
Biological Characterization of Human Autologous Pericardium Treated with the Ozaki Procedure for Aortic Valve Reconstruction



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Collection and Processing
2.2. Histological Analyisis
2.3. SEM
2.4. MTT Assay
2.5. Live/Dead Assay
2.6. Nuclear Morpholgy Analysis
2.7. Cytotoxicity Assay
2.8. Cell Seeding onto Pericardium Samples and Biomarkers Analysis
2.9. Statistical Analysis
3. Results
3.1. The Ozaki Procedure Alters the Arrangement of Collagen and Elastic Fibers in the ECM
3.2. The Ozaki Procedure Triggers Cell Death in Pericardium
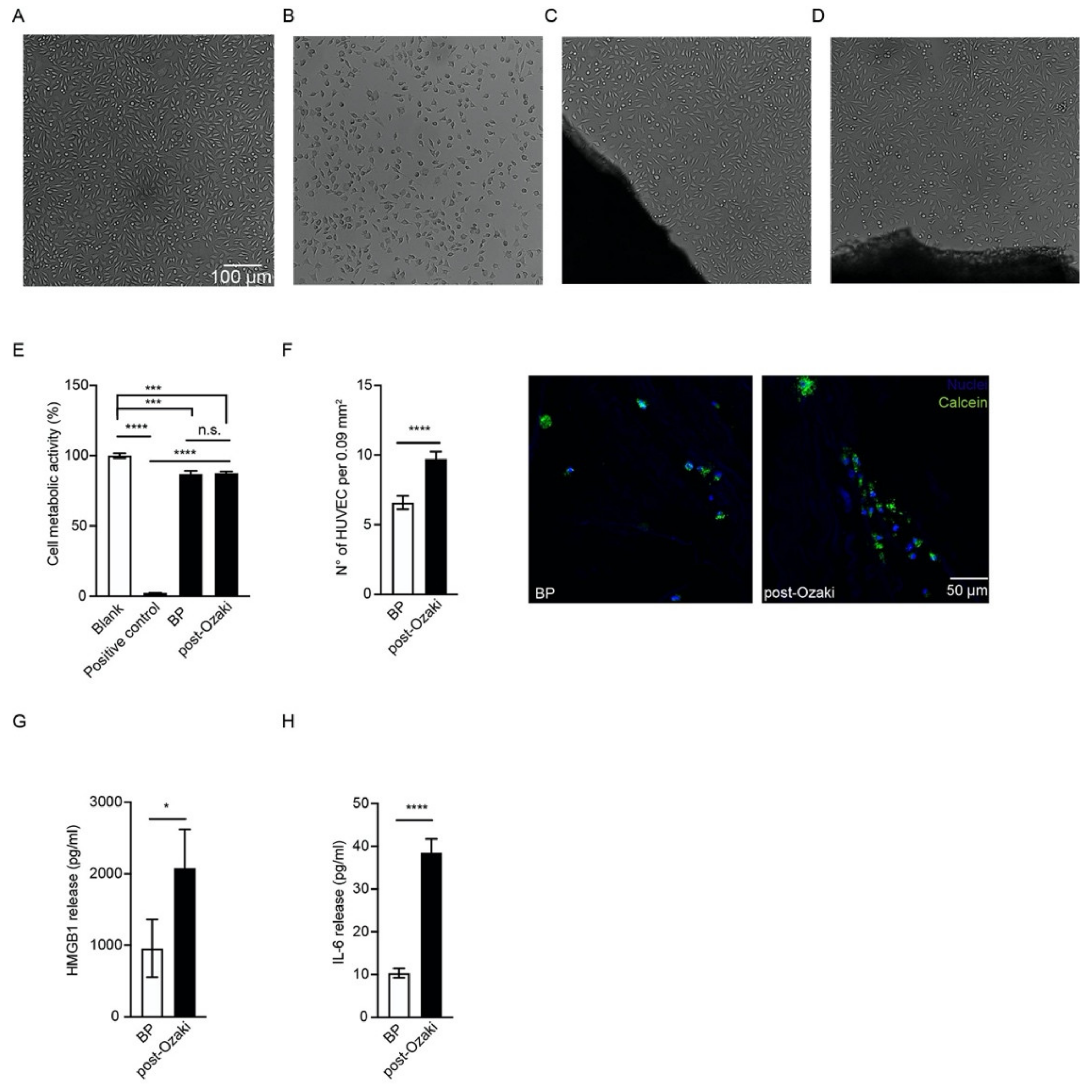
3.3. The Ozaki Procedure Is Not Toxic and Allows for Endothelial Cell Repopulation In Vitro
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bjoerk, V.O.; Hultquist, G. Teflon and Pericardial Aortic Valve Prostheses. J. Thorac. Cardiovasc. Surg. 1964, 47, 693–701. [Google Scholar] [CrossRef]
- Bahnson, H.T.; Hardesty, R.L.; Baker, L.D.; Brooks, D.H.; Gall, D.A. Fabrication and Evaluation of Tissue Leaflets for Aortic and Mitral Valve Replacement. Ann. Surg. 1970, 171, 939–947. [Google Scholar] [CrossRef]
- Love, J.; Calvin, J.; Phelan, R.; Love, C. Rapid intra-operative fabrication of an autogenous tissue heart valve: A new technique. In Proceedings of the Third International Symposium on Cardiac Bioprostheses; Bodnar, E., Yacoub, M., Eds.; Yorke Medical Books: New York, NY, USA, 1986; pp. 691–698. [Google Scholar]
- Duran, C.M.; Gometza, B.; Kumar, N.; Gallo, R.; Martin-Duran, R. Aortic valve replacement with freehand autologous pericardium. J. Thorac. Cardiovasc. Surg. 1995, 110, 511–516. [Google Scholar] [CrossRef]
- Ozaki, S.; Kawase, I.; Yamashita, H.; Uchida, S.; Nozawa, Y.; Matsuyama, T.; Takatoh, M.; Hagiwara, S. Aortic valve reconstruction using self-developed aortic valve plasty system in aortic valve disease. Interact. Cardiovasc. Thorac. Surg. 2011, 12, 550–553. [Google Scholar] [CrossRef]
- Talwar, S.; Das, A.; Siddarth, B.; Choudhary, S.K.; Airan, B. Patch materials for right ventricular outflow reconstruction: Past, present, and future. Indian J. Thorac. Cardiovasc. Surg. 2019, 35, 41–50. [Google Scholar] [CrossRef]
- Maizato, M.J.; Higa, O.Z.; Mathor, M.B.; Camillo, M.A.; Spencer, P.J.; Pitombo, R.N.; Zavaglia, C.A.; Leirner, A.A. Glutaraldehyde-treated Bovine Pericardium: Effects of Lyophilization on Cytotoxicity and Residual Aldehydes. Artif. Organs 2003, 27, 692–694. [Google Scholar] [CrossRef]
- Simionescu, D.T. Prevention of calcification in bioprosthetic heart valves: Challenges and perspectives. Expert Opin. Biol. Ther. 2004, 4, 1971–1985. [Google Scholar] [CrossRef] [PubMed]
