
Attitudes towards COVID-19 Vaccination among Hospital Staff—Understanding What Matters to Hesitant People

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Questionnaire Development and Outcome
2.3. Statistical Analysis
3. Results
3.1. Respondents’ Characteristics and Intention to Get the COVID-19 Vaccine
3.2. Determinants of Attitude towards COVID-19 Vaccination
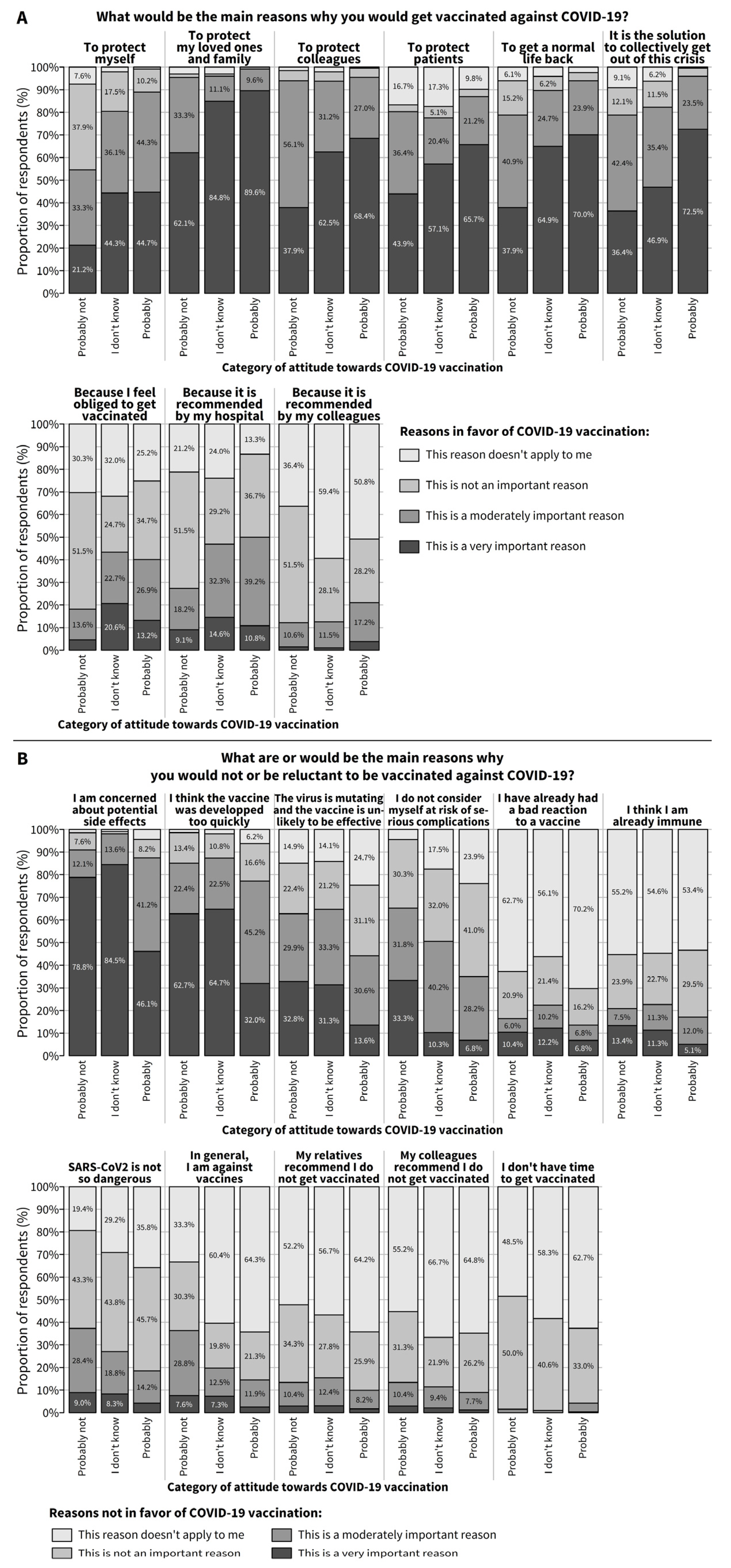
3.3. Characteristics of the Hesitant Subgroup: Reasons for and against COVID-19 Vaccination
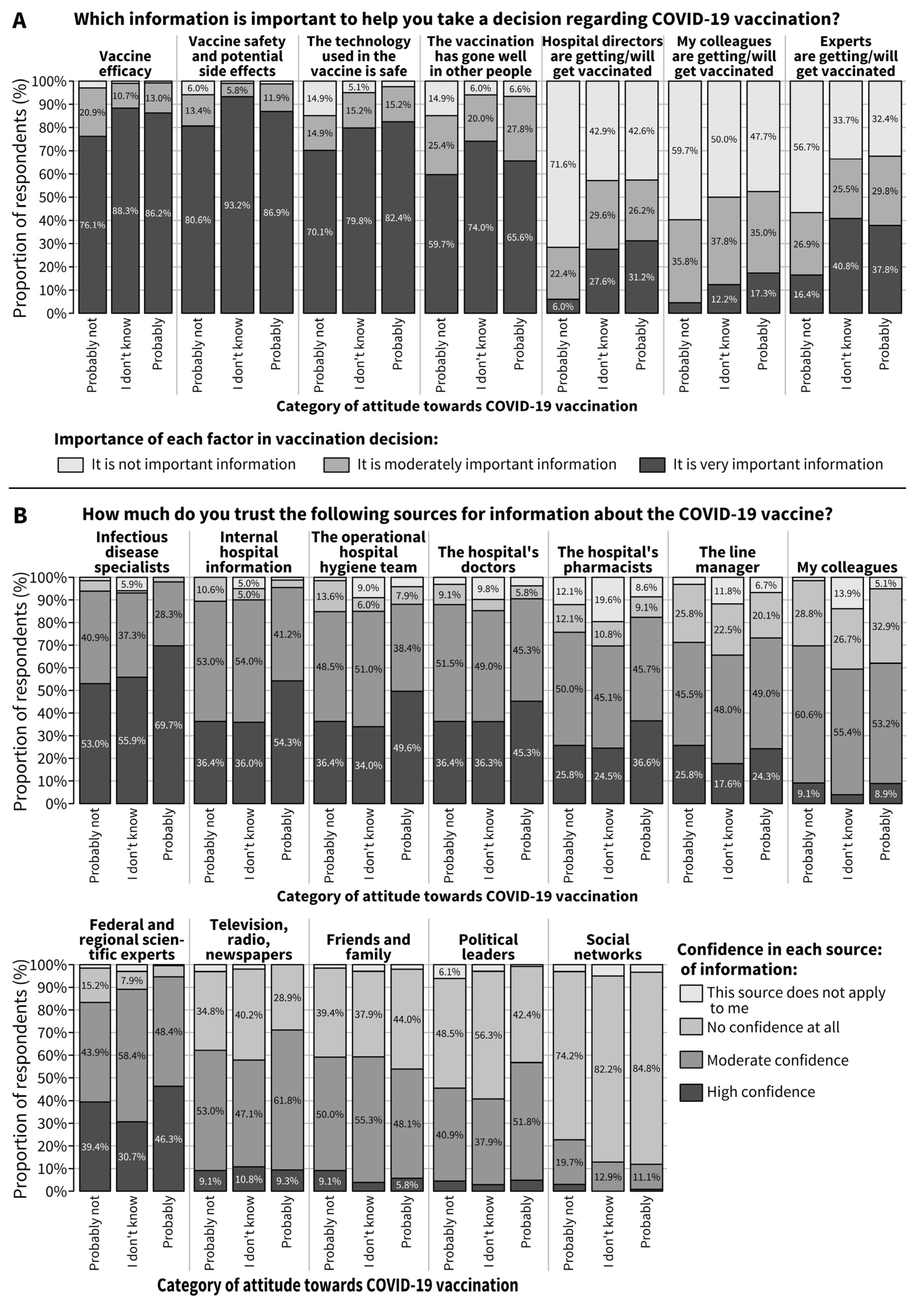
3.4. Need for Information about COVID-19 Vaccine and Trust in Different Sources of Information among Hesitant Respondents
4. Discussion
4.1. Summary of Results
4.2. Vaccination Intention and Factors Associated with Positive Attitude (or Hesitancy)
4.3. Characteristics of the Hesitant Subgroup and Key Messages for Further Tailoring the Vaccination Campaign
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Scores Computed for the Analysis of Factors Associated with Positive Attitudes towards COVID-19 Vaccination
References
- World Health Organization. Weekly Epidemiological Update-1 December 2020. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update---1-december-2020 (accessed on 31 March 2021).
