The Acute Effect of Exercise on Arterial Stiffness in Healthy Subjects: A Meta-Analysis

 ,
,  , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
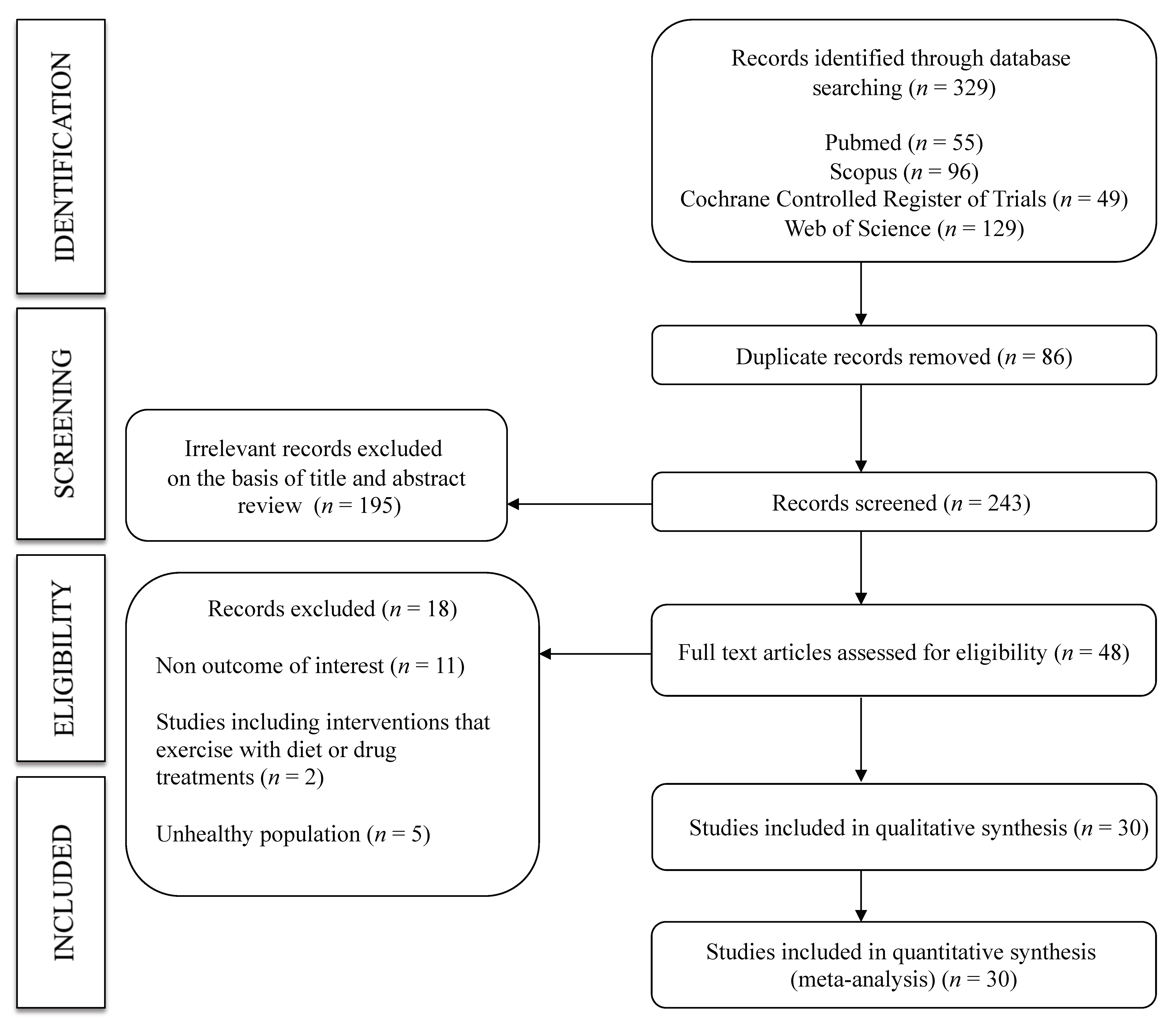
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction and Risk of Bias Assessment
2.4. Data Synthesis and Statistical Analysis
3. Results
3.1. Systematic Review
3.2. Risk of Bias
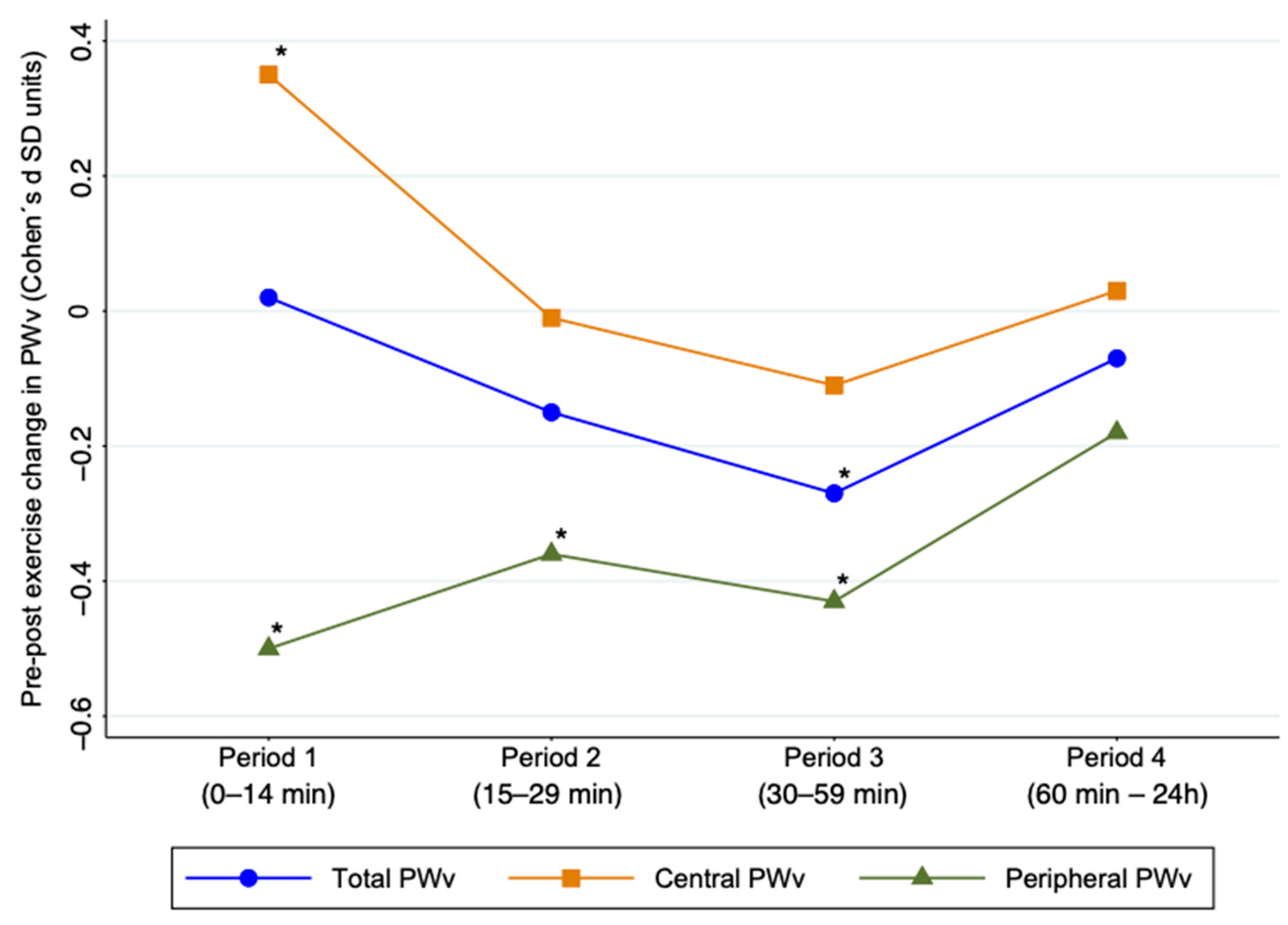
3.3. Meta-Analysis
3.4. Sensitivity Analysis
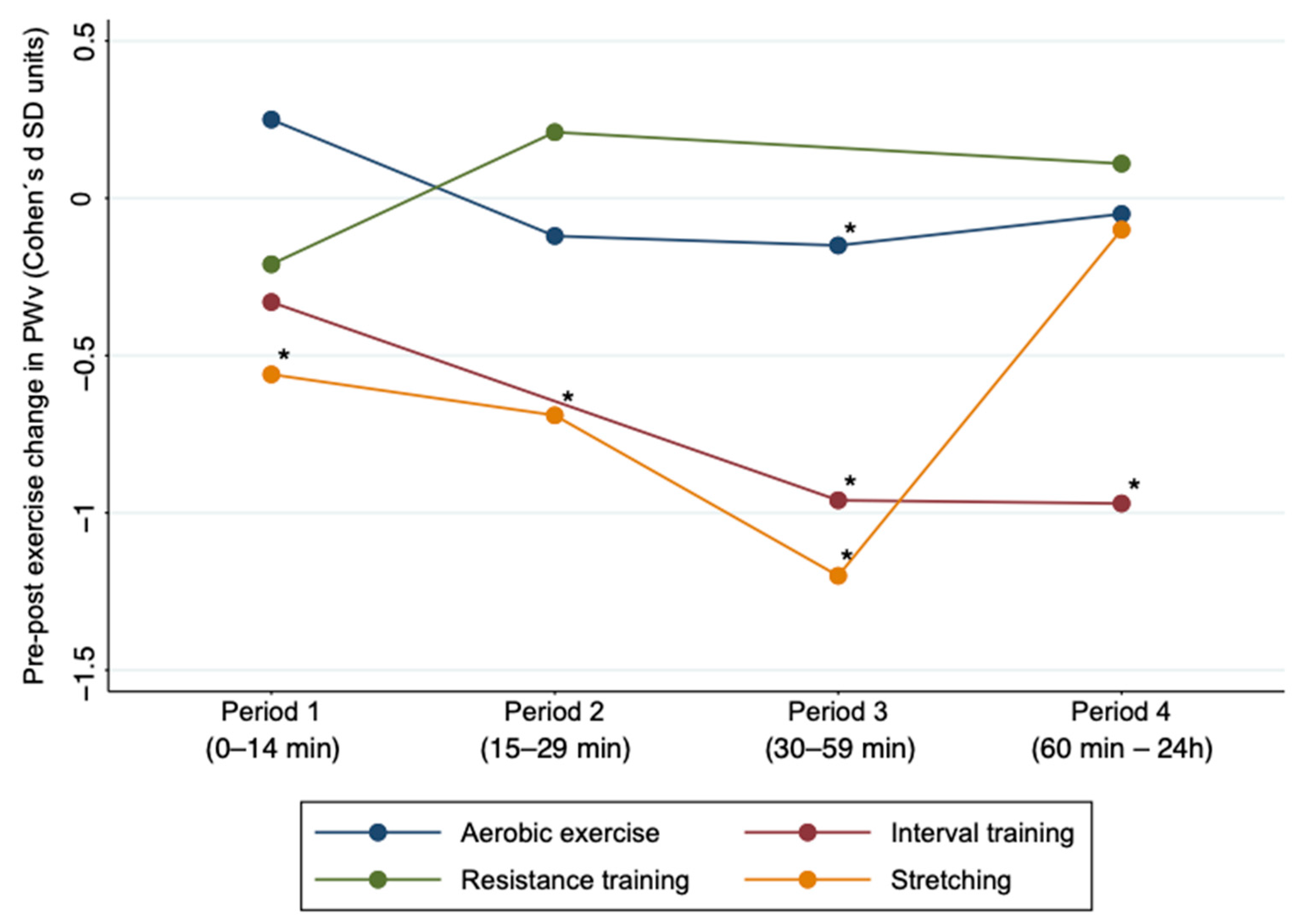
3.5. Subgroup Analyses and Meta-Regression
3.6. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Lee, J.G.; Joo, S.J. Arterial stiffness and cardiovascular risk. Korean J. Intern. Med. 2019, 34, 504–506. [Google Scholar]
- Shirwany, N.A.; Zou, M. Arterial stiffness: A brief review. Acta Pharmacol. Sin. 2010, 31, 1267–1276. [Google Scholar] [CrossRef]
- Tanaka, H.; Dinenno, F.A.; Monahan, K.D.; Clevenger, C.M.; DeSouza, C.A.; Seals, D.R. Aging, habitual exercise, and dynamic arterial compliance. Circulation 2000, 102, 1270–1275. [Google Scholar]
- Rajzer, M.W.; Wojciechowska, W.; Klocek, M.; Palka, I.; Brzozowska-Kiszka, M.; Kawecka-Jaszcz, K. Comparison of aortic pulse wave velocity measured by three techniques: Complior, SphygmoCor and Arteriograph. J. Hypertens. 2008, 26, 2001–2007. [Google Scholar]
- Amar, J.; Ruidavets, J.B.; Chamontin, B.; Drouet, L.; Ferrières, J. Arterial stiffness and cardiovascular risk factors in a population-based study. J. Hypertens. 2001, 19, 381–387. [Google Scholar]
- Laurent, S.; Cockcroft, J.; Van Bortel, L.; Boutouyrie, P.; Giannattasio, C.; Hayoz, D.; Pannier, B.; Vlachopoulos, C.; Wilkinson, I.; Struijker-Boudier, H. Expert consensus document on arterial stiffness: Methodological issues and clinical applications. Eur. Heart J. 2006, 27, 2588–2605. [Google Scholar]
- Nocon, M.; Hiemann, T.; Müller-Riemenschneider, F.; Thalau, F.; Roll, S.; Willich, S.N. Association of physical activity with all-cause and cardiovascular mortality: A systematic review and meta-analysis. Eur. J. Cardiovasc. Prev. Rehabil. 2008, 15, 239–246. [Google Scholar]
- Schuler, G.; Adams, V.; Goto, Y. Role of exercise in the prevention of cardiovascular disease: Results, mechanisms, and new perspectives. Eur. Heart J. 2013, 34, 1790–1799. [Google Scholar]
- Ashor, A.W.; Lara, J.; Siervo, M.; Celis-Morales, C.; Mathers, J.C. Effects of exercise modalities on arterial stiffness and wave reflection: A systematic review and meta-analysis of randomized controlled trials. PLoS ONE 2014, 9, e110034. [Google Scholar]
- Li, Y.; Hanssen, H.; Cordes, M.; Rossmeissl, A.; Endes, S.; Schmidt-Trucksäss, A. Aerobic, resistance and combined exercise training on arterial stiffness in normotensive and hypertensive adults: A review. Eur. J. Sport Sci. 2015, 15, 443–457. [Google Scholar] [CrossRef]
- Pierce, D.R.; Doma, K.; Leicht, A.S. Acute Effects of Exercise Mode on Arterial Stiffness and Wave Reflection in Healthy Young Adults: A Systematic Review and Meta-Analysis. Front. Physiol. 2018, 9. [Google Scholar] [CrossRef]
