
Vitamin D Levels in COVID-19 Outpatients from Western Mexico: Clinical Correlation and Effect of Its Supplementation

 , , , ,
, , , ,  ,
,  , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Clinical Assessment
2.3. Laboratory Determinations
2.4. Statistical Analysis
3. Results
3.1. Demographic and Clinical Features of Vitamin D Supplemented and Non-Supplemented COVID-19 Outpatients at Baseline
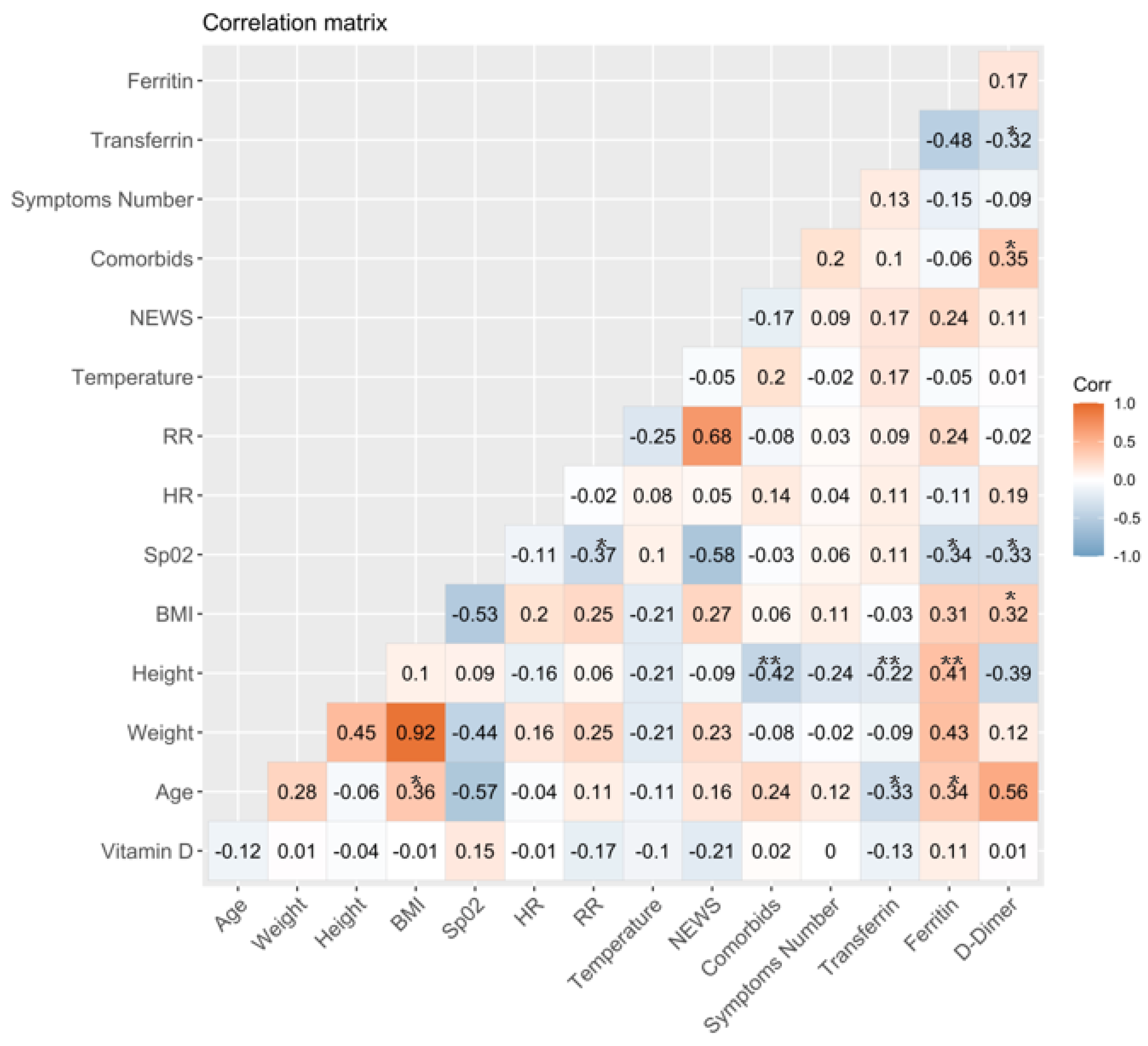
3.2. Association between Vitamin D Serum Levels and Clinical and Laboratory Variables at Baseline
