
COVID-19 in Children with Down Syndrome: Data from the Trisomy 21 Research Society Survey
 ,
,  , , ,
, , ,  , and add
Show full author list
, and add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
2.1. T21RS DS Survey
2.2. US COVID-NET Comparison Data
2.3. Statistical Analyses
3. Results
4. Discussion
4.1. Hospitalisation and Outcomes
4.2. Implications for Policy and Practice
4.3. Limitations and Areas for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
| Spain | The study was approved by the Hospital del Mar ethics committee (CEIC Parc de Salut Mar, CEIM 2020/9197) |
| United Kingdom | The T21RS survey was approved by the Health research agency (HRA) 20/HRA/2452. The ISARIC4C analysis was approved by the study board (IDAMAC) |
| Brazil | This study was approved by the Brazilian Federal Ethics Committee (CONEP, CAAE: 30847520.8.0000.0071) |
| Emory University, USA | This study was deemed exempt from human subject research under 45 CFR 46.104(d)(2i) (IRB ID: STUDY00000386) |
| Italy | The study was approved by the Bambino Gesù children’s Hospital Ethics Committee (2091_OPBG_2020) |
| Advocate Health Care Institutional Review Board | Determined to have Exempt Status IRB# 20-151ET |
| France | This study was approved by CPP Sud Mediterranée IV dated 29/04/2020 (ID RCB 2020-A00940-39) |
| Ludwig-Maximilians-Universität (LMU), Munich, Germany | Determined to have Exempt Status (IRB ID: 20-573 KB) |
| India | The study was approved by the Ethics Committee constituted by the University of Calcutta (CU/BIOETHICS/HUMAN/2306/3044/2020) |
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Children with DS | |
|---|---|
| n | 328 |
| Signs and symptoms of COVID-19 (%) | 312 (95.4) |
| COVID-19 testing performed (%) | 233 (71.5) |
| Reason for COVID-10 testing (%) | |
| Contact with affected individuals | 38 (16.6) |
| Routine testing | 3 (1.3) |
| Symptoms were present | 188 (82.1) |
| Results of the testing (%) | |
| Negative | 16 (7.4) |
| Pending | 6 (2.8) |
| Positive | 194 (89.8) |
| Overall | India | Brazil | UK | USA | Spain | Other | |
|---|---|---|---|---|---|---|---|
| n | 328 | 137 | 56 | 36 | 30 | 12 | 47 |
| Age (mean (SD)) | 9.55 (5.24) | 12.71 (3.14) | 5.68 (5.26) | 8.42 (4.72) | 7.33 (5.80) | 6.25 (5.50) | 8.44 (4.76) |
| Male (%) | 173 (52.7) | 61 (44.5) | 29 (51.8) | 20 (55.6) | 18 (60.0) | 9 (75.0) | 28 (60.9) |
| Ethnicity (%) | |||||||
| South Asian | 142 (43.2) | 136 (99.3) | 0 (0.0) | 2 (5.6) | 0 (0.0) | 0 (0.0) | 3 (6.4) |
| White | 110 (33.4) | 0 (0.0) | 25 (44.6) | 29 (80.6) | 21 (70.0) | 10 (83.3) | 22 (46.8) |
