
Evaluation of the Efficacy of Lacer HaliTM Treatment on the Management of Halitosis: A Randomized Double-Blind Clinical Trial



Abstract
1. Introduction
2. Materials and Methods
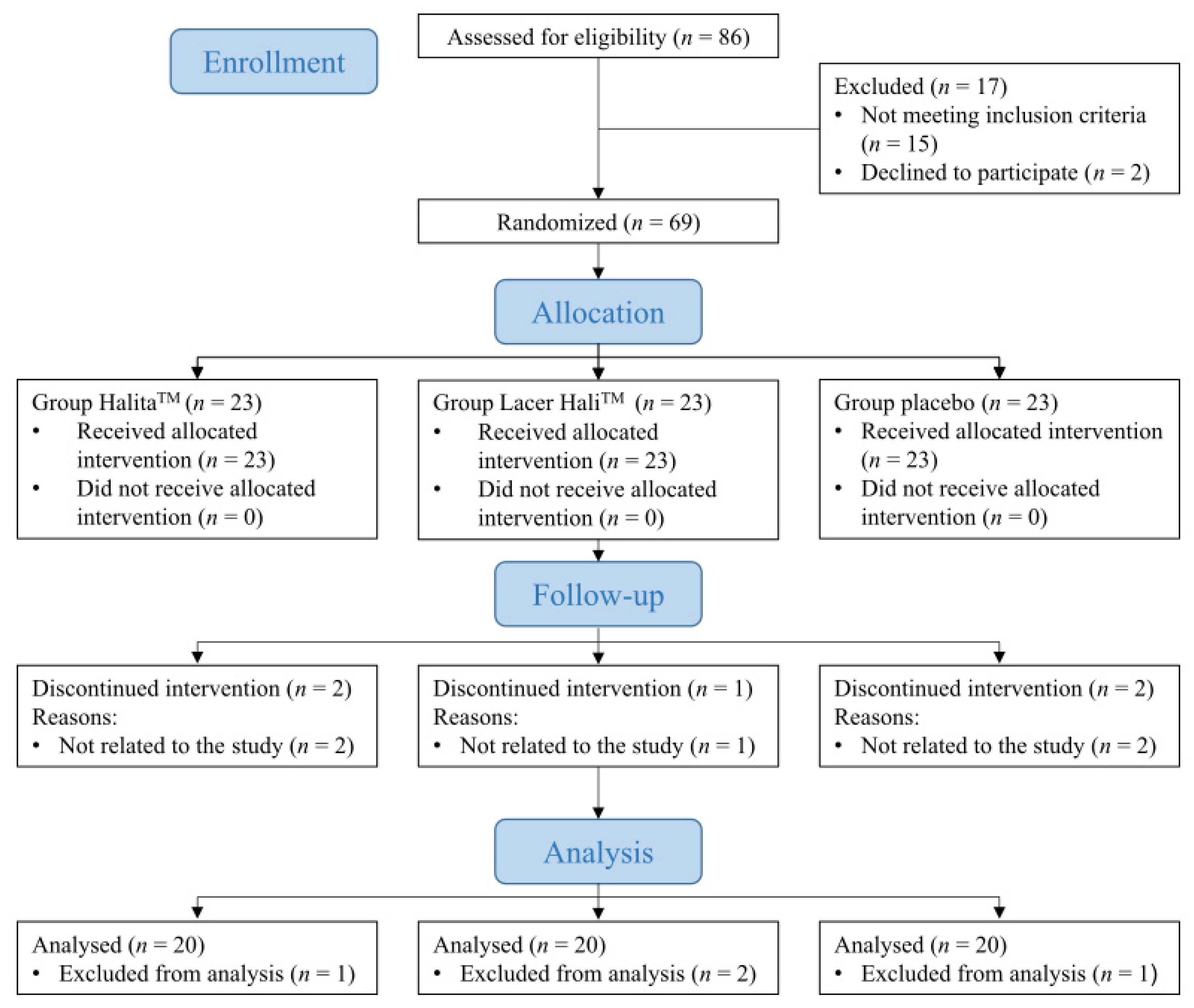
2.1. Experimental Design
2.2. Patient Population
2.3. Patient Follow-Up
2.3.1. Baseline Visit
2.3.2. Follow-Up Visits
2.3.3. Final Visit (T4)
2.4. Procedure and Adverse Events
2.5. Data Analysis
3. Results
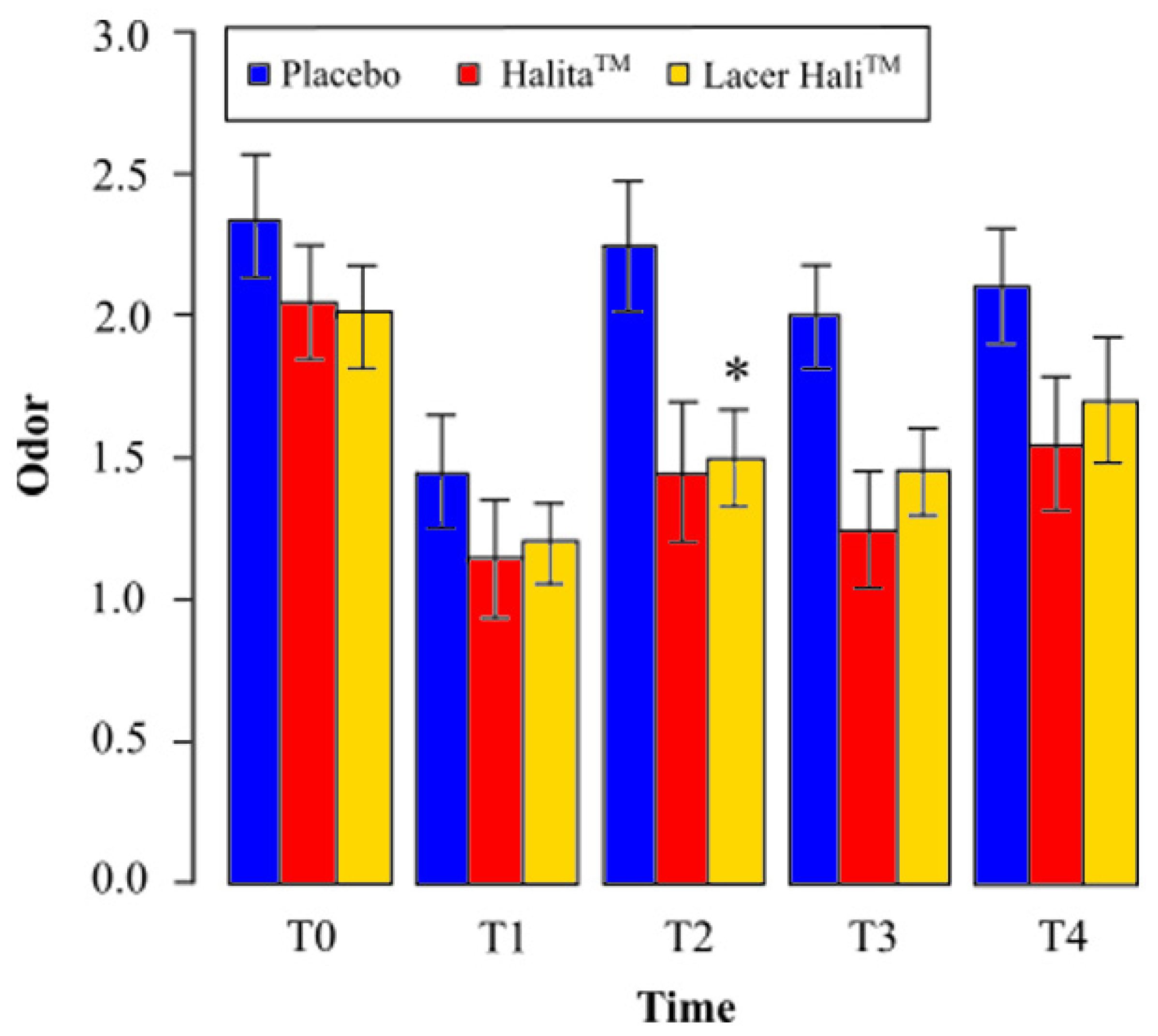
3.1. Analysis of the Organoleptic Test
3.1.1. Lacer HaliTM vs. Placebo
3.1.2. Lacer HaliTM vs. HalitaTM
3.2. Analysis of Gases (VCS)
3.2.1. Lacer HaliTM vs. Placebo
3.2.2. Lacer HaliTM vs. HalitaTM
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Silva, M.F.; Leite, F.R.M.; Ferreira, L.B.; Pola, N.M.; Scannapieco, F.A.; Demarco, F.F.; Nascimento, G.G. Estimated prevalence of halitosis: A systematic review and meta-regression analysis. Clin. Oral Investig. 2018, 22, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Quirynen, M.; Mongardini, C.; van Steenberghe, D. The effect of a 1-stage full-mouth disinfection on oral malodor and microbial colonization of the tongue in periodontitis. A pilot study. J. Periodontol. 1998, 69, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Tangerman, A. Halitosis in medicine: A review. Int. Dent. J. 2002, 52 (Suppl. 3), 201–206. [Google Scholar] [CrossRef] [PubMed]
- Porter, S.R.; Scully, C. Oral malodour (halitosis). Br. Med. J. 2006, 333, 632–635. [Google Scholar] [CrossRef] [PubMed]
- Van der Sluijs, E.; Slot, D.E.; Bakker, E.W.P.; Van der Weijden, G.A. The effect of water on morning bad breath: A randomized clinical trial. Int. J. Dent. Hyg. 2016, 14, 124–134. [Google Scholar] [CrossRef] [PubMed]
- Van Steenberghe, D. Breath malodor. Curr. Opin. Periodontol. 1997, 4, 137–143. [Google Scholar] [PubMed]
- Bosy, A.; Kulkarni, G.V.; Rosenberg, M.; McCulloch, C.A.G. Relationship of Oral Malodor to Periodontitis: Evidence of Independence in Discrete Subpopulations. J. Periodontol. 1994, 65, 37–46. [Google Scholar] [CrossRef]
- Inchingolo, F.; Tatullo, M.; Abenavoli, F.M.; Marrelli, M.; Inchingolo, A.D.; Palladino, A.; Inchingolo, A.M.; Dipalma, G. Oral piercing and oral diseases: A short time retrospective study. Int. J. Med. Sci. 2011, 8, 649–652. [Google Scholar] [CrossRef] [PubMed]
- Marrelli, M.; Tatullo, M.; Dipalma, G.; Inchingolo, F. Oral infection by Staphylococcus aureus in patients affected by White Sponge Nevus: A description of two cases occurred in the same family. Int. J. Med. Sci. 2012, 9, 47–50. [Google Scholar] [CrossRef]
- Inchingolo, F.; Tatullo, M.; Abenavoli, F.M.; Marrelli, M.; Inchingolo, A.D.; Inchingolo, A.M.; Dipalma, G. Non-Hodgkin lymphoma affecting the tongue: Unusual intra-oral location. Head Neck Oncol. 2011, 3, 1. [Google Scholar] [CrossRef]
- Quirynen, M.; Zhao, H.; van Steenberghe, D. Review of the treatment strategies for oral malodour. Clin. Oral Investig. 2002, 6, 1–10. [Google Scholar] [CrossRef]