- Sciensano. COVID-19–Bulletin Épidémiologique du 5 Décembre 2020. Available online: https://covid-19.sciensano.be/sites/default/files/Covid19/COVID-19_Daily%20report_20201205%20-%20FR.pdf (accessed on 31 March 2021).
- Bruyneel, A.; Gallani, M.-C.; Tack, J.; d’Hondt, A.; Canipel, S.; Franck, S.; Reper, P.; Pirson, M. Impact of COVID-19 on nursing time in intensive care units in Belgium. Intensive Crit. Care Nurs. 2021, 62, 102967. [Google Scholar] [CrossRef]
- Crowe, S.; Howard, A.F.; Vanderspank-Wright, B.; Gillis, P.; McLeod, F.; Penner, C.; Haljan, G. The effect of COVID-19 pandemic on the mental health of Canadian critical care nurses providing patient care during the early phase pandemic: A mixed method study. Intensive Crit. Care Nurs. 2020, 102999. [Google Scholar] [CrossRef]
- Zheng, R.; Zhou, Y.; Fu, Y.; Xiang, Q.; Cheng, F.; Chen, H.; Xu, H.; Fu, L.; Wu, X.; Feng, M.; et al. Prevalence and associated factors of depression and anxiety among nurses during the outbreak of COVID-19 in China: A cross-sectional study. Int. J. Nurs. Stud. 2021, 114, 103809. [Google Scholar] [CrossRef]
- European Commission. EU Vaccines Strategy: Speeding Up Vaccination in the EU. Available online: https://ec.europa.eu/info/live-work-travel-eu/coronavirus-response/public-health/coronavirus-vaccines-strategy_en#speeding-up-vaccination-in-the-eu (accessed on 23 March 2021).
- Federal Public Service Health Food Chain Safety and Environment. Coronavirus COVID-19: Vaccination. Available online: https://www.info-coronavirus.be/en/vaccination/ (accessed on 23 March 2021).
- Verger, P.; Scronias, D.; Dauby, N.; Adedzi, K.A.; Gobert, C.; Bergeat, M.; Gagneur, A.; Dubé, E. Attitudes of healthcare workers towards COVID-19 vaccination: A survey in France and French-speaking parts of Belgium and Canada, 2020. Eurosurveillance 2021, 26, 2002047. [Google Scholar] [CrossRef]
- Gharpure, R.; Guo, A.; Bishnoi, C.K.; Patel, U.; Gifford, D.; Tippins, A.; Jaffe, A.; Shulman, E.; Stone, N.; Mungai, E.; et al. Early COVID-19 First-Dose Vaccination Coverage Among Residents and Staff Members of Skilled Nursing Facilities Participating in the Pharmacy Partnership for Long-Term Care Program-United States, December 2020–January 2021. Mmwr. Morb. Mortal. Wkly. Rep. 2021, 70, 178–182. [Google Scholar] [CrossRef] [PubMed]
- Eskola, J.; Duclos, P.; Schuster, M.; MacDonald, N.E. How to deal with vaccine hesitancy? Vaccine 2015, 33, 4215–4217. [Google Scholar] [CrossRef] [PubMed]
- French, J.; Deshpande, S.; Evans, W.; Obregon, R. Key Guidelines in Developing a Pre-Emptive COVID-19 Vaccination Uptake Promotion Strategy. Int. J. Environ. Res. Public Health 2020, 17, 5893. [Google Scholar] [CrossRef]
- Blasi, F.; Palange, P.; Rohde, G.; Severin, T.; Cornaglia, G.; Finch, R. Healthcare workers and influenza vaccination: An ERS-ESCMID Web-based survey. Clin. Microbiol. Infect. 2011, 17, 1223–1225. [Google Scholar] [CrossRef] [PubMed]
- Bults, M.; Beaujean, D.J.M.A.; de Zwart, O.; Kok, G.; van Empelen, P.; van Steenbergen, J.E.; Richardus, J.H.; Voeten, H.A.C.M. Perceived risk, anxiety, and behavioural responses of the general public during the early phase of the Influenza A (H1N1) pandemic in the Netherlands: Results of three consecutive online surveys. BMC Public Health 2011, 11, 2. [Google Scholar] [CrossRef]
- Rosenstock, I.M. Why People Use Health Services. Milbank Q. 2005, 83. [Google Scholar] [CrossRef]