| Latin American | 31 (9.4) | 0 (0.0) | 20 (35.7) | 0 (0.0) | 4 (13.3) | 0 (0.0) | 5 (10.6) |
| Black | 6 (1.8) | 0 (0.0) | 1 (1.8) | 2 (5.6) | 3 (10.0) | 0 (0.0) | 0 (0.0) |
| Arab | 1 (0.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (2.1) |
| West Asian | 1 (0.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (2.1) |
| Admixed | 12 (3.6) | 0 (0.0) | 9 (16.1) | 1 (2.8) | 1 (3.3) | 1 (8.3) | 0 (0.0) |
| Unknown | 26 (7.9) | 1 (0.7) | 1 (1.8) | 2 (5.6) | 1 (3.3) | 1 (8.3) | 15 (31.9) |
| CDC Controls | T21RS Individuals with Down Syndrome | T21RS Individuals with Down Syndrome, High-Income Countries | T21RS Individuals with Down Syndrome, Low to Mid-Income Countries | |
|---|---|---|---|---|
| Age, n (%) | ||||
| <1 year | 157 (27.3) | 14 (4.3) | 6 (5.4) | 7 (3.4) |
| 1 year | 31 (5.4) | 17 (4.9) | 8 (7.1) | 9 (4.4) |
| 2–4 years | 50 (8.7) | 43 (13.1) | 20 (17.9) | 20 (9.7) |
| 5–11 years | 97 (16.8) | 119 (36.3) | 49 (43.8) | 68 (33.0) |
| 12–17 years | 241 (41.8) | 136 (41.5) | 29 (25.9) | 102 (49.5) |
| Gender, n (%) | ||||
| Male | 292 (50.7) | 155 (47.4) | 45 (40.2) | 106 (51.4) |
| Female | 284 (49.3) | 172 (52.6) | 67 (59.8) | 99 (48.1) |
| T21RS COVID-19 Patients from High-Income Countries | T21RS COVID-19 Patients from Low to Mid-Income Countries | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Non-Hospitalised Controls | Hospitalised Patients | Non-Hospitalised Controls | Hospitalised Patients | |||||||
| n | n | p Value (Comparison with Controls) | n | n | p Value (Comparison with Controls) | |||||
| Cough, n (%) | 59 (67.0) | 88 | 19 (82.6) | 23 | 0.202 | 38 (36.5) | 104 | 47 (47.0) | 100 | 0.156 |
| Fever, n (%) | 55 (62.5) | 88 | 21 (91.3) | 23 | 0.010 | 64 (61.5) | 104 | 95 (95.0) | 100 | <0.001 |
| Nasal congestion, n (%) | 49 (55.7) | 88 | 13 (56.5) | 23 | 1 | 63 (60.6) | 104 | 67 (67.0) | 100 | 0.383 |
| Shortness of breath, n (%) | 25 (28.4) | 88 | 18 (78.3) | 23 | <0.001 | 39 (37.5) | 104 | 56 (56.0) | 100 | 0.011 |
| Abdominal pain, n (%) | 18 (20.5) | 88 | 3 (13.0) | 23 | 0.557 | 13 (12.5) | 104 | 20 (20.0) | 100 | 0.183 |
| Vomiting/nausea, n (%) | 17 (19.3) | 88 | 3 (13.0) | 23 | 0.059 | 10 (9.6) | 104 | 20 (20.0) | 100 | 0.047 |
| Diarrhoea, n (%) | 30 (34.1) | 88 | 6 (26.1) | 23 | 0.618 | 15 (14.4) | 104 | 12 (12.0) | 100 | 0.682 |
| Overall | Not Hospitalised | Hospitalised | |
|---|---|---|---|
| n | 133 | 100 | 25 |
| Additional information through follow-up (%) | 12 (9.0) | 11 (11.0) | 1 (4.0) |
| Country (%) | |||
| India | 34 (25.8) | 23 (23.0) | 7 (29.2) |
| Brazil | 24 (18.2) | 20 (20.0) | 3 (12.5) |
| United Kingdom | 6 (4.5) | 5 (5.0) | 1 (4.2) |
