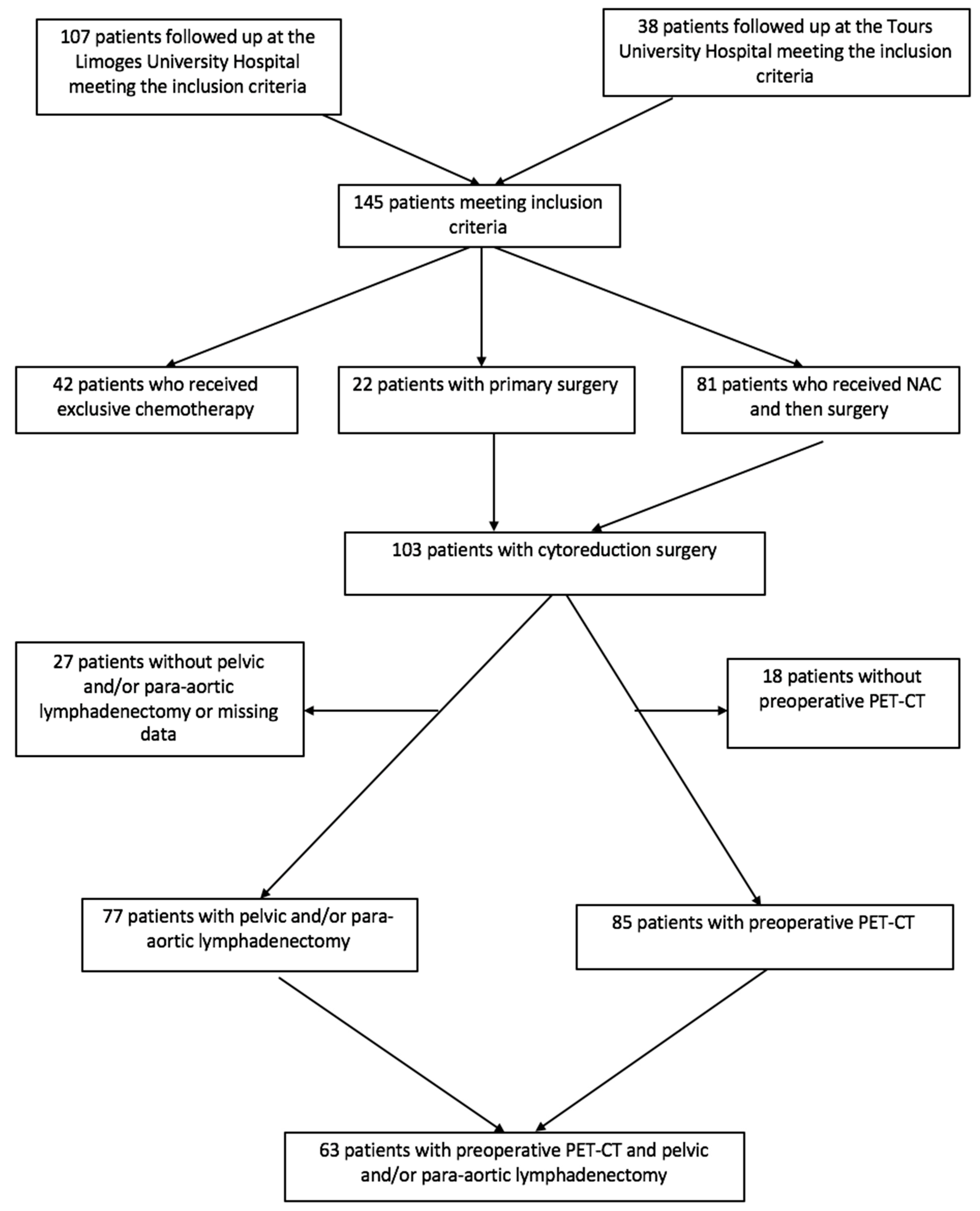
3.1. Population
3.2. FIGO Stage
3.3. Treatment
3.4. PET-CT Performance
4. Discussion
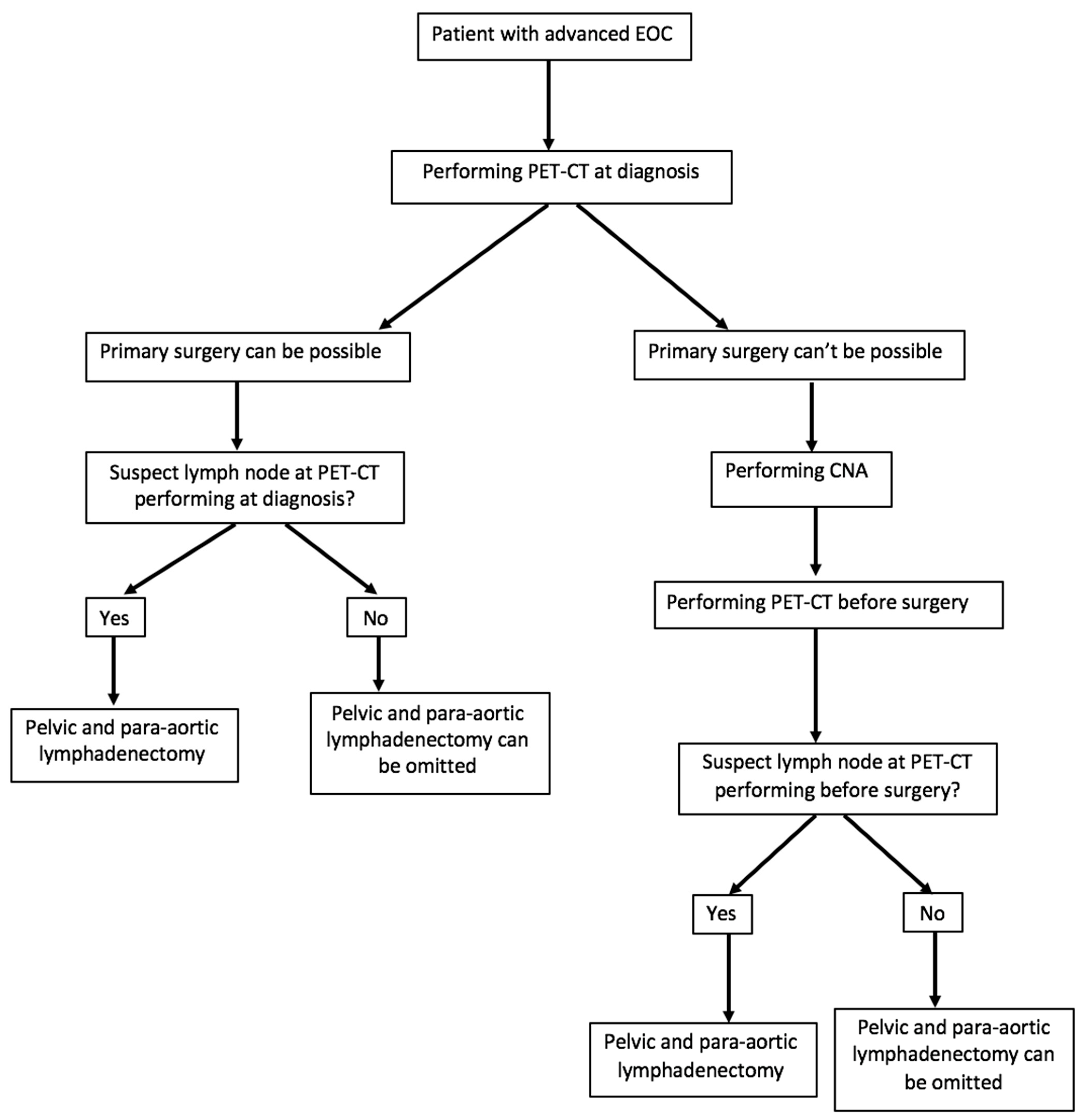
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Ferron, G.; Narducci, F.; Pouget, N.; Touboul, C. [Surgery for advanced stage ovarian cancer: Article drafted from the French Guidelines in oncology entitled «Initial management of patients with epithelial ovarian cancer» developed by FRANCOGYN, CNGOF, SFOG, GINECO-ARCAGY under the aegis of CNGOF and endorsed by INCa]. Gynecol. Obstet. Fertil. Senol. 2019, 47, 197–213. [Google Scholar]
- Abe, A.; Furumoto, H.; Irahara, M.; Ino, H.; Kamada, M.; Naka, O.; Sasaki, M.; Kagawa, T.; Okitsu, O.; Kushiki, N. The impact of systematic para-aortic and pelvic lymphadenectomy on survival in patients with optimally debulked ovarian cancer. J. Obstet. Gynaecol. Res. 2010, 36, 1023–1030. [Google Scholar] [CrossRef]
- Bogani, G.; Tagliabue, E.; Ditto, A.; Signorelli, M.; Martinelli, F.; Casarin, J.; Chiappa, V.; Dondi, G.; Maggiore, U.L.R.; Scaffa, C.; et al. Assessing the risk of pelvic and para-aortic nodal involvement in apparent early-stage ovarian cancer: A predictors- and nomogram-based analyses. Gynecol. Oncol. 2017, 147, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Ditto, A.; Martinelli, F.; Reato, C.; Kusamura, S.; Solima, E.; Fontanelli, R.; Haeusler, E.A.; Raspagliesi, F. Systematic para-aortic and pelvic lymphadenectomy in early stage epithelial ovarian cancer: A prospective study. Ann. Surg. Oncol. 2012, 19, 3849–3855. [Google Scholar] [CrossRef] [PubMed]
- Gouy, S.; Saidani, M.; Maulard, A.; Faron, M.; Bach-Hamba, S.; Bentivegna, E.; Leary, A.; Pautier, P.; Devouassoux-Shisheboran, M.; Genestie, C.; et al. Staging surgery in early-stage ovarian mucinous tumors according to expansile and infiltrative types. Gynecol. Oncol. Rep. 2017, 22, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Heintz, A.; Odicino, F.; Maisonneuve, P.; Quinn, M.A.; Benedet, J.L.; Creasman, W.T.; Ngan, H.; Pecorelli, S.; Beller, U. Carcinoma of the ovary. FIGO 26th Annual Report on the Results of Treatment in Gynecological Cancer. Int. J. Gynaecol. Obstet. 2006, 95, S161–S192. [Google Scholar] [CrossRef]