- Prematunge, C.; Corace, K.; McCarthy, A.; Nair, R.C.; Pugsley, R.; Garber, G. Factors influencing pandemic influenza vaccination of healthcare workers—A systematic review. Vaccine 2012, 30, 4733–4743. [Google Scholar] [CrossRef]
- Wong, M.C.S.; Wong, E.L.Y.; Huang, J.; Cheung, A.W.L.; Law, K.; Chong, M.K.C.; Ng, R.W.Y.; Lai, C.K.C.; Boon, S.S.; Lau, J.T.F.; et al. Acceptance of the COVID-19 vaccine based on the health belief model: A population-based survey in Hong Kong. Vaccine 2021, 39, 1148–1156. [Google Scholar] [CrossRef]
- Zampetakis, L.A.; Melas, C. The health belief model predicts vaccination intentions against COVID-19: A survey experiment approach. Appl. Psychol. Health Well-Being 2021. [Google Scholar] [CrossRef] [PubMed]
- Fagerland, M.W.; Hosmer, D.W. Tests for goodness of fit in ordinal logistic regression models. J. Stat. Comput. Simul. 2016, 86, 3398–3418. [Google Scholar] [CrossRef]
- R CoreTeam. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018; Available online: https://www.R-project.org/ (accessed on 2 April 2021).
- Kociolek, L.K.; Elhadary, J.; Jhaveri, R.; Patel, A.B.; Stahulak, B.; Cartland, J. Coronavirus disease 2019 vaccine hesitancy among children’s hospital staff: A single-center survey. Infect. Control Hosp. Epidemiol. 2021, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Papagiannis, D.; Rachiotis, G.; Malli, F.; Papathanasiou, I.V.; Kotsiou, O.; Fradelos, E.C.; Giannakopoulos, K.; Gourgoulianis, K.I. Acceptability of COVID-19 Vaccination among Greek Health Professionals. Vaccines 2021, 9, 200. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, J.B.; Bell, R.A. Predictors of intention to vaccinate against COVID-19: Results of a nationwide survey. Vaccine 2021, 39, 1080. [Google Scholar] [CrossRef]
- Gadoth, A.; Halbrook, M.; Martin-Blais, R.; Gray, A.; Tobin, N.H.; Ferbas, K.G.; Aldrovandi, G.M.; Rimoin, A.W. Cross-sectional Assessment of COVID-19 Vaccine Acceptance Among Health Care Workers in Los Angeles. Ann. Intern. Med. 2021. [Google Scholar] [CrossRef]
- Nguyen, K.H.; Srivastav, A.; Razzaghi, H.; Williams, W.; Lindley, M.C.; Jorgensen, C.; Abad, N.; Singleton, J.A. COVID-19 Vaccination Intent, Perceptions, and Reasons for Not Vaccinating Among Groups Prioritized for Early Vaccination-United States, September and December 2020. Mmwr. Morb. Mortal. Wkly. Rep. 2021, 70, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Saied, S.M.; Saied, E.M.; Kabbash, I.A.; Abdo, S.A.E. Vaccine Hesitancy: Beliefs and Barriers Associated with COVID-19 Vaccination among Egyptian Medical Students. J. Med. Virol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Di Martino, G.; Di Giovanni, P.; Di Girolamo, A.; Scampoli, P.; Cedrone, F.; D’Addezio, M.; Meo, F.; Romano, F.; Di Sciascio, M.B.; Staniscia, T. Knowledge and Attitude towards Vaccination among Healthcare Workers: A Multicenter Cross-Sectional Study in a Southern Italian Region. Vaccines 2020, 8, 248. [Google Scholar] [CrossRef] [PubMed]
- Yaqub, O.; Castle-Clarke, S.; Sevdalis, N.; Chataway, J. Attitudes to vaccination: A critical review. Soc. Sci. Med. 2014, 112, 1–11. [Google Scholar] [CrossRef]
- Chou, W.-Y.S.; Burgdorf, C.E.; Gaysynsky, A.; Hunter, C. COVID-19 Vaccination Communication; National Institutes of Health (NIH). Available online: https://obssr.od.nih.gov/wp-content/uploads/2020/12/COVIDReport_Final.pdf (accessed on 2 March 2021).