| United States | 17 (12.9) | 16 (16.0) | 1 (4.2) |
| Spain | 9 (6.8) | 7 (7.0) | 0 (0.0) |
| other | 42 (31.8) | 29 (29.0) | 12 (50.0) |
| Age (mean (SD)) | 9.04 (5.24) | 9.32 (5.10) | 7.60 (6.28) |
| Male (%) | 72 (54.1) | 51 (51.0) | 15 (60.0) |
| Ethnicity (%) | |||
| South Asian | 33 (24.8) | 22 (22.0) | 7 (28.0) |
| White | 64 (48.1) | 56 (56.0) | 5 (20.0) |
| Latin American | 15 (11.3) | 12 (12.0) | 2 (8.0) |
| Black | 2 (1.5) | 0 (0.0) | 2 (8.0) |
| Arab | 3 (2.3) | 1 (1.0) | 2 (8.0) |
| West Asian | 3 (2.3) | 2 (2.0) | 1 (4.0) |
| Admixed | --- | --- | --- |
| Unknown | 13 (9.8) | 7 (7.0) | 6 (24.0) |
| Living situation (%) | |||
| Living at home with family | 126 (99.2) | 95 (99.0) | 23 (100) |
| Living alone with support | 1 (0.8) | 1 (1.0) | 0 (0) |
| Small group home with support | 0 (0) | 0 (0) | 0 (0) |
| Residential care facility | 0 (0) | 0 (0) | 0 (0) |
| Other | 0 (0) | 0 (0) | 0 (0) |
| Type of trisomy 21 (%) | |||
| Full/standard | 121 (94.5) | 91 (93.8) | 23 (100.0) |
| Mosaic | 4 (3.1) | 3 (3.1) | 0 (0.0) |
| Partial trisomy | 0 (0) | 0 (0) | 0 (0) |
| Translocation | 3 (2.3) | 3 (3.1) | 0 (0.0) |
| Level of intellectual disability (%) | |||
| Borderline/normal/mild | 27 (24.1) | 17 (19.8) | 7 (38.9) |
| Moderate | 72 (64.3) | 58 (67.4) | 10 (55.6) |
| Severe/Profound | 13 (11.6) | 11 (12.8) | 1 (5.6) |
| Admitted to hospital (%) | 25 (20.0) | 0 (0.0) | 25 (100.0) |
| Days in hospital (mean (SD)) | 22.39 (42.18) | NA | 22.39 (42.18) |
| Admitted to ICU (%) | 13 (52.0) | 0 (0.0) | 13 (52.0) |
| Days in ICU (mean (SD)) | 16.73 (24.82) | NA | 16.73 (24.82) |
| Mechanical ventilation (%) | 7 (10.4) | 0 (0.0) | 7 (28.0) |
| Clinical situation at last evaluation (%) | |||
| Currently in hospital with symptoms | 0 (0) | 0 (0) | 0 (0) |
| Died | 1 (0.8) | 0 (0.0) | 1 (4.2) |
| Not currently in hospital but with symptoms | 15 (11.5) | 10 (10.0) | 3 (12.5) |
| Other | 4 (3.1) | 2 (2.0) | 2 (8.3) |
| Recovered from COVID-19 | 89 (67.9) | 67 (67.0) | 18 (75.0) |
| Tested positive but still no symptoms | 22 (16.8) | 21 (21.0) | 0 (0.0) |
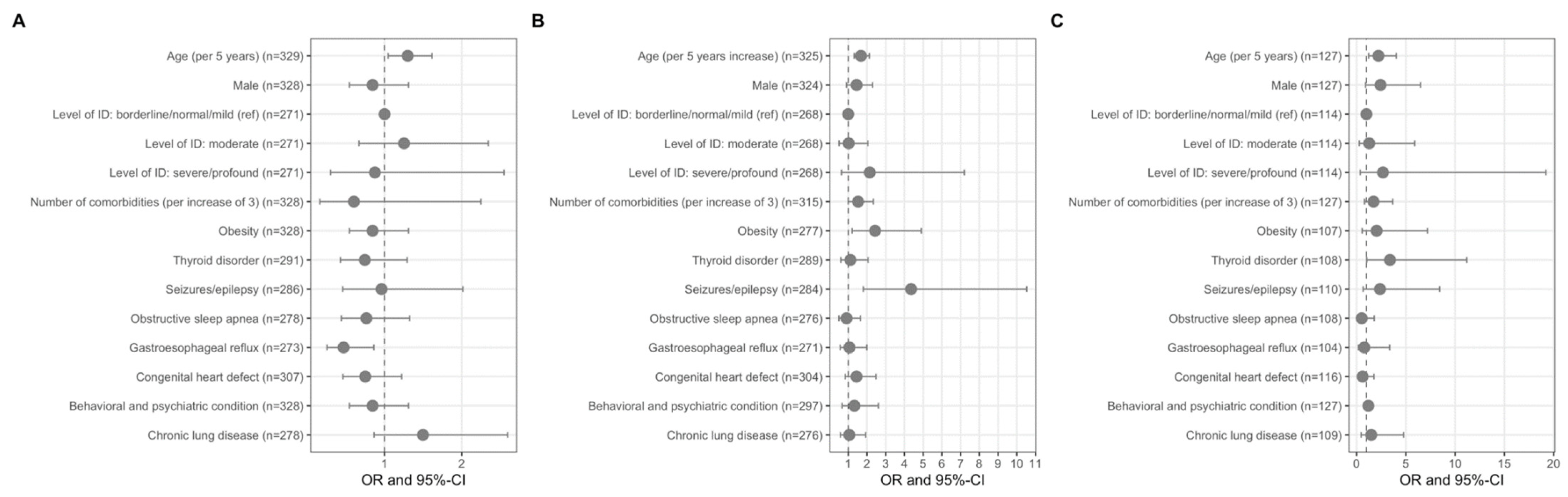
| Shortness of Breath OR, (CI) | Hospitalised OR, (CI) | ARDS OR, (CI) | |
|---|---|---|---|
| Age (per 5 years) | 1.31 (1.05–1.63) | 1.75 (1.37–2.23) | 2.29 (1.26–4.15) |
| Male | 0.81 (0.52–1.27) | 1.45 (0.90–2.34) | 2.44 (0.91–6.55) |
| Level of ID: borderline/normal/mild (ref) | 1 (1–1) | 1 (1–1) | 1 (1–1) |
| Level of ID: moderate | 1.20 (0.63–2.30) | 0.95 (0.46–1.93) | 1.40 (0.28–6.91) |
| Level of ID: severe/profound | 0.83 (0.28–2.42) | 1.94 (0.57–6.55) | 2.68 (0.36–19.9) |
