Clinical Impact of Lymphadenectomy after Neoadjuvant Chemotherapy in Advanced Epithelial Ovarian Cancer: A Review of Available Data

 , ,
, ,
Abstract
1. Introduction
2. Method
3. Results
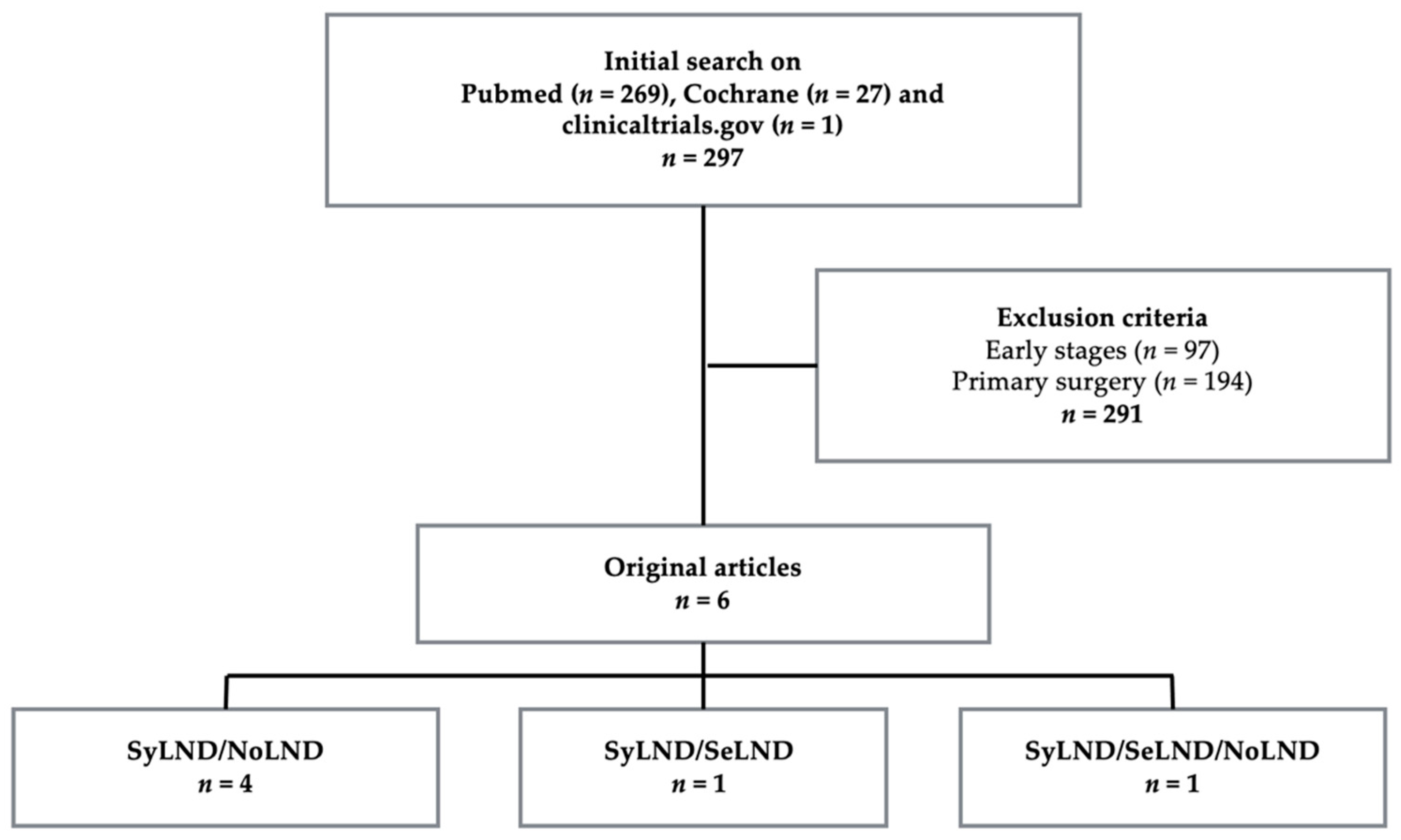
3.1. Study Selection and Characteristics of the Population
- Systematic lymph node dissection (SyLND): systematic pelvic and para-aortic lymph node dissection up to the renal vein.
- Selective lymphadenectomy (SeLND): resection of bulky nodes only or resection of previously known positive lymph nodes, based on pre-operative imaging.
- No lymphadenectomy (NoLND): no lymph node dissection.
