
Tumor Necrosis Factor Receptor-Associated Periodic Syndrome (TRAPS) with a New Pathogenic Variant in TNFRSF1A Gene in a Family of the Adult Male with Renal AA Amyloidosis—Diagnostic and Therapeutic Challenge for Clinicians

 , , , and
, , , and 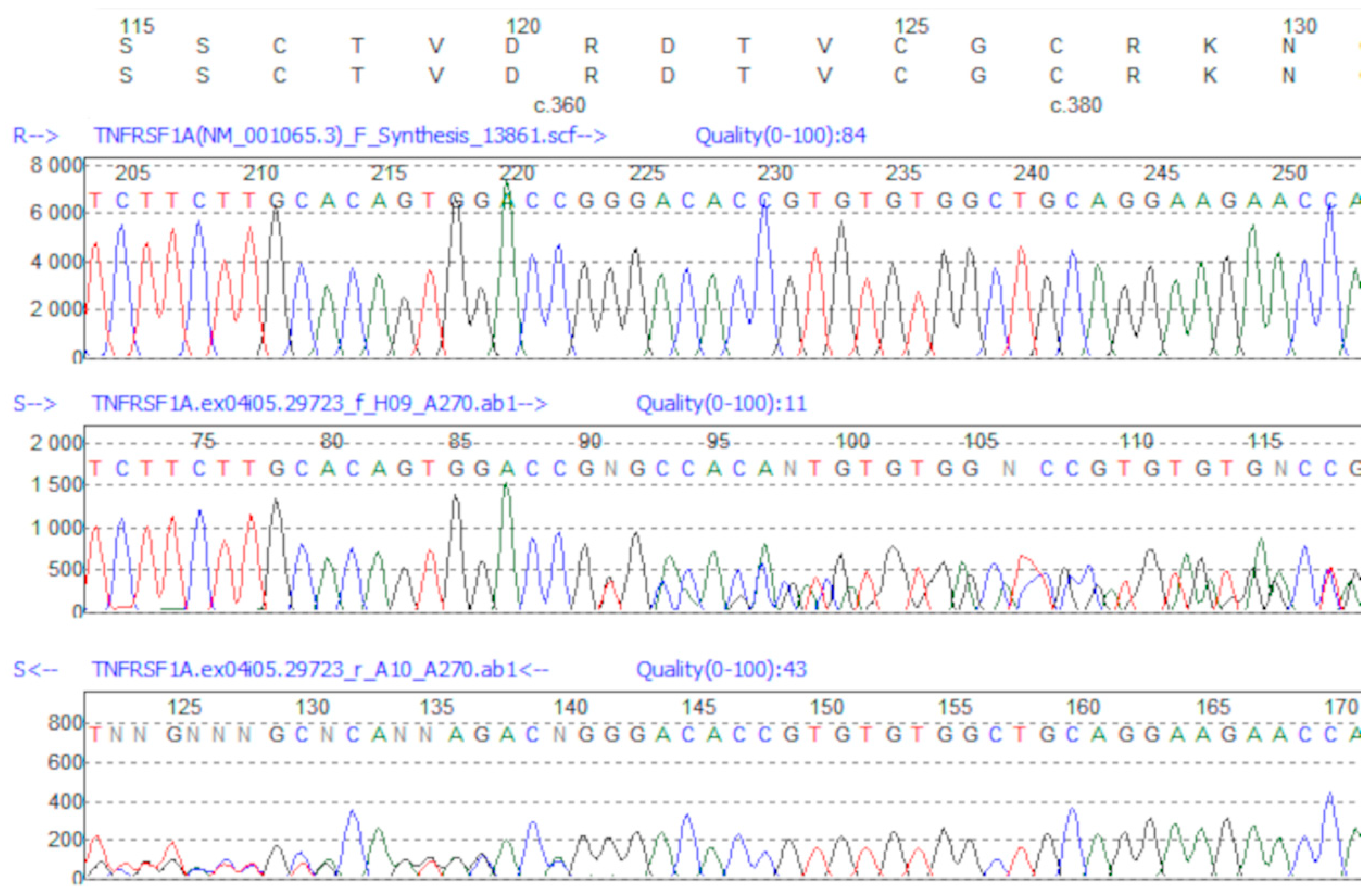{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Methods of Molecular Analysis
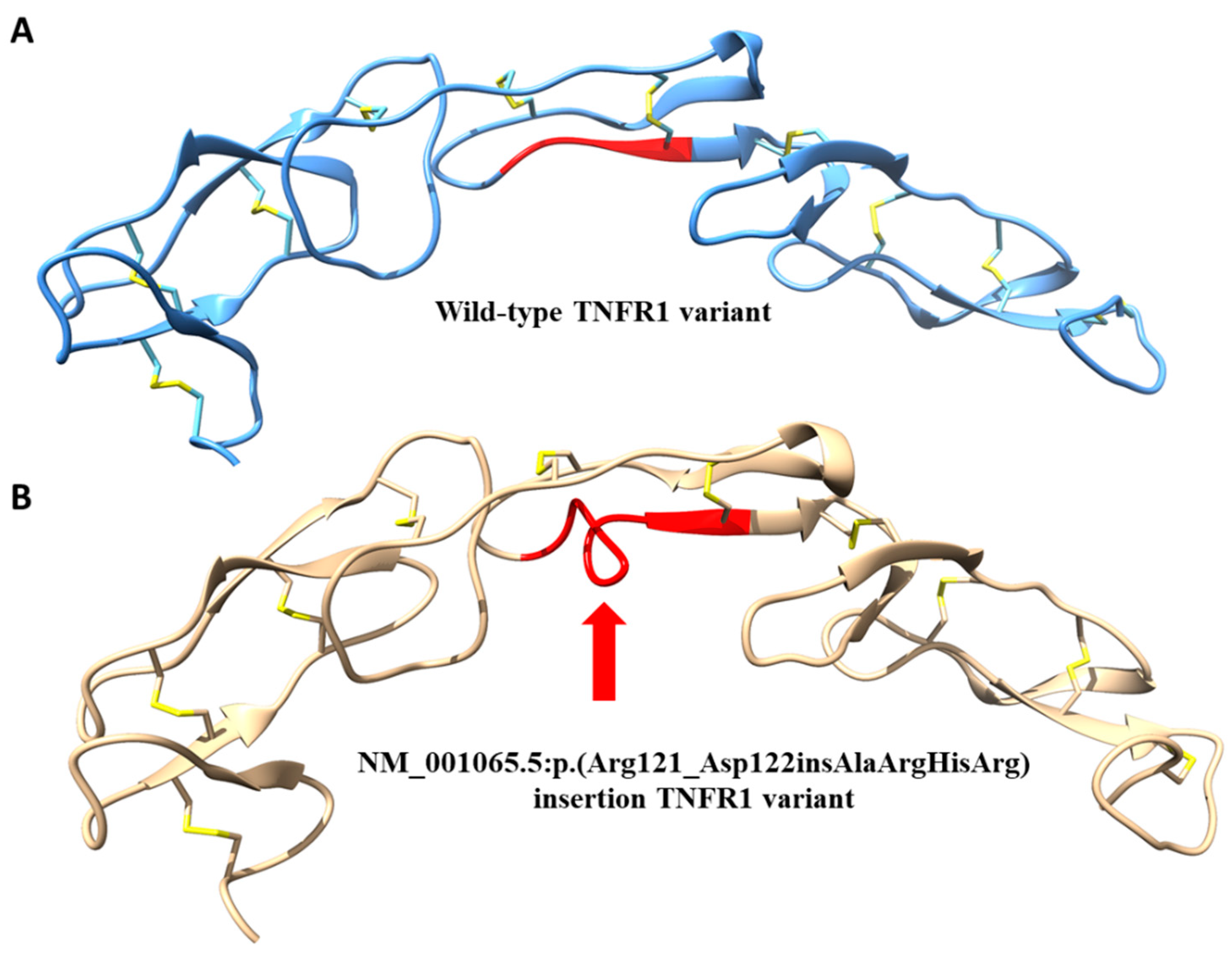
2.3. 3D Protein Modeling
3. Results
3.1. Patients
3.1.1. Patient 1—Proband
3.1.2. Remaining Patients
Patient 2
Patient 3
Patient 4
3.2. Genetic Results
Genetic Variant Identification
3.3. Management
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McDermott, M.F.; Aksentijevich, I.; Galon, J.; McDermott, E.M.; Ogunkolade, B.W.; Centola, M.; Mansfield, E.; Gadina, M.; Karenko, L.; Pettersson, T.; et al. Germline mutations in the extracellular domains of the 55 kDa TNF receptor, TNFR1, define a family of dominantly inherited autoinflammatory syndromes. Cell 1999, 97, 133–144. [Google Scholar] [CrossRef]
- Hull, K.M.; Drewe, E.; Aksentijevich, I.; Singh, H.K.; Wong, K.; McDermott, E.M.; Dean, J.; Powell, R.J.; Kastner, D.L. The TNF receptor-associated periodic syndrome (TRAPS): Emerging concepts of an autoinflammatory disorder. Medicine (Baltimore) 2002, 81, 349–368. [Google Scholar] [CrossRef] [PubMed]