| Number of comorbidities (per increase of 3) | 0.53 (0.14–2.05) | 1.48 (0.96–2.28) | 1.82 (0.84–3.97) |
| Obesity | 0.81 (0.52–1.27) | 2.27 (1.12–4.59) | 2.14 (0.58–7.91) |
| Thyroid disorder | 0.74 (0.42–1.29) | 1.19 (0.64–2.22) | 3.40 (1.03–11.9) |
| Seizures/epilepsy | 0.92 (0.44–1.92) | 3.97 (1.65–9.58) | 2.10 (0.58–7.66) |
| Obstructive sleep apnea | 0.77 (0.44–1.36) | 0.96 (0.52–1.76) | 0.67 (0.19–2.40) |
| Gastroesophageal reflux | 0.43 (0.24–0.79) | 1.00 (0.53–1.87) | 0.78 (0.18–3.37) |
| Congenital Heart Defect | 0.72 (0.44–1.18) | 1.39 (0.81–2.42) | 0.52 (0.18–1.54) |
| Behavioural and psychiatric condition | 0.81 (0.52–1.27) | 1.29 (0.65–2.55) | 1.22 (0.94–1.58) |
| Chronic Lung Disease | 1.47 (0.85–2.56) | 1.02 (0.56–1.87) | 1.31 (0.40–4.24) |
| Overall | Patients with Shortness of Breath | Hospitalised Patients | Patients with ARDS | |
|---|---|---|---|---|
| n | 328 | 259 | 127 | 20 |
| Obesity | 65 (23.0) | 37 (29.4) | 41 (38.7) | 9 (56.3) |
| Thyroid disorder | 93 (28.4) | 34 (26.0) | 34 (31.2) | 9 (56.3) |
| Seizures/epilepsy | 38 (13.1) | 19 (14.8) | 28 (25.5) | 6 (37.5) |
| Obstructive sleep apnea | 100 (35.5) | 45 (36.3) | 42 (39.3) | 4 (25.0) |
| Gastroesophageal reflux | 87 (31.4) | 35 (28.0) | 36 (34.3) | 3 (21.4) |
| Congenital Heart Defect | 149 (47.5) | 57 (42.9) | 61 (51.7) | 8 (42.1) |
| Behavioural and psychiatric condition | 103 (33.6) | 52 (38.8) | 60 (52.6) | 9 (52.9) |
| Chronic Lung Disease | 103 (36.5) | 58 (46.0) | 48 (44.0) | 9 (52.9) |
| Shortness of Breath OR, (CI) | Hospitalised OR, (CI) | ARDS OR, (CI) | |
|---|---|---|---|
| Age (per 5 years) | 1.31 (1.05–1.63) | 1.75 (1.37–2.23) | 2.29 (1.26–4.15) |
| Male | 0.81 (0.52–1.27) | 1.45 (0.90–2.34) | 2.44 (0.91–6.55) |
| Level of ID: borderline/normal/mild (ref) | 1 (1–1) | 1 (1–1) | 1 (1–1) |
| Level of ID: moderate | 1.20 (0.63–2.30) | 0.95 (0.46–1.93) | 1.40 (0.28–6.91) |
| Level of ID: severe/profound | 0.83 (0.28–2.42) | 1.94 (0.57–6.55) | 2.68 (0.36–19.9) |
| Number of comorbidities (per increase of 3) | 0.53 (0.14–2.05) | 1.48 (0.96–2.28) | 1.82 (0.84–3.97) |
| Obesity | 0.81 (0.52–1.27) | 2.27 (1.12–4.59) | 2.14 (0.58–7.91) |
| Thyroid disorder | 0.74 (0.42–1.29) | 1.19 (0.64–2.22) | 3.40 (1.03–11.9) |
| Seizures/epilepsy | 0.92 (0.44–1.92) | 3.97 (1.65–9.58) | 2.10 (0.58–7.66) |
| Obstructive sleep apnea | 0.77 (0.44–1.36) | 0.96 (0.52–1.76) | 0.67 (0.19–2.40) |
| Gastroesophageal reflux | 0.43 (0.24–0.79) | 1.00 (0.53–1.87) | 0.78 (0.18–3.37) |
| Congenital Heart Defect | 0.72 (0.44–1.18) | 1.39 (0.81–2.42) | 0.52 (0.18–1.54) |
| Behavioural and psychiatric condition | 0.81 (0.52–1.27) | 1.29 (0.65–2.55) | 1.22 (0.94–1.58) |