- Carvalho, M.D.; Tabchoury, C.M.; Cury, J.A.; Toledo, S.; Nogueira-Filho, G.R. Impact of mouthrinses on morning bad breath in healthy subjects. J. Clin. Periodontol. 2004, 31, 85–90. [Google Scholar] [CrossRef]
- Farrell, S.; Baker, R.A.; Somogyi-Mann, M.; Witt, J.J.; Gerlach, R.W. Oral malodor reduction by a combination of chemotherapeutical and mechanical treatments. Clin. Oral Investig. 2006, 10, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Greenman, J.; Duffield, J.; Spencer, P.; Rosenberg, M.; Corry, D.; Saad, S.; Lenton, P.; Majerus, G.; Nachnani, S.; El-Maaytah, M. Study on the organoleptic intensity scale for measuring oral malodor. J. Dent. Res. 2004, 83, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.-J.; Lee, J.-Y.; Kho, H.-S.; Chung, J.-W.; Park, H.-K.; Kim, Y.-K. A New Organoleptic Testing Method for Evaluating Halitosis. J. Periodontol. 2009, 80, 93–97. [Google Scholar] [CrossRef]
- Tangerman, A.; Winkel, E.G. The portable gas chromatograph OralChromaTM: A method of choice to detect oral and extra-oral halitosis. J. Breath Res. 2008, 2. [Google Scholar] [CrossRef]
- Rösing, C.K.; Jonski, G.; Rølla, G. Comparative analysis of some mouthrinses on the production of volatile sulfur-containing compounds. Acta Odontol. Scand. 2002, 60, 10–12. [Google Scholar] [CrossRef]
- Addy, M.; Moran, J.; Wade, W. Chemical Plaque Control in the Prevention of Gingivitis and Periodontitis. In Proceedings of the 1st European Workshop in Periodontology, Thurgau, Switzerland, 1–4 February 1993; Quintessence: London, UK, 1994. [Google Scholar]
- Blom, T.; Slot, D.E.; Quirynen, M.; Van der Weijden, G.A. The effect of mouthrinses on oral malodor: A systematic review. Int. J. Dent. Hyg. 2012, 10, 209–222. [Google Scholar] [CrossRef]
- Jamali, Z.; Alipour, M.; Ebrahimi, S.; Aghazadeh, M. Effect of Halita mouthwash on oral halitosis treatment: A randomized triple-blind clinical trial. J. Dent. Res. Dent. Clin. Dent. Prospect. 2019, 13, 31–35. [Google Scholar] [CrossRef]
- Roldán, S.; Winkel, E.G.; Herrera, D.; Sanz, M.; Van Winkelhoff, A.J. The effects of a new mouthrinse containing chlorhexidine, cetylpyridinium chloride and zinc lactate on the microflora of oral halitosis patients: A dual-centre, double-blind placebo-controlled study. J. Clin. Periodontol. 2003, 30, 427–434. [Google Scholar] [CrossRef]
- Roldán, S.; Herrera, D.; Santa-Cruz, I.; O’Connor, A.; González, I.; Sanz, M. Comparative effects of different chlorhexidine mouth-rinse formulations on volatile sulphur compounds and salivary bacterial counts. J. Clin. Periodontol. 2004, 31, 1128–1134. [Google Scholar] [CrossRef] [PubMed]
- Fedorowicz, Z.; Aljufairi, H.; Nasser, M.; Outhouse, T.L.; Pedrazzi, V. Mouthrinses for the treatment of halitosis. Cochrane Database Syst. Rev. 2008. [Google Scholar] [CrossRef]
- Slot, D.E.; De Geest, S.; Van Der Weijden, F.A.; Quirynen, M. Treatment of oral malodour. Medium-term efficacy of mechanical and/or chemical agents: A systematic review. J. Clin. Periodontol. 2015, 42, S303–S316. [Google Scholar] [CrossRef] [PubMed]
