
Gender-Related Differences in Prodromal Multiple Sclerosis Characteristics: A 7-Year Observation Study

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Total MS Population Prodromal Symptom Analysis
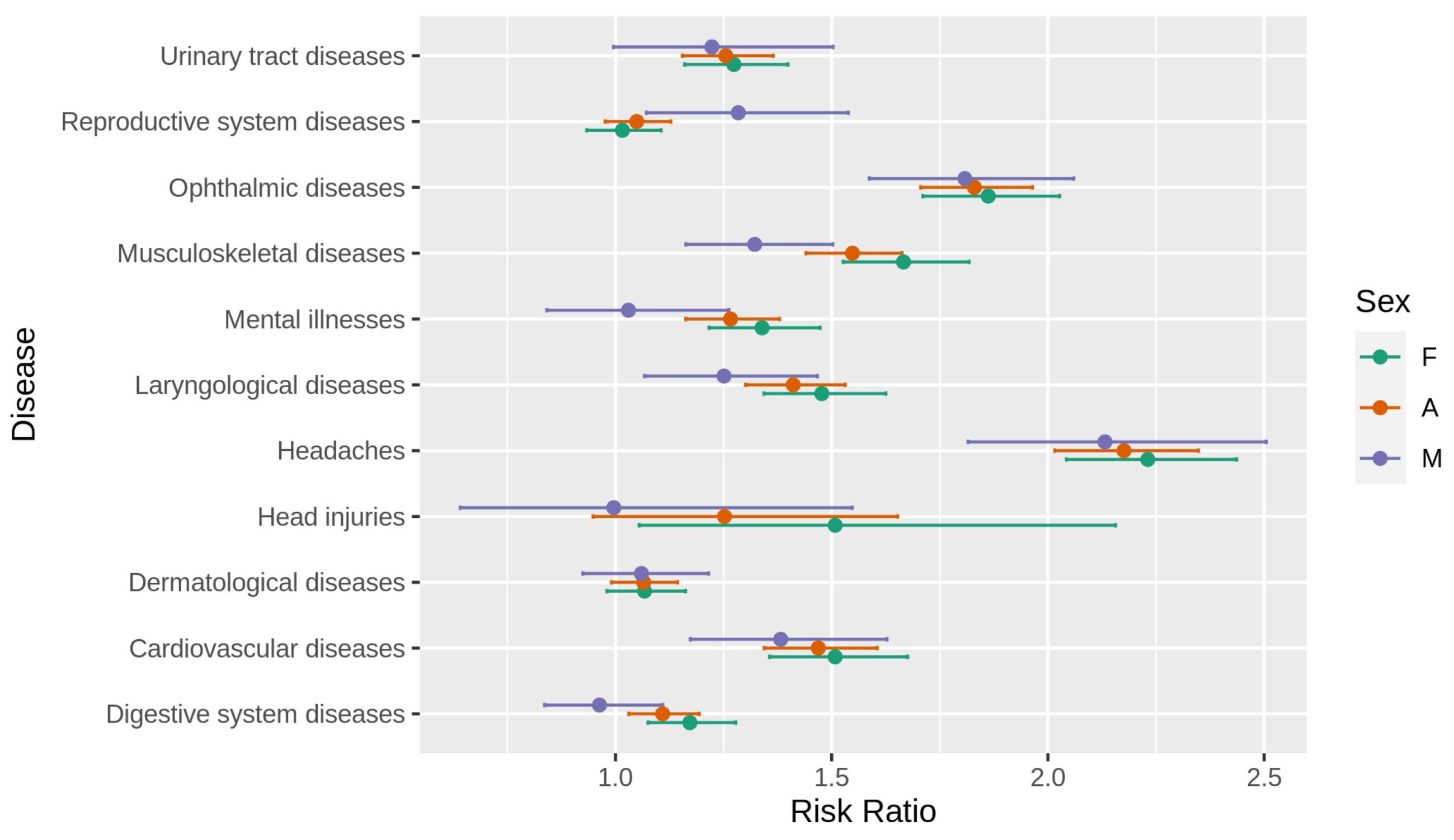
3.2. Gender-Related Prodromal Symptom Analysis
4. Discussion
5. Conclusions
6. Study Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Disanto, G.; Zecca, C.; MacLachlan, S.; Sacco, R.; Handunnetthi, L.; Meier, U.-C.; Simpson, A.; McDonald, L.; Rossi, A.; Benkert, P.; et al. Prodromal symptoms of multiple sclerosis in primary care. Ann. Neurol. 2018, 83, 1162–1173. [Google Scholar] [CrossRef]
- Wijnands, J.M.; Zhu, F.; Kingwell, E.; Zhao, Y.; Evans, C.; Fisk, J.D.; Marrie, R.A.; Tremlett, H. Prodrome in relapsing-remitting and primary progressive multiple sclerosis. Eur. J. Neurol. 2019, 26, 1032–1036. [Google Scholar] [CrossRef] [PubMed]
- Marrie, R.A. Mounting evidence for a multiple sclerosis prodrome. Nat. Rev. Neurol. 2019, 15, 689–690. [Google Scholar] [CrossRef]
- Tremlett, H.; Marrie, R.A. The multiple sclerosis prodrome: Emerging evidence, challenges, and opportunities. Mult. Scler. J. 2021, 27, 6–12. [Google Scholar] [CrossRef]
- Wijnands, J.M.A.; Kingwell, E.; Zhu, F.; Zhao, Y.; Högg, T.; Stadnyk, K.; Ekuma, O.; Lu, X.; Evans, C.; Fisk, J.D.; et al. Health-care use before a first demyelinating event suggestive of a multiple sclerosis prodrome: A matched cohort study. Lancet Neurol. 2017, 16, 445–451. [Google Scholar] [CrossRef]
- LA Yusuf, F.; Wijnands, J.M.; Kingwell, E.; Zhu, F.; Evans, C.; Fisk, J.D.; Zhao, Y.; Sutherland, J.M.; Patrick, D.M.; Marrie, R.A.; et al. Fatigue, sleep disorders, anaemia and pain in the multiple sclerosis prodrome. Mult. Scler. J. 2021, 27, 290–302. [Google Scholar] [CrossRef]
- Golden, L.C.; Voskuhl, R. The importance of studying sex differences in disease: The example of multiple sclerosis. J. Neurosci. Res. 2017, 95, 633–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gasperi, C.; Hapfelmeier, A.; Daltrozzo, T.; Schneider, A.; Donnachie, E.; Hemmer, B. Systematic Assessment of Medical Diagnoses Preceding the First Diagnosis of Multiple Sclerosis. Neurology 2021, 96, e2977–e2988. [Google Scholar] [CrossRef]
- Whitacre, C.; Reingold, S.; O’Looney, P.; Blankenhorn, E.; Brinley, F.; Collier, E.; Duquette, P.; Fox, H.N.; Giesser, B.; Gilmore, W.; et al. A Gender Gap in Autoimmunity. Science 1999, 283, 1277–1278. [Google Scholar] [CrossRef]