| Chronic Lung Disease | 1.47 (0.85–2.56) | 1.02 (0.56–1.87) | 1.31 (0.40–4.24) |
References
- Espinosa, J.M. Down Syndrome and COVID-19: A Perfect Storm? Cell Rep. Med. 2020, 1, 100019. [Google Scholar] [CrossRef] [PubMed]
- Hüls, A.; Costa, A.; Dierssen, M.; Baksh, A.; Bargagna, S.; Baumer, N. An International Survey on the Impact of COVID-19 in Individuals with Down Syndrome. MedXRiv (Preprint) 2020. [Google Scholar]
- De Toma, I.; Dierssen, M. Network analysis of Down Syndrome and SARS-CoV-2 identifies risk and protective factors for COVID-19. Sci. Rep. 2021, 11, 1930. [Google Scholar] [CrossRef]
- Prayle, A.P.; Vyas, H.G. Respiratory Complications of Down Syndrome. Kendig’s Disord. Respir. Tract Child. 2019, 2019, 992–1006.e2. [Google Scholar] [CrossRef]
- Carsetti, R.; Valentini, D.; Marcellini, V.; Scarsella, M.; Marasco, E.; Giustini, F.; Bartuli, A.; Villani, A.; Ugazio, A.G. Reduced numbers of switched memory B cells with high terminal differentiation potential in Down Syndrome. Eur. J. Immunol. 2014, 45, 903–914. [Google Scholar] [CrossRef]
- Bloemers, B.L.; Broers, C.J.; Bont, L.; Weijerman, M.E.; Gemke, R.J.; van Furth, A.M. Increased risk of respiratory tract infections in children with Down Syndrome: The consequence of an altered immune system. Microbes Infect. 2010, 12, 799–808. [Google Scholar] [CrossRef] [PubMed]
- Kantar, A.; Mazza, A.; Bonanomi, E.; Odoni, M.; Seminara, M.; Verde, I.D.; Lovati, C.; Bolognini, S.; D’Antiga, L. COVID-19 and children with Down Syndrome: Is there any real reason to worry? Two case reports with severe course. BMC Pediatr. 2020, 20, 561. [Google Scholar] [CrossRef]
- Newman, A.M.; Jhaveri, R.; Patel, A.B.; Tan, T.Q.; Toia, J.M.; Arshad, M. Trisomy 21 and Coronavirus Disease 2019 in Pediatric Patients. J. Pediatr. 2021, 228, 294–296. [Google Scholar] [CrossRef]
- Stewart, R.; El-Harakeh, A.; Cherian, S.A. Evidence synthesis communities in low-income and middle-income countries and the COVID-19 response. Lancet 2020, 396, 1539–1541. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Kim, L.; Whitaker, M.; O’Halloran, A.; Kambhampati, A.; Chai, S.J.; Reingold, A.; Armistead, I.; Kawasaki, B.; Meek, J.; Yousey-Hindes, K.; et al. Hospitalization Rates and Characteristics of Children Aged <18 Years Hospitalized with Laboratory-Confirmed COVID-19—COVID-NET, 14 States, March 1–July 25 2020. MMWR Morb. Mortal Wkly. Rep. 2020, 69, 1081–1088. [Google Scholar] [CrossRef]
- High Income Countries. 2021. Available online: https://worldpopulationreview.com/country-rankings/high-income-countries (accessed on 8 June 2021).