- Tabara, Y.; Yuasa, T.; Oshiumi, A.; Kobayashi, T.; Miyawaki, Y.; Miki, T.; Kohara, K. Effect of Acute and Long-Term Aerobic Exercise on Arterial Stiffness in the Elderly. Hypertens. Res. 2007, 30, 895–902. [Google Scholar]
- Kobayashi, R.; Hatakeyama, H.; Hashimoto, Y.; Okamoto, T. Acute effects of different aerobic exercise duration on pulse wave velocity in healthy young men. J. Sports Med. Phys. Fitness 2017, 57, 1695–1701. [Google Scholar] [CrossRef]
- Maeda, S.; Tanabe, T.; Otsuki, T.; Sugawara, J.; Ajisaka, R.; Matsuda, M. Acute exercise increases systemic arterial compliance after 6-month exercise training in older women. Hypertens. Res. 2008, 31, 377–381. [Google Scholar]
- Sugawara, J.; Komine, H.; Miyazawa, T.; Imai, T.; Ogoh, S. Influence of single bout of aerobic exercise on aortic pulse pressure. Eur. J. Appl. Physiol. 2015, 115, 739–746. [Google Scholar]
- Campbell, R.; Fisher, J.P.; Sharman, J.E.; McDonnell, B.J.; Frenneaux, M.P. Contribution of nitric oxide to the blood pressure and arterial responses to exercise in humans. J. Hum. Hypertens. 2011, 25, 262–270. [Google Scholar] [CrossRef]
- Ranadive, S.M.; Fahs, C.A.; Yan, H.; Rossow, L.M.; Agiovlasitis, S.; Fernhall, B. Comparison of the acute impact of maximal arm and leg aerobic exercise on arterial stiffness. Eur. J. Appl. Physiol. 2012, 112, 2631–2635. [Google Scholar] [CrossRef]
- Ribeiro, F.; Oliveira, N.L.; Pires, J.; Alves, A.J.; Oliveira, J. Treadmill walking with load carriage increases aortic pressure wave reflection. Rev. Port. Cardiol. 2014, 33, 425–430. [Google Scholar] [CrossRef]
- Fahs, C.A.; Heffernan, K.S.; Fernhall, B. Hemodynamic and vascular response to resistance exercise with l-arginine. Med. Sci. Sports Exerc. 2009, 41, 773–779. [Google Scholar] [CrossRef]
- Yoon, E.; Jung, S.; Cheun, S.; Oh, Y.; Kim, S.; Jae, S. Effects of acute resistance exercise on arterial stiffness in young men. Korean Circ. J. 2010, 40, 16–22. [Google Scholar] [CrossRef]
- Kingsley, J.D.P.D.; Mayo, X.M.S.; Tai, Y.L.M.S.; Fennell, C.M.S. Arterial stiffness and autonomic modulation following free-weight resistance exercises in resistance trained individuals. J. Strength Cond. Res. 2016, 30, 3373–3380. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar]
- Higgins, J.P.T.; Green, S. Selecting studies and collecting data. In Cochrane Handbook of Systematic Reviews of Interventions; Version 5.1.0.; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomized studies of interventions. BMJ 2016, 355, i4919. [Google Scholar]
- Kingwell, B.A.; Berry, K.L.; Cameron, J.D.; Jennings, G.L.; Dart, A.M. Arterial compliance increases after moderate-intensity cycling. Am. J. Physiol. 1997, 273, 2186–2191. [Google Scholar]