- Glanz, J.M.; Kraus, C.R.; Daley, M.F. Addressing Parental Vaccine Concerns: Engagement, Balance, and Timing. PLoS Biol. 2015, 13, e1002227. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). How to Build Healthcare Personnel’s Confidence in COVID-19 Vaccines. Available online: https://www.cdc.gov/vaccines/covid-19/downloads/Build-Healthcare-Personnel-Confidence.pdf (accessed on 2 March 2021).
- Germani, F.; Biller-Andorno, N. The anti-vaccination infodemic on social media: A behavioral analysis. PLoS ONE 2021, 16, e0247642. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Total (N = 1132) n (%) | Attitude towards COVID-19 Vaccination | ||
|---|---|---|---|---|
| Will Certainly Not Get the Vaccine (n = 55) n (%) | Is Hesitant to Get the Vaccine (n = 420) n (%) | Will Certainly Get the Vaccine (n = 657) n (%) | ||
| Period of questionnaire completion | ||||
| 1 (6 January to 11 January 2021) | 548 (48.4) | 31 (56.4) | 221 (52.6) | 296 (45.1) |
| 2 (12 January to 15 January 2021) | 247 (21.8) | 12 (21.8) | 86 (20.5) | 149 (22.7) |
| 3 (16 January to 20 January 2021) | 337 (29.8) | 12 (21.8) | 113 (26.9) | 212 (32.3) |
| Socio-demographic variables | ||||
| Age group | ||||
| <35 years | 321 (28.4) | 24 (43.6) | 154 (36.7) | 143 (21.8) |
| 35–44 years | 275 (24.3) | 22 (40.0) | 121 (28.8) | 132 (20.1) |
| 45–54 years | 274 (24.2) | 5 (9.1) | 88 (21.0) | 181 (27.5) |
| ≥55 years | 262 (23.1) | 4 (7.3) | 57 (13.6) | 201 (30.6) |
| Female | 823 (72.7) | 43 (78.2) | 341 (81.2) | 439 (66.8) |
| Work ‡ | ||||
| Medical doctor | 185 (16.5) | 0 (0.0) | 32 (7.6) | 153 (23.6) |
| Nurse or Nursing assistant | 319 (28.5) | 17 (30.9) | 128 (30.5) | 174 (26.9) |
| Paramedical staff | 206 (18.4) | 5 (9.1) | 89 (21.2) | 112 (17.3) |
| Administrative, technical, or logistic staff | 329 (29.3) | 29 (52.7) | 149 (35.6) | 151 (23.3) |
| Other | 82 (7.3) | 4 (7.3) | 21 (5.0) | 57 (8.8) |
| Hospital site | ||||
| Teaching hospital (one site) | 649 (57.3) | 25 (45.5) | 217 (51.7) | 407 (61.9) |
| Non-teaching hospital (two sites) | 468 (41.3) | 29 (52.7) | 197 (46.9) | 242 (36.8) |
| Working at several sites | 15 (1.3) | 1 (1.8) | 6 (1.4) | 8 (1.2) |
| COVID-19 experience | ||||
| Contact with non-COVID-19 and COVID-19 patients * | ||||
| Not in contact with patients at all | 232 (20.5) | 9 (16.7) | 106 (25.3) | 117 (17.8) |
| Contact with non-COVID-19 patients | 230 (20.4) | 16 (29.6) | 87 (20.8) | 127 (19.4) |
| Previously in contact with COVID-19 patient, but not now | 333 (29.5) | 16 (29.6) | 114 (27.2) | 203 (30.9) |
| Current contact with COVID-19 patients | 334 (29.6) | 13 (24.1) | 112 (26.7) | 209 (31.9) |
| Personal infection with SARS-CoV-2 and COVID-19 symptoms ** | ||||