3.3. Comparison between Laboratory Parameters and Clinical Features of Outpatients with or without Sufficient Levels of Total Vitamin D
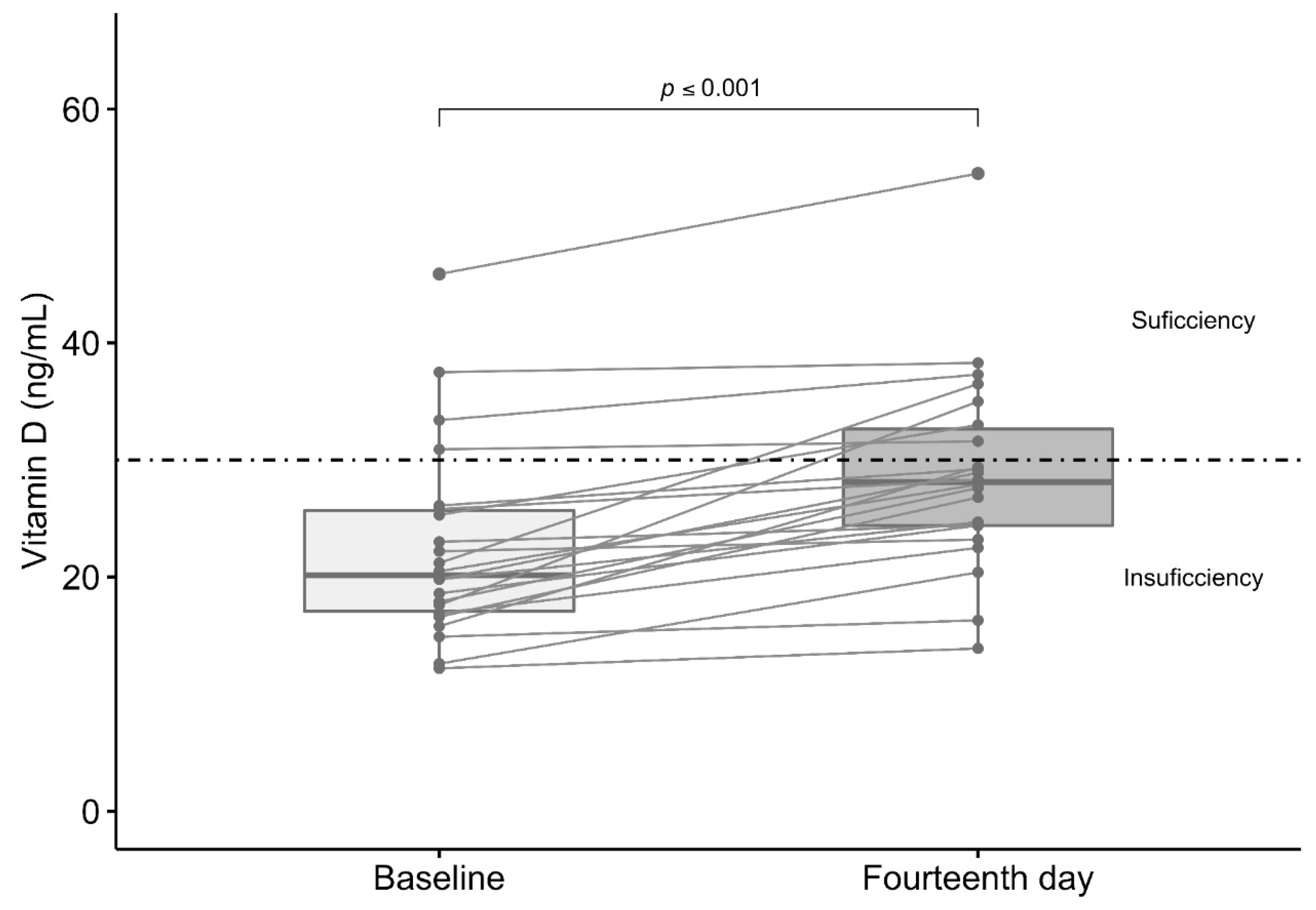
3.4. Effect of Vitamin D3 Supplementation in Total Serum Levels of Vitamin D
3.5. Comparison between Symptoms, Treatment, and Viral Load in Supplemented and Non-Supplemented Outpatients Study Groups
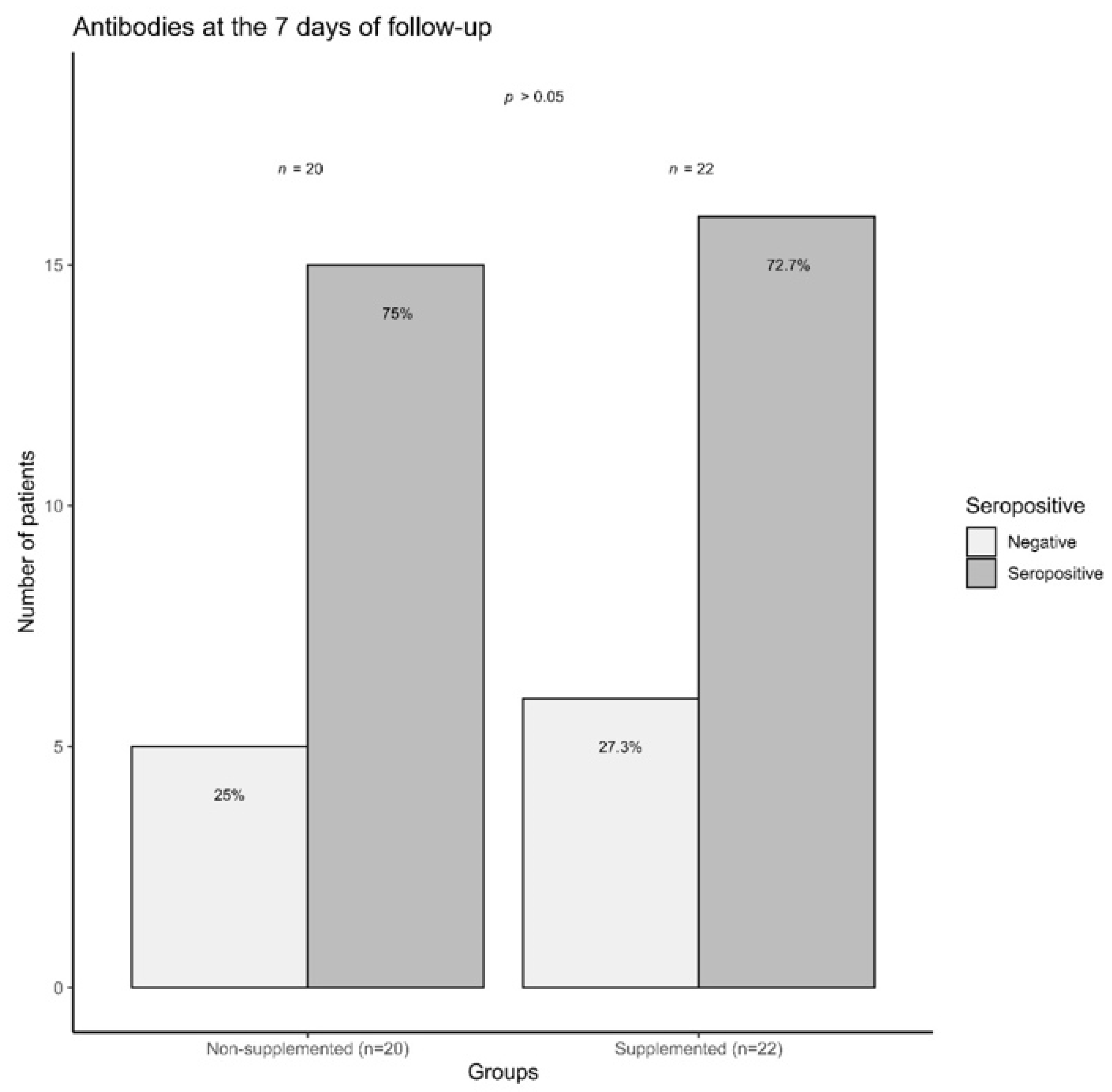
3.6. COVID-19 Outpatients Seropositivity Rate on the Seventh Day of Follow-Up
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tay, M.Z.; Poh, C.M.; Rénia, L.; MacAry, P.A.; Ng, L.F.P. The Trinity of COVID-19: Immunity, Inflammation and Intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus Disease (COVID-19) Situation Reports. Available online: https://covid19.who.int (accessed on 15 March 2021).
- Mortality Analyses—Johns Hopkins Coronavirus Resource. Available online: https://coronavirus.jhu.edu/data/mortality (accessed on 15 March 2021).