- Naka, K.K.; Tweddel, A.C.; Parthimos, D.; Henderson, A.; Goodfellow, J.; Frenneaux, M.P. Arterial distensibility: Acute changes following dynamic exercise in normal subjects. Am. J. Physiol. Heart Circ. Physiol. 2003, 284, 970–978. [Google Scholar]
- Sugawara, J.; Otsuki, T.; Tanabe, T.; Maeda, S.; Kuno, S.; Ajisaka, R.; Matsuda, M. The Effects of Low-Intensity Single-Leg Exercise on Regional Arterial Stiffness. Jpn. J. Physiol. 2003, 53, 239–241. [Google Scholar]
- Heffernan, K.S.; Rossow, L.; Jae, S.Y.; Shokunbi, H.G.; Gibson, E.M.; Fernhall, B. Effect of single-leg resistance exercise on regional arterial stiffness. Eur. J. Appl. Physiol. 2006, 98, 185–190. [Google Scholar] [CrossRef]
- Heffernan, K.S.; Jae, S.Y.; Echols, G.H.; Lepine, N.R.; Fernhall, B. Arterial Stiffness and Wave Reflection following Exercise in Resistance-Trained Men. Med. Sci. Sports Exerc. 2007, 39, 842–848. [Google Scholar] [CrossRef]
- Heffernan, K.S.; Jae, S.Y.; Edwards, D.G.; Kelly, E.E.; Fernhall, B. Arterial stiffness following repeated Valsalva maneuvers and resistance exercise in young men. Appl. Physiol. Nutr. Metab. 2007, 32, 257–264. [Google Scholar] [CrossRef]
- Heffernan, K.S.; Collier, S.R.; Kelly, E.E.; Jae, S.Y.; Fernhall, B. Arterial Stiffness and Baroreflex Sensitivity Following Bouts of Aerobic and Resistance Exercise. Int. J. Sports Med. 2007, 28, 197–203. [Google Scholar] [CrossRef]
- Barnes, J.N.; Trombold, J.R.; Dhindsa, M.; Lin, H.F.; Tanaka, H. Arterial stiffening following eccentric exercise-induced muscle damage. J. Appl. Physiol. 2010, 109, 1102–1108. [Google Scholar] [CrossRef]
- Tordi, N.; Mourot, L.; Colin, E.; Regnard, J. Intermittent versus constant aerobic exercise: Effects on arterial stiffness. Eur. J. Appl. Physiol. 2010, 108, 801–809. [Google Scholar] [CrossRef]
- Vlachopoulos, C.; Kardara, D.; Anastasakis, A.; Baou, K.; Terentes-Printzios, D.; Tousoulis, D.; Stefanadis, C. Arterial Stiffness and Wave Reflections in Marathon Runners. Am. J. Hypertens. 2010, 23, 974–979. [Google Scholar] [CrossRef]
- Doonan, R.J.; Scheffler, P.; Yu, A.; Egiziano, G.; Mutter, A.; Bacon, S.; Carli, F.; Daskalopoulos, M.E.; Daskalopoulou, S.S. Altered Arterial Stiffness and Subendocardial Viability Ratio in Young Healthy Light Smokers after Acute Exercise. PLoS ONE 2011, 6, e26151. [Google Scholar] [CrossRef]
- Hull, J.H.; Ansley, L.; Bolton, C.E.; Sharman, J.E.; Knight, R.K.; Cockcroft, J.R.; Shale, D.J.; Garrod, R. The effect of exercise on large artery haemodynamics in cystic fibrosis. J. Cyst. Fibros 2011, 10, 121–127. [Google Scholar] [CrossRef]
- McClean, C.M.; Clegg, M.; Shafat, A.; Murphy, M.H.; Trinick, T.; Duly, E.; McLaughlin, J.; Fogarty, M.; Davison, G.W. The Impact of Acute Moderate Intensity Exercise on Arterial Regional Stiffness, Lipid Peroxidation, and Antioxidant Status in Healthy Males. Res. Sports Med. 2011, 19, 1–13. [Google Scholar] [CrossRef]
- Lane, A.D.; Ranadive, S.M.; Yan, H.; Kappus, R.M.; Cook, M.D.; Sun, P.; Woods, J.A.; Wilund, K.; Fernhall, B. Effect of Sex on Wasted Left Ventricular Effort Following Maximal Exercise. Int. J. Sports Med. 2013, 34, 770–776. [Google Scholar] [CrossRef]