- Schoen, F.J.; Levy, R.J. Calcification of Tissue Heart Valve Substitutes: Progress Toward Understanding and Prevention. Ann. Thorac. Surg. 2005, 79, 1072–1080. [Google Scholar] [CrossRef] [PubMed]
- Pedriali, G.; Morciano, G.; Patergnani, S.; Cimaglia, P.; Morelli, C.; Mikus, E.; Ferrari, R.; Gasbarro, V.; Giorgi, C.; Wieckowski, M.R.; et al. Aortic Valve Stenosis and Mitochondrial Dysfunctions: Clinical and Molecular Perspectives. Int. J. Mol. Sci. 2020, 21, 4899. [Google Scholar] [CrossRef]
- Ozaki, S.; Kawase, I.; Yamashita, H.; Uchida, S.; Takatoh, M.; Kiyohara, N. Midterm outcomes after aortic valve neocuspidization with glutaraldehyde-treated autologous pericardium. J. Thorac. Cardiovasc. Surg. 2018, 155, 2379–2387. [Google Scholar] [CrossRef] [PubMed]
- Ozaki, S. Ozaki Procedure: 1100 patients with up to 12 years of follow-up. Turk. J. Thorac. Cardiovasc. Surg. 2019, 27, 454. [Google Scholar] [CrossRef]
- Roussakis, A.; Calvi, S.; Raviola, E.; Albertini, A. Patient with Unicuspid Aortic Valve and Ascending Aorta Aneurysm Treated with Ozaki Procedure and Ascending Aorta Replacement. Braz. J. Cardiovasc. Surg. 2021, 36, 125–129. [Google Scholar] [CrossRef]
- Schindelin, J.; Arganda-Carreras, I.; Frise, E.; Kaynig, V.; Longair, M.; Pietzsch, T.; Preibisch, S.; Rueden, C.; Saalfeld, S.; Schmid, B.; et al. Fiji: An open-source platform for biological-image analysis. Nat. Methods 2012, 9, 676–682. [Google Scholar] [CrossRef]
- Gardin, C.; Bosco, G.; Ferroni, L.; Quartesan, S.; Rizzato, A.; Tatullo, M.; Zavan, B. Hyperbaric Oxygen Therapy Improves the Osteogenic and Vasculogenic Properties of Mesenchymal Stem Cells in the Presence of Inflammation In Vitro. Int. J. Mol. Sci. 2020, 21, 1452. [Google Scholar] [CrossRef]
- ISO. ISO-10993-5. Biological Evaluation of Medical Devices, Part 5: Tests for in Vitro Cytotoxicity. ISO Central Secretaria: Geneva, Switzerland, 2009. [Google Scholar]
- Cummings, B.S.; Schnellmann, R.G.; Wills, L.P. Measurement of Cell Death in Mammalian Cells. Curr. Protoc. Pharmacol. 2004, 25, 12.8.1–12.8.22. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, H.; Ozaki, S.; Iwasaki, K.; Kawase, I.; Nozawa, Y.; Umezu, M. Tensile Strength of Human Pericardium Treated with Glutaraldehyde. Ann. Thorac. Cardiovasc. Surg. 2012, 18, 434–437. [Google Scholar] [CrossRef]
- Grefen, L.; König, F.; Grab, M.; Hagl, C.; Thierfelder, N. Pericardial tissue for cardiovascular application: An in-vitro evaluation of established and advanced production processes. J. Mater. Sci. Mater. Med. 2018, 29, 172. [Google Scholar] [CrossRef] [PubMed]