- Aksentijevich, I.; Galon, J.; Soares, M.; Mansfield, E.; Hull, K.; Oh, H.H.; Goldbach-Mansky, R.; Dean, J.; Athreya, B.; Reginato, A.J.; et al. The tumor-necrosis-factor receptor-associated periodic syndrome: New mutations in TNFRSF1A, ancestral origins, genotype-phenotype studies, and evidence for further genetic heterogeneity of periodic fevers. Am. J. Hum. Genet. 2001, 69, 301–314. [Google Scholar] [CrossRef] [PubMed]
- Toro, J.R.; Aksentijevich, I.; Hull, K.; Dean, J.; Kastner, D.L. Tumor necrosis factor receptor-associated periodic syndrome: A novel syndrome with cutaneous manifestations. Arch. Dermatol. 2000, 136, 1487–1494. [Google Scholar] [CrossRef] [PubMed]
- Lachmann, H.J.; Papa, R.; Gerhold, K.; Obici, L.; Touitou, I.; Cantarini, L.; Frenkel, J.; Anton, J.; Kone-Paut, I.; Cattalini, M.; et al. The phenotype of TNF receptor-associated autoinflammatory syndrome (TRAPS) at presentation: A series of 158 cases from the Eurofever/EUROTRAPS international registry. Ann. Rheum. Dis. 2014, 73, 2160–2167. [Google Scholar] [CrossRef]
- Cudrici, C.; Deuitch, N.; Aksentijevich, I. Revisiting TNF Receptor-Associated Periodic Syndrome (TRAPS): Current Perspectives. Int. J. Mol. Sci. 2020, 21, 3263. [Google Scholar] [CrossRef]
- Brunger, A.F.; Nienhuis, H.L.A.; Bijzet, J.; Hazenberg, B.P.C. Causes of AA amyloidosis: A systematic review. Amyloid 2020, 27, 1–12. [Google Scholar] [CrossRef]