- Burr, J.F.; Boulter, M.; Beck, K. Arterial stiffness results from eccentrically biased downhill running exercise. J. Sci. Med. Sport 2014. [Google Scholar] [CrossRef]
- Jatoi, N.A.; Kyvelou, S.M.; Feely, J. The acute effects of mental arithmetic, cold pressor and maximal voluntary contraction on arterial stiffness in young healthy subjects. Artery Res. 2014, 8, 44–50. [Google Scholar] [CrossRef]
- Sun, P.; Yan, H.; Ranadive, S.M.; Lane, A.D.; Kappus, R.M.; Bunsawat, K.; Baynard, T.; Li, S.; Fernhall, B. Blood Pressure Changes Following Aerobic Exercise in Caucasian and Chinese Descendants. Int. J. Sports Med. 2015, 36, 189–196. [Google Scholar] [CrossRef]
- Lefferts, W.K.; Heffernan, K.S.; Hultquist, E.M.; Fehling, P.C.; Smith, D.L. Vascular and central hemodynamic changes following exercise-induced heat stress. Vasc. Med. 2015, 20, 222–229. [Google Scholar] [CrossRef]
- Perdomo, S.J.; Moody, A.M.; McCoy, S.M.; Barinas-Mitchell, E.; Jakicic, J.M.; Gibbs, B.B. Effects on carotid–femoral pulse wave velocity 24h post exercise in young healthy adults. Hypertens. Res. 2016. [Google Scholar] [CrossRef]
- Siasos, G.; Athanasiou, D.; Terzis, G.; Stasinaki, A.; Oikonomou, E.; Tsitkanou, S.; Kolokytha, T.; Spengos, K.; Papavassiliou, A.G.; Tousoulis, D. Acute effects of different types of aerobic exercise on endothelial function and arterial stiffness. Eur. J. Prev. Cardiol. 2016, 23, 1565–1572. [Google Scholar] [CrossRef]
- Yamato, Y.; Hasegawa, N.; Sato, K.; Hamaoka, T.; Ogoh, S.; Iemitsu, M. Acute effect of static stretching exercise on arterial stiffness in healthy young adults. Am. J. Phys. Med. Rehabil. 2016, 95, 764–770. [Google Scholar] [CrossRef]
- Kingsley, J.D.; Tai, Y.L.; Vaughan, J.A.; Mayo, X. High-intensity interval cycling exercise on wave reflection and pulse wave velocity. J. Strength Cond. Res. 2017, 31, 1313–1320. [Google Scholar]
- Yamato, Y.; Haseqawa, N.; Fujie, S.; Ogoh, S.; Iemitsu, M. Acute effect of stretching one leg on regional arterial stiffness in young men. Eur. J. Appl. Physiol. 2017, 117, 1227–1232. [Google Scholar] [CrossRef]
- Logan, J.G.; Kim, S.S.; Lee, M.; Byon, H.D.; Yeo, S. Effects of Static Stretching Exercise on Lumbar Flexibility and Central Arterial Stiffness. J. Cardiovasc. Nurs. 2018, 33, 322–328. [Google Scholar]
- Okamoto, T.; Min, S.K.; Sakamaki-Sunaga, M. Acute Effect of Interval Walking on Arterial Stiffness in Healthy Young Adults. Int. J. Sports Med. 2018, 39, 495–501. [Google Scholar] [CrossRef]
- Peres, D.; Mourot, L.; Ménétrier, A.; Bouhaddi, M.; Degano, B.; Regnard, J.; Tordi, N. Intermittent versus constant aerobic exercise in middle-aged males: Acute effects on arterial stiffness and factors influencing the changes. Eur. J. Appl. Physiol. 2018, 118, 1625–1633. [Google Scholar] [CrossRef]