3.2. Main Outcomes
3.2.1. Lymph Node Status Assessment
3.2.2. Pathology Results
3.2.3. Oncological Outcomes
Recurrence-Free Survival
Overall Survival
3.3. Secondary Outcomes
4. Discussion
4.1. Metastatic Lymph Node and Its Effect on Outcomes
4.2. Recurrence Occurrence and Location
4.3. Pre-Operative Imaging
4.4. Studies Limitations and Interest of This Review
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harter, P.; Sehouli, J.; Lorusso, D.; Reuss, A.; Vergote, I.; Marth, C.; Kim, J.W.; Raspagliesi, F.; Lampe, B.; Aletti, G.; et al. A Randomized Trial of Lymphadenectomy in Patients with Advanced Ovarian Neoplasms. N. Engl. J. Med. 2019, 380, 822–832. [Google Scholar] [CrossRef] [PubMed]
- Fagotti, A.; Ferrandina, M.G.; Vizzielli, G.; Pasciuto, T.; Fanfani, F.; Gallotta, V.; Margariti, P.A.; Chiantera, V.; Costantini, B.; Alletti, S.G.; et al. Randomized trial of primary debulking surgery versus neoadjuvant chemotherapy for advanced epithelial ovarian cancer (SCORPION-NCT01461850). Int. J. Gynecol. Cancer 2020, 30. [Google Scholar] [CrossRef] [PubMed]
- Jaime, P. FIGO Committee on Gynecologic Oncology. FIGO’s staging classification for cancer of the ovary, fallopian tube, and peritoneum: Abridged republication. J. Gynecol. Oncol. 2015, 26, 87–89. [Google Scholar]
- Fagotti, A.; De Iaco, P.; Fanfani, F.; Vizzielli, G.; Perelli, F.; Pozzati, F.; Perrone, A.M.; Turco, L.C.; Scambia, G. Systematic Pelvic and Aortic Lymphadenectomy in Advanced Ovarian Cancer Patients at the Time of Interval Debulking Surgery: A Double-Institution Case–Control Study. Ann. Surg. Oncol. 2012, 19, 3522–3527. [Google Scholar] [CrossRef] [PubMed]
- Iwase, H.; Takada, T.; Iitsuka, C.; Nomura, H.; Abe, A.; Taniguchi, T.; Takizawa, K. Clinical significance of systematic retroperitoneal lymphadenectomy during interval debulking surgery in advanced ovarian cancer patients. J. Gynecol. Oncol. 2015, 26, 303. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, L.; Schrot-Sanyan, S.; Brigand, C.; Baldauf, J.-J.; Wattiez, A.; Akladios, C. Impact of Pelvic and Para-aortic Lymphadenectomy in Advanced Ovarian Cancer After Neoadjuvant Chemotherapy. Anticancer Res. 2015, 35, 5503–5509. [Google Scholar] [PubMed]
- Eoh, K.J.; Yoon, J.W.; Lee, I.; Lee, J.Y.; Kim, S.; Kim, S.W.; Kim, Y.T.; Nam, E.J. The efficacy of systematic lymph node dissection in advanced epithelial ovarian cancer during interval debulking surgery performed after neoadjuvant chemotherapy. J. Surg. Oncol. 2017, 116, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Song, N.; Gao, Y. Therapeutic value of selective lymphadenectomy in interval debulking surgery for stage IIIc and IV epithelial ovarian cancer. Int. J. Gynecol. Cancer 2019, 29, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Bund, V.; Lecointre, L.; Velten, M.; Ouldamer, L.; Bendifallah, S.; Koskas, M.; Bolze, P.A.; Collinet, P.; Canlorbe, G.; Touboul, C.; et al. Impact of Lymphadenectomy on Survival of Patients with Serous Advanced Ovarian Cancer After Neoadjuvant Chemotherapy: A French National Multicenter Study (FRANCOGYN). J. Clin. Med. 2020, 9, 2427. [Google Scholar] [CrossRef] [PubMed]
