
Neutralizing Anti-SARS-CoV-2 Antibody Titer and Reported Adverse Effects, in a Sample of Italian Nursing Home Personnel after Two Doses of the BNT162b2 Vaccine Administered Four Weeks Apart

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Context and Population
- -
- being an employee of the nursing home at work during the period January–February 2021
- -
- being vaccinated with the BNT162b2 anti-SARS-CoV-2 vaccine
- -
- having completed the two-dose cycle with an interval of four weeks between the first and the second dose.
2.2. Quantification of Neutralizing Antibodies in the Serum
2.3. Collection of Information from the Study Participants
- (a).
- socio-demographic (age, sex) and anthropometric (height, weight) information, as well as on smoking and alcohol consumption habits
- (b).
- occupational anamnesis including an investigation of job tasks and of the eventual performance of nightshifts at work
- (c).
- a pathological anamnesis, investigating in particular a previous SARS-CoV-2 infection and medical conditions, because immunosuppression is able to influence the immune response to the vaccine
- (d).
- the occurrence and duration of adverse effects after the first and the second anti-SARS-Cov-2 vaccine doses, based on a list of effects reported in the Vaccine Surveillance Report of the AIFA [10] and on a recent study [11], including both local (pain and/or redness in the injection site) and general symptoms (fever, asthenia/fatigue, muscle aches, anaphylaxis and other).
2.4. Statistical Analysis
3. Results
3.1. General Characteristics of the Study Population and Anti-SARS-CoV-2 Antibody Titer in the Vaccinated Subjects
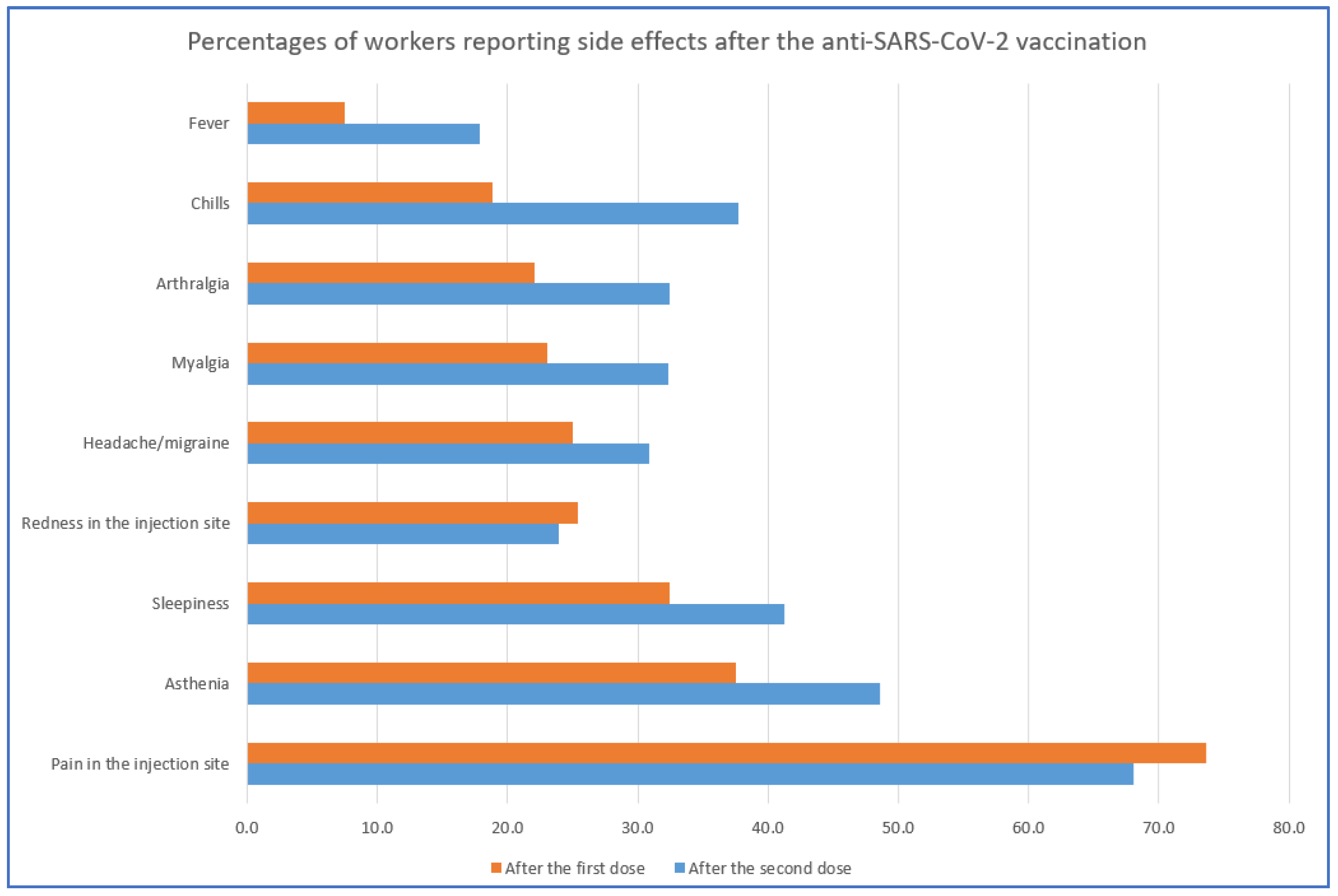
3.2. Analysis of the Adverse Effects Reported after the Anti-SARS-CoV-2 Vaccine
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ministero Della Salute. Vaccine Day il 27 Dicembre in Tutta Italia e in Europa. Available online: http://www.salute.gov.it/portale/news/p3_2_1_1_1.jsp?lingua=italiano&menu=notizie&p=dalministero&id=5242 (accessed on 19 May 2021).