| Never infected | 866 (76.8) | 43 (79.6) | 312 (74.5) | 511 (78.0) |
| Yes, with no, mild, or moderate symptoms | 214 (19.0) | 10 (18.5) | 82 (19.6) | 122 (18.6) |
| Yes, with major symptoms or hospitalization | 48 (4.3) | 1 (1.9) | 25 (6.0) | 22 (3.4) |
| Infection of people living under the same roof with SARS-CoV-2 and COVID-19 symptoms *** | ||||
| No-one infected | 847 (75.2) | 43 (78.2) | 301 (72.2) | 503 (76.8) |
| Yes, with no, mild or moderate symptoms | 268 (23.8) | 11 (20.0) | 112 (26.9) | 145 (22.1) |
| Yes, and required hospitalization | 12 (1.1) | 1 (1.8) | 4 (1.0) | 7 (1.1) |
| Infection of colleagues with SARS-CoV-2 and COVID-19 symptoms † | ||||
| No-one infected | 149 (13.3) | 13 (23.6) | 66 (15.9) | 70 (10.7) |
| Yes, with no, mild, or moderate symptoms | 892 (79.5) | 41 (74.5) | 324 (78.3) | 527 (80.7) |
| Yes, and required hospitalization | 81 (7.2) | 1 (1.8) | 24 (5.8) | 56 (8.6) |
| Attitude towards COVID-19 vaccination | ||||
| Certainly not getting the COVID-19 vaccine | 55 (4.9) | |||
| Probably not getting the COVID-19 vaccine | 67 (5.9) | |||
| I don’t know | 103 (9.1) | |||
| Yes, probably getting the COVID-19 vaccine | 250 (22.1) | |||
| Yes, certainly getting the COVID-19 vaccine | 657 (58.0) | |||
| Variables | n (%) or Median [P25; P75] | Univariate Analysis (N = 1132) | Multivariable Analysis (N = 1077) | ||
|---|---|---|---|---|---|
| OR [95% CI] | p-Value | OR [95% CI] | p-Value | ||
| Period of questionnaire completion | |||||
| 1 (Jan 6 to Jan 11, 2021) | 548 (48.4) | 1.00 | 1.00 | ||
| 2 (Jan 12 to Jan 15, 2021) | 247 (21.8) | 1.29 [0.97; 1.74] | 0.084 | 1.41 [0.98; 2.02] | 0.063 |
| 3 (Jan 16 to Jan 20, 2021) | 337 (29.8) | 1.39 [1.07; 1.82] | 0.016 | 2.11 [1.52; 2.95] | <0.001 |
| Socio-demographic variables | |||||
| Age group | |||||
| <35 years | 321 (28.4) | 1.00 | 1.00 | ||
| 35–44 years | 275 (24.3) | 1.19 [0.88; 1.60] | 0.257 | 1.18 [0.83; 1.69] | 0.348 |
| 45–54 years | 274 (24.2) | 2.57 [1.87; 3.54] | <0.001 | 2.30 [1.56; 3.39] | <0.001 |
| ≥55 years | 262 (23.1) | 4.22 [2.98; 6.02] | <0.001 | 3.45 [2.20; 5.47] | <0.001 |
| Female | 0.47 [0.36; 0.62] | <0.001 | 0.48 [0.34; 0.68] | <0.001 | |
| Work ††† | |||||
| Medical doctor | 185 (16.5) | 5.77 [3.80; 8.98] | <0.001 | 1.88 [1.07; 3.36] | 0.030 |
| Nurse or Nursing assistant | 319 (28.5) | 1.35 [1.01; 1.81] | 0.042 | 0.68 [0.47; 0.98] | 0.040 |
| Paramedical staff | 206 (18.4) | 1.41 [1.02; 1.96] | 0.040 | 1.03 [0.70; 1.53] | 0.883 |
| Administrative, technical, or logistic staff | 329 (29.3) | 1.00 | 1.00 | ||
| Other | 82 (7.3) | 2.54 [1.54; 4.27] | <0.001 | 1.08 [0.56; 2.12] | 0.830 |
| Working in a teaching hospital | 1.61 [1.28; 2.02] | <0.001 | |||
| Personal health status | |||||