- Ayhan, A.; Gultekin, M.; Çelik, N.Y.; Dursun, P.; Taskiran, C.; Aksan, G.; Yüce, K. Occult metastasis in early ovarian cancers: Risk factors and associated prognosis. Am. J. Obstet. Gynecol. 2007, 196, 81.e1–81.e6. [Google Scholar] [CrossRef]
- Maggioni, A.P.; Panici, P.B.; Dellanna, T.; Landoni, F.; Lissoni, A.; Pellegrino, A.; Rossi, R.; Chiari, S.; Campagnutta, E.; Greggi, S.; et al. Randomised study of systematic lymphadenectomy in patients with epithelial ovarian cancer macroscopically confined to the pelvis. Br. J. Cancer 2006, 95, 699–704. [Google Scholar] [CrossRef]
- Minig, L.; Heitz, F.; Cibula, D.; Bakkum-Gamez, J.N.; Germanova, A.; Dowdy, S.C.; Kalogera, E.; Zapardiel, I.; Lindemann, K.; Harter, P.; et al. Patterns of Lymph Node Metastases in Apparent Stage I Low-Grade Epithelial Ovarian Cancer: A Multicenter Study. Ann. Surg. Oncol. 2017, 24, 2720–2726. [Google Scholar] [CrossRef]
- Muyldermans, K.; Moerman, P.; Amant, F.; Leunen, K.; Neven, P.; Vergote, I. Primary invasive mucinous ovarian carcinoma of the intestinal type: Importance of the expansile versus infiltrative type in predicting recurrence and lymph node metastases. Eur. J. Cancer 2013, 49, 1600–1608. [Google Scholar] [CrossRef]
- Kleppe, M.; Van Der Aa, M.A.; Van Gorp, T.; Slangen, B.F.M.; Kruitwagen, R.F. The impact of lymph node dissection and adjuvant chemotherapy on survival: A nationwide cohort study of patients with clinical early-stage ovarian cancer. Eur. J. Cancer 2016, 66, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Oshita, T.; Itamochi, H.; Nishimura, R.; Numa, F.; Takehara, K.; Hiura, M.; Tanimoto, H.; Noma, J.; Hayase, R.; Murakami, A.; et al. Clinical impact of systematic pelvic and para-aortic lymphadenectomy for pT1 and pT2 ovarian cancer: A retrospective survey by the Sankai Gynecology Study Group. Int. J. Clin. Oncol. 2013, 18, 1107–1113. [Google Scholar] [CrossRef]
