
COVID-19 Vaccination in Patients with Severe Asthma on Biologic Treatment: Safety, Tolerability, and Impact on Disease Control

 ,
, 


Abstract
:1. Introduction
2. Materials and Methods
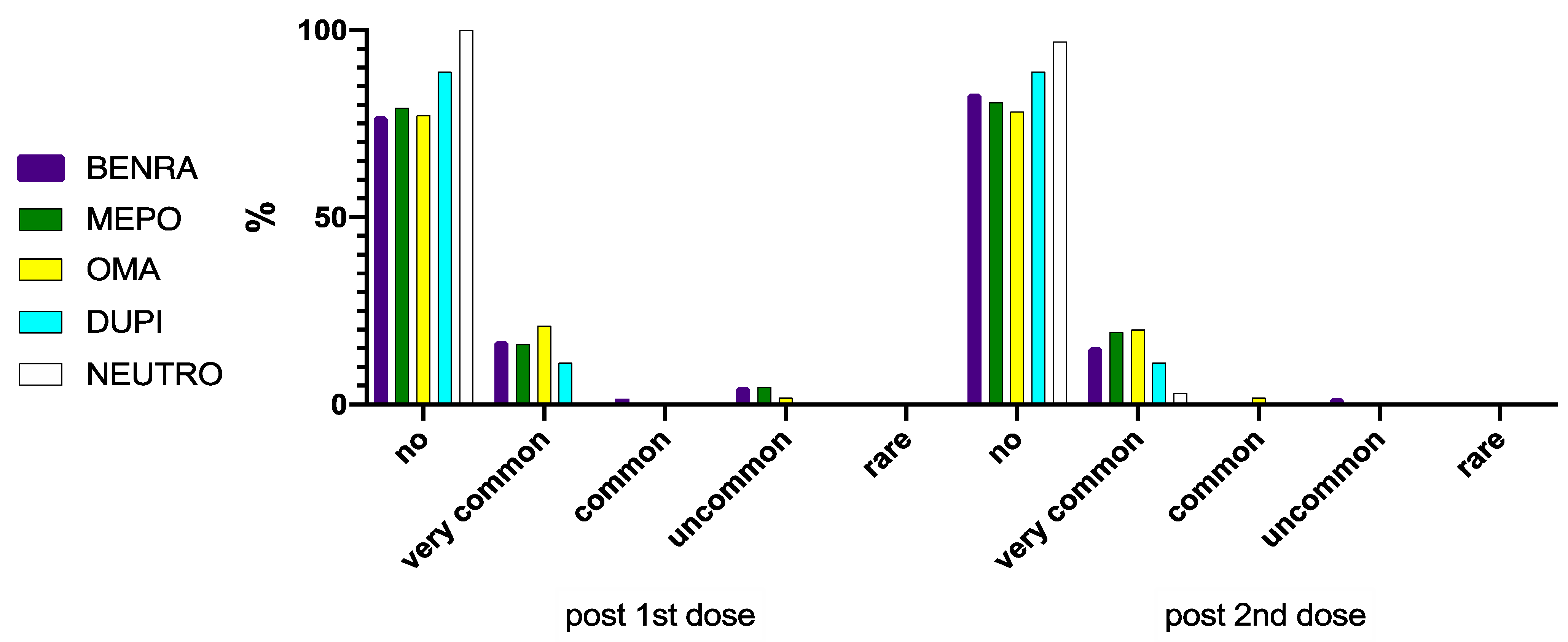
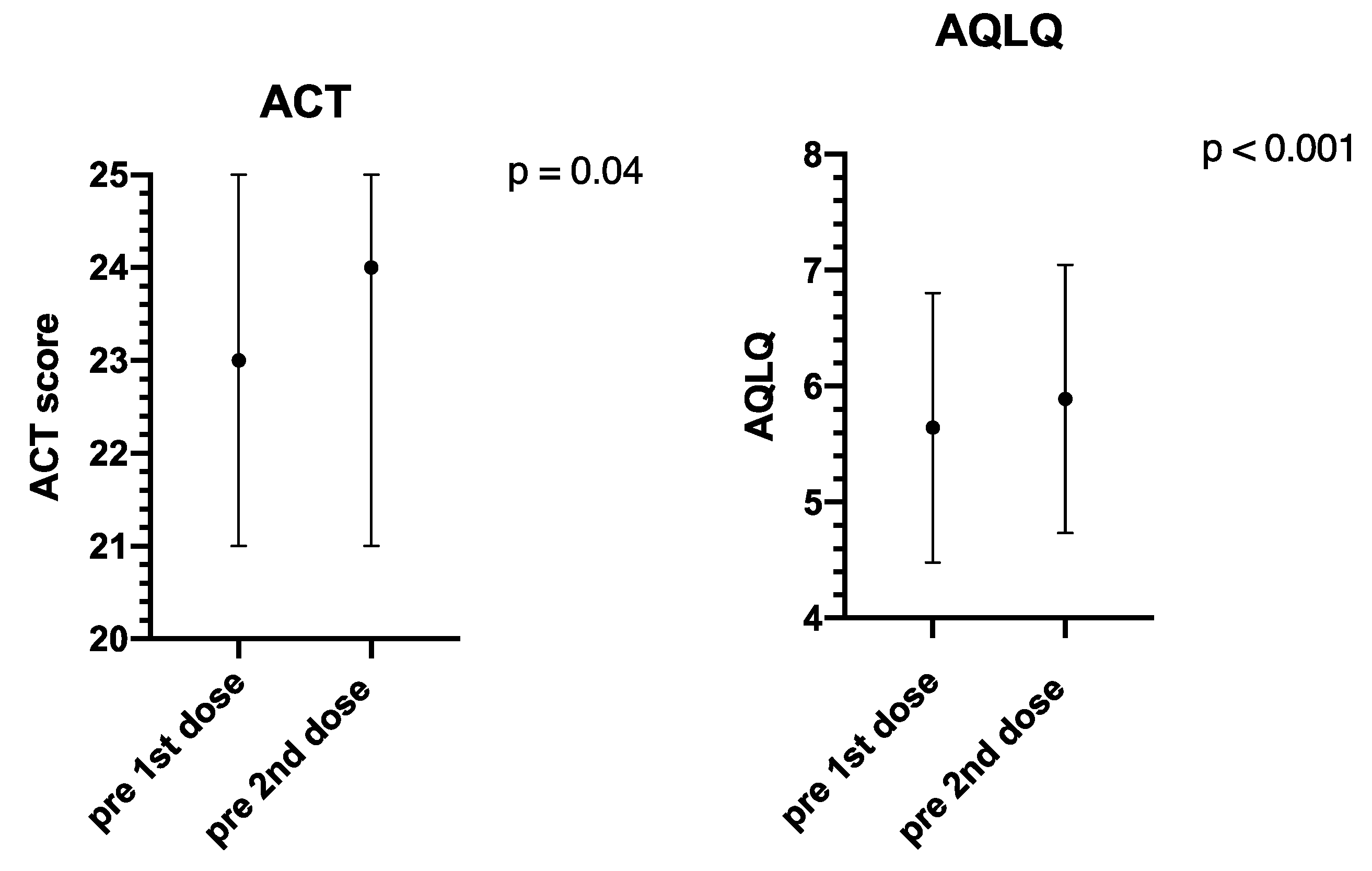
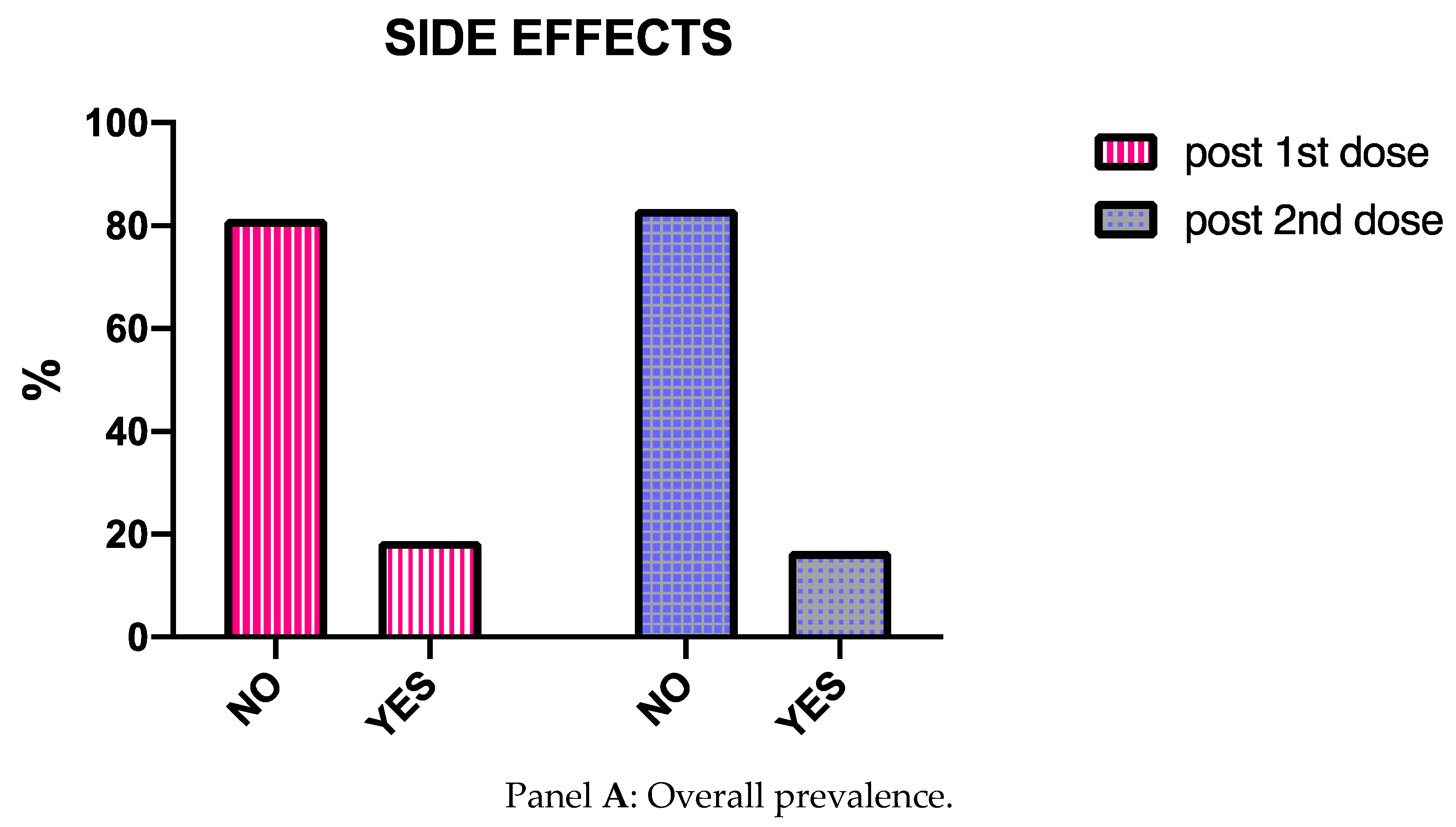
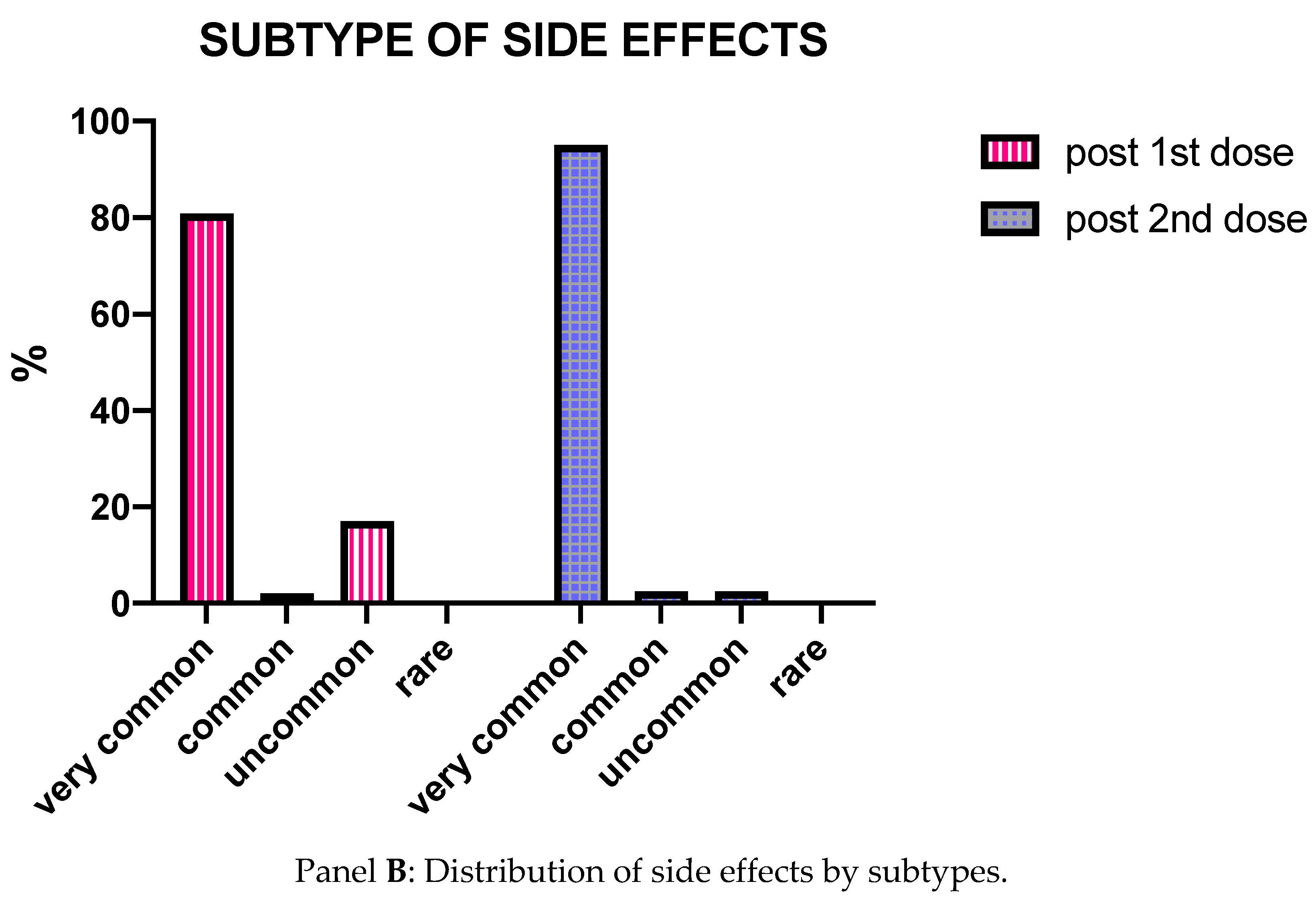
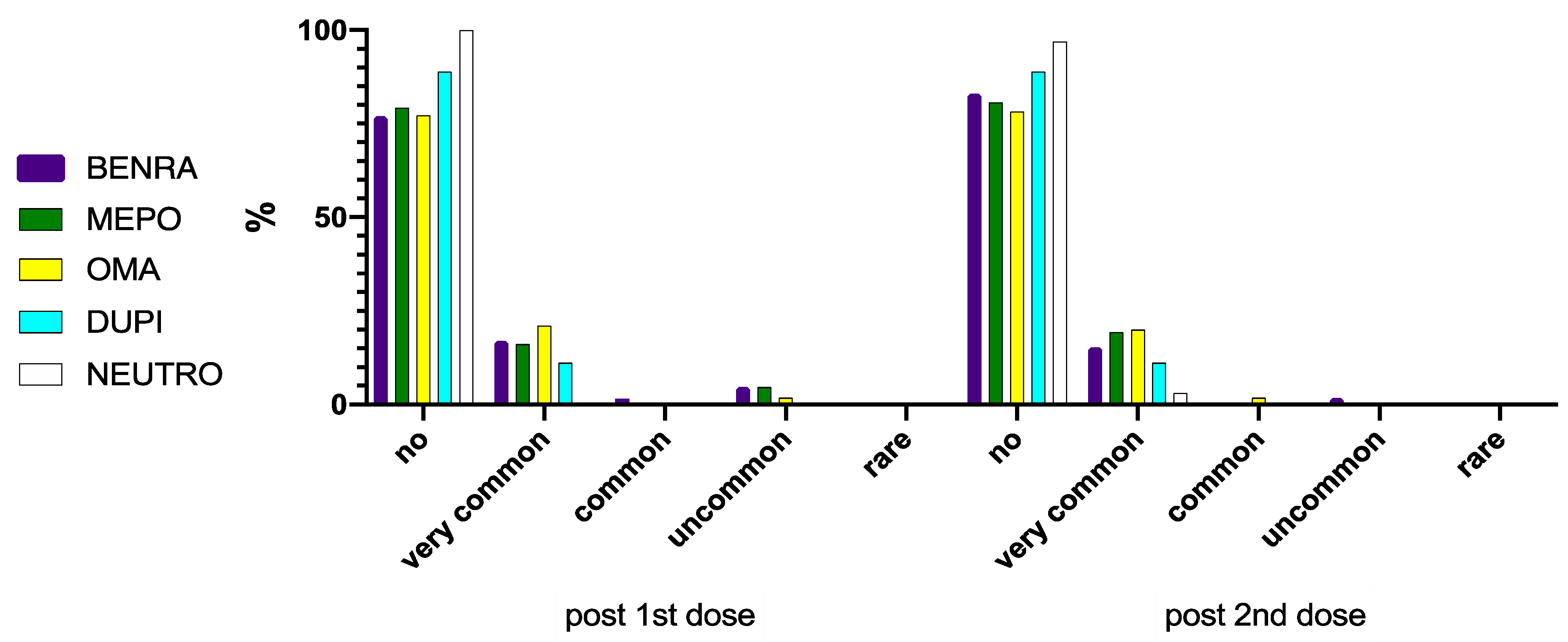
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Full Text Questionnaire Administered to the Patients
References
- Choi, Y.J.; Park, J.-Y.; Lee, H.S.; Suh, J.; Song, J.Y.; Byun, M.K.; Cho, J.H.; Kim, H.J.; Lee, J.-H.; Park, J.-W.; et al. Effect of asthma and asthma medication on the prognosis of patients with COVID-19. Eur. Respir. J. 2021, 57, 2002226. [Google Scholar] [CrossRef] [PubMed]
