
Effects of Non-Pharmacological Treatment on Pain, Flexibility, Balance and Quality of Life in Women with Fibromyalgia: A Randomised Clinical Trial

 ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
4.1. Balance
4.2. Flexibility
4.3. Perceived Exertion
4.4. Pain and Quality of Life
4.5. Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin. Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef]
- Rivera, J.; Alegre, C.; Ballina, F.J.; Carnonell, J.; Carmoa, L.; Castel, B.; Collado, A.; Esteve, J.J.; Martínez, F.G.; Tornero, J.; et al. Documento de consenso de la Sociedad Española de Reumatología sobre la fibromialgia. Reumatol. Clín. 2006, 2, s55–s65. [Google Scholar] [CrossRef]
- Derek, J.; Panton, L.; Toole, T.; Sirithienthad, P.; Mathis, R.; McMillan, V. The effects of a 12-week strength-training program on strength and functionality in women with fibromialgia. Arch. Phys. Med. Rehabil. 2005, 86, 1713–1721. [Google Scholar] [CrossRef]
- Assumpção, A.; Sauer, J.F.; Mango, P.C.; Pascual, A. Physical function interfering with pain and symptoms in fibromyalgia patients. Clin. Exp. Rheumatol. 2010, 28, S57–S63. [Google Scholar] [PubMed]
- Jones, K.D.; Horak, F.B.; Winters-Stone, K.; Irvine, J.M.; Bennett, R.M. Fibromyalgia is associated with impaired balance and falls. J. Clin. Rheumatol. 2009, 15, 16–21. [Google Scholar] [CrossRef]
- Rasouli, O.; Stensdotter, A.; Van, A. TauG-guidance of dynamic balance control during gait initiation in patients with chronic fatigue syndrome and fibromialgia. Clin. Biomech. 2016, 37, 147–152. [Google Scholar] [CrossRef]
- Paul, L.M.; Wood, L.; Maclaren, W. The effect of exercise on gait and balance in patients with chronic fatigue síndrome. Gait Posture 2001, 14, 19–27. [Google Scholar] [CrossRef]
- Serrador, J.; Quigley, K.; Zhao, C.; Findley, T.; Natelson, B. Balance deficits in Chronic Fatigue Syndrome with and without fibromialgia. Neuro Rehabil. 2018, 42, 235–246. [Google Scholar] [CrossRef]
- Jones, C.J.; Rutledge, D.N.; Aquino, J. Predictors of physical performance and functional ability in people 50+ with and without fibromyalgia. J. Aging Phys. Act. 2010, 18, 353–368. [Google Scholar] [CrossRef]
- Valim, V.; Oliveira, L.M.; Suda, A.L.; Silva, L.E.; Faro, M.; Neto, T.L.B.; Feldman, D.; Natour, J. Peak oxygen uptake and ventilatory anaerobic threshold in fibromyalgia. J. Rheumatol. 2002, 29, 353–357. [Google Scholar] [PubMed]
- Mannerkorpi, K.; Burckhardt, C.S.; Bjelle, A. Physical performance characteristics of women with fibromyalgia. Arthritis Care Res. 1994, 7, 123–129. [Google Scholar] [CrossRef]
- Holland, G.J.; Tanaka, K.; Shigematsu, R.; Nakagaichi, M. Flexibility and physical functions of older adults: A review. J. Aging Phys. Act. 2002, 10, 169–206. [Google Scholar] [CrossRef]
- Heredia, J.M.; Aparicio, V.A.; Porres, J.M.; Delgado, M.; Soto, V. Spatial-temporal parameters of gait in women with fibromyalgia. Clin. Rheumatol. 2009, 28, 595–598. [Google Scholar] [CrossRef]
- Villafaina, S.; Gusi, N.; Rodriguez, S.; Martin, J.D.; Fuentes, J.P.; Collado, D. Influence of a Cell-Phone Conversation on Balance Performance in Women with Fibromyalgia: A Cross-Sectional Descriptive Study. BioMed Res. Int. 2019, 2019, 5132802. [Google Scholar] [CrossRef] [PubMed]
- Rutledge, D.N.; Martinez, A.; Traska, T.K.; Rose, D.J. Fall experiences of persons with fibromyalgia over 6 months. J. Adv. Nurs. 2013, 69, 435–448. [Google Scholar] [CrossRef] [PubMed]
- Collado, D.; Gallego, J.M.; Adsuar, J.C.; Dominguez, F.; Olivares, P.; Gusi, N. Fear of falling in women with fibromyalgia and its relation with number of falls and balance performance. BioMed Res. Int. 2015, 2015, 589014. [Google Scholar] [CrossRef][Green Version]
- Busch, A.J.; Barber, K.A.; Overend, T.J.; Peloso, P.M.; Schachter, C.L. Exercise for treating fibromyalgia syndrome. Cochrane Database Syst. Rev. 2007, CD003786. [Google Scholar] [CrossRef]
- Jones, K.D.; Adams, D.; Winters-Stone, K.; Burckhardt, C.S. A comprehensive review of 46 exercise treatment studies in fibromyalgia (1988–2005). Health Qual. Life Outcomes 2006, 4, 67. [Google Scholar] [CrossRef]
- Häuser, W.; Klose, P.; Langhorst, J.; Moradi, B.; Steinbach, M.; Schiltenwolf, M.; Busch, A. Efficacy of different types of aerobic exercise in fibromyalgia syndrome: A systematic review and meta-analysis of randomised controlled trials. Arthritis Res. Ther. 2010, 12, R79. [Google Scholar] [CrossRef]
- Bidonde, J.; Busch, A.J.; Schachter, C.L.; Webber, S.; Musselman, K.E.; Overend, T.J.; Góes, S.M.; Bello-Haas, V.D.; Boden, C. Mixed exercise training for adults with fibromyalgia. Cochrane Database Syst. Rev. 2019, 5, CD013340. [Google Scholar] [CrossRef]
- Jiao, J.; Russell, I.J.; Wang, W.; Wang, J.; Zhao, Y.-Y.; Jiang, Q. Ba-Duan-Jin alleviates pain and fibromyalgia-symptoms in patients with fibromyalgia: Results of a randomised controlled trial. Clin. Exp. Rheumatol. 2019, 37, 953–962. [Google Scholar]
- Estrategia de La OMS Sobre Medicina Tradicional 2002–2005. Organización Mundial de la Salud: Geneva, Switzerland, 2002. Available online: http://apps.who.int/iris/bitstream/handle/10665/67314/WHO_EDM_TRM_2002.1_spa.pdf;jsessionid=BD142DC22F7C85ADCB84488FAE99A7ED?sequence=1 (accessed on 20 May 2021).