- Harter, P.; Heitz, F.; Ataseven, B.; Schneider, S.; Baert, T.; Prader, S.; Du Bois, A. How to manage lymph nodes in ovarian cancer. Cancer 2019, 125, 4573–4577. [Google Scholar] [CrossRef]
- Kemppainen, J.; Hynninen, J.; Virtanen, J.; Seppänen, M. PET/CT for Evaluation of Ovarian Cancer. Semin. Nucl. Med. 2019, 49, 484–492. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Gu, Z.-X.; Tao, X.-F.; Liu, S.-Y. Computer tomography, magnetic resonance imaging, and positron emission tomography or positron emission tomography/computer tomography for detection of metastatic lymph nodes in patients with ovarian cancer: A meta-analysis. Eur. J. Radiol. 2012, 81, 1002–1006. [Google Scholar] [CrossRef] [PubMed]
- Ataseven, B.; Grimm, C.; Harter, P.; Prader, S.; Traut, A.; Heitz, F.; Du Bois, A. Prognostic value of lymph node ratio in patients with advanced epithelial ovarian cancer. Gynecol. Oncol. 2014, 135, 435–440. [Google Scholar] [CrossRef]
- Harter, P.; Sehouli, J.; Lorusso, D.; Reuss, A.; Vergote, I.; Marth, C.; Kim, J.-W.; Raspagliesi, F.; Lampe, B.; Aletti, G.; et al. A Randomized Trial of Lymphadenectomy in Patients with Advanced Ovarian Neoplasms. N. Engl. J. Med. 2019, 380, 822–832. [Google Scholar] [CrossRef] [PubMed]
- Ouldamer, L.; Caille, A.; Giraudeau, B. A lion with only two legs. J. Gynecol. Obstet. Hum. Reprod. 2020, 49, 101686. [Google Scholar] [CrossRef] [PubMed]
- Signorelli, M.; Guerra, L.; Pirovano, C.; Crivellaro, C.; Fruscio, R.; Buda, A.; Cuzzucrea, M.; Elisei, F.; Ceppi, L.; Messa, C. Detection of nodal metastases by 18F-FDG PET/CT in apparent early stage ovarian cancer: A prospective study. Gynecol. Oncol. 2013, 131, 395–399. [Google Scholar] [CrossRef]
- Gouy, S.; Morice, P.; Narducci, F.; Uzan, C.; Gilmore, J.; Kolesnikov-Gauthier, H.; Querleu, D.; Haie-Meder, C.; Leblanc, E. Nodal-staging surgery for locally advanced cervical cancer in the era of PET. Lancet Oncol. 2012, 13, e212–e220. [Google Scholar] [CrossRef]