- Agenzia Italiana del Farmaco (AIFA). Vaccini COVID-19. Available online: https://www.aifa.gov.it/vaccini-covid-19 (accessed on 19 May 2021).
- Widge, A.T.; Rouphael, N.G.; Jackson, L.A.; Anderson, E.J.; Roberts, P.C.; Makhene, M.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; Pruijssers, A.J.; et al. Durability of Responses after SARS-CoV-2 mRNA-1273 Vaccination. N. Engl. J. Med. 2021, 384, 80–82. [Google Scholar] [CrossRef] [PubMed]
- Goel, R.R.; Apostolidis, S.A.; Painter, M.M.; Mathew, D.; Pattekar, A.; Kuthuru, O.; Gouma, S.; Kuri-Cervantes, L.; Meng, W.; Adamski, S.; et al. Longitudinal Analysis Reveals Distinct Antibody and Memory B Cell Responses in SARS-CoV2 Naïve and Recovered Individuals Following mRNA Vaccination. medRxiv 2021. [Google Scholar] [CrossRef]
- Colucci, M.; Piano Mortari, E.; Zotta, F.; Corrente, F.; Concato, C.; Carsetti, R.; Emma, F.; Vivarelli, M. Evaluation of Immune and Vaccine Competence in Steroid-Sensitive Nephrotic Syndrome Pediatric Patients. Front. Immunol. 2021, 12, 602826. [Google Scholar] [CrossRef] [PubMed]
- Chia, W.N.; Zhu, F.; Ong, S.W.X.; Young, B.E.; Fong, S.W.; Le Bert, N.; Tan, C.W.; Tiu, C.; Zhang, J.; Tan, S.Y.; et al. Dynamics of SARS-CoV-2 neutralising antibody responses and duration of immunity: A longitudinal study. Lancet Microbe 2021. [Google Scholar] [CrossRef]
- Watanabe, M.; Balena, A.; Tuccinardi, D.; Tozzi, R.; Risi, R.; Masi, D.; Caputi, A.; Rossetti, R.; Spoltore, M.E.; Filippi, V.; et al. Central obesity, smoking habit and hypertension are associated with lower antibody titers in response to COVID-19 mRNA vaccine. Diabetes Metab. Res. Rev. 2021. [Google Scholar] [CrossRef] [PubMed]
- Euroimun. Anti-SARS-CoV-2 QuantiVac ELISA (IgG). Available online: https://www.coronavirus-diagnostics.com/documents/Indications/Infections/Coronavirus/EI_2606_D_UK_E.pdf (accessed on 19 May 2021).