- Scott, D.; Firestone, K.; Dupree, K. Complementary and alternative exercise for fibromyalgia: A meta-analysis. J. Pain Res. 2013, 6, 247–260. [Google Scholar] [CrossRef]
- Sawynok, J.; Lynch, M.E. Qigong and Fibromyalgia circa 2017. Medicines 2017, 4, 37. [Google Scholar] [CrossRef] [PubMed]
- Jahnke, R.; Larkey, L.; Rogers, C.; Etnier, J.; Lin, F. A Comprehensive Review of Health Benefits of Qigong and Tai Chi. Am. J. Health Promot. 2010, 24, e1–e25. [Google Scholar] [CrossRef]
- Park, K.S.; Jeong, H.Y.; Kim, Y.H. The effects of Qi-gong exercise on the health of the elderly-with respect to the physical health status, the fear of falling, balance efficacy, and Hwa-Byung. J. Orient. Neuropsychiatr. 2016, 27, 207–214. [Google Scholar] [CrossRef][Green Version]
- Shin, H.S.; Sok, S.R.; Yoo, J.H.; Im, Y.J.; Jang, M.H.; Jang, A.K.; Jang, A.K.; Jeong, Y.H.; Kang, Y.M.; Kim, Y.J.; et al. Understanding and Practice in Oriental Nursing: Kyung Hee University, College of Nursing Science; Su Moon Sa Press: Seoul, Korea, 2018. [Google Scholar]
- Requena, Y. Qigong: Gimnasia China Para la Salud y Longevidad; La Liebre de Marzo: Barcelona, Spain, 2013. [Google Scholar]
- Ahn, Y.J.; Jo, S.H.; Lee, S.H.; Lim, J.H. The review study on Yoga, Qigong, and Tai Chi interventions for anxiety: Based on Korean journal articles from 2009 to 2015. J. Orient. Neuropsychiatr. 2016, 27, 23–31. [Google Scholar] [CrossRef]
- Hauser, W. Fibromyalgia syndrome: Basic knowledge, diagnosis and treatment. Med. Mon. Pharm. 2016, 39, 504–511. [Google Scholar]
- Francielle, B.; Mendes, R.; Yukio, L.; Okino, L.; Goulart, I.; Okino, N. Benefits of Qigong as an integrative and complementary practice for health: A systematic review. Rev. Lat.-Am. Enferm. 2020, 28, e3317. [Google Scholar] [CrossRef]