- Legros, M.; Margueritte, F.; Tardieu, A.; Deluche, E.; Mbou, V.B.; Lacorre, A.; Ceuca, A.; Aubard, Y.; Monteil, J.; Sallee, C.; et al. Para-aortic Lymph Node Invasion in High-risk Endometrial Cancer: Performance of 18FDG PET-CT. Anticancer. Res. 2019, 39, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.-J.; Bristow, R.E. Evolution of surgical treatment paradigms for advanced-stage ovarian cancer: Redefining “optimal“ residual disease. Gynecol. Oncol. 2012, 125, 483–492. [Google Scholar] [CrossRef]
- Michielsen, K.; Vergote, I.; De Beeck, K.O.; Amant, F.; Leunen, K.; Moerman, P.; Deroose, C.; Souverijns, G.; Dymarkowski, S.; De Keyzer, F.; et al. Whole-body MRI with diffusion-weighted sequence for staging of patients with suspected ovarian cancer: A clinical feasibility study in comparison to CT and FDG-PET/CT. Eur. Radiol. 2014, 24, 889–901. [Google Scholar] [CrossRef] [PubMed]
- Kitajima, K.; Murakami, K.; Yamasaki, E.; Kaji, Y.; Fukasawa, I.; Inaba, N.; Sugimura, K. Diagnostic accuracy of integrated FDG-PET/contrast-enhanced CT in staging ovarian cancer: Comparison with enhanced CT. Eur. J. Nucl. Med. Mol. Imaging 2008, 35, 1912–1920. [Google Scholar] [CrossRef] [PubMed]
- Nam, E.J.; Yun, M.J.; Oh, Y.T.; Kim, J.W.; Kim, S.; Jung, Y.W.; Kim, S.W.; Kim, Y.T. Diagnosis and staging of primary ovarian cancer: Correlation between PET/CT, Doppler US, and CT or MRI. Gynecol. Oncol. 2010, 116, 389–394. [Google Scholar] [CrossRef]
- Yoshida, Y.; Kurokawa, T.; Kawahara, K.; Tsuchida, T.; Okazawa, H.; Fujibayashi, Y.; Yonekura, Y.; Kotsuji, F. Incremental benefits of FDG positron emission tomography over CT alone for the preoperative staging of ovarian cancer. Am. J. Roentgenol. 2004, 182, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Grant, P.; Sakellis, C.; Jacene, H.A. Gynecologic oncologic imaging with PET/CT. Semin. Nucl. Med. 2014, 44, 461–478. [Google Scholar] [CrossRef]
- Konishi, H.; Takehara, K.; Kojima, A.; Okame, S.; Yamamoto, Y.; Shiroyama, Y.; Yokoyama, T.; Nogawa, T.; Sugawara, Y. Maximum standardized uptake value of fluorodeoxyglucose positron emission tomography/computed tomography is a prognostic factor in ovarian clear cell adenocarcinoma. Int. J. Gynecol. Cancer 2014, 24, 1190–1194. [Google Scholar] [CrossRef]