- Tomschi, F.; Ottmann, H.; Latsch, J.; Predel, H.G.; Bloch, W.; Grau, M. Does the acute hemodynamic response to a maximum running exercise depend on the aerobic training status of the subjects? Artery Res. 2018, 23, 28–31. [Google Scholar] [CrossRef]
- Perdomo, S.J.; Balzer, J.R.; Jakicic, J.M.; Kline, C.E.; Gibbs, B.B. Acute effects of aerobic exercise duration on blood pressure, pulse wave velocity and cerebral blood flow velocity in middle-aged adults. Sport Sci. Health 2019, 15, 647–658. [Google Scholar] [CrossRef]
- Schroeder, E.C.; Ranadive, S.M.; Yan, H.; Lane-Cordova, A.D.; Kappus, R.M.; Cook, M.D.; Fernhall, B. Effect of acute maximal exercise on vasodilatory function and arterial stiffness in African-American and white adults. J. Hypertens. 2019, 37, 1262–1268. [Google Scholar] [CrossRef]
- DerSimonian, R.; Kacker, R. Random-effects model for meta-analysis of clinical trials: An update. Contemp. Clin. Trials 2007, 28, 105–114. [Google Scholar]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a metaanalysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar]
- Sterne, J.A.; Egger, M.; Smith, G.D. Systematic reviews in health care: Investigating and dealing with publication and other biases in meta-analysis. BMJ 2001, 323, 101–105. [Google Scholar]
- Green, D.J.; Hopman, M.T.; Padilla, J.; Laughlin, M.H.; Thijssen, D.H. Vascular Adaptation to Exercise in Humans: Role of Hemodynamic Stimuli. Physiol. Rev. 2017, 97, 495–528. [Google Scholar]
- Nystoriak, M.A.; Bhatnagar, A. Cardiovascular effects and benefits of exercise. Front. Cardiovasc. Med. 2018, 5, 135. [Google Scholar]
- Matsumoto, A.; Hirata, Y.; Momomura, S.; Fujita, H.; Yao, A.; Sata, M.; Serizawa, T. Increased nitric oxide production during exercise. Lancet 1994, 343, 849–850. [Google Scholar]
- Roberts, C.K.; Barnard, R.J.; Jasman, A.; Balon, T.W. Acute exercise increases nitric oxide synthase activity in skeletal muscle. Am. J. Physiol. 1999, 277, 390–394. [Google Scholar]
- Endo, T.; Imaizumi, T.; Tagawa, M.; Shiramoto, S.; Ando, S.; Takeshita, A. Role of nitric oxide in exercise-induced vasodilation of the forearm. Circulation 1994, 90, 2886–2890. [Google Scholar]
- Wilson, J.; Kapoor, S. Contribution of endothelium-derived relaxing factor to exercise-induced vasodilation in humans. J. Appl. Physiol. 1993, 75, 2740–2744. [Google Scholar]
- Sarelius, I.; Pohl, U. Control of muscle blood flow during exercise: Local factors and integrative mechanisms. Acta Physiol. 2010, 199, 349–365. [Google Scholar]
- Laughlin, M.H.; Yang, H.T.; Tharp, D.L.; Rector, R.S.; Padilla, J.; Bowles, D.K. Vascular cell transcriptomic changes to exercise training differ directionally along and between skeletal muscle arteriolar trees. Microcirculation 2017, 24, e12336. [Google Scholar]
- Nichols, W.W.; Singh, B.M. Augmentation index as a measure of peripheral vascular disease state. Curr. Opin. Cardiol. 2002, 17, 543–551. [Google Scholar]