- Costa-Carvalho, B.; Martinez, R.; Dias, A.; Kubo, C.; Barros-Nunes, P.; Leiva, L.; Solé, D.; Carneiro-Sampaio, M.; Naspitz, C.; Sorensen, R. Antibody response to pneumococcal capsular polysaccharide vaccine in Down syndrome patients. Braz. J. Med. Biol. Res. 2006, 39, 1587–1592. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Utiyama, S.R.D.R.; Nisihara, R.M.; Nass, F.R.; Oliveira, N.P.; Fiedler, P.T.; De Messias-Reason, I.T. Autoantibodies in patients with Down Syndrome: Early senescence of the immune system or precocious markers for immunological diseases? J. Paediatr. Child Health 2008, 44, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Valentini, D.; Marcellini, V.; Bianchi, S.; Villani, A.; Facchini, M.; Donatelli, I.; Castrucci, M.R.; Marasco, E.; Farroni, C.; Carsetti, R. Generation of switched memory B cells in response to vaccination in Down Syndrome children and their siblings. Vaccine 2015, 33, 6689–6696. [Google Scholar] [CrossRef]
- Eijsvoogel, N.B.; Hollegien, M.I.; Bok, V.L.; Derksen− Lubsen, A.G.; Dikken, F.P.; Leenders, S.A.; Pijning, A.; Post, E.; Wojciechowski, M.; Hilbink, M.; et al. Declining antibody levels after hepatitis B vaccination in Down Syndrome: A need for booster vaccination? J. Med. Virol. 2017, 89, 1682–1685. [Google Scholar] [CrossRef]
- Palaiodimos, L.; Kokkinidis, D.G.; Li, W.; Karamanis, D.; Ognibene, J.; Arora, S.; Southern, W.N.; Mantzoros, C.S. Severe obesity, increasing age and male sex are independently associated with worse in-hospital outcomes, and higher in-hospital mortality, in a cohort of patients with COVID-19 in the Bronx, New York. Metabolism 2020, 108, 154262. [Google Scholar] [CrossRef]
- Docherty, A.B.; Harrison, E.M.; Green, C.A.; Hardwick, H.E.; Pius, R.; Norman, L.; Holden, K.A.; Read, J.M.; Dondelinger, F.; Carson, G.; et al. Features of 20 133 UK patients in hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: Prospective observational cohort study. BMJ 2020, 369, m1985. [Google Scholar] [CrossRef] [PubMed]
- Peckham, H.; de Gruijter, N.M.; Raine, C.; Radziszewska, A.; Ciurtin, C.; Wedderburn, L.R.; Rosser, E.C.; Webb, K.; Deakin, C.T. Male sex identified by global COVID-19 meta-analysis as a risk factor for death and ITU admission. Nat. Commun. 2020, 11, 6317. [Google Scholar] [CrossRef]
- French, J.A.; Brodie, M.J.; Caraballo, R.; Devinsky, O.; Ding, D.; Jehi, L.; Jette, N.; Kanner, A.; Modi, A.C.; Newton, C.R.; et al. Keeping people with epilepsy safe during the COVID-19 pandemic. Neurology 2020, 94, 1032–1037. [Google Scholar] [CrossRef]
- Kuroda, N. Epilepsy and COVID-19: Associations and important considerations. Epilepsy Behav. 2020, 108, 107122. [Google Scholar] [CrossRef] [PubMed]
- Asadi-Pooya, A.A.; Attar, A.; Moghadami, M.; Karimzadeh, I. Management of COVID-19 in people with epilepsy: Drug considerations. Neurol. Sci. 2020, 41, 2005–2011. [Google Scholar] [CrossRef] [PubMed]
- Niazkar, H.R.; Zibaee, B.; Nasimi, A.; Bahri, N. The neurological manifestations of COVID-19: A review article. Neurol. Sci. 2020, 41, 1667–1671. [Google Scholar] [CrossRef]
- Chen, M.; Zhou, W.; Xu, W.-W. Thyroid Function Analysis in 50 Patients with COVID-19: A Retrospective Study. Thyroid 2021, 31, 8–11. [Google Scholar] [CrossRef] [PubMed]
- Millet, J.K.; Whittaker, G.R. Host cell proteases: Critical determinants of coronavirus tropism and pathogenesis. Virus Res. 2015, 202, 120–134. [Google Scholar] [CrossRef] [PubMed]