- Dadamio, J.; Tournout, M.; Teughels, W.; Dekeyser, C.; Coucke, W.; Quirynen, M. Efficacy of different mouthrinse formulations in reducing oral malodour: A randomized clinical trial. J. Clin. Periodontol. 2013, 40, 505–513. [Google Scholar] [CrossRef]
- Young, A.; Jonski, G.; Rölla, G.; Wåler, S.M. Effects of metal salts on the oral production of volatile sulfur-containing compounds (VSC). J. Clin. Periodontol. 2001, 28, 776–781. [Google Scholar] [CrossRef] [PubMed]
- Navada, R.; Kumari, H.; Le, S.; Zhang, J. Oral malodor reduction from a zinc-containing toothpaste. J. Clin. Dent. 2008, 19, 69–73. [Google Scholar]
- Newby, E.E.; Hickling, J.M.; Hughes, F.J.; Proskin, H.M.; Bosma, M.P. Control of oral malodour by dentifrices measured by gas chromatography. Arch. Oral Biol. 2008, 53 (Suppl. 1), S19–S25. [Google Scholar] [CrossRef]
- Young, A.; Jonski, G. Effect of a single brushing with two Zn-containing toothpastes on VSC in morning breath: A 12 h, randomized, double-blind, cross-over clinical study. J. Breath Res. 2011, 5, 046012. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D.; CONSORT Group. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, M.; McCulloch, C.A.G. Measurement of Oral Malodor: Current Methods and Future Prospects. J. Periodontol. 1992, 63, 776–782. [Google Scholar] [CrossRef]
- Tangerman, A.; Winkel, E.G. Intra- and extra-oral halitosis: Finding of a new form of extra-oral blood-borne halitosis caused by dimethyl sulphide. J. Clin. Periodontol. 2007, 34, 748–755. [Google Scholar] [CrossRef]
- Aung, E.E.; Ueno, M.; Zaitsu, T.; Furukawa, S.; Kawaguchi, Y. Effectiveness of three oral hygiene regimens on oral malodor reduction: A randomized clinical trial. Trials 2015, 16, 31. [Google Scholar] [CrossRef] [PubMed]
- Khurana, C.; Tandon, S.; Chinmaya, B.R. A crossover clinical trial to assess the effectiveness of different oral hygiene regimens on the reduction of morning bad breath in healthy young adults. Indian J. Dent. Res. Off. Publ. Indian Soc. Dent. Res. 2018, 29, 434–439. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.S.; Suprono, M.S.; Stephens, J.; Withers, S.A.; Li, Y. Efficacy of stabilized chlorine dioxide-based unflavored mouthwash in reducing oral malodor: An 8-week randomized controlled study. Am. J. Dent. 2018, 31, 309–312. [Google Scholar]
- Van der Sluijs, E.; Van der Weijden, G.A.; Hennequin-Hoenderdos, N.L.; Slot, D.E. The effect of a tooth/tongue gel and mouthwash regimen on morning oral malodour: A 3-week single-blind randomized clinical trial. Int. J. Dent. Hyg. 2018, 16, 92–102. [Google Scholar] [CrossRef] [PubMed]
- Feres, M.; Figueiredo, L.C.; Faveri, M.; Guerra, M.C.; Mateo, L.R.; Stewart, B.; Williams, M.; Panagakos, F. The efficacy of two oral hygiene regimens in reducing oral malodour: A randomised clinical trial. Int. Dent. J. 2015, 65, 292–302. [Google Scholar] [CrossRef] [PubMed]
- Mendes, L.; Coimbra, J.; Pereira, A.L.; Resende, M.; Pinto, M.G. Comparative effect of a new mouthrinse containing chlorhexidine, triclosan and zinc on volatile sulphur compounds: A randomized, crossover, double-blind study. Int. J. Dent. Hyg. 2016, 14, 202–208. [Google Scholar] [CrossRef]