- Langhorst, J.; Heldmann, P.; Henningsen, P.; Kopke, K.; Krumbein, L.; Lucius, H.; Winkelmann, A.; Wolf, B.; Häuser, W. Complementary and alternative procedures for fibromyalgia syndrome: Updated guidelines 2017 and overview of systematic review articles. Schmerz 2017, 31, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Wells, K.F.; Dillon, E.K. The sit and reach. A test of back and leg flexibility. Res. Q. Exerc. Sport 2013, 23, 115–118. [Google Scholar] [CrossRef]
- Avala, F.; Sainz, P.; Ste, M.; Santonja, F. Fiabilidad y validez de las pruebas sit-and-reach, revisión sistemática. Rev. Andal. Med. Deporte 2012, 5, 57–66. [Google Scholar] [CrossRef]
- Scott, J.; Huskisson, E.C. Vertical or horizontal visual analogue scales. Ann. Rheum. Dis. 1979, 38, 560. [Google Scholar] [CrossRef]
- Hawker GAMian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain),McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011, 63, S240–S252. [Google Scholar] [CrossRef]
- Monterde, S.; Salvat, I.; Montull, S.; Fernández-Ballart, J. Validación de la versión española del Fibromyalgia Impact Questionaire. Rev. Esp. Reumatol. 2004, 31, 507–513. [Google Scholar]
- Burckhardt, C.S.; Clark, S.R.; Bennet, R.M. The Fibromyalgia Impact Questionnaire: Development and validation. J. Rheumatol. 1991, 18, 728–733. [Google Scholar]
- Castellanos, R.; Pulido, M.A. Validity and reliability of Borg’s Perceived Exertion Scale. Enseñanza E Investig. En Psicol. 2009, 14, 169–177. [Google Scholar]
- Borg, G. Psychophysical scaling with applications in physical work and the perception of exertion. Scand. J. Work Environ. Health 1990, 16, 55–58. [Google Scholar] [CrossRef]
