
Virtual Reality vs. Tablet Video as an Experiential Education Platform for Pediatric Patients Undergoing Chest Radiography: A Randomized Clinical Trial

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study
2.2. Patients
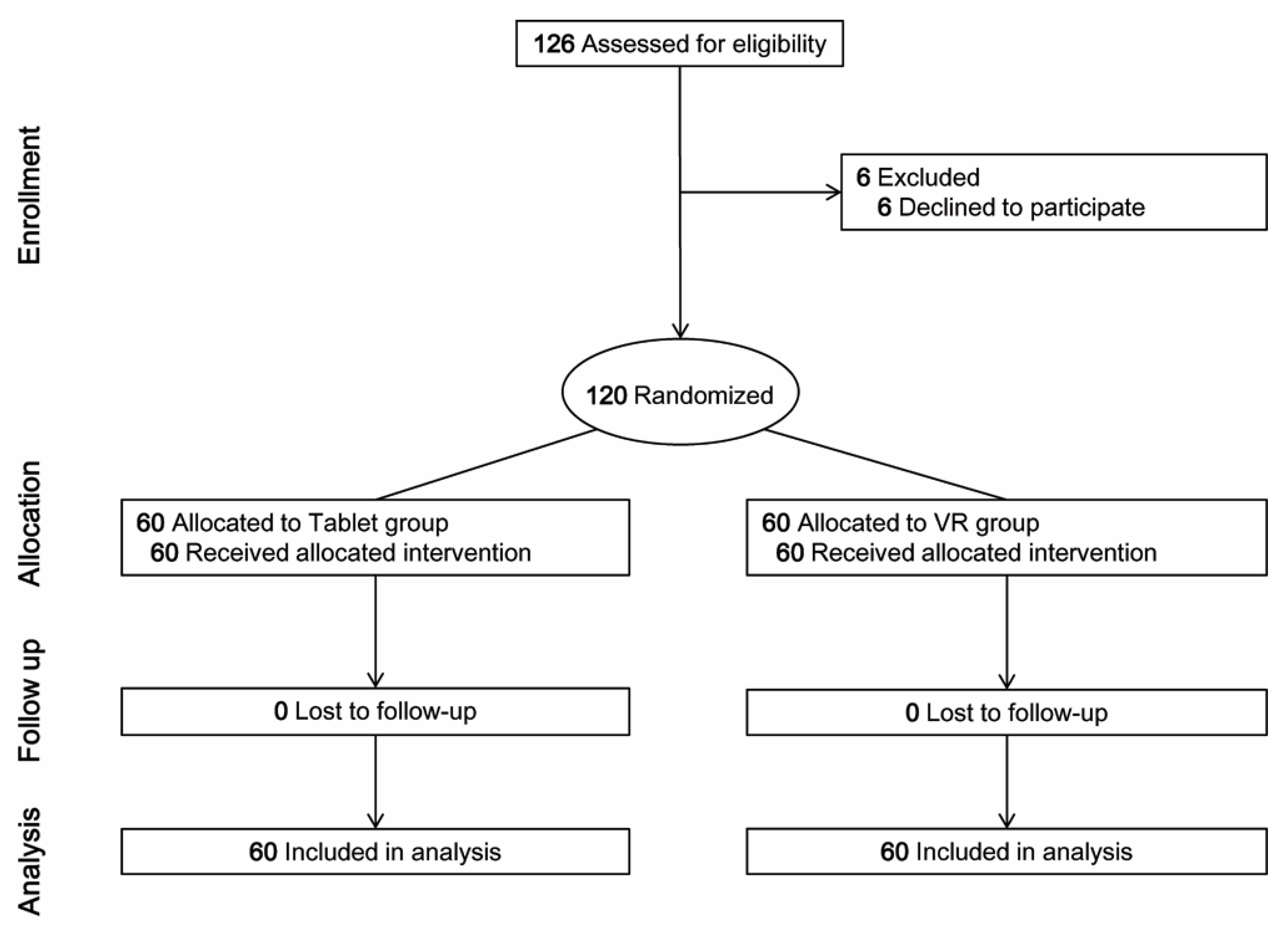
2.3. Randomization
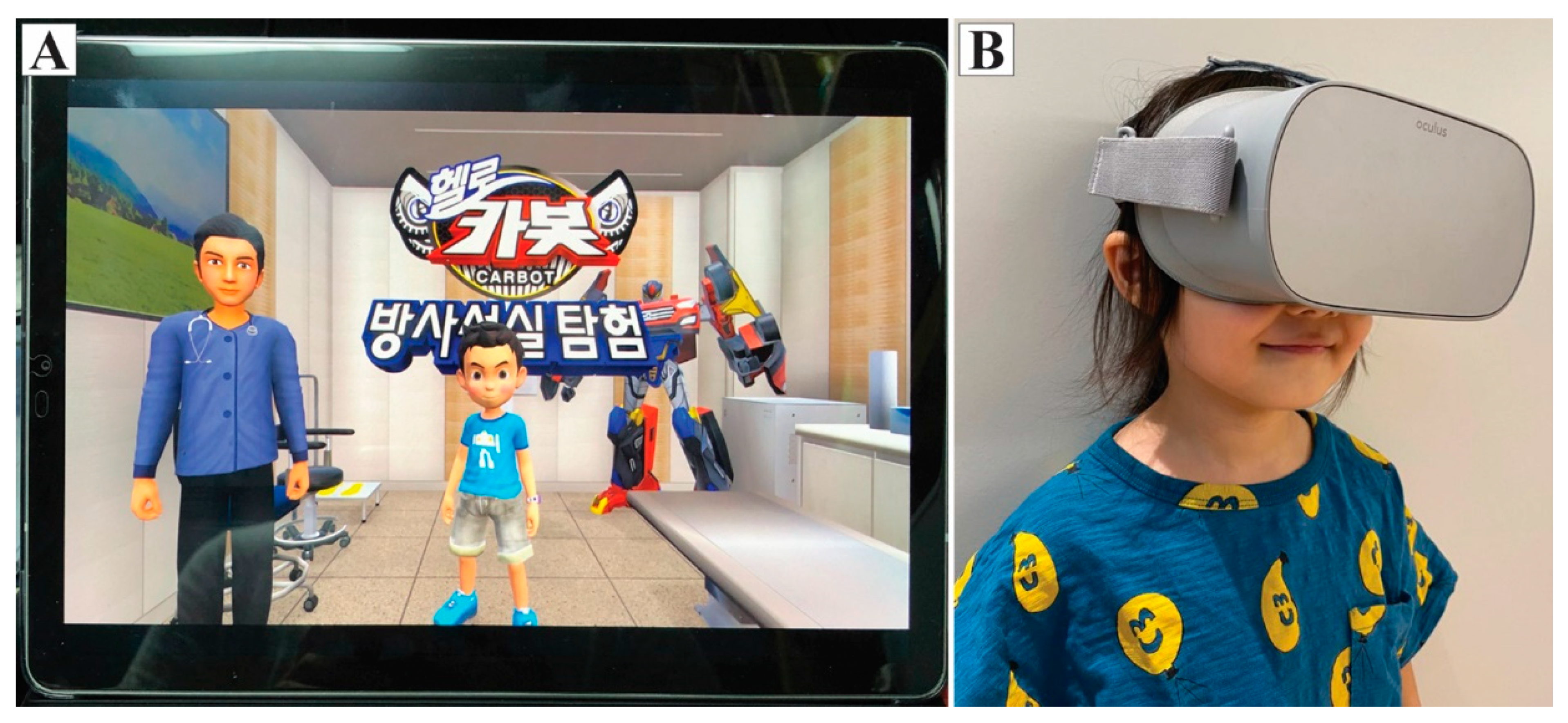
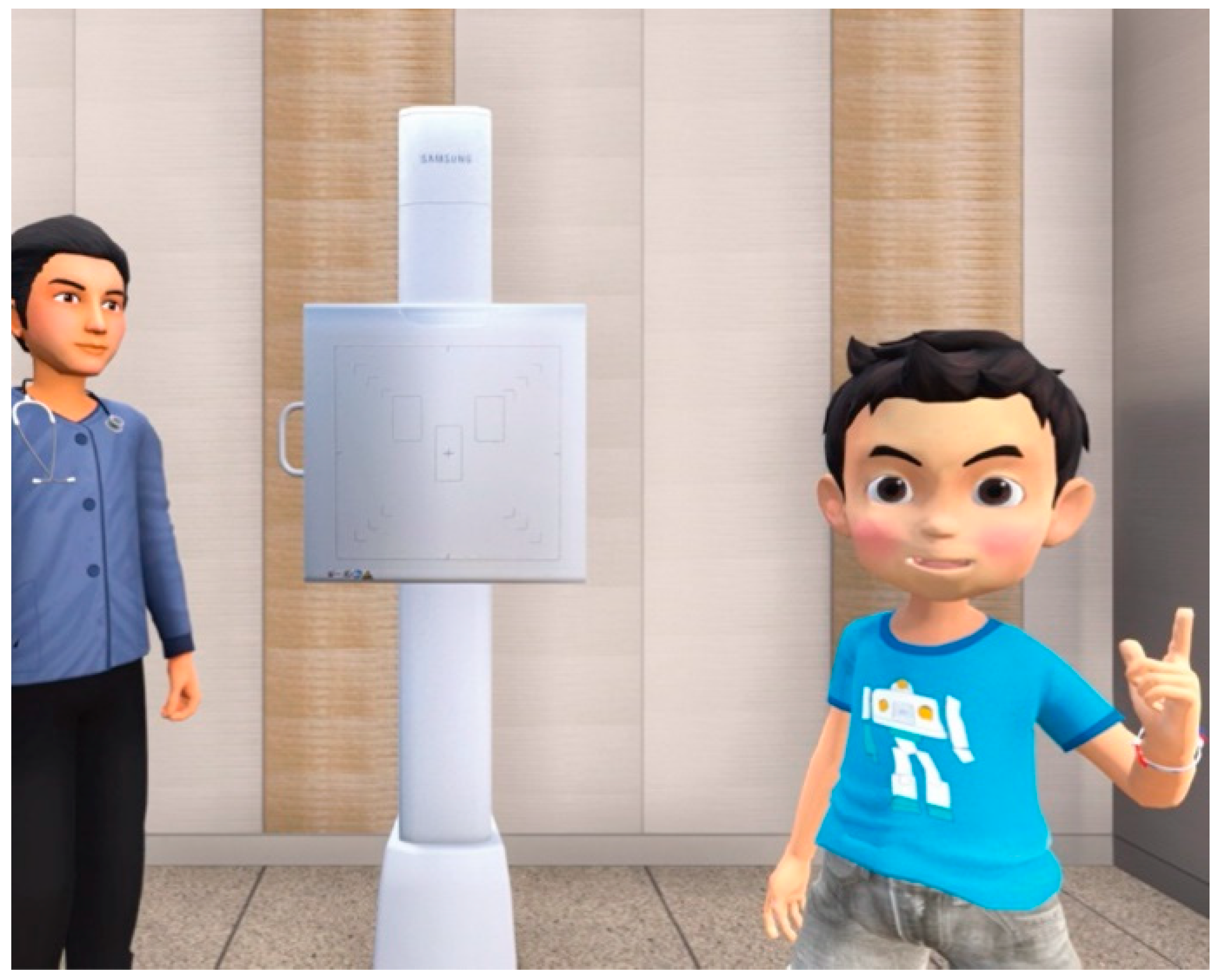
2.4. Intervention
2.5. Outcome Measurement
2.6. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fernandez-Alvarez, J.; Di Lernia, D.; Riva, G. Virtual Reality for Anxiety Disorders: Rethinking a Field in Expansion. Adv. Exp. Med. Biol. 2020, 1191, 389–414. [Google Scholar] [CrossRef] [PubMed]
- Tieri, G.; Morone, G.; Paolucci, S.; Iosa, M. Virtual reality in cognitive and motor rehabilitation: Facts, fiction and fallacies. Expert Rev. Med. Devices 2018, 15, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Arai, Y.C.; Ito, H.; Kandatsu, N.; Kurokawa, S.; Kinugasa, S.; Komatsu, T. Parental presence during induction enhances the effect of oral midazolam on emergence behavior of children undergoing general anesthesia. Acta Anaesthesiol. Scand. 2007, 51, 858–861. [Google Scholar] [CrossRef] [PubMed]
- Rice, M.; Glasper, A.; Keeton, D.; Spargo, P. The effect of a preoperative education programme on perioperative anxiety in children: An observational study. Paediatr. Anaesth. 2008, 18, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Han, S.H.; Park, J.W.; Choi, S.I.; Kim, J.Y.; Lee, H.; Yoo, H.J.; Ryu, J.H. Effect of Immersive Virtual Reality Education before Chest Radiography on Anxiety and Distress among Pediatric Patients: A Randomized Clinical Trial. JAMA Pediatr. 2019. [Google Scholar] [CrossRef]