- Conti, P. Induction of Pro-Inflammatory Cytokines (IL-1 and IL-6) and Lung Inflammation by COVID-19: Anti-Inflammatory Strategies. J. Biol. Regul. Homeost. Agents 2020, 34, 1. [Google Scholar] [CrossRef] [PubMed]
- Ebadi, M.; Montano-Loza, A.J. Perspective: Improving Vitamin D Status in the Management of COVID. Eur. J. Clin. Nutr. 2020, 74, 856–859. [Google Scholar] [CrossRef] [PubMed]
- Velavan, T.P.; Meyer, C.G. Mild versus Severe COVID-19: Laboratory Markers. Int. J. Infect. Dis. 2020, 95, 304–307. [Google Scholar] [CrossRef]
- Bolondi, G.; Russo, E.; Gamberini, E.; Circelli, A.; Meca, M.C.C.; Brogi, E.; Viola, L.; Bissoni, L.; Poletti, V.; Agnoletti, V. Iron Metabolism and Lymphocyte Characterisation during Covid-19 Infection in ICU Patients: An Observational Cohort Study. World J. Emerg. Surg. 2020, 15, 41. [Google Scholar] [CrossRef]
- Dai, X. ABO Blood Group Predisposes to COVID-19 Severity and Cardiovascular Diseases. Eur. J. Prev. Cardiol. 2020, 27, 1436–1437. [Google Scholar] [CrossRef]
- Latz, C.A.; DeCarlo, C.; Boitano, L.; Png, C.Y.M.; Patell, R.; Conrad, M.F.; Eagleton, M.; Dua, A. Blood Type and Outcomes in Patients with COVID-19. Ann. Hematol. 2020, 99, 2113–2118. [Google Scholar] [CrossRef] [PubMed]
- de Lucena, T.M.C.; da Silva Santos, A.F.; de Lima, B.R.; de Albuquerque Borborema, M.E.; de Azevêdo Silva, J. Mechanism of Inflammatory Response in Associated Comorbidities in COVID. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 597–600. [Google Scholar] [CrossRef]
- Sanyaolu, A.; Okorie, C.; Marinkovic, A.; Patidar, R.; Younis, K.; Desai, P.; Hosein, Z.; Padda, I.; Mangat, J.; Altaf, M. Comorbidity and Its Impact on Patients with COVID. SN Compr. Clin. Med. 2020, 2, 1069–1076. [Google Scholar] [CrossRef]
- Shahid, Z.; Kalayanamitra, R.; McClafferty, B.; Kepko, D.; Ramgobin, D.; Patel, R.; Aggarwal, C.S.; Vunnam, R.; Sahu, N.; Bhatt, D.; et al. COVID -19 and Older Adults: What We Know. J. Am. Geriatr. Soc. 2020, 68, 926–929. [Google Scholar] [CrossRef]
- Malaguarnera, L. Vitamin D3 as Potential Treatment Adjuncts for COVID. Nutrients 2020, 12, 3512. [Google Scholar] [CrossRef]
- Turrubiates-Hernández, F.; Sánchez-Zuno, G.; González-Estevez, G.; Hernández-Bello, J.; Macedo-Ojeda, G.; Muñoz-Valle, J. Potential Immunomodulatory Effects of Vitamin D in the Prevention of Severe Coronavirus Disease 2019: An Ally for Latin America (Review). Int. J. Mol. Med. 2021, 47, 32. [Google Scholar] [CrossRef]
- Shi, Y.-Y.; Liu, T.-J.; Fu, J.-H.; Xu, W.; Wu, L.-L.; Hou, A.-N.; Xue, X.-D. Vitamin D/VDR Signaling Attenuates Lipopolysaccharide-Induced Acute Lung Injury by Maintaining the Integrity of the Pulmonary Epithelial Barrier. Mol. Med. Rep. 2016, 13, 1186–1194. [Google Scholar] [CrossRef]
- Xu, J.; Yang, J.; Chen, J.; Luo, Q.; Zhang, Q.; Zhang, H. Vitamin D Alleviates Lipopolysaccharide-Induced Acute Lung Injury via Regulation of the Renin-Angiotensin System. Mol. Med. Rep. 2017, 16, 7432–7438. [Google Scholar] [CrossRef]
- Greiller, C.; Martineau, A. Modulation of the Immune Response to Respiratory Viruses by Vitamin D. Nutrients 2015, 7, 4240–4270. [Google Scholar] [CrossRef] [PubMed]
- Baeke, F.; Takiishi, T.; Korf, H.; Gysemans, C.; Mathieu, C. Vitamin D: Modulator of the Immune System. Curr. Opin. Pharmacol. 2010, 10, 482–496. [Google Scholar] [CrossRef] [PubMed]