- Kitajima, K.; Murakami, K.; Yamasaki, E.; Kaji, Y.; Sugimura, K. Accuracy of integrated FDG-PET/contrast-enhanced CT in detecting pelvic and paraaortic lymph node metastasis in patients with uterine cancer. Eur. Radiol. 2009, 19, 1529–1536. [Google Scholar] [CrossRef]
- Prakash, P.; Cronin, C.G.; Blake, M.A. Role of PET/CT in ovarian cancer. Am. J. Roentgenol. 2010, 194, W464–W470. [Google Scholar] [CrossRef]
- Chantalat, E.; Fabien, V.; Lèguevaque, P.; Lepage, B.; Lambaudie, E.; Hebert, T.; Motton, S. Para-aortic workup in locally advanced cervical cancer: Heterogeneity is still the rule. Results from a retrospective multicenter study. Arch. Gynecol. Obstet. 2016, 293, 1081–1086. [Google Scholar] [CrossRef]
- Martinez, A.; Voglimacci, M.; Lusque, A.; Ducassou, A.; Gladieff, L.; Dupuis, N.; Angeles, M.A.; Le Gac, Y.T.; Chantalat, E.; Hitzel, A.; et al. Tumour and pelvic lymph node metabolic activity on FDG-PET/CT to stratify patients for para-aortic surgical staging in locally advanced cervical cancer. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1252–1260. [Google Scholar] [CrossRef] [PubMed]
- Fagotti, A.; De Iaco, P.; Fanfani, F.; Vizzielli, G.; Perelli, F.; Pozzati, F.; Perrone, A.M.; Turco, L.C.; Scambia, G. Systematic pelvic and aortic lymphadenectomy in advanced ovarian cancer patients at the time of interval debulking surgery: A double-institution case-control study. Ann. Surg. Oncol. 2012, 19, 3522–3527. [Google Scholar] [CrossRef]
- Kitajima, K.; Murakami, K.; Sakamoto, S.; Kaji, Y.; Sugimura, K. Present and future of FDG-PET/CT in ovarian cancer. Ann. Nucl. Med. 2011, 25, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Viswanathan, C.; Bhosale, P.R.; Shah, S.N.; Vikram, R. Positron emission tomography-computed tomography imaging for malignancies in women. Radiol. Clin. N. Am. 2013, 51, 1111–1125. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Demographic Characteristics of Patients | n | % |
|---|---|---|