- Ryu, J.H.; Oh, A.Y.; Yoo, H.J.; Kim, J.H.; Park, J.W.; Han, S.H. The effect of an immersive virtual reality tour of the operating theater on emergence delirium in children undergoing general anesthesia: A randomized controlled trial. Paediatr. Anaesth. 2019, 29, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Ryu, J.H.; Park, J.W.; Nahm, F.S.; Jeon, Y.T.; Oh, A.Y.; Lee, H.J.; Kim, J.H.; Han, S.H. The Effect of Gamification through a Virtual Reality on Preoperative Anxiety in Pediatric Patients Undergoing General Anesthesia: A Prospective, Randomized, and Controlled Trial. J. Clin. Med. 2018, 7, 284. [Google Scholar] [CrossRef] [PubMed]
- Ryu, J.H.; Park, S.J.; Park, J.W.; Kim, J.W.; Yoo, H.J.; Kim, T.W.; Hong, J.S.; Han, S.H. Randomized clinical trial of immersive virtual reality tour of the operating theatre in children before anaesthesia. Br. J. Surg. 2017, 104, 1628–1633. [Google Scholar] [CrossRef]
- Park, J.W.; Nahm, F.S.; Kim, J.H.; Jeon, Y.T.; Ryu, J.H.; Han, S.H. The Effect of Mirroring Display of Virtual Reality Tour of the Operating Theatre on Preoperative Anxiety: A Randomized Controlled Trial. IEEE J. Biomed. Health Inf. 2019, 23, 2655–2660. [Google Scholar] [CrossRef] [PubMed]