- Yadav, S.R.; Kini, V.V.; Padhye, A. Inhibition of Tongue Coat and Dental Plaque Formation by Stabilized Chlorine Dioxide Vs Chlorhexidine Mouthrinse: A Randomized, Triple Blinded Study. J. Clin. Diagn. Res. 2015, 9, ZC69. [Google Scholar] [CrossRef]
- Winkel, E.G.; Roldán, S.; Van Winkelhoff, A.J.; Herrera, D.; Sanz, M. Clinical effects of a new mouthrinse containing chlorhexidine, cetylpyridinium chloride and zinc-lactate on oral halitosis. A dual-center, double-blind placebo-controlled study. J. Clin. Periodontol. 2003, 30, 300–306. [Google Scholar] [CrossRef]
- Erovic Ademovski, S.; Mårtensson, C.; Persson, G.R.; Renvert, S. The long-term effect of a zinc acetate and chlorhexidine diacetate containing mouth rinse on intra-oral halitosis-A randomized clinical trial. J. Clin. Periodontol. 2017, 44, 1010–1019. [Google Scholar] [CrossRef]
- Young, A.; Jonski, G.; Rölla, G. Inhibition of orally produced volatile sulfur compounds by zinc, chlorhexidine or cetylpyridinium chloride--effect of concentration. Eur. J. Oral Sci. 2003, 111, 400–404. [Google Scholar] [CrossRef] [PubMed]
- Young, A.; Jonski, G.; Rölla, G. Combined effect of zinc ions and cationic antibacterial agents on intraoral volatile sulphur compounds (VSC). Int. Dent. J. 2003, 53, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Thrane, P.S.; Young, A.; Jonski, G.; Rölla, G. A new mouthrinse combining zinc and chlorhexidine in low concentrations provides superior efficacy against halitosis compared to existing formulations: A double-blind clinical study. J. Clin. Dent. 2007, 18, 82–86. [Google Scholar] [PubMed]
- Saad, S.; Greenman, J.; Shaw, H. Comparative effects of various commercially available mouthrinse formulations on oral malodor. Oral Dis. 2011, 17, 180–186. [Google Scholar] [CrossRef]
- Ademovski, S.E.; Persson, G.R.; Winkel, E.; Tangerman, A.; Lingström, P.; Renvert, S. The short-term treatment effects on the microbiota at the dorsum of the tongue in intra-oral halitosis patients—A randomized clinical trial. Clin. Oral Investig. 2013, 17, 463–473. [Google Scholar] [CrossRef] [PubMed]
- Jervøe-Storm, P.-M.; Schulze, H.; Jepsen, S. A randomized cross-over short-term study on the short-term effects of a zinc-lactate containing mouthwash against oral malodour. J. Breath Res. 2019, 13, 26005. [Google Scholar] [CrossRef]
- Chung, S.-H. The effects of an essential oil mouthrinse on oral health in the community indwelling elderly. Taehan Kanho Hakhoe Chi 2006, 36, 84–93. [Google Scholar] [CrossRef]
- Satthanakul, P.; Taweechaisupapong, S.; Paphangkorakit, J.; Pesee, M.; Timabut, P.; Khunkitti, W. Antimicrobial effect of lemongrass oil against oral malodour micro-organisms and the pilot study of safety and efficacy of lemongrass mouthrinse on oral malodour. J. Appl. Microbiol. 2015, 118, 11–17. [Google Scholar] [CrossRef]
- Frascella, J.; Gilbert, R.D.; Fernandez, P.; Hendler, J. Efficacy of a chlorine dioxide-containing mouthrinse in oral malodor. Compend. Contin. Educ. Dent. 2000, 21, 241–244, 246, 248 passim; quiz 256. [Google Scholar]