- Izquierdo, J.L.; Almonacid, C.; González, Y.; Del Rio-Bermudez, C.; Ancochea, J.; Cárdenas, R.; Lumbreras, S.; Soriano, J.B. The impact of COVID-19 on patients with asthma. Eur. Respir. J. 2021, 57, 2003142. [Google Scholar] [CrossRef] [PubMed]
- Caminati, M.; Vultaggio, A.; Matucci, A.; Senna, G.; Almerigogna, F.; Bagnasco, D.; Chieco-Bianchi, F.; Cosini, F.; Girelli, D.; Guarnieri, G.; et al. Asthma in a large COVID-19 cohort: Prevalence, features, and determinants of COVID-19 disease severity. Respir. Med. 2021, 176, 106261. [Google Scholar] [CrossRef] [PubMed]
- Morais-Almeida, M.; Aguiar, R.; Martin, B.; Ansotegui, I.J.; Ebisawa, M.; Arruda, L.K.; Caminati, M.; Canonica, G.W.; Carr, T.; Chupp, G.; et al. COVID-19, asthma, and biological therapies: What we need to know. World Allergy Organ. J. 2020, 13, 100126. [Google Scholar] [CrossRef] [PubMed]
- Matucci, A.; Caminati, M.; Vivarelli, E.; Vianello, A.; Micheletto, C.; Menzella, F.; Crisafulli, E.; Passalacqua, G.; Bagnasco, D.; Lombardi, C.; et al. COVID-19 in severe asthmatic patients during ongoing treatment with biologicals targeting type 2 inflammation: Results from a multicenter Italian survey. Allergy 2021, 76, 871–874. [Google Scholar] [CrossRef] [PubMed]