- Yılmaz, K.; Şen, V. Is Vitamin D Deficiency a Risk Factor for COVID-19 in Children? Pediatr. Pulmonol. 2020, 55, 3595–3601. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, D.O.; Best, T.J.; Zhang, H.; Vokes, T.; Arora, V.; Solway, J. Association of Vitamin D Status and Other Clinical Characteristics With COVID-19 Test Results. JAMA Netw. Open 2020, 3, e2019722. [Google Scholar] [CrossRef] [PubMed]
- Mohan, M.; Cherian, J.J.; Sharma, A. Exploring Links between Vitamin D Deficiency and COVID. PLoS Pathog. 2020, 16, e1008874. [Google Scholar] [CrossRef]
- Radujkovic, A.; Hippchen, T.; Tiwari-Heckler, S.; Dreher, S.; Boxberger, M.; Merle, U. Vitamin D Deficiency and Outcome of COVID-19 Patients. Nutrients 2020, 12, 2757. [Google Scholar] [CrossRef]
- Whittemore, P.B. COVID-19 Fatalities, Latitude, Sunlight, and Vitamin D. Am. J. Infect. Control 2020, 48, 1042–1044. [Google Scholar] [CrossRef] [PubMed]
- McCartney, D.M.; O’Shea, P.M.; Faul, J.L.; Healy, M.J.; Byrne, G.; Griffin, T.P.; Walsh, J.B.; Byrne, D.G.; Kenny, R.A. Vitamin D and SARS-CoV-2 Infection—Evolution of Evidence Supporting Clinical Practice and Policy Development: A Position Statement from the Covit-D Consortium. Ir. J. Med. Sci. 1971. 2020. [Google Scholar] [CrossRef]
- Grant, W.B.; Lahore, H.; McDonnell, S.L.; Baggerly, C.A.; French, C.B.; Aliano, J.L.; Bhattoa, H.P. Evidence That Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths. Nutrients 2020, 12, 988. [Google Scholar] [CrossRef]
- Smith, G.B.; Prytherch, D.R.; Meredith, P.; Schmidt, P.E.; Featherstone, P.I. The Ability of the National Early Warning Score (NEWS) to Discriminate Patients at Risk of Early Cardiac Arrest, Unanticipated Intensive Care Unit Admission, and Death. Resuscitation 2013, 84, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Kuriacose, R.; Olive, K.E. Vitamin D Insufficiency/Deficiency Management. South. Med. J. 2014, 107, 66–70. [Google Scholar] [CrossRef]
- Cheng, L.; Li, H.; Li, L.; Liu, C.; Yan, S.; Chen, H.; Li, Y. Ferritin in the Coronavirus Disease 2019 (COVID-19): A Systematic Review and Meta-analysis. J. Clin. Lab. Anal. 2020, 34. [Google Scholar] [CrossRef] [PubMed]
- Terpos, E.; Ntanasis-Stathopoulos, I.; Elalamy, I.; Kastritis, E.; Sergentanis, T.N.; Politou, M.; Psaltopoulou, T.; Gerotziafas, G.; Dimopoulos, M.A. Hematological Findings and Complications of COVID. Am. J. Hematol. 2020, 95, 834–847. [Google Scholar] [CrossRef] [PubMed]
- Yuan, X.; Huang, W.; Ye, B.; Chen, C.; Huang, R.; Wu, F.; Wei, Q.; Zhang, W.; Hu, J. Changes of Hematological and Immunological Parameters in COVID-19 Patients. Int. J. Hematol. 2020, 112, 553–559. [Google Scholar] [CrossRef] [PubMed]
- Weitz, J.I.; Fredenburgh, J.C.; Eikelboom, J.W. A Test in Context: D-Dimer. J. Am. Coll. Cardiol. 2017, 70, 2411–2420. [Google Scholar] [CrossRef] [PubMed]
- Linkins, L.-A.; Takach Lapner, S. Review of D-Dimer Testing: Good, Bad, and Ugly. Int. J. Lab. Hematol. 2017, 39, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Taneri, P.E.; Gómez-Ochoa, S.A.; Llanaj, E.; Raguindin, P.F.; Rojas, L.Z.; Roa-Díaz, Z.M.; Salvador, D.; Groothof, D.; Minder, B.; Kopp-Heim, D.; et al. Anemia and Iron Metabolism in COVID-19: A Systematic Review and Meta-Analysis. Eur. J. Epidemiol. 2020, 35, 763–773. [Google Scholar] [CrossRef] [PubMed]
- Kell, D.B.; Pretorius, E. Serum Ferritin Is an Important Inflammatory Disease Marker, as It Is Mainly a Leakage Product from Damaged Cells. Metallomics 2014, 6, 748–773. [Google Scholar] [CrossRef] [PubMed]