- Holmes, J.D.; Jenkins, M.E.; Johnson, A.M.; Hunt, M.; Clark, R. Validity of the Nintendo Wii(R) balance board for the assessment of standing balance in Parkinson’s disease. Clin. Rehabil. 2012, 27, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Meldrum, D.; Glennon, A.; Herdman, S.; Murray, D.; McConn, R. Virtual reality rehabilitation of balance: Assessment of the usability of the Nintendo Wii (®) Fit Plus. Disabil. Rehabil. Assist. Technol. 2011, 7, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Huurnink, A.; Fransz, D.P.; Kingma, I.; van Dieen, J. Comparison of a laboratory grade force platform with a Nintendo Wii Balance Board on measurement of postural control in single-leg stance balance tasks. J. Biomech. 2013, 46, 1392–1395. [Google Scholar] [CrossRef]
- Espí, G.V.; Inglés, M.; Ruescas, M.A.; Moreno, N. Effect of low-impact aerobic exercise combined with music therapy on patients with fibromyalgia. A pilot study. Complement. Ther. Med. 2016, 28, 1–7. [Google Scholar] [CrossRef]
- Kibar, S.; Yıldız, H.E.; Ay, S.; Evcik, D.; Sureyya, E. New Approach in Fibromyalgia Exercise Program: A Preliminary Study Regarding the Effectiveness of Balance Training. Arch. Phys. Med. Rehabil. 2015, 96, 1576–1582. [Google Scholar] [CrossRef] [PubMed]
- Garrido, E.M.; González, M.V.; Jiménez, M.; García, A.; Rodríguez, J. Effectiveness of acupuncture vs. core stability training in balance and functional capacity of women with fibromyalgia: A randomized controlled trial. Clin. Rehabil. 2020, 34, 630–645. [Google Scholar] [CrossRef]
- Ulger, O.; Yağlı, N.V. Effects of Yoga on balance and gait properties in women with musculoskeletal problems: A pilot study. Complement. Ther. Clin. Pract. 2011, 17, 13–15. [Google Scholar] [CrossRef]