- Blount, R.L.; Loiselle, K.A. Effect of Immersive Virtual Reality Education before Chest Radiography on Anxiety and Distress among Pediatric Patients: A Randomized Clinical Trial. Pain Res. Manag. 2009, 14, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Bradford, R. Short communication: The importance of psychosocial factors in understanding child distress during routine X-ray procedures. J. Child. Psychol. Psychiatry 1990, 31, 973–982. [Google Scholar] [CrossRef] [PubMed]
- Cieslik, B.; Mazurek, J.; Rutkowski, S.; Kiper, P.; Turolla, A.; Szczepanska-Gieracha, J. Virtual reality in psychiatric disorders: A systematic review of reviews. Complement. Med. 2020, 52, 102480. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Yu, F.; Shi, D.; Shi, J.; Tian, Z.; Yang, J.; Wang, X.; Jiang, Q. Application of virtual reality technology in clinical medicine. Am. J. Transl. Res. 2017, 9, 3867–3880. [Google Scholar] [PubMed]
- Kim, Y.; Kim, H.; Kim, Y.O. Virtual Reality and Augmented Reality in Plastic Surgery: A Review. Arch. Plast. Surg. 2017, 44, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Neroni, M.A.; Oti, A.; Crilly, N. Virtual Reality design-build-test games with physics simulation: Opportunities for researching design cognition. Int. J. Des. Creat. Innov. 2021, 1–34. [Google Scholar] [CrossRef]
- Houillon, A.; Lorenz, R.C.; Boehmer, W.; Rapp, M.A.; Heinz, A.; Gallinat, J.; Obermayer, K. The effect of novelty on reinforcement learning. Prog. Brain Res. 2013, 202, 415–439. [Google Scholar] [CrossRef] [PubMed]