| Personal history of neoplasia | ||
| Breast | 16 | 11 |
| Other | 7 | 4.8 |
| Missing data | 31 | 21.4 |
| Family history of neoplasia | ||
| Breast | 27 | 18.6 |
| Ovarian | 6 | 4.1 |
| Uterine | 5 | 3.4 |
| Other | 25 | 17.2 |
| Anatomopathology of cancer | ||
| High-grade serous adenocarcinoma | 77 | 53.1 |
| Low-grade serous adenocarcinoma | 11 | 7.6 |
| Mucinous adenocarcinoma | 5 | 3.4 |
| Endometrioid adenocarcinoma | 3 | 2.1 |
| Clear cell adenocarcinoma | 2 | 1.4 |
| Carcinoma | 2 | 1.4 |
| Others | 45 | 31 |
| Survival | ||
| Median recurrence-free survival in months | 28 [1–107] | |
| Median overall survival in months | 61 [1–107] |
| Treatment | n |
|---|---|
| Primary surgery (%) | 22 (15.2 %) |
| NAC (%) | 81 (55.9 %) |
| Mean peritoneal cancer index (standard deviation) [extreme] | 8.3 (± 4.8) [0–18] |
| Lymphadenectomy performed (%) | |
| Yes | 77 (74.8 %) |
| No | 25 (24.3 %) |
| Missing data | 1 (1 %) |
| Pelvic | 75 (72.8 %) |
| Para-aortic | 74 (71.8 %) |
| Average number of lymph nodes harvested | |
| (standard deviation) [extreme] | |
| Pelvic area | 13.2 (± 7) [2–32] |
| Para-aortic area | 21.5 (±1 5) [3–79] |
| Number of patients with positive lymphadenectomy (%) | |
| Total | 36/77 (46.8 %) |
| Pelvic | 24/75 (32 %) |
| Para-aortic | 22/74 (29.7 %) |
| Missing data | 1/77 (1.3 %) |
| Mean number of metastatic lymph nodes (standard deviation) [extreme] | |
| Pelvic | 3.3 (± 2.7) [1–11] |
| Para-aortic | 4.2 (± 4.2) [1–21] |
| n | FN (%) | TN (%) | FP (%) | TP (%) | Se (%) | Sp (%) | PPV (%) | NPV (%) | Accuracy (%) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Global | 63 | 34.9 | 47.6 | 4.8 | 12.7 | 26.7 | 90.9 | 72.7 | 57.7 | 60.3 |
| Before primary surgery | 16 | 25 | 43.8 | 6.3 | 25 | 50 | 87.5 | 80 | 63.6 | 68.8 |
| After NAC | 47 | 38.3 | 48.9 | 4.3 | 8.5 | 18.2 | 92 | 66.7 | 56.1 | 57.5 |
| For pelvic lymph nodes | 63 | 22.6 | 66.1 | 6.5 | 4.8 | 17.6 | 91.1 | 42.9 | 74.5 | 71 |
| For para-aortic lymph nodes | 63 | 21.3 | 65.6 | 1.6 | 11.5 | 35 | 97.6 | 87.5 | 75.5 | 77.1 |