- Masson-Meyers, D.; Bumah, V.V.; Enwemeka, C.S. A comparison of four methods for determining viability in human dermal fibroblasts irradiated with blue light. J. Pharmacol. Toxicol. Methods 2016, 79, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Fotakis, G.; Timbrell, J.A. In vitro cytotoxicity assays: Comparison of LDH, neutral red, MTT and protein assay in hepatoma cell lines following exposure to cadmium chloride. Toxicol. Lett. 2006, 160, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Lalande, M.E.; Ling, V.; Miller, R.G. Hoechst 33342 dye uptake as a probe of membrane permeability changes in mammalian cells. Proc. Natl. Acad. Sci. USA 1981, 78, 363–367. [Google Scholar] [CrossRef]
- Lopez-Moya, M.; Melgar-Lesmes, P.; Kolandaivelu, K.; Hernández, J.M.D.L.T.; Edelman, E.R.; Balcells, M. Optimizing Glutaraldehyde-Fixed Tissue Heart Valves with Chondroitin Sulfate Hydrogel for Endothelialization and Shielding against Deterioration. Biomacromolecules 2018, 19, 1234–1244. [Google Scholar] [CrossRef] [PubMed]
- Polak, R.; Rodas, A.C.; Chicoma, D.L.; Giudici, R.; Beppu, M.M.; Higa, O.Z.; Pitombo, R.N. Inhibition of calcification of bovine pericardium after treatment with biopolymers, E-beam irradiation and in vitro endothelization. Mater. Sci. Eng. C 2013, 33, 85–90. [Google Scholar] [CrossRef]
- Lee, W.K.; Park, K.D.; Han, D.K.; Suh, H.; Park, J.-C.; Kim, Y.H. Heparinized bovine pericardium as a novel cardiovascular bioprosthesis. Biomaterials 2000, 21, 2323–2330. [Google Scholar] [CrossRef]
- Chachques, J.C.; Gardin, C.; Lila, N.; Gasbarro, V.; Lila, N.; Ferroni, L.; Migonney, V.; Falentin-Daudre, C.; Zanotti, F.; Trentini, M.; et al. Elastomeric cardiowrap scaffolds functionalized with mesenchymal stem cells-derived exosomes induce a positive modlation in the inflammatory and wound healing response of mesenchymal stem cell and macrophage. Biomedicines 2021, 7, 824. [Google Scholar] [CrossRef]
- Toeg, H.D.; Abessi, O.; Al-Atassi, T.; de Kerchove, L.; El-Khoury, G.; Labrosse, M.; Boodhwani, M. Finding the ideal biomaterial for aortic valve repair with ex vivo porcine left heart simulator and finite element modeling. J. Thorac. Cardiovasc. Surg. 2014, 148, 1739–1745. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Blum, K.M.; Drews, J.D.; Breuer, C.K. Tissue-Engineered Heart Valves: A Call for Mechanistic Studies. Tissue Eng. Part B Rev. 2018, 24, 240–253. [Google Scholar] [CrossRef]