- Tomassini, V.; Pozzilli, C. Sex hormones, brain damage and clinical course of Multiple Sclerosis. J. Neurol. Sci. 2009, 286, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Voskuhl, R.R.; Gold, S. Sex-related factors in multiple sclerosis susceptibility and progression. Nat. Rev. Neurol. 2012, 8, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Tiwari-Woodruff, S.; Morales, L.B.J.; Lee, R.; Voskuhl, R.R. Differential Neuroprotective and Antiinflammatory Effects of Estrogen Receptor (ER)Alpha and ERbeta Ligand Treatment. Proc. Natl. Acad. Sci. USA 2007, 104, 14813–14818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koch, M.; Kingwell, E.; Rieckmann, P.; Tremlett, H.; Neurologists, U.M.C. The natural history of secondary progressive multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2010, 81, 1039–1043. [Google Scholar] [CrossRef] [Green Version]
- Shirani, A.; Zhao, Y.; Kingwell, E.; Rieckmann, P.; Tremlett, H. Temporal trends of disability progression in multiple sclerosis: Findings from British Columbia, Canada (1975–2009). Mult. Scler. J. 2011, 18, 442–450. [Google Scholar] [CrossRef]
- Angeloni, B.; Bigi, R.; Bellucci, G.; Mechelli, R.; Ballerini, C.; Romano, C.; Morena, E.; Pellicciari, G.; Reniè, R.; Rinaldi, V.; et al. A Case of Double Standard: Sex Differences in Multiple Sclerosis Risk Factors. Int. J. Mol. Sci. 2021, 22, 3696. [Google Scholar] [CrossRef]
- International Multiple Sclerosis Genetics Consortium. Multiple sclerosis genomic map implicates peripheral immune cells and microglia in susceptibility. Science 2019, 365, eaav7188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lenz, K.M.; McCarthy, M.M. A Starring Role for Microglia in Brain Sex Differences. Neuroscientist 2015, 21, 306–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjornevik, K.; Munger, K.L.; Cortese, M.; Barro, C.; Healy, B.C.; Niebuhr, D.W.; Scher, A.I.; Kuhle, J.; Ascherio, A. Serum Neurofilament Light Chain Levels in Patients with Presymptomatic Multiple Sclerosis. JAMA Neurol. 2020, 77, 58–64. [Google Scholar] [CrossRef]
- Gerdes, L.A.; Janoschka, C.; Eveslage, M.; Mannig, B.; Wirth, T.; Schulte-Mecklenbeck, A.; Lauks, S.; Glau, L.; Gross, C.C.; Tolosa, E.; et al. Immune signatures of prodromal multiple sclerosis in monozygotic twins. Proc. Natl. Acad. Sci. USA 2020, 117, 21546–21556. [Google Scholar] [CrossRef] [PubMed]