| Study | Staff | FIGO Stage Included | Lymph Nodes Sites | Se (%) | Sp (%) | VPP (%) | VPN (%) | AR (%) |
|---|---|---|---|---|---|---|---|---|
| Our study 2020 | 64 | Advanced | Pelvis + para-aortic | 26.7 | 91.2 | 72.7 | 58.5 | 60.9 |
| Kitajima * [25] 2008 | 40 | Early (50%) + Advanced (50%) | Pelvis | 75 | 100 | NR | NR | 95 |
| Nam * [26] 2010 | 91 | Early (25.2%) + Advanced (74.8%) | Para-aortic Pelvis + para-aortic | 88 83.8 | 94 92.6 | NR 81.6 | NR 93.6 | 93 NR |
| Yoshida * [27] 2004 Michielsen et al. [24] 2014 | 15 22 | Early (33.3%) + Advanced (66.7%) | Pelvis Para-aortic Pelvis + para-aortic | 100 100 77 | 100 100 91 | 100 100 77 | 100 100 91 | 100 100 87 |
| Advanced |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tardieu, A.; Ouldamer, L.; Margueritte, F.; Rossard, L.; Lacorre, A.; Bourdel, N.; Lades, G.; Sallée, C.; Monteil, J.; Gauthier, T. Assessment of Lymph Node Involvement with PET-CT in Advanced Epithelial Ovarian Cancer. A FRANCOGYN Group Study. J. Clin. Med. 2021, 10, 602. https://doi.org/10.3390/jcm10040602
Tardieu A, Ouldamer L, Margueritte F, Rossard L, Lacorre A, Bourdel N, Lades G, Sallée C, Monteil J, Gauthier T. Assessment of Lymph Node Involvement with PET-CT in Advanced Epithelial Ovarian Cancer. A FRANCOGYN Group Study. Journal of Clinical Medicine. 2021; 10(4):602. https://doi.org/10.3390/jcm10040602
Chicago/Turabian StyleTardieu, Antoine, Lobna Ouldamer, François Margueritte, Lauranne Rossard, Aymeline Lacorre, Nicolas Bourdel, Guillaume Lades, Camille Sallée, Jacques Monteil, and Tristan Gauthier. 2021. "Assessment of Lymph Node Involvement with PET-CT in Advanced Epithelial Ovarian Cancer. A FRANCOGYN Group Study" Journal of Clinical Medicine 10, no. 4: 602. https://doi.org/10.3390/jcm10040602
APA StyleTardieu, A., Ouldamer, L., Margueritte, F., Rossard, L., Lacorre, A., Bourdel, N., Lades, G., Sallée, C., Monteil, J., & Gauthier, T. (2021). Assessment of Lymph Node Involvement with PET-CT in Advanced Epithelial Ovarian Cancer. A FRANCOGYN Group Study. Journal of Clinical Medicine, 10(4), 602. https://doi.org/10.3390/jcm10040602