- Wong, A.; Figueroa, A.; Sanchez, M.A.; Mok, W.; Chernykh, O.; Young, S. Effectiveness of Tai Chi on Cardiac Autonomic Function and Symptomatology in Women With Fibromyalgia: A Randomized Controlled Trial. J. Aging Phys. Act. 2018, 26, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Valencia, M.; Alonso, B.; Alvarez, M.J.; Barrientos, M.J.; Ayán, C.; Martín, V. Effects of 2 physiotherapy programs on pain perception, muscular flexibility, and illness impact in women with fibromyalgia: A pilot study. J. Manip. Physiol. Ther. 2009, 32, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Jones, K.D.; Burckhardt, C.S.; Clark, S.R.; Bennett, R.M.; Potempa, K.M. A randomized controlled trial of muscle strengthening versus flexibility training in fibromyalgia. J. Rheumatol. 2002, 29, 1041–1048. [Google Scholar] [PubMed]
- Ayan, C.; Alvarez, M.J.; Alonso, B.; Barrientos, M.J.; Valencia, M.; Martín, V. Health education home-based program in females with fibromyalgia: A pilot study. J. Back Musculoskelet. Rehabil. 2009, 22, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Nielens, H.; Boisset, V.; Masquelier, E. Fitness and perceived exertion in patients with fibromyalgia syndrome. Clin. J. Pain 2000, 16, 209–213. [Google Scholar] [CrossRef]
- Castro, A.M.; Matarán, G.A.; Arroyo, M.; Saavedra, M.; Fernández, C.; Moreno, C. Effects of myofascial release techniques on pain, physical function, and postural stability in patients with fibromyalgia: A randomized controlled trial. Clin. Rehabil. 2011, 25, 800–813. [Google Scholar] [CrossRef]
- Kesiktas, N.; Karagülle, Z.; Erdogan, N.; Yazicioglu, K.; Yilmaz, H.; Paker, N. The efficacy of balneotherapy and physical modalities on the pulmonary system of patients with fibromialgia. J. Back Musculoskelet. Rehabil. 2011, 24, 57–65. [Google Scholar] [CrossRef]