- Pfaar, O.; Klimek, L.; Hamelmann, E.; Kleine-Tebbe, J.; Taube, C.; Wagenmann, M.; Werfel, T.; Brehler, R.; Novak, N.; Mülleneisen, N.; et al. COVID-19 vaccination of patients with allergies and type-2 inflammation with concurrent antibody therapy (biologicals)—A Position Paper of the German Society of Allergology and Clinical Immunology (DGAKI) and the German Society for Applied Allergology (AeDA). Allergol. Select 2021, 5, 140–147. [Google Scholar] [PubMed]
- Kelso, J.M. Anaphylactic reactions to novel mRNA SARS CoV2/COVID 19 vaccines. Vaccine 2021, 39, 865–870. [Google Scholar] [CrossRef] [PubMed]
- Caminati, M.; Guarnieri, G.; Senna, G. Who Is Really at Risk for Anaphylaxis Due to COVID-19 Vaccine? Vaccines 2021, 9, 38. [Google Scholar] [CrossRef] [PubMed]
- Klimek, L.; Bergmann, K.C.; Brehler, R.; Pfützner, W.; Zuberbier, T.; Hartmann, K.; Jakob, T.; Novak, N.; Ring, J.; Merk, H.; et al. Practical handling of allergic reactions to COVID-19 vaccines: A position paper from German and Austrian Allergy Societies AeDA, DGAKI, GPA and OGAI. Allergol. J. Int. 2021, 19, 1–17. [Google Scholar]
- Turner, P.J.; Ansotegui, I.J.; Campbell, D.E.; Cardona, V.; Ebisawa, M.; El-Gamal, Y.; Fineman, S.; Geller, M.; Gonzalez-Estrada, A.; Greenberger, P.A.; et al. WAO Anaphylaxis Committee. COVID-19 vaccine-associated anaphylaxis: A statement of the World Allergy Organization Ana-phylaxis Committee. World Allergy Organ. J. 2021, 14, 100517. [Google Scholar] [CrossRef] [PubMed]
- Bijlsma, J.W.J. EULAR December 2020 viewpoints on SARS-CoV-2 vaccination in patients with RMDs. Ann. Rheum. Dis. 2021, 80, 411–412. [Google Scholar] [CrossRef] [PubMed]
- Italian Society of Allergy and Clinical Immunology. Position Statement on COVID-19 Vaccine. Available online: http://www.siaaic.org/wp-content/uploads/2021/05/Linee-di-Indirizzo-per-la-vaccinazione-anti-COVID-19.pdf (accessed on 30 July 2021).
- Available online: www.ema.europa.eu%2Fen%2Fdocuments%2Fall-authorised%20presentations%2Fcomirnaty-epar-all-authorised%20presenta-tions_it.pdf&usg=AOvVaw0NpIjtXI4KnqJ_gVkSwu8w (accessed on 30 June 2021).