- First WHO International Standard Anti-SARS-CoV-2 Immunoglobulin (Human). Product Number 20/136. Available online: https://www.nibsc.org/products/brm_product_catalogue/detail_page.aspx?catid=20/136 (accessed on 19 May 2021).
- Agenzia Italiana del Farmaco. Terzo Rapporto AIFA Sulla Sorveglianza dei Vaccini COVID-19. Available online: https://www.aifa.gov.it/-/terzo-rapporto-aifa-sulla-sorveglianza-dei-vaccini-covid-19 (accessed on 19 May 2021).
- Hall, V.J.; Foulkes, S.; Saei, A.; Andrews, N.; Oguti, B.; Charlett, A.; Wellington, E.; Stowe, J.; Gillson, N.; Atti, A.; et al. COVID-19 vaccine coverage in health-care workers in England and effectiveness of BNT162b2 mRNA vaccine against infection (SIREN): A prospective, multicentre, cohort study. Lancet 2021, 397, 1725–1735. [Google Scholar] [CrossRef]
- Meo, S.A.; Bukhari, I.A.; Akram, J.; Meo, A.S.; Klonoff, D.C. COVID-19 vaccines: Comparison of biological, pharmacological characteristics and adverse effects of Pfizer/BioNTech and Moderna Vaccines. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 1663–1669. [Google Scholar] [CrossRef] [PubMed]
- Favresse, J.; Bayart, J.L.; Mullier, F.; Dogné, J.M.; Closset, M.; Douxfils, J. Early antibody response in healthcare professionals after two doses of SARS-CoV-2 mRNA vaccine (BNT162b2). Clin. Microbiol. Infect. 2021. [Google Scholar] [CrossRef] [PubMed]
- Manisty, C.; Otter, A.D.; Treibel, T.A.; McKnight, Á.; Altmann, D.M.; Brooks, T.; Noursadeghi, M.; Boyton, R.J.; Semper, A.; Moon, J.C. Antibody response to first BNT162b2 dose in previously SARS-CoV-2-infected individuals. Lancet 2021, 397, 1057–1058. [Google Scholar] [CrossRef]
- Padoan, A.; Dall’Olmo, L.; Rocca, F.D.; Barbaro, F.; Cosma, C.; Basso, D.; Cattelan, A.; Cianci, V.; Plebani, M. Antibody response to first and second dose of BNT162b2 in a cohort of characterized healthcare workers. Clin. Chim. Acta 2021, 519, 60–63. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food and Druhs Administration. Pfizer-BioNTech COVID-19 Vaccine. Available online: https://www.fda.gov/emergency-preparedness-and-response/coronavirus-disease-2019-covid-19/pfizer-biontech-covid-19-vaccine (accessed on 19 May 2021).