- Sarihan, I.; Caliskan, Y.; Mirioglu, S.; Ozluk, Y.; Senates, B.; Seyahi, N.; Basturk, T.; Yildiz, A.; Kilicaslan, I.; Sever, M.S. Amyloid A Amyloidosis After Renal Transplantation: An Important Cause of Mortality. Transplantation 2020, 104, 1703–1711. [Google Scholar] [CrossRef]
- Ter Haar, N.; Lachmann, H.; Ozen, S.; Woo, P.; Uziel, Y.; Modesto, C.; Kone-Paut, I.; Cantarini, L.; Insalaco, A.; Neven, B.; et al. Treatment of autoinflammatory diseases: Results from the Eurofever Registry and a literature review. Ann. Rheum. Dis. 2013, 72, 678–685. [Google Scholar] [CrossRef]
- Ozen, S.; Demir, S. Monogenic Periodic Fever Syndromes: Treatment Options for the Pediatric Patient. Paediatr. Drugs 2017, 19, 303–311. [Google Scholar] [CrossRef]
- Li, H.; Durbin, R. Fast and accurate long-read alignment with Burrows-Wheeler transform. Bioinformatics 2010, 26, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Bousfiha, A.; Jeddane, L.; Al-Herz, W.; Ailal, F.; Casanova, J.L.; Chatila, T.; Conley, M.E.; Cunningham-Rundles, C.; Etzioni, A.; Franco, J.L.; et al. The 2015 IUIS Phenotypic Classification for Primary Immunodeficiencies. J. Clin. Immunol. 2015, 35, 727–738. [Google Scholar] [CrossRef] [PubMed]
- 1000Genomes. Available online: http://www.l000genomes.org (accessed on 19 October 2016).
- Exome Variant Server. Available online: http://evs.gs.washington.edu/EVS (accessed on 19 October 2016).