| Overall | Not Hospitalised | Hospitalised | |
|---|---|---|---|
| n | 328 | 197 | 127 |
| Additional information through follow-up (%) # | 29 (8.8) | 25 (12.7) | 4 (3.1) |
| Country (%) | |||
| India | 137 (42.9) | 52 (27.1) | 85 (69.1) |
| Brazil | 56 (17.6) | 44 (22.9) | 11 (8.9) |
| United Kingdom | 36 (11.3) | 28 (14.6) | 8 (6.5) |
| United States | 30 (9.4) | 22 (11.5) | 7 (5.7) |
| Spain | 12 (3.8) | 9 (4.7) | 3 (2.4) |
| other | 48 (15.0) | 37 (19.3) | 9 (7.3) |
| Age (mean (SD)) | 9.55 (5.24) | 8.47 (4.99) | 11.37 (5.07) |
| Male (%) | 173 (52.7) | 97 (48.5) | 74 (58.3) |
| Ethnicity (%) | |||
| South Asian | 142 (43.2) | 54 (27.4) | 88 (69.3) |
| White | 110 (33.4) | 89 (44.2) | 21 (16.5) |
| Latin American | 31 (9.4) | 23 (11.7) | 7 (5.5) |
| Black | 6 (1.8) | 3 (1.5) | 3 (2.4) |
| Arab | 1 (0.3) | 1 (0.5) | 0 (0.0) |
| West Asian | 1 (0.3) | 1 (0.5) | 0 (0.0) |
| Admixed | 12 (3.6) | 9 (4.6) | 3 (2.4) |
| Unknown | 26 (7.9) | 19 (9.6) | 5 (3.9) |
| Living situation (%) | |||
| Living at home with family | 304 (98.1) | 190 (97.9) | 110 (98.2) |
| Living alone with support | 1 (0.3) | 0 (0.0) | 1 (0.9) |
| Small group home with support | 2 (0.6) | 2 (1.0) | 0 (0.0) |
| Residential care facility | 2 (0.6) | 1 (0.5) | 1 (0.9) |
| Other | 1 (0.3) | 1 (0.5) | 0 (0.0) |
| Type of trisomy 21 (%) | |||
| Full/standard | 274 (88.4) | 167 (87.9) | 105 (89.7) |
| Mosaic | 29 (9.4) | 17 (8.9) | 11 (9.4) |
| Partial trisomy | 2 (0.6) | 2 (1.0) | 0 (0.0) |
| Translocation | 5 (1.6) | 4 (2.1) | 1 (0.9) |
| Level of intellectual disability (%) | |||
| Borderline/normal/mild | 83 (30.0) | 59 (37.1) | 23 (20.2) |
| Moderate | 172 (62.1) | 91 (57.2) | 78 (68.4) |
| Severe/Profound | 22 (7.9) | 9 (5.7) | 13 (11.4) |
| Admitted to hospital (%) | 127 (39.2) | 0 (0.0) | 127 (100.0) |
| Days in hospital (mean (SD)) * | 11.03 (5.18) | NA | 11.03 (5.18) |
| Admitted to ICU (%) * | 48 (38.4) | 0 (0) | 48 (38.4) |
| Days in ICU (mean (SD)) * | 6.91 (2.52) | NA | 6.91 (2.52) |
| Mechanical ventilation (%) * | 28 (16.1) | 0 (0.0) | 28 (24.8) |
| Clinical situation at last evaluation (%) | |||
| Currently in hospital with symptoms | 38 (12.5) | 0 (0.0) | 37 (31.4) |
| Died | 4 (1.3) | 0 (0.0) | 4 (3.4) |
| Not currently in hospital but with symptoms | 45 (14.8) | 34 (18.6) | 10 (8.5) |
| Other | 12 (3.9) | 9 (4.9) | 3 (2.5) |
| Recovered from COVID-19 | 197 (64.8) | 132 (71.1) | 64 (54.2) |
| Tested positive but still no symptoms | 8 (2.6) | 8 (4.4) | 0 (0.0) |
| A. Signs and Symptoms Related to COVID-19 | |||||||||||
| CDC controls | T21RS Individuals with Down Syndrome | T21RS Individuals with Down Syndrome, High Income Countries | T21RS Individuals with Down Syndrome, Low-to-Mid Income Countries | ||||||||
| n | n | p Value (Comparison with Controls) | n | p Value (Comparison with Controls) | n | p Value (Comparison with Controls) | |||||
| Cough, n (%) | 66 (29.5) | 224 | 66 (53.7) | 123 | 0.005 | 19 (82.6) | 23 | <0.001 | 47 (47.0) | 100 | 0.003 |
| Fever, n (%) | 121 (54.0) | 224 | 116 (94.3) | 123 | 0.001 | 21 (91.3) | 23 | <0.001 | 95 (95.0) | 100 | <0.001 |
| Nasal congestion 1, n (%) | 53 (23.7) | 224 | 80 (65.0) | 123 | <0.001 | 13 (56.5) | 23 | 0.002 | 67 (67.0) | 100 | <0.001 |
| Shortness of breath, n (%) | 50 (22.3) | 224 | 74 (60.2) | 123 | <0.001 | 18 (78.3) | 23 | <0.001 | 56 (56.0) | 100 | <0.001 |