- Joulie, F.; Morice, P.; Rey, A.; Thoury, A.; Camatte, S.; Pautier, P.; Lhommé, C.; Haie-Meder, C.; Duvillard, P.; Castaigne, D. Les métastases ganglionnaires du cancer épithélial de l’ovaire sont-elles chimio-sensibles? Étude comparative de la lymphadénectomie première ou après chimiothérapie. Gynécologie Obs. Fertil. 2004, 32, 502–507. [Google Scholar] [CrossRef]
- Di Re, F.; Baiocchi, G. Value of lymph node assessment in ovarian cancer: Status of the art at the end of the second millennium. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2000, 10, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Dell’Anna, T.; Signorelli, M.; Benedetti-Panici, P.; Maggioni, A.; Fossati, R.; Fruscio, R.; Milani, R.; Bocciolone, L.; Buda, A.; Mangioni, C.; et al. Systematic lymphadenectomy in ovarian cancer at second-look surgery: A randomised clinical trial. Br. J. Cancer 2012, 107, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Widschwendter, P.; Blersch, A.; Friedl, T.W.; Janni, W.; Kloth, C.; de Gregorio, A.; de Gregorio, N. CT Scan in the Prediction of Lymph Node Involvement in Ovarian Cancer—A Retrospective Analysis of a Tertiary Gyneco-Oncological Unit. Geburtshilfe Frauenheilkd. 2020, 80, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Azaïs, H.; Canlorbe, G.; Nikpayam, M.; Gonthier, C.; Belghiti, J.; Uzan, C. Are there still indications of lymph node dissection in epithelial ovarian cancers after the LION trial? Bull. Cancer 2019, 107, 707–714. [Google Scholar] [CrossRef] [PubMed]
- Mimoun, C.; Benifla, J.L.; Fauconnier, A.; Huchon, C. Intraoperative Clinical Examination for Assessing Pelvic and Para-Aortic Lymph Node Involvement in Advanced Epithelial Ovarian Cancer: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 2793. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors | Type of LND | Sample Size | Age (Years-Median) or n (%) | FIGO Stage n (%) | Histopathologic Type n (%) | Median Number NACT Cycles | Residual Tumor (cm) n (%) |
|---|---|---|---|---|---|---|---|
| Fagotti [4] | NoLND (9 SeLND) | 101 | 62.0 | III: 81 (80.2) IV:20 (19.8) | Serous: 99 (98.0) Others: 2 (2.0) | 4 | 0: 81 (80.2) <1: 20 (19.8) |
| SyLND | 50 | 62.0 | III: 37 (74.0) IV:13 (26.0) | Serous: 47 (94.0) Others: 3 (6.0) | 6 | 0: 41 (82.0) <1: 9 (18.0) | |
| Iwase [5] | NoLND SyLND | 124 (38 NoLND/86 SyLND) | 58.0 | III: 83 (66.9) IV:41 (33.1) | Serous: 105 (85.0) Others: 19 (15.0) | 6 | 0: 98 (79.0) <1: 15 (12.1) ≥1: 11 (8.9) |
| Schwartz [6] | NoLND | 47 | ≤55: 14 (29.8) 56–69: 22 (46.8) ≥71: 11 (23.4) | III: 27 (57.4) IV: 20 (42.6) | Serous: 38 (82.6) Others: 9 (17.4) | 6 | 0: 47 (100.0) |
| SyLND | 54 | ≤55: 22 (40.8) 56–69: 24 (44.4) ≥71: 8 (14.8) | III: 43 (79.6) IV:11 (20.4) | Serous: 47 (87.0) Others: 7 (13.0) | 5 | 0: 54 (100.0) | |
| Eoh [7] | SeLND | 68 | 60.5 | III: 27 (39.7) IV: 41 (60.3) | Serous: 62 (91.2) Mucinous: 1 (1.5) Endometrioid: 3 (4.4) Clear cells: 2 (2.9) | 3 | 0: 25 (36.8) <1: 43 (63.2) |
| SyLND | 65 | 53.8 | III: 33 (50.8) IV: 32 (49.2) | Serous: 56 (86.2) Mucinous: 0 (0) Endometrioid: 3 (4.6) Clear cells: 4 (6.2) Others: 2 (3.0) | 3 | 0: 22 (33.8) <1: 43 (66.2) | |
| Song [8] | NoLND | 67 | 56.0 | III: 52 (77.6) IV: 15 (22.4) | Serous: 54 (80.6) Others: 13 (19.4) | 3 | 0: 67 (100.0) |