- Kim, J.-S.; Park, J.-W.; Kim, D.-J.; Kim, Y.-K.; Lee, J.-Y. Direct effect of chlorine dioxide, zinc chloride and chlorhexidine solution on the gaseous volatile sulfur compounds. Acta Odontol. Scand. 2014, 72, 645–650. [Google Scholar] [CrossRef]
- Alsaffar, D.; Alzoman, H. Efficacy of antioxidant mouthwash in the reduction of halitosis: A randomized, double blind, controlled crossover clinical trial. J. Dent. Sci. 2021, 16, 621–627. [Google Scholar] [CrossRef]
- Erovic Ademovski, S.; Lingström, P.; Renvert, S. The effect of different mouth rinse products on intra-oral halitosis. Int. J. Dent. Hyg. 2016, 14, 117–123. [Google Scholar] [CrossRef]
- Wilhelm, D.; Himmelmann, A.; Krause, C.; Wilhelm, K.-P. Short term clinical efficacy of new meridol HALITOSIS tooth & tongue gel in combination with a tongue cleaner to reduce oral malodor. J. Clin. Dent. 2013, 24, 12–19. [Google Scholar] [PubMed]
- Wilhelm, D.; Gysen, K.; Himmelmann, A.; Krause, C.; Wilhelm, K.-P. Short-term effect of a new mouthrinse formulation on oral malodour after single use in vivo: A comparative, randomized, single-blind, parallel-group clinical study. J. Breath Res. 2010, 4, 36002. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, H.; MacHigashira, M.; Yamashita, D.; Kozono, S.; Nakajima, Y.; Miyamoto, M.; Takeuchi, N.; Setoguchi, T.; Noguchi, K. The association of periodontal disease with oral malodour in a Japanese population. Oral Dis. 2010, 16, 702–706. [Google Scholar] [CrossRef] [PubMed]
- Murata, T.; Fujiyama, Y.; Yamaga, T.; Miyazaki, H. Breath malodor in an asthmatic patient caused by side-effects of medication: A case report and review of the literature. Oral Dis. 2003, 9, 273–276. [Google Scholar] [CrossRef]
- Suarez, F.; Springfield, J.; Furne, J.; Levitt, M. Differentiation of mouth versus gut as site of origin of odoriferous breath gases after garlic ingestion. Am. J. Physiol. 1999, 276, G425–G430. [Google Scholar] [CrossRef]
- Kawamoto, A.; Sugano, N.; Motohashi, M.; Matsumoto, S.; Ito, K. Relationship between oral malodor and the menstrual cycle. J. Periodontal Res. 2010, 45, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Greenman, J.; El-Maaytah, M.; Duffield, J.; Spencer, P.; Rosenberg, M.; Corry, D.; Saad, S.; Lenton, P.; Majerus, G.; Nachnani, S. Assessing the relationship between concentrations of malodor compounds and odor scores from judges. J. Am. Dent. Assoc. 2005, 136, 749–757. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, S.; Kozlovsky, A.; Gordon, D.; Gelernter, I.; Sintov, A.; Rosenberg, M. Cadaverine as a putative component of oral malodor. J. Dent. Res. 1994, 73, 1168–1172. [Google Scholar] [CrossRef] [PubMed]
- Loesche, W.J.; Kazor, C. Microbiology and treatment of halitosis. Periodontol. 2000 2002, 28, 256–279. [Google Scholar] [CrossRef]
- Kazor, C.E.; Mitchell, P.M.; Lee, A.M.; Stokes, L.N.; Loesche, W.J.; Dewhirst, F.E.; Paster, B.J. Diversity of bacterial populations on the tongue dorsa of patients with halitosis and healthy patients. J. Clin. Microbiol. 2003, 41, 558–563. [Google Scholar] [CrossRef]