- Makhani, N.; Tremlett, H. The multiple sclerosis prodrome. Nat. Rev. Neurol. 2021, 17, 515–521. [Google Scholar] [CrossRef]
- Wnuk, M.; Maluchnik, M.; Perwieniec, J.; Podwojcic, K.; Szelag, M.; Walkiewicz, D.; Zakrzewski, M.; Kulakowska, A.; Brola, W.; Rejdak, K.; et al. Multiple Sclerosis Incidence and Prevalence in Poland: Data from Administrative Health Claims. Mult. Scler. Relat. Disord. 2021, 55, 103162. [Google Scholar] [CrossRef]

{kind=link}
| All | Female | Male | |||||
|---|---|---|---|---|---|---|---|
| MS-Cases (Group %) | Controls (Group %) | MS-Cases (Group %) | Controls (Group %) | MS-Cases (Group %) | Controls (Group %) | ||
| Age | <20 | 170 (5.56%) | 16,728 (5.58%) | 121 (5.69%) | 11,903 (5.70%) | 49 (5.28%) | 4825 (5.30%) |
| 20–29 | 683 (22.35%) | 67,046 (22.35%) | 468 (21.99%) | 45,942 (21.99%) | 215 (23.17%) | 21,104 (23.16%) | |
| 30–39 | 841 (27.52%) | 82,538 (27.51%) | 585 (27.49%) | 57,407 (27.48%) | 256 (27.59%) | 25,131 (27.58%) | |
| 40–49 | 634 (20.75%) | 62,225 (20.74%) | 456 (21.43%) | 44,753 (21.42%) | 178 (19.18%) | 17,472 (19.18%) | |
| 50+ | 728 (23.82%) | 71,463 (23.82%) | 498 (23.40%) | 48,884 (23.40%) | 230 (24.78%) | 22,579 (24.78%) | |
| Age | Mean | 39.17 | 39.17 | 39.13 | 39.13 | 39.26 | 39.26 |
| SD | 14.02 | 14.03 | 13.84 | 13.84 | 14.45 | 14.44 | |
| Total | 3056 | 300,000 | 2128 | 208,889 | 928 | 91,111 | |
| Condition | ICD-10 Codes |
|---|---|
| Urinary tract diseases | N23.x, N30.x, N39.x |
| Reproductive system diseases | N34.x, N35.x, N36.x, N40.x, N41.x, N42.x, N43.x, N44.x, N45.x, N46.x, N47.x, N48.x, N49.x, N50.x, N70.x, N72.x, N76.x, N83.x, N86.x, N91.x, N92.x, N93.x, N94.x, N97.x |
| Ophthalmic diseases | H10.x, H35.x, H40.0, H46.x, H47.x, H52.x, H53.x, H57.x |
| Musculoskeletal diseases | M12.8, M13.x, M15.x, M17.x, M23.x, M25.x, M41.x, M47.x, M48, M50.x, M51.x, M54.x, M65.x, M70.x |
| Mental illnesses | F32.x, F33.x, F41.x, F43.x, F48.x |
| Laryngological diseases | H60.x, H61.x, H65.x, H66.x, H68.x, H81.x, H82.x, H90.x, H91.x, H93.x |
| Headaches | G43.x, G44.x, R51.x, R52.x |
| Head injuries | S02.0, S02.1, S02.7, S02.8, S02.9, S04, S06, S07, S09.7, S09.8, S09.9, T02.0, T03.0, T90.5 |
| Dermatological diseases | L02.x, L08.x, L20.x, L21.x, L23.x, L24.x, L25.x, L30.x, L50.x, L60.x, L65.x, L70.x, L98.x |
| Cardiovascular diseases | I11.x, I25.x, I49.x, I69.x, I70.x |
| Digestive system diseases | K21.x, K29.x, K30.x, K52.x, K58.x, K59.x, K63.x, K80.x |
| All | Female | Male | ||||