- Barros, J.A.G.; Filippin-Monteiro, F.; De Oliveira, E.M.; Campa, A.; Catalani, L.H.; Pitombo, R.D.N.M.; Polakiewicz, B. Cytotoxicity of PVPAC-treated bovine pericardium: A potential replacement for glutaraldehyde in biological heart valves. J. Biomed. Mater. Res. Part B Appl. Biomater. 2013, 102, 574–582. [Google Scholar] [CrossRef]
- Shklover, J.; McMasters, J.; Alfonso-Garcia, A.; Higuita, M.L.; Panitch, A.; Marcu, L.; Griffiths, L. Bovine pericardial extracellular matrix niche modulates human aortic endothelial cell phenotype and function. Sci. Rep. 2019, 9, 16688. [Google Scholar] [CrossRef]
- Lei, L.; Tao, X.; Xie, L.; Hong, Z. Vascular endothelial growth factor-loaded elastin-hydrogel modification of the pericardium improves endothelialization potential of bioprosthetic heart valves. J. Biomater. Appl. 2019, 34, 451–459. [Google Scholar] [CrossRef]
- Feugier, P.; Black, R.; Hunt, J.; How, T. Attachment, morphology and adherence of human endothelial cells to vascular prosthesis materials under the action of shear stress. Biomaterials 2005, 26, 1457–1466. [Google Scholar] [CrossRef] [PubMed]
- Yuan, S.; Liu, Z.; Xu, Z.; Liu, J.; Zhang, J. High mobility group box 1 (HMGB1): A pivotal regulator of hematopoietic malignancies. J. Hematol. Oncol. 2020, 13, 1–19. [Google Scholar] [CrossRef]
- Mullins, G.E.; Sundén-Cullberg, J.; Johansson, A.-S.; Rouhiainen, A.; Erlandsson-Harris, H.; Yang, H.; Tracey, K.J.; Rauvala, H.; Palmblad, J.; Andersson, J.; et al. Activation of Human Umbilical Vein Endothelial Cells Leads to Relocation and Release of High-Mobility Group Box Chromosomal Protein 1. Scand. J. Immunol. 2004, 60, 566–573. [Google Scholar] [CrossRef]
- Zhang, Y.; You, B.; Liu, X.; Chen, J.; Peng, Y.; Yuan, Z. High-Mobility Group Box 1 (HMGB1) Induces Migration of Endothelial Progenitor Cell via Receptor for Advanced Glycation End-Products (RAGE)-Dependent PI3K/Akt/eNOS Signaling Pathway. Med. Sci. Monit. 2019, 25, 6462–6473. [Google Scholar] [CrossRef]
- Marin, V.; Montero-Julian, F.A.; Grès, S.; Boulay, V.; Bongrand, P.; Farnarier, C.; Kaplanski, G. The IL-6-Soluble IL-6Rα Autocrine Loop of Endothelial Activation as an Intermediate Between Acute and Chronic Inflammation: An Experimental Model Involving Thrombin. J. Immunol. 2001, 167, 3435–3442. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.S.; Zhai, W.; Young, W.L.; Yang, G.-Y. Interleukin-6 triggers human cerebral endothelial cells proliferation and migration: The role for KDR and MMP-9. Biochem. Biophys. Res. Commun. 2006, 342, 1396–1404. [Google Scholar] [CrossRef] [PubMed]
- Brun, P.; Cortivo, R.; Zavan, B.; Vecchiato, N.; Abatangelo, G. In vitro reconstructed tissues on hyaluronan-based temporary scaffolding. J. Mater. Sci. Mater. Med. 1999, 10, 683–688. [Google Scholar] [CrossRef]