- Oliveira-Neto, J.M.; Sato, S.; Pedrazzi, V. How to deal with morning bad breath: A randomized, crossover clinical trial. J. Indian Soc. Periodontol. 2013, 17, 757–761. [Google Scholar] [CrossRef] [PubMed]
- Washio, J.; Sato, T.; Koseki, T.; Takahashi, N. Hydrogen sulfide-producing bacteria in tongue biofilm and their relationship with oral malodour. J. Med. Microbiol. 2005, 54, 889–895. [Google Scholar] [CrossRef] [PubMed]
- Ye, W.; Zhang, Y.; He, M.; Zhu, C.; Feng, X.-P. Relationship of tongue coating microbiome on volatile sulfur compounds in healthy and halitosis adults. J. Breath Res. 2019, 14, 16005. [Google Scholar] [CrossRef] [PubMed]
- Seerangaiyan, K.; Jüch, F.; Winkel, E.G. Tongue coating: Its characteristics and role in intra-oral halitosis and general health—A review. J. Breath Res. 2018, 12, 34001. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.G. Chlorhexidine: Is it still the gold standard? Periodontol. 2000 1997, 15, 55–62. [Google Scholar] [CrossRef]
- García-Caballero, L.; Quintas, V.; Prada-López, I.; Seoane, J.; Donos, N.; Tomás, I. Chlorhexidine substantivity on salivary flora and plaque-like biofilm: An in situ model. PLoS ONE 2013, 8, e83522. [Google Scholar] [CrossRef]
- Adedapo, A.H.; Kolude, B.; Dada-Adegbola, H.O.; Lawoyin, J.O.; Adeola, H.A. Targeted polymerase chain reaction-based expression of putative halitogenic bacteria and volatile sulphur compound analysis among halitosis patients at a tertiary hospital in Nigeria. Odontology 2020, 108, 450–461. [Google Scholar] [CrossRef]
- Yasukawa, T.; Ohmori, M.; Sato, S. The relationship between physiologic halitosis and periodontopathic bacteria of the tongue and gingival sulcus. Odontology 2010, 98, 44–51. [Google Scholar] [CrossRef]
- Kamaraj, D.; Bhushan, K.S. An evaluation of microbial profile in halitosis with tongue coating using PCR (polymerase chain reaction)—A clinical and microbiological study. J. Clin. Diagn. Res. 2014, 8, 263. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Organoleptic | Hydrogen Sulfide | Methyl Mercaptan | VSC | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Stage | Group | Mean | SD | Mean | SD | Mean | SD | Mean | SD |
| T0 | Lacer HaliTM | 2.00 | 0.79 | 253.75 | 335.55 | 108.60 | 117.30 | 383.30 | 433.92 |
| Placebo | 2.35 | 0.93 | 102.15 | 91.07 | 93.20 | 165.15 | 223.50 | 179.95 | |
| HalitaTM | 2.05 | 0.89 | 145.20 | 131.27 | 138.30 | 168.98 | 322.65 | 265.32 | |
| T1 | Lacer HaliTM | 1.20 | 0.62 | 40.50 | 48.16 | 22.10 | 38.11 | 74.30 | 95.17 |
| Placebo | 1.45 | 0.89 | 82.00 | 157.82 | 35.70 | 48.13 | 139.25 | 176.29 | |
| HalitaTM | 1.15 | 0.93 | 37.75 | 61.34 | 34.30 | 49.53 | 94.70 | 128.32 | |
| T2 | Lacer HaliTM | 1.50 | 0.76 | 91.20 | 108.11 | 63.45 | 91.17 | 201.75 | 209.89 |
| Placebo | 2.25 | 1.02 | 178.65 | 275.70 | 60.90 | 61.61 | 263.45 | 330.27 | |
| HalitaTM | 1.45 | 1.10 | 49.10 | 81.56 | 46.90 | 90.27 | 104.80 | 169.93 | |