|---|---|---|---|---|---|---|
| Condition | MS Cases Incidence | Controls Incidence | MS Cases Incidence | Controls Incidence | MS Cases Incidence | Controls Incidence |
| Urinary tract diseases | 0.230 | 0.192 | 0.284 | 0.237 | 0.108 | 0.090 |
| Reproductive system diseases | 0.392 | 0.380 | 0.499 | 0.495 | 0.147 | 0.118 |
| Ophthalmic diseases | 0.499 | 0.351 | 0.541 | 0.386 | 0.402 | 0.270 |
| Musculoskeletal diseases | 0.592 | 0.482 | 0.624 | 0.498 | 0.517 | 0.447 |
| Mental illnesses | 0.218 | 0.180 | 0.264 | 0.210 | 0.112 | 0.109 |
| Laryngological diseases | 0.249 | 0.189 | 0.269 | 0.199 | 0.203 | 0.168 |
| Headaches | 0.307 | 0.168 | 0.356 | 0.197 | 0.195 | 0.101 |
| Head injuries | 0.016 | 0.013 | 0.014 | 0.009 | 0.022 | 0.022 |
| Dermatological diseases | 0.406 | 0.391 | 0.442 | 0.426 | 0.324 | 0.312 |
| Cardiovascular diseases | 0.196 | 0.142 | 0.199 | 0.141 | 0.188 | 0.143 |
| Digestive system diseases | 0.364 | 0.340 | 0.396 | 0.358 | 0.289 | 0.297 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perwieniec, J.; Podwójcic, K.; Maluchnik, M.; Szeląg, M.; Walkiewicz, D.; Zakrzewski, M.; Droździkowska, A.; Kamiński, B.; Zasybska, A.; Wnuk, M.; et al. Gender-Related Differences in Prodromal Multiple Sclerosis Characteristics: A 7-Year Observation Study. J. Clin. Med. 2021, 10, 3821. https://doi.org/10.3390/jcm10173821
Perwieniec J, Podwójcic K, Maluchnik M, Szeląg M, Walkiewicz D, Zakrzewski M, Droździkowska A, Kamiński B, Zasybska A, Wnuk M, et al. Gender-Related Differences in Prodromal Multiple Sclerosis Characteristics: A 7-Year Observation Study. Journal of Clinical Medicine. 2021; 10(17):3821. https://doi.org/10.3390/jcm10173821
Chicago/Turabian StylePerwieniec, Jakub, Krzysztof Podwójcic, Michał Maluchnik, Mateusz Szeląg, Dorota Walkiewicz, Michał Zakrzewski, Amelia Droździkowska, Bogumił Kamiński, Adriana Zasybska, Marcin Wnuk, and et al. 2021. "Gender-Related Differences in Prodromal Multiple Sclerosis Characteristics: A 7-Year Observation Study" Journal of Clinical Medicine 10, no. 17: 3821. https://doi.org/10.3390/jcm10173821
APA StylePerwieniec, J., Podwójcic, K., Maluchnik, M., Szeląg, M., Walkiewicz, D., Zakrzewski, M., Droździkowska, A., Kamiński, B., Zasybska, A., Wnuk, M., Słowik, A., & Rejdak, K. (2021). Gender-Related Differences in Prodromal Multiple Sclerosis Characteristics: A 7-Year Observation Study. Journal of Clinical Medicine, 10(17), 3821. https://doi.org/10.3390/jcm10173821