- Figallo, E.; Flaibani, M.; Zavan, B.; Abatangelo, G.; Elvassore, N. Micropatterned Biopolymer 3D Scaffold for Static and Dynamic Culture of Human Fibroblasts. Biotechnol. Prog. 2007, 23, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Gardin, C.; Bressan, E.; Ferroni, L.; Nalesso, E.; Vindigni, V.; Stellini, E.; Pinton, P.; Sivolella, S.; Zavan, B. In Vitro Concurrent Endothelial and Osteogenic Commitment of Adipose-Derived Stem Cells and Their Genomical Analyses Through Comparative Genomic Hybridization Array: Novel Strategies to Increase the Successful Engraftment of Tissue-Engineered Bone Grafts. Stem Cells Dev. 2012, 21, 767–777. [Google Scholar] [CrossRef] [PubMed]
- Azzena, B.; Mazzoleni, F.; Abatangelo, G.; Zavan, B.; Vindigni, V. Autologous Platelet-Rich Plasma as an Adipocyte In Vivo Delivery System: Case Report. Aesthetic Plast. Surg. 2008, 32, 155–158. [Google Scholar] [CrossRef]
- Ettorre, V.; De Marco, P.; Zara, S.; Perrotti, V.; Scarano, A.; Di Crescenzo, A.; Petrini, M.; Hadad, C.; Bosco, D.; Zavan, B.; et al. In vitro and in vivo characterization of graphene oxide coated porcine bone granules. Carbon 2016, 103, 291–298. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gardin, C.; Morciano, G.; Ferroni, L.; Mikus, E.; Tripodi, A.; Pin, M.; Tremoli, E.; Albertini, A.; Zavan, B. Biological Characterization of Human Autologous Pericardium Treated with the Ozaki Procedure for Aortic Valve Reconstruction. J. Clin. Med. 2021, 10, 3954. https://doi.org/10.3390/jcm10173954
Gardin C, Morciano G, Ferroni L, Mikus E, Tripodi A, Pin M, Tremoli E, Albertini A, Zavan B. Biological Characterization of Human Autologous Pericardium Treated with the Ozaki Procedure for Aortic Valve Reconstruction. Journal of Clinical Medicine. 2021; 10(17):3954. https://doi.org/10.3390/jcm10173954
Chicago/Turabian StyleGardin, Chiara, Giampaolo Morciano, Letizia Ferroni, Elisa Mikus, Alberto Tripodi, Maurizio Pin, Elena Tremoli, Alberto Albertini, and Barbara Zavan. 2021. "Biological Characterization of Human Autologous Pericardium Treated with the Ozaki Procedure for Aortic Valve Reconstruction" Journal of Clinical Medicine 10, no. 17: 3954. https://doi.org/10.3390/jcm10173954
APA StyleGardin, C., Morciano, G., Ferroni, L., Mikus, E., Tripodi, A., Pin, M., Tremoli, E., Albertini, A., & Zavan, B. (2021). Biological Characterization of Human Autologous Pericardium Treated with the Ozaki Procedure for Aortic Valve Reconstruction. Journal of Clinical Medicine, 10(17), 3954. https://doi.org/10.3390/jcm10173954