- Tré-Hardy, M.; Cupaiolo, R.; Papleux, E.; Wilmet, A.; Horeanga, A.; Antoine-Moussiaux, T.; Della Vecchia, A.; Beukinga, I.; Vekemans, M.; Blairon, L. Reactogenicity, safety and antibody response, after one and two doses of mRNA-1273 in seronegative and seropositive healthcare workers. J. Infect. 2021. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Chapin-Bardales, J.; Gee, J.; Myers, T. Reactogenicity Following Receipt of mRNA-Based COVID-19 Vaccines. JAMA 2021. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics of the Studied Subjects | % (N) * | Anti-SARS-CoV-2 IgG (BAU/mL) MD (Range) | p Value | |
|---|---|---|---|---|
| Sex | Males | 18.9 (14) | 3335 (764–17,300) | 0.198 |
| Females | 81.1 (60) | 5285 (830–27,600) | ||
| Age class | ≤30 | 12.2 (9) | 7050 (3272–13,749) | 0.165 |
| 31–40 | 16.2 (12) | 3086.5 (1824–11,390) | ||
| 41–50 | 18.9 (14) | 4820 (1243–20,300) | ||
| 51–60 | 31.1 (23) | 4821 (830–15,474) | ||
| >60 | 21.6 (16) | 6542.5 (764–27,600) | ||
| BMI | <25 | 53.4 (39) | 4821 (830–20,300) | 0.819 |
| 25–29.9 | 37.0 (27) | 6783 (764–17,300) | ||
| ≥30 | 9.6 (7) | 4557 (1794–14,834) | ||
| Smoking habit | Non–smokers | 77.0 (57) | 4557 (764–27,600) | 0.554 |
| Smokers | 23.0 (17) | 6783 (1824–13,551) | ||
| Job category | High infectious risk HCWs ** | 44.6 (33) | 6783 (1504–27,600) | 0.027 |
| Medium/low infectious risk *** | 55.4 (41) | 4150 (764–20,300) | ||
| Nightshifts at work | No | 77.8 (56) | 4202 (764–20,300) | 0.124 |
| Yes | 22.2 (16) | 6953 (2508–27,600) | ||
| Anti-influenza vaccine | No | 60.8 (45) | 5062 (830–27,600) | 0.465 |
| Yes | 39.2 (29) | 4497 (764–17,300) | ||
| Previous COVID-19 diagnosis | No | 58.1 (43) | 3746 (764–27,600) | 0.006 |
| Yes | 41.9 (31) | 6856 (1310–20,300) | ||
| Adverse Effect Reported | Vaccination Dose | Workers with the Adverse Effects% (N) * | Workers with the Adverse Effects in the COVID-19 Group% (N) * | Workers with the Adverse Effects in the Non-COVID-19 Group % (N) * | p-Value |
|---|---|---|---|---|---|
| Redness in the injection site | 1st | 25.4 (17) | 33.3 (9) | 20.0 (8) | 0.219 |
| 2nd | 23.9 (16) | 25.9 (7) | 22.5 (9) | 0.747 | |
| Pain in the injection site | 1st | 73.6 (53) | 80.0 (24) | 69. 0 (29) | 0.299 |
| 2nd | 68.1 (49) | 73.3 (22) | 64.3 (27) | 0.417 | |
| Fever | 1st | 7.5 (5) | 7.1 (2) | 7.7 (3) | 0.933 |
| 2nd | 17.9 (12) | 17.9 (5) | 17.9 (7) | 0.992 | |
| Asthenia | 1st | 37.5 (27) | 51.7 (15) | 27.9 (12) | 0.041 |
| 2nd | 48.6 (35) | 48.3 (14) | 48.8 (21) | 0.963 | |
| Myalgia | 1st | 23.1 (15) | 29.6 (8) | 18.4 (7) | 0.291 |
| 2nd | 32.3 (21) | 37.0 (10) | 28.9 (11) | 0.492 | |
| Arthralgia * | 1st | 22.1 (15) | 35.7 (10) | 12.5 (5) | 0.023 |
| 2nd | 32.4 (22) | 42.9 (10) | 25.0 (10) | 0.121 | |
| Headache/migraine | 1st | 25.0 (17) | 35.7 (10) | 17.5 (7) | 0.088 |
| 2nd | 30.9 (21) | 39.3 (11) | 25.0 (10) | 0.210 | |
| Chills | 1st | 18.8 (13) | 20.0 (6) | 17.9 (7) | 0.829 |
| 2nd | 37.7 (26) | 40.0 (12) | 35.9 (14) | 0.727 | |