- Fu, Y.; Bruce, K.E.; Wu, H.; Giedroc, D.P. The S2 Cu( i ) Site in CupA from Streptococcus Pneumoniae Is Required for Cellular Copper Resistance. Metallomics 2016, 8, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Park, H.K.; Kwon, M.-J.; Ham, S.-Y.; Kim, J.M.; Lim, S.-Y.; Song, J.-U. Decreased Lung Function Is Associated with Elevated Ferritin but Not Iron or Transferrin Saturation in 42,927 Healthy Korean Men: A Cross-Sectional Study. PLoS ONE 2020, 15, e0231057. [Google Scholar] [CrossRef]
- Franco, C.K.; Silva, D.R.; Barreto, S.S.M. Relationship of Body Mass Index and Waist-to-Hip Ratio with Fibrinolytic Activity Measured as d-Dimer. Obes. Res. Clin. Pract. 2011, 5, e37–e41. [Google Scholar] [CrossRef]
- Shitrit, D.; Peled, N.; Shitrit, A.B.-G.; Meidan, S.; Bendayan, D.; Sahar, G.; Kramer, M.R. An Association between Oxygen Desaturation and D-Dimer in Patients with Obstructive Sleep Apnea Syndrome. Thromb. Haemost. 2005, 94, 544–547. [Google Scholar] [CrossRef]
- Rastogi, A.; Bhansali, A.; Khare, N.; Suri, V.; Yaddanapudi, N.; Sachdeva, N.; Puri, G.D.; Malhotra, P. Short Term, High-Dose Vitamin D Supplementation for COVID-19 Disease: A Randomised, Placebo-Controlled, Study (SHADE Study). Postgrad. Med. J. 2020. [Google Scholar] [CrossRef]
- Martineau, A.R.; Jolliffe, D.A.; Hooper, R.L.; Greenberg, L.; Aloia, J.F.; Bergman, P.; Dubnov-Raz, G.; Esposito, S.; Ganmaa, D.; Ginde, A.A.; et al. Vitamin D Supplementation to Prevent Acute Respiratory Tract Infections: Systematic Review and Meta-Analysis of Individual Participant Data. BMJ 2017, i6583. [Google Scholar] [CrossRef]
- Dancer, R.C.A.; Parekh, D.; Lax, S.; D’Souza, V.; Zheng, S.; Bassford, C.R.; Park, D.; Bartis, D.G.; Mahida, R.; Turner, A.M.; et al. Vitamin D Deficiency Contributes Directly to the Acute Respiratory Distress Syndrome (ARDS). Thorax 2015, 70, 617–624. [Google Scholar] [CrossRef]
- O’Brien, K.M.; Sandler, D.P.; Taylor, J.A.; Weinberg, C.R. Serum Vitamin D and Risk of Breast Cancer within Five Years. Environ. Health Perspect. 2017, 125, 077004. [Google Scholar] [CrossRef]
- Jolliffe, D.A.; Greenberg, L.; Hooper, R.L.; Griffiths, C.J.; Camargo, C.A.; Kerley, C.P.; Jensen, M.E.; Mauger, D.; Stelmach, I.; Urashima, M.; et al. Vitamin D Supplementation to Prevent Asthma Exacerbations: A Systematic Review and Meta-Analysis of Individual Participant Data. Lancet Respir. Med. 2017, 5, 881–890. [Google Scholar] [CrossRef]
- Bedolla-Barajas, M.; López-Hernández, J.C.; García-Padilla, L.F.; Morales-Romero, J.; Velarde-Rivera, F.A.; Robles-Figueroa, M.; Ortiz-Peregrina, J.R. Prevalencia de insuficiencia y deficiencia de vitamina D en adultos mexicanos con asma alérgica. Rev. Alerg. México 2017, 64, 178. [Google Scholar] [CrossRef] [PubMed]
- Azrielant, S.; Shoenfeld, Y. Vitamin D and the Immune System. Israel Med. Assoc. J. 2017, 19, 510–511. [Google Scholar]
- Hansen, K.E.; Johnson, M.G. An Update on Vitamin D for Clinicians. Curr. Opin. Endocrinol. Diabetes Obes. 2016, 23, 440–444. [Google Scholar] [CrossRef] [PubMed]
- Clark, P.; Vivanco-Muñoz, N.; Piña, J.T.; Rivas-Ruiz, R.; Huitrón, G.; Chico-Barba, G.; Reza-Albarrán, A.A. High Prevalence of Hypovitaminosis D in Mexicans Aged 14 Years and Older and Its Correlation with Parathyroid Hormone. Arch. Osteoporos. 2015, 10, 19. [Google Scholar] [CrossRef] [PubMed]
- Pinzon, R.T.; Angela; Pradana, A.W. Vitamin D Deficiency among Patients with COVID-19: Case Series and Recent Literature Review. Trop. Med. Health 2020, 48, 102. [Google Scholar] [CrossRef]