- Gkaliagkousi, E.; Douma, S. The pathogenesis of arterial stiffness and its prognostic value in essential hypertension and cardiovascular diseases. Hippokratia 2009, 13, 70–75. [Google Scholar]
- Nagao, T.; Vanhoutte, P.M. Endothelium-derived hyperpolarizing factor and endothelium-dependent relaxations. Am. J. Respir. Cell Mol. Biol. 1993, 8, 1–6. [Google Scholar]
- Trachsel, Y.; Herzig, D.; Marcin, T.; Zenger, N.; Dysli, M.; Trachsel, L.D.; Wilhelm, M.; Eser, P. Response of peripheral arterial pulse wave velocity to acute exercise in patients after recent myocardial infarction and healthy controls. PLoS ONE 2019, 14, e0219146. [Google Scholar] [CrossRef]
- Spronck, B.; Heusinkveld, M.H.G.; Vanmolkot, F.H.; Roodt, J.O.; Hermeling, E.; Delhaas, T.; Kroon, A.A.; Reesink, K.D. Pressure-dependence of arterial stiffness: Potential clinical implications. J. Hypertens. 2015, 33, 330–338. [Google Scholar] [CrossRef]
- Van Hoof, R.; Hespel, P.; Fagard, R.; Lijnen, P.; Staessen, J.; Amery, A. Effect of Endurance Training on Blood Pressure at Rest, During Exercise and During 24 Hours in Sedentary Men. Am. J. Cardiol. 1989, 63, 945–949. [Google Scholar]
- Clegg, M.; McClean, C.; Davison, W.G.; Murphy, H.M.; Trinick, T.; Duly, E.; McLaughlin, J.; Fogarty, M.; Shafat, A. Exercise and postprandial lipaemia: Effects on peripheral vascular function, oxidative stress and gastrointestinal transit. Lipids Health Dis. 2007, 6. [Google Scholar] [CrossRef]
- McClean, C.M.; McLaughlin, J.; Burke, G.; Murphy, M.H.; Trinick, T.; Duly, E.; Davison, G.W. The effect of acute aerobic exercise on pulse wave velocity and oxidative stress following postprandial hypertriglyceridemia in healthy men. Eur. J. Appl. Physiol. 2007, 100, 225–234. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Reference | Country | Study Design | Population Characteristics | Outcome (Arterial Stiffness: PWv) | Exercise Intervention | ||||
|---|---|---|---|---|---|---|---|---|---|
| Sample Size (n) | Age (Years) | Type of PWv | Basal PWv (m/s) | Assessment Time Points | Method Used | ||||
| Kingwell et al., 1997 [26] | Australia | Crossover | 12 | 24.0 ± 6.0 | cf-PWv fd-PWv | 6.2 ± 1.4 8.3 ± 1.0 | Baseline and 30 min post | Doppler flow velocimeter | AE |
| Naka et al., 2003 [27] | UK | Non randomized CT | 25 | 31.0 ± 6.0 | ba-PWv | 7.6 ± 1.1 | Baseline and 60 min post | QVL SciMed | AE |
| Sugawara et al., 2003 [28] | Japan | Non randomized CT | 18 | 24.0 ± 4.2 | fa-PWv | 9.1 ± 1.3 | Baseline and 2 min post | Form PWV/ABI | AE |
| Heffernan et al., 2006 [29] | USAs | Non randomized CT | 13 | 21.5 ± 2.5 | cf-PWv fd-PWv | 6.1 ± 1.1 7.9 ± 1.1 | Baseline, 5 min and 25 min post | Task Force III | RT |
| Heffernan et al., 2007 (a) [30] | USAs | Non randomized CT | 15 | 21.9 ± 2.3 | cf-PWv | 6.4 ± 1.6 | Baseline, 10 min, 20 min and 30 min post | SphygmoCor | AE |
| Heffernan et al., 2007 (b) [31] | USAs | Non randomized CT | 14 | 27.9 ± 7.5 | cf-PWv fd-PWv | 7.2 ± 1.1 8.5 ± 0.8 | Baseline and 20 min post | SphygmoCor | RT |