- Pettersen, E.F.; Goddard, T.D.; Huang, C.C.; Couch, G.S.; Greenblatt, D.M.; Meng, E.C.; Ferrin, T.E. UCSF Chimera—A visualization system for exploratory research and analysis. J. Comput. Chem. 2004, 25, 1605–1612. [Google Scholar] [CrossRef] [PubMed]
- Sali, A.; Blundell, T.L. Comparative protein modelling by satisfaction of spatial restraints. J. Mol. Biol. 1993, 234, 779–815. [Google Scholar] [CrossRef] [PubMed]
- Shen, M.Y.; Sali, A. Statistical potential for assessment and prediction of protein structures. Protein Sci. 2006, 15, 2507–2524. [Google Scholar] [CrossRef]
- Greco, E.; Aita, A.; Galozzi, P.; Gava, A.; Sfriso, P.; Negm, O.H.; Tighe, P.; Caso, F.; Navaglia, F.; Dazzo, E.; et al. The novel S59P mutation in the TNFRSF1A gene identified in an adult onset TNF receptor associated periodic syndrome (TRAPS) constitutively activates NF-kappaB pathway. Arthritis Res. Ther. 2015, 17, 93. [Google Scholar] [CrossRef]
- Tsuji, S.; Matsuzaki, H.; Iseki, M.; Nagasu, A.; Hirano, H.; Ishihara, K.; Ueda, N.; Honda, Y.; Horiuchi, T.; Nishikomori, R.; et al. Functional analysis of a novel G87V TNFRSF1A mutation in patients with TNF receptor-associated periodic syndrome. Clin. Exp. Immunol. 2019, 198, 416–429. [Google Scholar] [CrossRef]
- Federici, S.; Sormani, M.P.; Ozen, S.; Lachmann, H.J.; Amaryan, G.; Woo, P.; Kone-Paut, I.; Dewarrat, N.; Cantarini, L.; Insalaco, A.; et al. Evidence-based provisional clinical classification criteria for autoinflammatory periodic fevers. Ann. Rheum. Dis. 2015, 74, 799–805. [Google Scholar] [CrossRef]
- Gattorno, M.; Hofer, M.; Federici, S.; Vanoni, F.; Bovis, F.; Aksentijevich, I.; Anton, J.; Arostegui, J.I.; Barron, K.; Ben-Cherit, E.; et al. Classification criteria for autoinflammatory recurrent fevers. Ann. Rheum. Dis. 2019, 78, 1025–1032. [Google Scholar] [CrossRef]
- Federici, S.; Vanoni, F.; Ben-Chetrit, E.; Cantarini, L.; Frenkel, J.; Goldbach-Mansky, R.; Gul, A.; Hoffman, H.; Kone-Paut, I.; Kuemmerle-Deschner, J.; et al. An International Delphi Survey for the Definition of New Classification Criteria for Familial Mediterranean Fever, Mevalonate Kinase Deficiency, TNF Receptor-associated Periodic Fever Syndromes, and Cryopyrin-associated Periodic Syndrome. J. Rheumatol. 2019, 46, 429–436. [Google Scholar] [CrossRef]
- Rowczenio, D.M.; Lachmann, H.J. How to prescribe a genetic test for the diagnosis of autoinflammatory diseases? Presse Med. 2019, 48, e49. [Google Scholar] [CrossRef] [PubMed]
- Rigante, D.; Frediani, B.; Cantarini, L. A Comprehensive Overview of the Hereditary Periodic Fever Syndromes. Clin. Rev. Allergy Immunol. 2018, 54, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Drewe, E.; McDermott, E.M.; Powell, R.J. Treatment of the nephrotic syndrome with etanercept in patients with the tumor necrosis factor receptor-associated periodic syndrome. N. Engl. J. Med. 2000, 343, 1044–1045. [Google Scholar] [CrossRef] [PubMed]
- Papa, R.; Lane, T.; Minden, K.; Touitou, I.; Cantarini, L.; Cattalini, M.; Obici, L.; Jansson, A.F.; Belot, A.; Frenkel, J.; et al. INSAID Variant Classification and Eurofever Criteria Guide Optimal Treatment Strategy in Patients with TRAPS: Data from the Eurofever Registry. J. Allergy Clin. Immunol. Pract. 2020. [Google Scholar] [CrossRef] [PubMed]