| SeLND | 145 | 54.0 | III: 108 (74.5) IV: 37 (25.5) | Serous: 124 (85.5) Others: 21 (14.5) | 3 | 0: 145 (100.0) | |
| SyLND | 118 | 55.5 | III: 95 (80.5) IV: 23 (19.5) | Serous: 105 (89.0) Others: 13 (11.0) | 3 | 0: 118 (100.0) | |
| Bund [9] | NoLND | 100 | 67.5 | III: 78 (78.0) IV: 22 (22.0) | Serous: 100 (100.0) | NA | 0: 50 (50.0) ≤0.25: 23 (23.0) >0.25: 27 (27.0) |
| SyLND | 155 | 59.0 | III: 127 (81.9) IV: 28 (18.1) | Serous: 100 (100.0) | NA | 0: 137 (88.4) ≤0.25: 9 (5.8) >0.25: 9 (5.8) |
| Authors | Number of Lymph Nodes Retrieved | Metastatic Lymph Node Rate on Pathological Examination | Overall Recurrence Rate | Lymph Node Recurrence Rate |
|---|---|---|---|---|
| Fagotti [4] | 38 (SyLND) | 28% (SyLND) 33% (NoLND) | 70% (SyLND) 62% (NoLND) | no difference |
| Iwase [5] | 46 (SyLND) | 56% | 81% | 20% (SyLND) 29% (NoLND) |
| Schwartz [6] | 26 (SyLND) | 41% | NA | NA |
| Eoh [7] | 27 (SyLND)/10 (SeLND) | 66% (SeLND) 54% (SyLND) | 80% | 11% (SeLND) 6% (SyLND) |
| Song [8] | 31 (SyLND)/8 (SeLND) | 24% | 70% | 16% (SeLND) 13% (SyLND) 32% (NoLND) |
| Bund [9] | 28 (SyLND) | 11% | NA | no difference |
| Authors | RFS (Months) | OS (Months) | ||
|---|---|---|---|---|
| Fagotti [4] | 2y RFS: 36% (SyLND) 25% (NoLND) | p = 0.834 | 2y OS: 69% (SyLND) 88% (NoLND) | p = 0.77 |
| Iwase [5] | 2y RFS: 56% (SyLND N-) 24% (SyLND N+) 26% (NoLND) | p = 0.534 | 5y OS: 62% (SyLND N-) 26% (SyLND N+) 19% (NoLND) | p = 0.97 |
| Schwartz [6] | 10.4 (SyLND) 9.7 (NoLND) | p = 0.80 | 33 (SyLND) 35 (NoLND) | p = 0.17 |
| Eoh [7] | 12 (SeLND) 17 (SyLND) | p = 0.74 | 28 (SeLND) 37 (SyLND) | p = 0.001 |
| Song [8] | 28 (SeLND) 30 (SyLND) 22 (NoLND) | p = 0.566 | 50 (SeLND) 59 (SyLND) 57 (NoLND) | p = 0.049 |
| Bund [9] | 18.2 (SyLND) 16.6 (NoLND) | p = 0.70 | 26.8 (SyLND) 27.8 (NoLND) | p = 0.48 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seidler, S.; Koual, M.; Achen, G.; Bentivegna, E.; Fournier, L.; Delanoy, N.; Nguyen-Xuan, H.-T.; Bats, A.-S.; Azaïs, H. Clinical Impact of Lymphadenectomy after Neoadjuvant Chemotherapy in Advanced Epithelial Ovarian Cancer: A Review of Available Data. J. Clin. Med. 2021, 10, 334. https://doi.org/10.3390/jcm10020334
Seidler S, Koual M, Achen G, Bentivegna E, Fournier L, Delanoy N, Nguyen-Xuan H-T, Bats A-S, Azaïs H. Clinical Impact of Lymphadenectomy after Neoadjuvant Chemotherapy in Advanced Epithelial Ovarian Cancer: A Review of Available Data. Journal of Clinical Medicine. 2021; 10(2):334. https://doi.org/10.3390/jcm10020334
Chicago/Turabian StyleSeidler, Stephanie, Meriem Koual, Guillaume Achen, Enrica Bentivegna, Laure Fournier, Nicolas Delanoy, Huyên-Thu Nguyen-Xuan, Anne-Sophie Bats, and Henri Azaïs. 2021. "Clinical Impact of Lymphadenectomy after Neoadjuvant Chemotherapy in Advanced Epithelial Ovarian Cancer: A Review of Available Data" Journal of Clinical Medicine 10, no. 2: 334. https://doi.org/10.3390/jcm10020334
APA StyleSeidler, S., Koual, M., Achen, G., Bentivegna, E., Fournier, L., Delanoy, N., Nguyen-Xuan, H.-T., Bats, A.-S., & Azaïs, H. (2021). Clinical Impact of Lymphadenectomy after Neoadjuvant Chemotherapy in Advanced Epithelial Ovarian Cancer: A Review of Available Data. Journal of Clinical Medicine, 10(2), 334. https://doi.org/10.3390/jcm10020334