- Blauvelt, A.; Simpson, E.L.; Tyring, S.K.; Purcell, L.A.; Petro, C.D.B.; Shumel, B.; Gadkari, A.; Eckert, L.; Graham, N.M.H.; Pirozzi, G.; et al. Dupilumab does not affect correlates of vaccine-induced immunity: A randomized, placebo-controlled trial in adults with moderate-to-severe atopic dermatitis. J. Am. Acad. Dermatol. 2019, 80, 158–167.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeitlin, O.M.; Leong, M.; Cole, J.; Mallory, R.M.; Shih, V.H.; Olsson, R.F.; Goldman, M. ALIZE Study Investigators. Benralizumab does not impair antibody response to seasonal influenza vaccination in adolescent and young adult patients with moderate to severe asthma: Results from the Phase IIIb ALIZE trial. J. Asthma Allergy 2018, 11, 181–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhalla, A.; Mukherjee, M.; Radford, K.; Nazy, I.; Kjarsgaard, M.; Bowdish, D.M.E. Parameswaran Nair. Dupilumab, severe asthma airway responses, and SARS-CoV-2 sierology. Allergy 2021, 76, 957–958. [Google Scholar] [CrossRef] [PubMed]
- Woo, E.J.; Moro, P.L. Postmarketing safety surveillance of quadrivalent recombinant influenza vaccine: Reports to the vaccine adverse event reporting system. Vaccine 2021, 39, 1812–1817. [Google Scholar] [CrossRef]
- Chung, K.F.; Wenzel, S.E.; Brozek, J.L.; Bush, A.; Castro, M.; Sterk, P.J.; Adcock, I.M.; Bateman, E.D.; Bel, E.H.; Bleecker, E.R.; et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur. Respir. J. 2014, 43, 343–373. [Google Scholar] [CrossRef] [Green Version]
- Rzymski, P.; Zeyland, J.; Poniedziałek, B.; Małecka, I.; Wysocki, J. The Perception and Attitudes toward COVID-19 Vaccines: A Cross-Sectional Study in Poland. Vaccines 2021, 9, 382. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total, n | 253 |
| Female, n (%) | 141 |
| Male, n (%) | 112 |
| Age, median (IQR) | 57 (49–65) |
| Benralizumab treatment, n (%) | 65 (26) |
| Mepolizumab treatment, n (%) | 88 (33) |
| Omalizumab treatment, n (%) | 58 (25) |
| Dupilumab treatment, n (%) | 9 (3) |
| Neutrophilic severe asthma, n (%) | 33 (13) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caminati, M.; Guarnieri, G.; Batani, V.; Scarpieri, E.; Finocchiaro, A.; Chieco-Bianchi, F.; Senna, G.; Vianello, A. COVID-19 Vaccination in Patients with Severe Asthma on Biologic Treatment: Safety, Tolerability, and Impact on Disease Control. Vaccines 2021, 9, 853. https://doi.org/10.3390/vaccines9080853
Caminati M, Guarnieri G, Batani V, Scarpieri E, Finocchiaro A, Chieco-Bianchi F, Senna G, Vianello A. COVID-19 Vaccination in Patients with Severe Asthma on Biologic Treatment: Safety, Tolerability, and Impact on Disease Control. Vaccines. 2021; 9(8):853. https://doi.org/10.3390/vaccines9080853
Chicago/Turabian StyleCaminati, Marco, Gabriella Guarnieri, Veronica Batani, Elena Scarpieri, Anita Finocchiaro, Fulvia Chieco-Bianchi, Gianenrico Senna, and Andrea Vianello. 2021. "COVID-19 Vaccination in Patients with Severe Asthma on Biologic Treatment: Safety, Tolerability, and Impact on Disease Control" Vaccines 9, no. 8: 853. https://doi.org/10.3390/vaccines9080853
APA StyleCaminati, M., Guarnieri, G., Batani, V., Scarpieri, E., Finocchiaro, A., Chieco-Bianchi, F., Senna, G., & Vianello, A. (2021). COVID-19 Vaccination in Patients with Severe Asthma on Biologic Treatment: Safety, Tolerability, and Impact on Disease Control. Vaccines, 9(8), 853. https://doi.org/10.3390/vaccines9080853