| Sleepiness | 1st | 32.4 (22) | 41.4 (12) | 25.6 (10) | 0.170 |
| 2nd | 41.2 (28) | 34.5 (10) | 46.2 (18) | 0.333 |
| Previous COVID-19 | After 1st Dose | After 2nd Dose | ||||||
|---|---|---|---|---|---|---|---|---|
| All the Adverse Effects | General Adverse Effects * | All the Adverse Effects | General Adverse Effects * | |||||
| Workers % (N) | Number of Effects ** | Workers % (N) | Number of Effects ** | Workers % (N) | Number of Effects ** | Workers % (N) | Number of Effects ** | |
| Yes | 44.1 (26) | 1 (0–11) | 47.5 (19) | 0 (0–10) | 43.3 (26) | 1 (0–10) | 38.0 (19) | 2 (0–9) *** |
| No | 55.1 (33) | 0 (0–5) | 52.5 (21) | 0 (0–5) | 56.7 (34) | 0 (0–9) | 62.0 (31) | 0 (0–8) *** |
| % (n) of Workers with/without the Adverse Effects & Median (Range) of Neutralizing Anti-SARS-CoV-2 IgG (BAU/mL) | |||||||
|---|---|---|---|---|---|---|---|
| After 1st Dose | After 2nd Dose | ||||||
| All the Adverse Effects% (N) | General Adverse Effects (Not Considering Local)% (N) | All the Adverse Effects% (N) | General Adverse Effects (Not Considering Local)% (N) | ||||
| Yes | No | Yes | No | Yes | No | Yes | No |
| 79.7 (59) 4821 (1243–27,600) | 20.3 (15) 5087 (764–13,749) | 54.0 (40) 5223 (1504–27,600) | 46.0 (34) 4256.5 (764–13,749) | 81.1 (60) 4699.5 (830–27,600) | 18.9 (14) 5651.5 (764–11,638) | 67.6 (50) 4699.5 (830–27,600) | 32.4 (14) 5361 (764–17,300) |
| n.s. | p = 0.017 | n.s. | n.s. | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Modenese, A.; Paduano, S.; Bargellini, A.; Bellucci, R.; Marchetti, S.; Bruno, F.; Grazioli, P.; Vivoli, R.; Gobba, F. Neutralizing Anti-SARS-CoV-2 Antibody Titer and Reported Adverse Effects, in a Sample of Italian Nursing Home Personnel after Two Doses of the BNT162b2 Vaccine Administered Four Weeks Apart. Vaccines 2021, 9, 652. https://doi.org/10.3390/vaccines9060652
Modenese A, Paduano S, Bargellini A, Bellucci R, Marchetti S, Bruno F, Grazioli P, Vivoli R, Gobba F. Neutralizing Anti-SARS-CoV-2 Antibody Titer and Reported Adverse Effects, in a Sample of Italian Nursing Home Personnel after Two Doses of the BNT162b2 Vaccine Administered Four Weeks Apart. Vaccines. 2021; 9(6):652. https://doi.org/10.3390/vaccines9060652
Chicago/Turabian StyleModenese, Alberto, Stefania Paduano, Annalisa Bargellini, Rossana Bellucci, Simona Marchetti, Fulvio Bruno, Pietro Grazioli, Roberto Vivoli, and Fabriziomaria Gobba. 2021. "Neutralizing Anti-SARS-CoV-2 Antibody Titer and Reported Adverse Effects, in a Sample of Italian Nursing Home Personnel after Two Doses of the BNT162b2 Vaccine Administered Four Weeks Apart" Vaccines 9, no. 6: 652. https://doi.org/10.3390/vaccines9060652
APA StyleModenese, A., Paduano, S., Bargellini, A., Bellucci, R., Marchetti, S., Bruno, F., Grazioli, P., Vivoli, R., & Gobba, F. (2021). Neutralizing Anti-SARS-CoV-2 Antibody Titer and Reported Adverse Effects, in a Sample of Italian Nursing Home Personnel after Two Doses of the BNT162b2 Vaccine Administered Four Weeks Apart. Vaccines, 9(6), 652. https://doi.org/10.3390/vaccines9060652