- Ozen, S.; Kuemmerle-Deschner, J.B.; Cimaz, R.; Livneh, A.; Quartier, P.; Kone-Paut, I.; Zeft, A.; Spalding, S.; Gul, A.; Hentgen, V.; et al. International Retrospective Chart Review of Treatment Patterns in Severe Familial Mediterranean Fever, Tumor Necrosis Factor Receptor-Associated Periodic Syndrome, and Mevalonate Kinase Deficiency/Hyperimmunoglobulinemia D Syndrome. Arthritis Care Res. (Hoboken) 2017, 69, 578–586. [Google Scholar] [CrossRef]
- Gentileschi, S.; Rigante, D.; Vitale, A.; Sota, J.; Frediani, B.; Galeazzi, M.; Cantarini, L. Efficacy and safety of anakinra in tumor necrosis factor receptor-associated periodic syndrome (TRAPS) complicated by severe renal failure: A report after long-term follow-up and review of the literature. Clin. Rheumatol. 2017, 36, 1687–1690. [Google Scholar] [CrossRef]
- La Torre, F.; Caparello, M.C.; Cimaz, R. Canakinumab for the treatment of TNF-receptor associated periodic syndrome. Expert Rev. Clin. Immunol. 2017, 13, 513–523. [Google Scholar] [CrossRef]
- De Benedetti, F.; Gattorno, M.; Anton, J.; Ben-Chetrit, E.; Frenkel, J.; Hoffman, H.M.; Kone-Paut, I.; Lachmann, H.J.; Ozen, S.; Simon, A.; et al. Canakinumab for the Treatment of Autoinflammatory Recurrent Fever Syndromes. N. Engl. J. Med. 2018, 378, 1908–1919. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zegarska, J.; Wiesik-Szewczyk, E.; Hryniewiecka, E.; Wolska-Kusnierz, B.; Soldacki, D.; Kacprzak, M.; Sobczynska-Tomaszewska, A.; Czerska, K.; Siedlecki, P.; Jahnz-Rozyk, K.; et al. Tumor Necrosis Factor Receptor-Associated Periodic Syndrome (TRAPS) with a New Pathogenic Variant in TNFRSF1A Gene in a Family of the Adult Male with Renal AA Amyloidosis—Diagnostic and Therapeutic Challenge for Clinicians. J. Clin. Med. 2021, 10, 465. https://doi.org/10.3390/jcm10030465
Zegarska J, Wiesik-Szewczyk E, Hryniewiecka E, Wolska-Kusnierz B, Soldacki D, Kacprzak M, Sobczynska-Tomaszewska A, Czerska K, Siedlecki P, Jahnz-Rozyk K, et al. Tumor Necrosis Factor Receptor-Associated Periodic Syndrome (TRAPS) with a New Pathogenic Variant in TNFRSF1A Gene in a Family of the Adult Male with Renal AA Amyloidosis—Diagnostic and Therapeutic Challenge for Clinicians. Journal of Clinical Medicine. 2021; 10(3):465. https://doi.org/10.3390/jcm10030465
Chicago/Turabian StyleZegarska, Jolanta, Ewa Wiesik-Szewczyk, Ewa Hryniewiecka, Beata Wolska-Kusnierz, Dariusz Soldacki, Magdalena Kacprzak, Agnieszka Sobczynska-Tomaszewska, Kamila Czerska, Pawel Siedlecki, Karina Jahnz-Rozyk, and et al. 2021. "Tumor Necrosis Factor Receptor-Associated Periodic Syndrome (TRAPS) with a New Pathogenic Variant in TNFRSF1A Gene in a Family of the Adult Male with Renal AA Amyloidosis—Diagnostic and Therapeutic Challenge for Clinicians" Journal of Clinical Medicine 10, no. 3: 465. https://doi.org/10.3390/jcm10030465
APA StyleZegarska, J., Wiesik-Szewczyk, E., Hryniewiecka, E., Wolska-Kusnierz, B., Soldacki, D., Kacprzak, M., Sobczynska-Tomaszewska, A., Czerska, K., Siedlecki, P., Jahnz-Rozyk, K., Bernatowska, E., Zagozdzon, R., & Paczek, L. (2021). Tumor Necrosis Factor Receptor-Associated Periodic Syndrome (TRAPS) with a New Pathogenic Variant in TNFRSF1A Gene in a Family of the Adult Male with Renal AA Amyloidosis—Diagnostic and Therapeutic Challenge for Clinicians. Journal of Clinical Medicine, 10(3), 465. https://doi.org/10.3390/jcm10030465