- Matsutani, L.A.; Marques, A.P.; Ferreira, E.A.; Assumpção, A.; Lage, L.V.; Casarotto, R.A.; Pereira, C.A.D.B. Effectiveness of muscle stretching exercises with and without laser therapy at tender points for patients with fibromyalgia. Clin. Exp. Rheumatol. 2007, 25, 410–415. [Google Scholar] [PubMed]
- Hooten, W.M.; Qu, W.; Townsend, C.O.; Judd, J.W. Effects of strength vs aerobic exercise on pain severity in adults with fibromyalgia: A randomized equivalence trial. Pain 2012, 153, 915–923. [Google Scholar] [CrossRef]
- Yang, K.H.; Kim, Y.H.; Lee, M.S. Efficacy of Qi-therapy (external Qigong) for elderly people with chronic pain. Int. J. Neurosci. 2005, 115, 949–963. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.W.; Hassett, A.L.; Hou, F.; Staller, J.; Lichtbroun, A.S. A pilot study of external qigong therapy for patients with fibromyalgia. J. Altern. Complement. Med. 2006, 12, 851–856. [Google Scholar] [CrossRef] [PubMed]
- Chaparro, M.; Diaz, V.; Gonzalez, J. Fibromialgia y osteoporosis. Rev. Osteoporos. Metab. Miner. 2011, 3, 113–118. [Google Scholar]
- Aparicio, A.; Ortega, F.; Herediaa, J.; Carbonell, A.; Delgado, M. Analysis of the body composition of Spanish women with fibromyalgia. Reumatol. Clin. 2011, 7, 7–12. [Google Scholar] [CrossRef]
- Neyro, J.L.; Franco, R.; Rodriguez, E.; Carrero, A.; Palacios, S. Fibromialgia y climaterio: ¿Asociación o coincidencia? Ginecol. Obstet. Mex. 2011, 79, 572–578. [Google Scholar]
- Vicente, T.P.J. Estudio Sobre Los Efectos Del Consumo Moderado de Vino Tinto en Mujeres Diagnosticadas de Fibromialgia (Study on the Effects of Moderate Consumption of Red Wine in Women Diagnosed with Fibromialgia). Ph.D. Thesis, University of Extremadura, Badajoz, Spain, 2009. [Google Scholar]