- Alexander, M. Managing patient stress in pediatric radiology. Radiol. Technol. 2012, 83, 549–560. [Google Scholar] [PubMed]
- Sanborn, P.A.; Michna, E.; Zurakowski, D.; Burrows, P.E.; Fontaine, P.J.; Connor, L.; Mason, K.P. Adverse cardiovascular and respiratory events during sedation of pediatric patients for imaging examinations. Radiology 2005, 237, 288–294. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Tablet Group (n = 60) | VR Group (n = 60) | |
|---|---|---|
| Age (years) | 6.0 (4.8–7.0) | 6.0 (5.0–7.3) |
| Male | 25 (41.7) | 32 (53.3) |
| Weight (kg) | 20.6 (18.2–26.4) | 22.3 (18.9–28.2) |
| Height (cm) | 113.8 (106.7–124.4) | 118.3 (109.8–127.8) |
| Reason for chest radiography | ||
| respiratory or cardiovascular symptom | 12 (20.0) | 16 (26.7) |
| preoperative work up | 48 (80.0) | 44 (73.3) |
| Tablet Group (n = 60) | VR Group (n = 60) | Risk Ratio (95% CI) | p-Value | |
|---|---|---|---|---|
| OSBD group | ||||
| More Distressed (≥5) | 28 (46.7) | 11 (18.3) | 3.9 (1.7–8.9) | 0.001 |
| Less distressed (<5) | 32 (53.3) | 49 (81.7) | ||
| OSBD score | 4.0 (2.0–7.0) | 1.0 (0.8–3.0) | <0.001 | |
| Parental presence | 19 (31.7) | 5 (8.3) | 5.1 (1.8–14.8) | 0.001 |
| Parental satisfaction score | 10.0 (9.0–10.0) | 10.0 (9.0–10.0) | 0.599 |
| Tablet Group (n = 60) | VR Group (n = 60) | Risk Ratio (95% CI) | p-Value | |
|---|---|---|---|---|
| Time for radiography procedure (s) | 65.0 (53.8–74.5) | 48.0 (43.0–54.3) | <0.001 | |