| Heffernan et al., 2007 (c) [32] | USAs | Non randomized CT | 13 | 25.0 ± 2.5 | cf-PWv fd-PWv | Session 1: 5.3 ± 0.6; Session 2: 4.8 ± 1.1 Session 1: 8.9 ± 0.9; Session 2: 8.7 ± 1.2 | Baseline and 20 min post | Doppler flow velocimeter | Session 1: AE Session 2: RT |
| Barnes et al., 2010 [33] | USAs | Crossover | G1: 11 G2: 16 | G1: 25.0 ± 3.3 G2: 24.0 ± 1.9 | cf-PWv | G1: 7.9 ± 1.0 G2: 7.6 ± 1.0 | Baseline, 90 min and 24 h post | Colin VP-2000 | RT |
| Tordi et al., 2010 [34] | France | Non randomized CT | 11 | 22.5 ± 2.3 | cd-PWv | Session 1: 8.6 ± 0.3 Session 2: 8.7 ± 0.7 | Baseline and 30 min post | Complior | Session 1: IT Session 2: AE |
| Vlachopoulos et al., 2010 [35] | Greece | Non randomized CT | 20 | 36.0 ± 10.0 | cf-PWv | 6.7 ± 0.9 | Baseline and 0 min post | Complior | AE |
| Doonan et al., 2011 [36] | Canada | Non randomized CT | G1: 53 G2: 24 | G1: 23.1 ± 5.4 G2: 26.0 ± 6.7 | cf-PWv | G1: 6.0 ± 0.7 G2: 6.3 ± 1.0 | Baseline, 2 min, 5 min, 10 min and 15min post | SphygmoCor | AE |
| Hull et al., 2011 [37] | UK | Non randomized CT | 36 | 28.9 ± 9.0 | cf-PWv | 6.2 ± 1.6 | Baseline and 0 min post | SphygmoCor | AE |
| McClean et al., 2011 [38] | Ireland | Crossover | 8 | 22.9 ± 2.8 | br-PWv | 7.1 ± 1.8 | Baseline and 0 min post | Sensor based PWV device | AE |
| Lane et al., 2012 [39] | USAs | Non randomized CT | G1: 31 G2: 31 | G1: 24.7 ± 3.3 G2: 24.8 ± 3.3 | cf-PWv fd-PWv | G1: 6.1 ± 1.2; G2: 5.5 ± 0.8 G1: 8.7 ± 1.7; G2: 8.1 ± 1.7 | Baseline, 15 min and 30 min post | SphygmoCor | AE |
| Ranadive et al., 2012 [17] | USAs | Crossover | 15 | 25.0 ± 5.0 | cr-PWv cf-PWv fd-PWv | Session 1: 7.0 ± 0.8; Session 2: 6.6 ± 1.2 Session 1: 5.5 ± 1.2; Session 2: 5.6 ± 1.12 Session 1: 9.1 ± 1.9; Session 2: 8.7 ± 1.9 | Baseline and 10 min post | SphygmoCor | Session 1: AE Session 2: AE |
| Burr et al., 2014 [40] | Canada | Non randomized CT | 13 | 25.0 ± 6.0 | cf-PWv | 5.1 ± 0.6 | Baseline, 10 min, 6 and 24 h post | SphygmoCor | AE |
| Jatoi et al., 2014 [41] | Saudi Arabia | Non randomized CT | 23 | 23.0 ± 3.0 | a-PWv | 6.8 ± 0.9 | Baseline, 5 min and 10 min post | Arteriograph | RT |
| Sun et al., 2014 [42] | China | Non randomized CT | G1: 32 G2: 30 | G1: 28.0 ± 4.0 G2: 24.0 ± 4.0 | cr-PWv cf-PWv fa-PWv | G1: 7.0 ± 1.0; G2: 7.1 ± 1.0 G1: 5.6 ± 1.1;G2: 5.6 ± 1.0 G1: 8.2 ± 1.2; G2: 8.9 ± 1.3 | Baseline, 30 min and 60 min post | SphygmoCor | AE |
| Lefferts et al., 2015 [43] | USAs | Non randomized CT | 12 | 22.0 ± 3.0 | cf-PWv | G1: 5.0 ± 0.4 G2: 5.0 ± 0.4 | Baseline and 15 min post | SphygmoCor | AE |
| Perdomo et al., 2016 [44] | USAs | Non randomized CT | 30 | 23.8 ± 2.5 | cf-PWv | 6.1 ± 0.8 | Baseline and 24 h post | Complior | AE |
| Siasos et al., 2016 [45] | Greece | Crossover | 20 | 22.6 ± 3.3 | cf-PWv fd-PWv | Session 1: 5.9 ± 0.7; Session 2: 5.9 ± 0.8 Session 1: 9.1 ± 1.1; Session 2: 9.2 ± 1.1 | Baseline and 10 min post | SphygmoCor | Session 1: IT Session 2: AE |