- Bosch, E.; Sáenz, N.; Valls, M.; Viñolas, S. Estudio de la calidad de vida en pacientes con fibromialgia: Impacto de un programa de educación sanitaria. Aten Primaria 2002, 30, 16–21. [Google Scholar] [CrossRef]
- Gelmana, S.M.; Lerab, S.; Caballero, F.; López, M.J. Tratamiento multidisciplinario de la fibromialgia. Estudio piloto prospectivo controlado. Rev. Esp. Reumatol. 2002, 29, 323–329. [Google Scholar]
- Bennett, R.M. Clinical manifestations and diagnosis of fibromyalgia. Rheum. Dis. Clin. N. Am. 2009, 35, 215–232. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outcomes | N | |
|---|---|---|
| Working status | Housewife | 41 |
| Unemployed | 10 | |
| Employed | 23 | |
| Incapacitated | 18 | |
| Retired | 1 | |
| Marital status | Married | 81 |
| Lives with her partner | 2 | |
| Single | 2 | |
| Separated | 2 | |
| Divorced | 3 | |
| Widow | 3 | |
| Education level | With no studies | 11 |
| Primary Education | 40 | |
| Secondary Education | 23 | |
| Bachelor’s Degree | 19 | |
| Smoking habits | No | 25 |
| Yes | 68 | |
| Baseline Outcomes | Mean ±SD | p-Value * | |||
|---|---|---|---|---|---|
| CG (N = 29) | AEG (N = 33) | EWG (N = 31) | |||
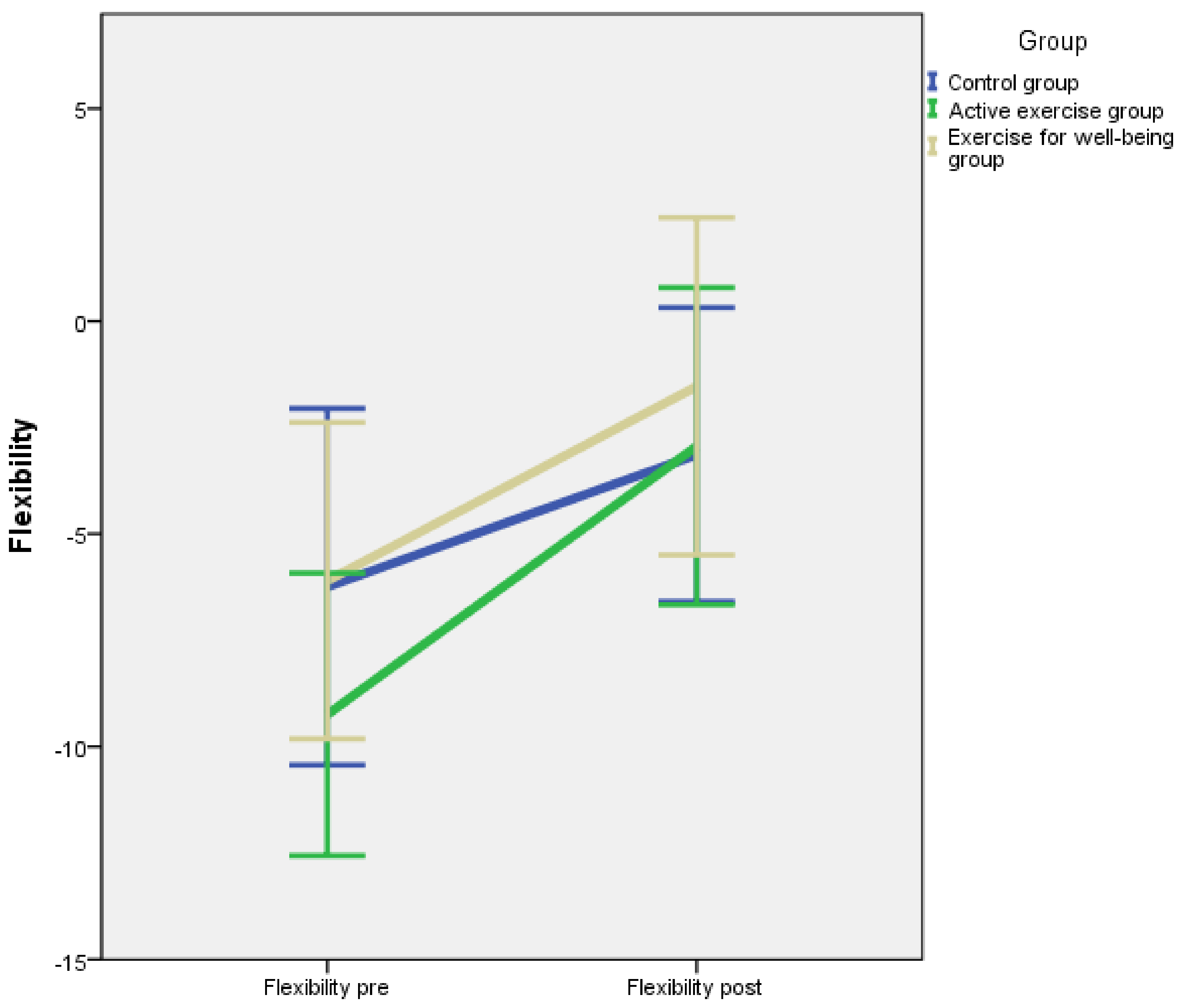
| Flexibility | Pre | −6.24 ± 11.01 | −9.24 ± 9.37 | −6.10 ± 9.96 | 0.193 |
| Post | −3.14 ± 9.08 | −2.94 ±10.51 | −2.03 ± 10.80 | ||
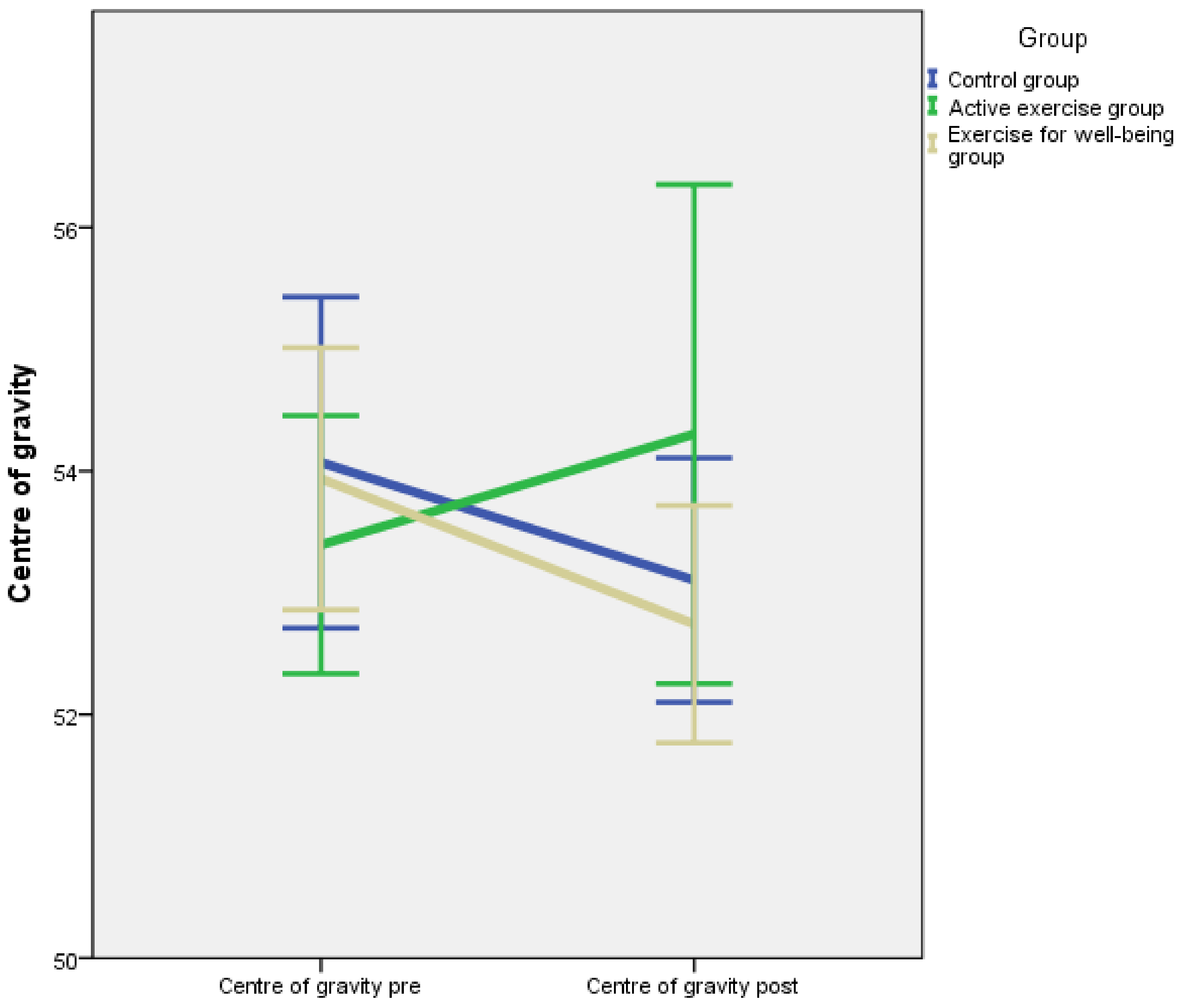
| Centre of gravity | Pre | 54.07 ± 3.58 | 53.39 ± 2.99 | 53.94 ± 2.93 | 0.184 |
| Post | 53.10 ± 2.64 | 54.30 ± 5.78 | 52.74 ± 2.66 | ||
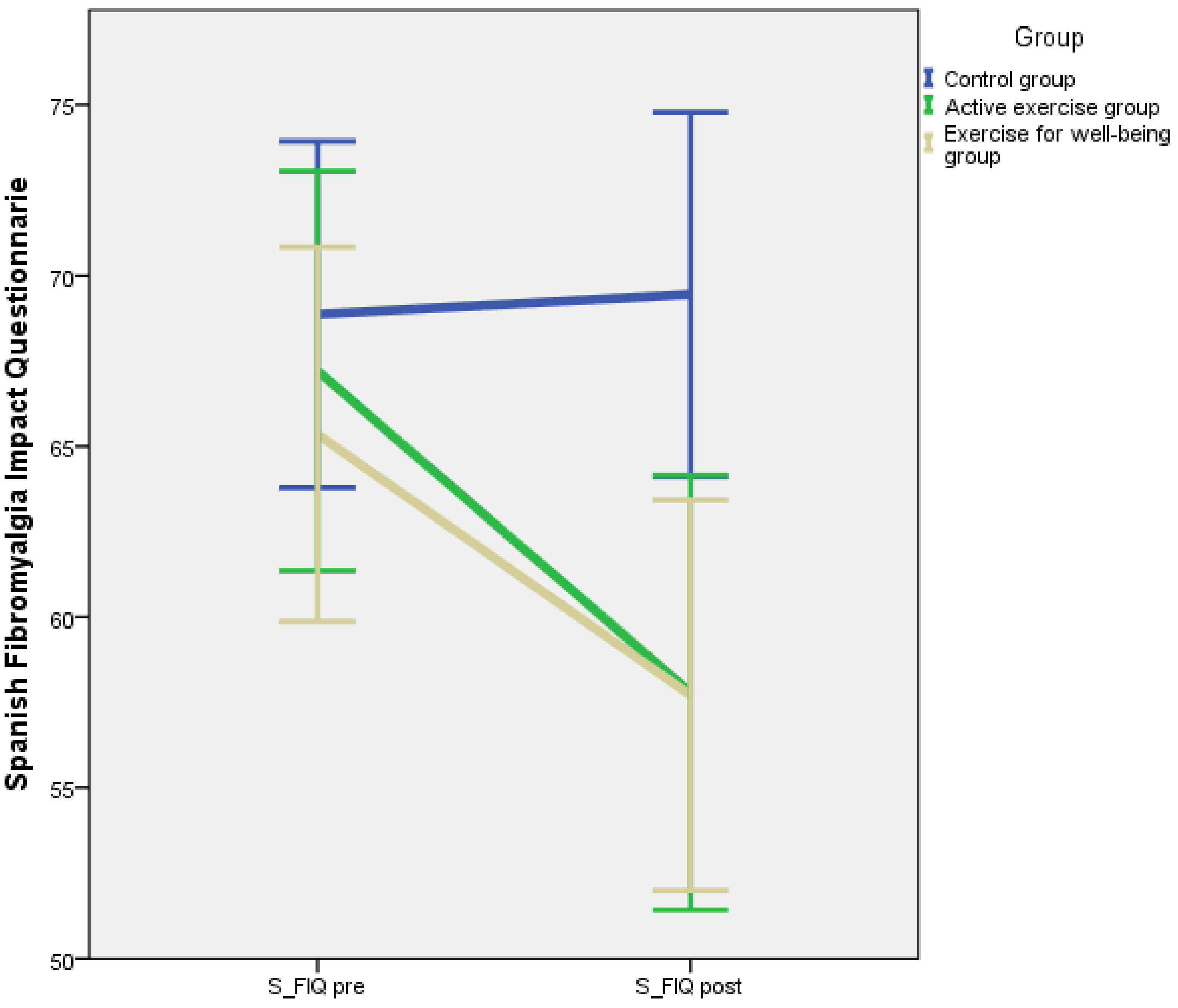
| S-FIQ | Pre | 68.86 ± 13.34 | 67.21 ± 16.51 | 65.35 ± 14.95 | 0.002 |
| Post | 69.45 ± 4.02 | 57.79 ± 17.95 | 57.71 ± 15.79 | ||
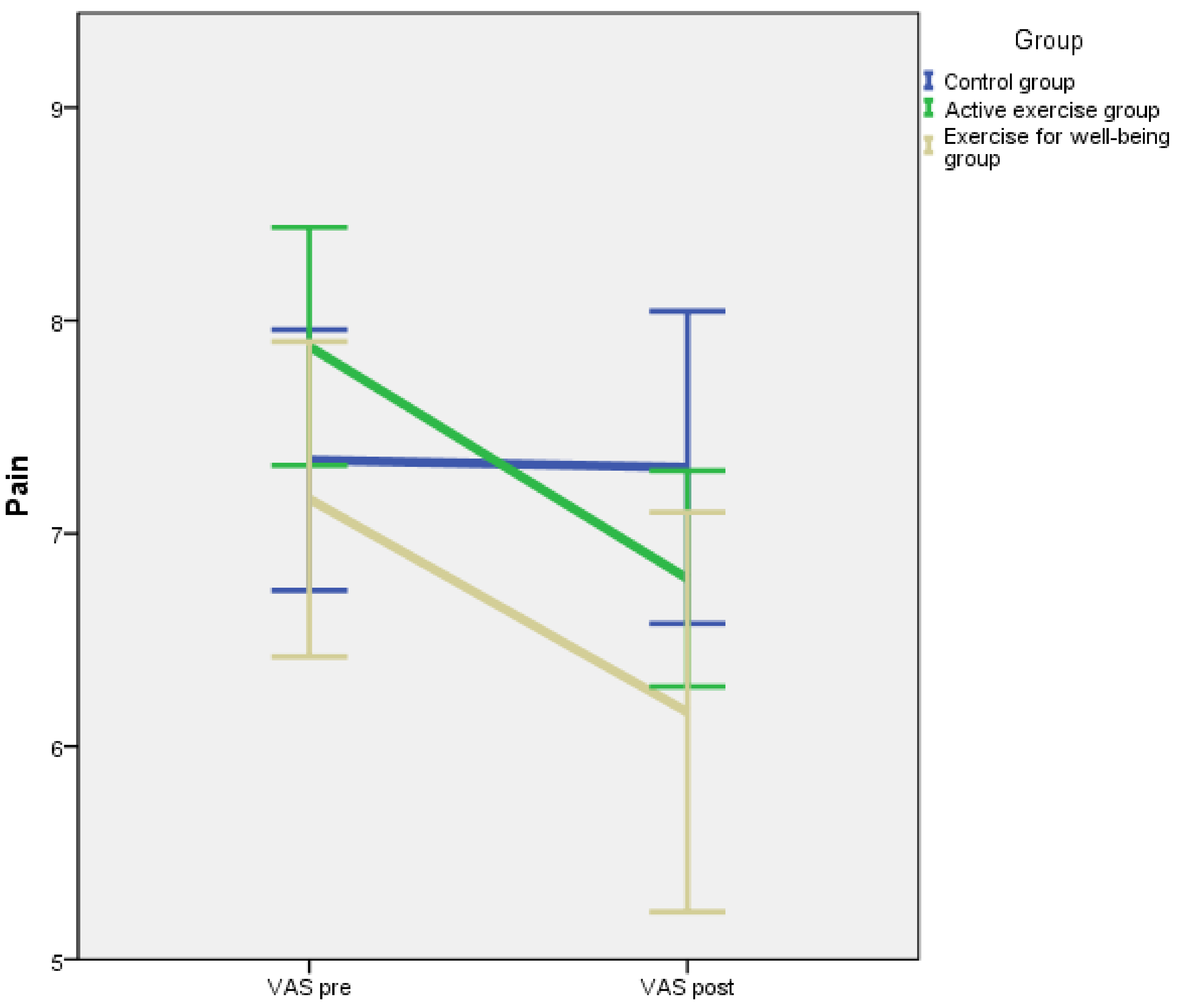
| VAS | Pre | 7.34 ± 1.61 | 7.88 ± 1.58 | 7.16 ± 2.02 | 0.020 |