- Nowaczewska, M.; Wiciński, M.; Osiński, S.; Kaźmierczak, H. The Role of Vitamin D in Primary Headache–from Potential Mechanism to Treatment. Nutrients 2020, 12, 243. [Google Scholar] [CrossRef]
- Ye, K.; Tang, F.; Liao, X.; Shaw, B.A.; Deng, M.; Huang, G.; Qin, Z.; Peng, X.; Xiao, H.; Chen, C.; et al. Does Serum Vitamin D Level Affect COVID-19 Infection and Its Severity?-A Case-Control Study. J. Am. Coll. Nutr. 2020, 1–8. [Google Scholar] [CrossRef]
- Jain, A.; Chaurasia, R.; Sengar, N.S.; Singh, M.; Mahor, S.; Narain, S. Analysis of Vitamin D Level among Asymptomatic and Critically Ill COVID-19 Patients and Its Correlation with Inflammatory Markers. Sci. Rep. 2020, 10, 20191. [Google Scholar] [CrossRef]
- Ajabshir, S. The Effects of Vitamin D on the Renin-Angiotensin System. Eff. Vitam. Renin. Angiotensin Syst. 2014. [Google Scholar] [CrossRef]
- Martínez-Zavala, N.; López-Sánchez, G.N.; Vergara-Lopez, A.; Chávez-Tapia, N.C.; Uribe, M.; Nuño-Lámbarri, N. Vitamin D Deficiency in Mexicans Have a High Prevalence: A Cross-Sectional Analysis of the Patients from the Centro Médico Nacional 20 de Noviembre. Arch. Osteoporos. 2020, 15, 88. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | n = 42 | Supplemented Outpatients n = 22 | Non-Supplemented Outpatients n = 20 | p-Value |
|---|---|---|---|---|
| Age (years) a | 43.0 (20–74) | 44.0 (20.0–71.0) | 43.0 (21.0–78.0) | 0.66 |
| Females b | 22 (52.3) | 7 (31.8) | 6 (30.0) | 1.00 |
| BMI (kg/m2) a | 25.5 (18.1–41.2) | 25.4 (19.7–41.2) | 26.3 (18.1–35.0) | 0.95 |
| Comorbidities | ||||
| 7 (16.7) | 4 (18.2) | 3 (15.0) | 0.55 |
| 4 (9.5) | 2 (9.1) | 2 (10.0) | 1.00 |
| 2 (4.8) | 0 (0.0) | 2 (10.0) | 0.22 |
| 1 (2.4) | 1 (2.4) | 0 (0.0) | 1.00 |
| Treatment | 30 (71.4) | 15 (68.2) | 15 (75.0) | 0.88 |
| 22 (52.4) | 12 (54.5) | 10 (50.0) | 1.00 |
| 17 (40.5) | 7 (31.8) | 10 (50.0) | 0.37 |
| 8 (19.0) | 2 (9.1) | 6 (30.0) | 0.12 |
| 6 (14.3) | 3 (13.6) | 3 (15.0) | 1.00 |
| 5 (11.9) | 1 (4.5) | 4 (20.0) | 0.17 |
| 10 (23.8) | 5 (22.7) | 5 (25.0) | 1.00 |
| Laboratory parameters | ||||
| 129.5 (6.62–842.0) | 72.8 (8.6–419.0) | 153.0 (6.62–842) | 0.05 |
| 286.1 (100–2825.6) | 306.7 (100–2825.6) | 263.6 (186.0–1038.5) | 0.89 |
| 236.0 (171.0–376.0) | 254.0 (193.0–376.0) | 226.0 (171.0–297) | 0.03 |
| Total vitamin D (ng/mL) a | 22.4 (12.1–45.9) | 20.2 (12.2–45.9) | 23.4 (12.1–45.6) | 0.06 |
| Sufficient vitamin D b | 8 (19.0) | 4 (18.2) | 4 (20.0) | 1.00 |
| Variable | Outpatients with Insufficient Levels of Vitamin D n = 34 | Outpatients with Sufficient Levels of Vitamin D n = 8 | p-Values |
|---|---|---|---|
| Age (years) a | 45 (20–74) | 38.5 (36–64) | 0.42 |
| Comorbid b | 11 (32.4) | 2 (25.0) | 0.70 |
| BMI (kg/m2) a | 25.5 (18.1–39.2) | 25.9 (19.6–41.2) | 0.75 |
| Symptoms b | 34 (100.0) | 6 (75.0) | 0.03 |
| >1 symptom b | 31 (91.2) | 5 (62.5) | 0.03 |
| >2 symptoms b | 27 (79.4) | 5 (62.5) | 0.37 |
| >3 symptoms b | 23 (67.6) | 4 (50.0) | 0.42 |
| >4 more symptoms b | 18 (52.9) | 4 (50.0) | 0.59 |
| Number of symptoms a | 6 (0–11) | 5 (0–10) | 0.36 |
| Treatment b | 24 (72.7) | 6 (75.0) | 0.89 |
| Laboratory parameters | |||
| 237.0 (178.0–376.0) | 234 (171.0–289.0) | 0.72 |
| 119–5 (6.6–842.0) | 186.5 (70.5-453) | 0.18 |
| 278.4 (100.0–1239.9) | 3310.4 (128.9–2825.6) | 0.56 |