| Yamato et el., 2016 [46] | Japan | Non randomized CT | 26 | 21.0 ± 5.1 | ba-PWv cf-PWv fa-PWv | NA NA NA | Baseline, 0, 15, 30 and 60 min post | Form PWV/ABI | S |
| Kingsley et al., 2017 [47] | USAs | Non randomized CT | 9 | 22.0 ± 2.0 | cf-PWv | 5.3 ± 0.8 | Baseline and 5 min post | SphygmoCor | IT |
| Yamato et al., 2017 [48] | Japan | Non randomized CT2 | 25 | 20.9 ± 1.5 | fa-PWv | 8.4 ± 0.8 | Baseline, o and 15 min post | Form PWV/ABI | S |
| Logan et al., 2018 [49] | USAs | Non randomized CT | 30 | 44.4 ± 10.9 | cf-PWv | 6.9 ± 1.5 | Baseline and 5 min post | SphygmoCor | S |
| Okamoto et al., 2018 [50] | Japan | Non randomized CT | 14 | 27.5 ± 3.7 | fa-PWv | Session 1: 8.5 ± 0.9 Session 2: 8.6 ± 0.7 | Baseline, 30 min and 60 min post | Form PWV/ABI | Session 1: IT Session 2: AE |
| Peres at al., 2018 [51] | France | Non randomized CT | 15 | 48.5 ± 5.04 | cr-PWv cf-PWv fd-PWv | Session 1: 8.2 ± 1.6; Session 2: 8.2 ± 1.9 Session 1: 9.3 ± 1.9; Session 2: 9.0 ± 1.6 Session 1: 9.1 ± 1.9; Session 2: 10.2 ± 2.7 | Baseline and 5 min post | SPT-301 | Session 1: IT Session 2: AE |
| Tomschi et al., 2018 [52] | Germany | Non randomized CT | G1: 21 G2: 20 | G1: 23.3 ± 3.2 G2: 23.2 ± 2.3 | a-PWv | IG1: 5.0 ± 0.4 IG2: 4.9 ± 0.4 | Baseline and 0 min post | Mobil-O-Graph | AE |
| Perdomo et al., 2019 [53] | USAs | Crossover | 15 | 45.4 ± 8.9 | cr-PWv cf-PWv | Session 1: 8.5 ± 1.5; Session 2: 8.7 ± 1.4 Session 1: 6.8 ± 0.7; Session 2: 6.9 ± 0.76 | Baseline, 30 min and 60 min post | Complior | Session 1: AE Session 2: AE |
| Schroeder et al., 2019 [54] | USAs | Non randomized CT | G1: 27 G2: 35 | G1: 25.0 ± 4.0 G2: 24.0 ± 4.0 | cf-PWv | G1: 5.8 ± 1.1 G2: 5.9 ± 1.1 | Baseline, 15 min and 30 min post | SphygmoCor | AE |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saz-Lara, A.; Cavero-Redondo, I.; Álvarez-Bueno, C.; Notario-Pacheco, B.; Ruiz-Grao, M.C.; Martínez-Vizcaíno, V. The Acute Effect of Exercise on Arterial Stiffness in Healthy Subjects: A Meta-Analysis. J. Clin. Med. 2021, 10, 291. https://doi.org/10.3390/jcm10020291
Saz-Lara A, Cavero-Redondo I, Álvarez-Bueno C, Notario-Pacheco B, Ruiz-Grao MC, Martínez-Vizcaíno V. The Acute Effect of Exercise on Arterial Stiffness in Healthy Subjects: A Meta-Analysis. Journal of Clinical Medicine. 2021; 10(2):291. https://doi.org/10.3390/jcm10020291
Chicago/Turabian StyleSaz-Lara, Alicia, Iván Cavero-Redondo, Celia Álvarez-Bueno, Blanca Notario-Pacheco, Marta Carolina Ruiz-Grao, and Vicente Martínez-Vizcaíno. 2021. "The Acute Effect of Exercise on Arterial Stiffness in Healthy Subjects: A Meta-Analysis" Journal of Clinical Medicine 10, no. 2: 291. https://doi.org/10.3390/jcm10020291
APA StyleSaz-Lara, A., Cavero-Redondo, I., Álvarez-Bueno, C., Notario-Pacheco, B., Ruiz-Grao, M. C., & Martínez-Vizcaíno, V. (2021). The Acute Effect of Exercise on Arterial Stiffness in Healthy Subjects: A Meta-Analysis. Journal of Clinical Medicine, 10(2), 291. https://doi.org/10.3390/jcm10020291