| T3 | Lacer HaliTM | 1.45 | 0.69 | 140.70 | 221.21 | 57.10 | 69.61 | 218.20 | 271.59 |
| Placebo | 2.00 | 0.79 | 113.80 | 124.66 | 68.65 | 181.20 | 198.60 | 206.33 | |
| HalitaTM | 1.25 | 0.91 | 47.25 | 113.92 | 39.25 | 74.98 | 102.40 | 184.99 | |
| T4 | Lacer HaliTM | 1.70 | 0.98 | 157.15 | 274.29 | 95.00 | 156.67 | 264.35 | 395.54 |
| Placebo | 2.10 | 0.91 | 137.10 | 203.13 | 46.50 | 57.17 | 192.20 | 252.78 | |
| HalitaTM | 1.55 | 1.05 | 118.15 | 201.71 | 80.10 | 121.86 | 213.60 | 305.49 | |
| Organoleptic | Hydrogen Sulfide | Methyl Mercaptan | VSC | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Stage | Group | % of Variation Relative to Baseline | % of Variation Relative to Placebo | % of Variation Relative to HalitaTM | % of Variation Relative to Baseline | % of Variation Relative to Placebo | % of Variation Relative to HalitaTM | % of Variation Relative to Baseline | % of Variation Relative to Placebo | % of Variation Relative to HalitaTM | % of Variation Relative to Baseline | % of Variation Relative to Placebo | % of Variation Relative to HalitaTM |
| T0 | Lacer HaliTM | -- | −15% | −2% | -- | 148% | 75% | -- | 17% | −21% | -- | 71% | 19% |
| Placebo | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | |
| HalitaTM | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | |
| T1 | Lacer HaliTM | −40% | −17% | 4% | −84% | −51% | 7% | −80% | −38% | −36% | −81% | −47% | −22% |
| Placebo | −38% | -- | -- | −20% | -- | -- | −62% | -- | -- | −38% | -- | -- | |
| HalitaTM | −44% | -- | -- | −84% | -- | -- | −75% | -- | -- | −71% | -- | -- | |
| T2 | Lacer HaliTM | −25% | −33% | 3% | −64% | −49% | 86% | −42% | 4% | 35% | −47% | −23% | 93% |
| Placebo | −4% | -- | -- | 75% | -- | -- | −35% | -- | -- | 18% | -- | -- | |
| HalitaTM | −29% | -- | -- | −64% | -- | -- | −66% | -- | -- | −68% | -- | -- | |
| T3 | Lacer HaliTM | −28% | −28% | 16% | −45% | 24% | 198% | −47% | −17% | 45% | −43% | 10% | 113% |
| Placebo | −15% | -- | -- | 11% | -- | -- | −26% | -- | -- | −11% | -- | -- | |
| HalitaTM | −39% | -- | -- | −45% | -- | -- | −72% | -- | -- | −68% | -- | -- | |
| T4 | Lacer HaliTM | −15% | −19% | 10% | −38% | 15% | 33% | −13% | 104% | 19% | −31% | 38% | 24% |
| Placebo | −11% | -- | -- | 34% | -- | -- | −50% | -- | -- | −14% | -- | -- | |
| HalitaTM | −24% | -- | -- | −38% | -- | -- | −42% | -- | -- | −34% | -- | -- | |
| Stage | Group | Predicted Probability | z | p-Value |
|---|---|---|---|---|
| T0 | Lacer HaliTM vs. Placebo | −61% | −0.98 | 0.326 |
| Lacer HaliTM vs. HalitaTM | −25% | −0.43 | 0.667 | |
| T1 | Lacer HaliTM vs. Placebo | −58% | −0.92 | 0.360 |
| Lacer HaliTM vs. HalitaTM | 29% | 0.39 | 0.694 | |
| T2 | Lacer HaliTM vs. Placebo | −92% | −2.60 | 0.009 |
| Lacer HaliTM vs. HalitaTM | 19% | 0.23 | 0.816 | |
| T3 | Lacer HaliTM vs. Placebo | −83% | −1.89 | 0.059 |
| Lacer HaliTM vs. HalitaTM | 56% | 0.94 | 0.345 | |
| T4 | Lacer HaliTM vs. Placebo | −72% | −1.35 | 0.177 |
| Lacer HaliTM vs. HalitaTM | 42% | 0.58 | 0.563 |
| Stage | Group | Predicted Probability | z | p-Value |
|---|---|---|---|---|