| Abdominal pain, n (%) | 42 (18.8) | 224 | 23 (18.7) | 123 | 1 | 3 (13.0) | 23 | 0.776 | 20 (20.0) | 100 | 0.879 |
| Vomiting/nausea, n (%) | 69 (30.8) | 224 | 23 (18.7) | 123 | 0.063 | 3 (13.0) | 23 | 0.092 | 20 (20.0) | 100 | 0.059 |
| Diarrhoea, n (%) | 27 (12.1) | 224 | 18 (14.6) | 123 | 0.621 | 6 (26.1) | 23 | 0.098 | 12 (12.0) | 100 | 1 |
| B. Other Indicators for a Severe Course of COVID-19 | |||||||||||
| n | n | p Value (Comparison with Controls) | n | p Value (Comparison with Controls) | n | p Value (Comparison with Controls) | |||||
| Hospitalisation length of stay, median (IQR) | 2.5 (4) | 208 | 10 (7) | 119 | n/a | 8 (9) | 22 | n/a | 10 (7) | 97 | n/a |
| ICU admission, n (%) | 69 (33.2) | 208 | 47 (38.5) | 122 | 0.506 | 4 (17.4) | 23 | 0.041 | 43 (43.4) | 99 | 0.099 |
| Mechanical ventilation, n (%) | 12 (5.8) | 207 | 28 (24.8) | 113 | <0.001 | 3 (14.3) | 21 | 0.149 | 25 (27.2) | 92 | <0.001 |
| Death, n (%) | 1 (0.5) | 208 | 4 (5.0) | 80 | 0.025 | 0 (0.0) | 20 | 1 | 4 (6.7) | 60 | <0.001 |
| C. Prevalence of Medical Complications among Hospitalised Patients 2 | |||||||||||
| n | n | p Value (Comparison with Controls) | n | p Value (Comparison with Controls) | n | p Value (Comparison with Controls) | |||||
| Pneumonia, n (%) | 23 (11.1) | 208 | 24 (36.9) | 65 | <0.001 | 5 (71.4) | 7 | <0.001 | 19 (32.8) | 58 | <0.001 |
| Acute Respiratory Syndrome, n (%) | 4 (1.9) | 208 | 20 (32.8) | 61 | <0.001 | 1 (33.3) | 3 | 0.070 | 19 (32.8) | 58 | <0.001 |
| Acute renal injury/acute renal failure, n (%) | 6 (2.9) | 208 | 18 (17.3) | 104 | <0.001 | 2 (10.0) | 20 | 0.149 | 16 (19.0) | 84 | <0.001 |
| Multisystem Inflammatory Syndrome, Kawasaki-like disease, n (%) | 9 (10.8) | 83 | 1 (2.2) | 46 | 0.164 | 1 (33.3) | 3 | 0.361 | 0 (0.0) | 43 | 0.057 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Emes, D.; Hüls, A.; Baumer, N.; Dierssen, M.; Puri, S.; Russell, L.; Sherman, S.L.; Strydom, A.; Bargagna, S.; Brandão, A.C.; et al. COVID-19 in Children with Down Syndrome: Data from the Trisomy 21 Research Society Survey. J. Clin. Med. 2021, 10, 5125. https://doi.org/10.3390/jcm10215125
Emes D, Hüls A, Baumer N, Dierssen M, Puri S, Russell L, Sherman SL, Strydom A, Bargagna S, Brandão AC, et al. COVID-19 in Children with Down Syndrome: Data from the Trisomy 21 Research Society Survey. Journal of Clinical Medicine. 2021; 10(21):5125. https://doi.org/10.3390/jcm10215125
Chicago/Turabian StyleEmes, David, Anke Hüls, Nicole Baumer, Mara Dierssen, Shiela Puri, Lauren Russell, Stephanie L. Sherman, Andre Strydom, Stefania Bargagna, Ana Cláudia Brandão, and et al. 2021. "COVID-19 in Children with Down Syndrome: Data from the Trisomy 21 Research Society Survey" Journal of Clinical Medicine 10, no. 21: 5125. https://doi.org/10.3390/jcm10215125
APA StyleEmes, D., Hüls, A., Baumer, N., Dierssen, M., Puri, S., Russell, L., Sherman, S. L., Strydom, A., Bargagna, S., Brandão, A. C., Costa, A. C. S., Feany, P. T., Chicoine, B. A., Ghosh, S., Rebillat, A.-S., Sgandurra, G., Valentini, D., Rohrer, T. R., Levin, J., ... on behalf of the Trisomy 21 Research Society COVID-19 Initiative Study Group. (2021). COVID-19 in Children with Down Syndrome: Data from the Trisomy 21 Research Society Survey. Journal of Clinical Medicine, 10(21), 5125. https://doi.org/10.3390/jcm10215125