| Baseline | 7 Days | 14 Days | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | Supplemented Outpatients n = 22 | Non-supplemented Outpatients n = 20 | p-Value | Supplemented Outpatients n = 22 | Non-supplemented Outpatients n = 20 | p-Value | Supplemented Outpatients n = 22 | Non-Supplemented Outpatients n = 20 | p-Value |
| Presence of symptoms | 21 (95.5) | 19 (95.0) | 1.00 | 13 (59.1) | 9 (45.0) | 0.53 | 14 (63.6) | 8 (40.0) | 0.22 |
| >1 symptom a | 18 (81.8) | 18 (90.0) | 0.66 | 5 (22.7) | 6 (30.0) | 0.43 | 6 (27.3) | 6 (30.0) | 1.00 |
| >2 symptoms a | 17 (77.3) | 15 (75.0) | 1.00 | 2 (9.1) | 4 (20.0) | 0.28 | 4 (18.2) | 4 (20.0) | 0.59 |
| >3 symptoms a | 14 (63.6) | 13 (65.0) | 1.00 | 0 (0.0) | 4 (20.0) | 0.04 | 0 (0.0) | 4 (20.0) | 0.04 |
| NEWS score b | 4 (0–9) | 3 (0–7) | 0.14 | --- | ---- | --- | --- | ---- | --- |
| Treatment a | 15 (68.2) | 15 (75.0) | 0.88 | 7 (31.8) | 8 (40.0) | 0.81 | 4 (18.2) | 4 (20.0) | 0.88 |
| Analgesic a | 12 (54.5) | 10 (50.0) | 1.00 | 2 (9.1) | 3 (15.0) | 0.57 | 2 (9.1) | 3 (15.0) | 0.65 |
| Antipyretic a | 7 (31.8) | 10 (50.0) | 0.35 | 4 (18.2) | 6 (30.0) | 0.53 | 1 (4.5) | 3 (15.0) | 0.27 |
| Antibiotic a | 2 (9.1) | 6 (30.0) | 0.12 | 0 (0.0) | 2 (10.0) | 0.12 | 1 (4.5) | 0 (0.0) | 1.00 |
| Antihistamine a | 3 (13.6) | 3 (15.0) | 1.00 | 1 (4.5) | 0 (0.0) | 1.00 | 0 (0.0) | 0 (0.0) | --- |
| Anticoagulant a | 1 (4.5) | 4 (20.0) | 0.17 | 0 (0.0) | 1 (5.0) | 1.00 | 0 (0.0) | 0 (0.0) | --- |
| Other drugs a | 5 (22.7) | 5 (25.0) | 1.00 | 4 (18.8) | 3 (15.0) | 1.00 | 0 (0.0) | 0 (0.0) | --- |
| Positive RT-PCR test a | 22 (100.0) | 20 (100.0) | --- | 12 (60.0) | 12 (54.5) | 0.97 | 1 (5.0) | 0 (0.0) | 0.47 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Zuno, G.A.; González-Estevez, G.; Matuz-Flores, M.G.; Macedo-Ojeda, G.; Hernández-Bello, J.; Mora-Mora, J.C.; Pérez-Guerrero, E.E.; García-Chagollán, M.; Vega-Magaña, N.; Turrubiates-Hernández, F.J.; et al. Vitamin D Levels in COVID-19 Outpatients from Western Mexico: Clinical Correlation and Effect of Its Supplementation. J. Clin. Med. 2021, 10, 2378. https://doi.org/10.3390/jcm10112378
Sánchez-Zuno GA, González-Estevez G, Matuz-Flores MG, Macedo-Ojeda G, Hernández-Bello J, Mora-Mora JC, Pérez-Guerrero EE, García-Chagollán M, Vega-Magaña N, Turrubiates-Hernández FJ, et al. Vitamin D Levels in COVID-19 Outpatients from Western Mexico: Clinical Correlation and Effect of Its Supplementation. Journal of Clinical Medicine. 2021; 10(11):2378. https://doi.org/10.3390/jcm10112378
Chicago/Turabian StyleSánchez-Zuno, Gabriela Athziri, Guillermo González-Estevez, Mónica Guadalupe Matuz-Flores, Gabriela Macedo-Ojeda, Jorge Hernández-Bello, Jesús Carlos Mora-Mora, Edsaúl Emilio Pérez-Guerrero, Mariel García-Chagollán, Natali Vega-Magaña, Francisco Javier Turrubiates-Hernández, and et al. 2021. "Vitamin D Levels in COVID-19 Outpatients from Western Mexico: Clinical Correlation and Effect of Its Supplementation" Journal of Clinical Medicine 10, no. 11: 2378. https://doi.org/10.3390/jcm10112378
APA StyleSánchez-Zuno, G. A., González-Estevez, G., Matuz-Flores, M. G., Macedo-Ojeda, G., Hernández-Bello, J., Mora-Mora, J. C., Pérez-Guerrero, E. E., García-Chagollán, M., Vega-Magaña, N., Turrubiates-Hernández, F. J., Machado-Sulbaran, A. C., & Muñoz-Valle, J. F. (2021). Vitamin D Levels in COVID-19 Outpatients from Western Mexico: Clinical Correlation and Effect of Its Supplementation. Journal of Clinical Medicine, 10(11), 2378. https://doi.org/10.3390/jcm10112378