| T0 | Hydrogen sulfide | |||
| Lacer HaliTM vs. Placebo | 46% | 1.72 | 0.0860 | |
| Lacer HaliTM vs. HalitaTM | 30% | 1.03 | 0.3010 | |
| Methyl mercaptan | ||||
| Lacer HaliTM vs. Placebo | 10% | 0.32 | 0.7470 | |
| Lacer HaliTM vs. HalitaTM | −15% | −0.48 | 0.6320 | |
| VSC | ||||
| Lacer HaliTM vs. Placebo | 25% | 1.05 | 0.2945 | |
| Lacer HaliTM vs. HalitaTM | 3% | 0.12 | 0.9050 | |
| T1 | Hydrogen sulfide | |||
| Lacer HaliTM vs. Placebo | −31% | −0.90 | 0.3673 | |
| Lacer HaliTM vs. HalitaTM | 16% | 0.40 | 0.6880 | |
| Methyl mercaptan | ||||
| Lacer HaliTM vs. Placebo | −49% | −1.55 | 0.1203 | |
| Lacer HaliTM vs. HalitaTM | −42% | −1.26 | 0.2070 | |
| VSC | ||||
| Lacer HaliTM vs. Placebo | −40% | −1.56 | 0.1190 | |
| Lacer HaliTM vs. HalitaTM | −5% | −0.15 | 0.8810 | |
| T2 | Hydrogen sulfide | |||
| Lacer HaliTM vs. Placebo | −57% | −2.23 | 0.0256 | |
| Lacer HaliTM vs. HalitaTM | 37% | 1.07 | 0.2852 | |
| Methyl mercaptan | ||||
| Lacer HaliTM vs. Placebo | −11% | −0.31 | 0.7560 | |
| Lacer HaliTM vs. HalitaTM | 26% | 0.76 | 0.4480 | |
| VSC | ||||
| Lacer HaliTM vs. Placebo | −28% | −1.09 | 0.2778 | |
| Lacer HaliTM vs. HalitaTM | 40% | 1.58 | 0.1142 | |
| T3 | Hydrogen sulfide | |||
| Lacer HaliTM vs. Placebo | 11% | 0.30 | 0.7630 | |
| Lacer HaliTM vs. HalitaTM | 64% | 2.49 | 0.0130 | |
| Methyl mercaptan | ||||
| Lacer HaliTM vs. Placebo | 22% | 0.62 | 0.5350 | |
| Lacer HaliTM vs. HalitaTM | 32% | 0.97 | 0.3340 | |
| VSC | ||||
| Lacer HaliTM vs. Placebo | −1% | −0.04 | 0.9673 | |
| Lacer HaliTM vs. HalitaTM | 53% | 2.35 | 0.0190 | |
| T4 | Hydrogen sulfide | |||
| Lacer HaliTM vs. Placebo | 4% | −0.11 | 0.9150 | |
| Lacer HaliTM vs. HalitaTM | 16% | 0.46 | 0.6440 | |
| Methyl mercaptan | ||||
| Lacer HaliTM vs. Placebo | 8% | 0.20 | 0.8380 | |
| Lacer HaliTM vs. HalitaTM | −21% | −0.62 | 0.5330 | |
| VSC | ||||
| Lacer HaliTM vs. Placebo | −1% | −0.03 | 0.9790 | |
| Lacer HaliTM vs. HalitaTM | 1% | −0.03 | 0.9756 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiang, L.; Rojo, R.; Prados-Frutos, J.C. Evaluation of the Efficacy of Lacer HaliTM Treatment on the Management of Halitosis: A Randomized Double-Blind Clinical Trial. J. Clin. Med. 2021, 10, 2256. https://doi.org/10.3390/jcm10112256
Xiang L, Rojo R, Prados-Frutos JC. Evaluation of the Efficacy of Lacer HaliTM Treatment on the Management of Halitosis: A Randomized Double-Blind Clinical Trial. Journal of Clinical Medicine. 2021; 10(11):2256. https://doi.org/10.3390/jcm10112256
Chicago/Turabian StyleXiang, Laiqi, Rosa Rojo, and Juan Carlos Prados-Frutos. 2021. "Evaluation of the Efficacy of Lacer HaliTM Treatment on the Management of Halitosis: A Randomized Double-Blind Clinical Trial" Journal of Clinical Medicine 10, no. 11: 2256. https://doi.org/10.3390/jcm10112256
APA StyleXiang, L., Rojo, R., & Prados-Frutos, J. C. (2021). Evaluation of the Efficacy of Lacer HaliTM Treatment on the Management of Halitosis: A Randomized Double-Blind Clinical Trial. Journal of Clinical Medicine, 10(11), 2256. https://doi.org/10.3390/jcm10112256