| Repeated procedures | 6 (10.0) | 2 (3.3) | 3.2 (0.6–16.7) | 0.272 |
| Easiness score for the procedure | 8.0 (7.0–9.0) | 10.0 (10.0–10.0) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ryu, J.-H.; Park, J.-W.; Choi, S.I.; Kim, J.Y.; Lee, H.; Yoo, H.-J.; Han, S.-H. Virtual Reality vs. Tablet Video as an Experiential Education Platform for Pediatric Patients Undergoing Chest Radiography: A Randomized Clinical Trial. J. Clin. Med. 2021, 10, 2486. https://doi.org/10.3390/jcm10112486
Ryu J-H, Park J-W, Choi SI, Kim JY, Lee H, Yoo H-J, Han S-H. Virtual Reality vs. Tablet Video as an Experiential Education Platform for Pediatric Patients Undergoing Chest Radiography: A Randomized Clinical Trial. Journal of Clinical Medicine. 2021; 10(11):2486. https://doi.org/10.3390/jcm10112486
Chicago/Turabian StyleRyu, Jung-Hee, Jin-Woo Park, Sang Il Choi, Ji Young Kim, Hyunju Lee, Hee-Jeong Yoo, and Sung-Hee Han. 2021. "Virtual Reality vs. Tablet Video as an Experiential Education Platform for Pediatric Patients Undergoing Chest Radiography: A Randomized Clinical Trial" Journal of Clinical Medicine 10, no. 11: 2486. https://doi.org/10.3390/jcm10112486
APA StyleRyu, J.-H., Park, J.-W., Choi, S. I., Kim, J. Y., Lee, H., Yoo, H.-J., & Han, S.-H. (2021). Virtual Reality vs. Tablet Video as an Experiential Education Platform for Pediatric Patients Undergoing Chest Radiography: A Randomized Clinical Trial. Journal of Clinical Medicine, 10(11), 2486. https://doi.org/10.3390/jcm10112486