| Post | 7.31 ±1.93 | 6.79 ± 1.43 | 6.16 ± 2.56 | ||
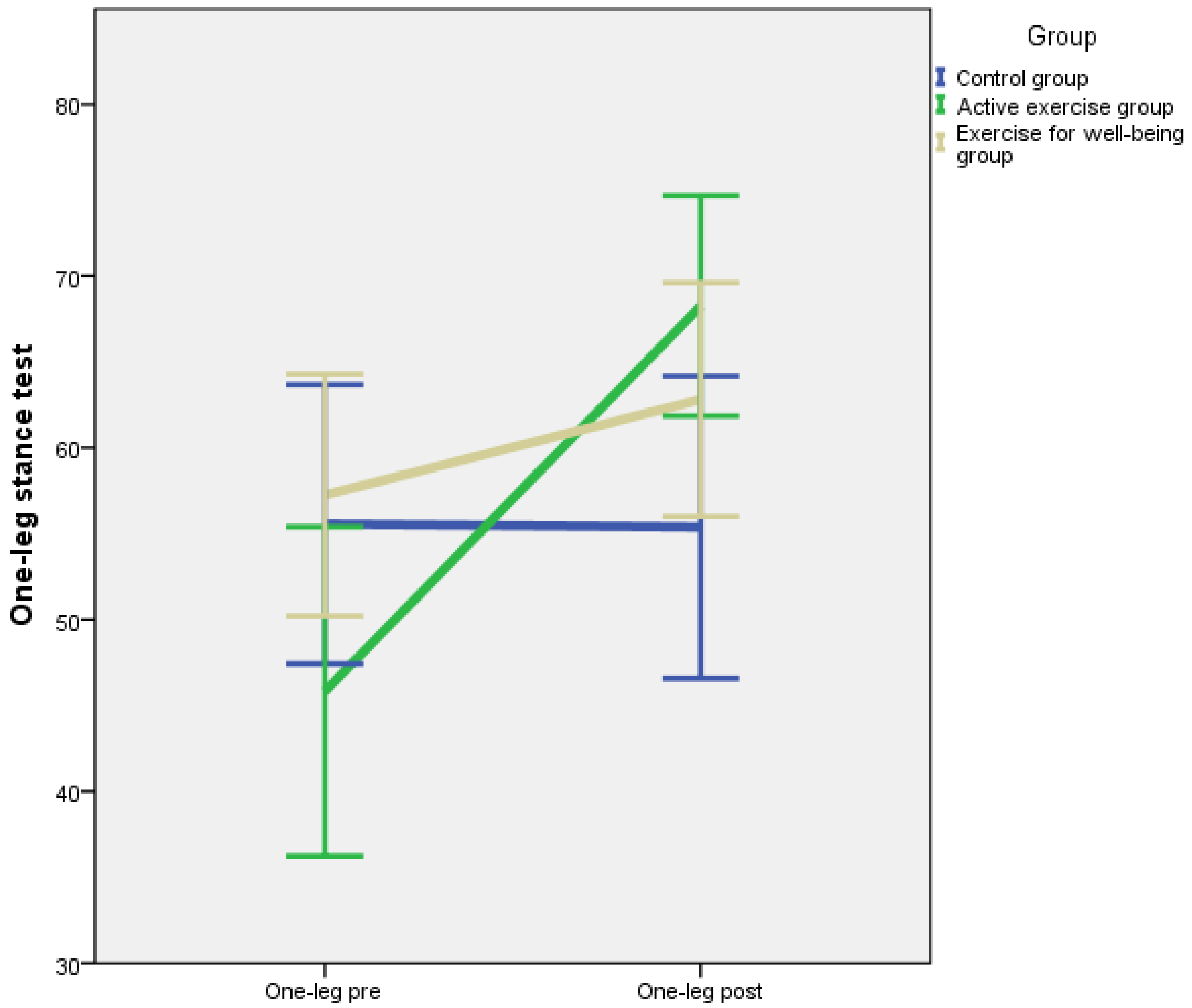
| One-leg stance test | Pre | 55.55 ± 21.35 | 45.82 ± 27.02 | 57.26 ± 19.20 | 0.002 |
| Post | 55.38 ± 23.14 | 68.27 ± 18.08 | 62.81 ± 18.56 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Mansilla, J.; Mejías-Gil, A.; Garrido-Ardila, E.M.; Jiménez-Palomares, M.; Montanero-Fernández, J.; González-López-Arza, M.V. Effects of Non-Pharmacological Treatment on Pain, Flexibility, Balance and Quality of Life in Women with Fibromyalgia: A Randomised Clinical Trial. J. Clin. Med. 2021, 10, 3826. https://doi.org/10.3390/jcm10173826
Rodríguez-Mansilla J, Mejías-Gil A, Garrido-Ardila EM, Jiménez-Palomares M, Montanero-Fernández J, González-López-Arza MV. Effects of Non-Pharmacological Treatment on Pain, Flexibility, Balance and Quality of Life in Women with Fibromyalgia: A Randomised Clinical Trial. Journal of Clinical Medicine. 2021; 10(17):3826. https://doi.org/10.3390/jcm10173826
Chicago/Turabian StyleRodríguez-Mansilla, Juan, Abel Mejías-Gil, Elisa María Garrido-Ardila, María Jiménez-Palomares, Jesús Montanero-Fernández, and María Victoria González-López-Arza. 2021. "Effects of Non-Pharmacological Treatment on Pain, Flexibility, Balance and Quality of Life in Women with Fibromyalgia: A Randomised Clinical Trial" Journal of Clinical Medicine 10, no. 17: 3826. https://doi.org/10.3390/jcm10173826
APA StyleRodríguez-Mansilla, J., Mejías-Gil, A., Garrido-Ardila, E. M., Jiménez-Palomares, M., Montanero-Fernández, J., & González-López-Arza, M. V. (2021). Effects of Non-Pharmacological Treatment on Pain, Flexibility, Balance and Quality of Life in Women with Fibromyalgia: A Randomised Clinical Trial. Journal of Clinical Medicine, 10(17), 3826. https://doi.org/10.3390/jcm10173826