| Presence of COVID-19 risk factor(s) † | 256 (22.7) | 1.31 [1.00; 1.73] | 0.053 | ||
| Seasonal flu vaccination in 2020 † | 564 (50.0) | 5.20 [4.05; 6.69] | <0.001 | 3.02 [2.22; 4.12] | <0.001 |
| COVID-19 experience | |||||
| Contact with non-COVID-19 and COVID-19 patients *** | |||||
| Not in contact with patients at all | 232 (20.5) | 1.00 | |||
| Contact with non-COVID-19 patients | 230 (20.4) | 1.18 [0.84; 1.66] | 0.349 | ||
| Previously in contact with COVID-19 patients, but not now | 333 (29.5) | 1.37 [0.99; 1.88] | 0.056 | ||
| Current contact with COVID-19 patients | 334 (29.6) | 1.48 [1.08; 2.05] | 0.016 | ||
| Personal infection with SARS-CoV-2 and COVID-19 symptoms † | |||||
| Never infected | 866 (76.8) | 1.00 | |||
| Yes, with no, mild, or moderate symptoms | 214 (19) | 0.94 [0.71; 1.26] | 0.678 | ||
| Yes, with major symptoms or hospitalization | 48 (4.3) | 0.77 [0.46; 1.31] | 0.330 | ||
| Infection of colleagues with SARS-CoV-2 and COVID-19 symptoms †† | |||||
| No-one infected | 149 (13.3) | 1.00 | 1.00 | ||
| No, mild, or moderate symptoms | 892 (79.5) | 1.72 [1.24; 2.39] | 0.001 | 1.69 [1.11; 2.55] | 0.014 |
| Required hospitalization | 81 (7.2) | 2.61 [1.52; 4.59] | 0.001 | 2.69 [1.37; 5.41] | 0.005 |
| HBM—perceived susceptibility | |||||
| Probability of being infected/re-infected * | |||||
| Fairly or very likely | 439 (38.8) | 1.00 | 1.00 | ||
| Not really likely | 243 (21.5) | 0.63 [0.46; 0.86] | 0.004 | 0.78 [0.54; 1.15] | 0.210 |
| Not at all likely | 15 (1.3) | 0.12 [0.04; 0.34] | <0.001 | 0.32 [0.09; 1.19] | 0.087 |
| No opinion | 434 (38.4) | 0.53 [0.40; 0.68] | <0.001 | 0.69 [0.50; 0.95] | 0.025 |
| HBM—perceived seriousness | |||||
| Expected consequences in case of future infection * | |||||
| Quite or very serious | 180 (15.9) | 1.00 | |||
| Not really serious | 434 (38.4) | 0.44 [0.30; 0.63] | <0.001 | ||
| Not at all serious | 50 (4.4) | 0.21 [0.11; 0.40] | <0.001 | ||
| No opinion | 467 (41.3) | 0.46 [0.32; 0.67] | <0.001 | ||
| Expected consequences in case of future infection for a relative ** | |||||
| Very serious | 223 (19.7) | 1.00 | 1.00 | ||
| Quite serious | 529 (46.8) | 0.57 [0.41; 0.79] | 0.001 | 0.68 [0.46; 1.01] | 0.060 |
| No consequences for any relatives | 139 (12.3) | 0.40 [0.26; 0.61] | <0.001 | 0.37 [0.22; 0.62] | <0.001 |
| No opinion | 239 (21.2) | 0.36 [0.25; 0.52] | <0.001 | 0.45 [0.29; 0.71] | 0.001 |
| HBM—perceived benefits of taking action | |||||
| Score for perceived personal benefits: for personal protection, to be able to get back to a more normal life (−2 to 2) †† | 1.0 [0.0; 2.0] | 2.37 [2.09; 2.69] | <0.001 | 1.35 [1.15; 1.58] | <0.001 |
| Score for perceived benefits for others: to protect relatives, to protect patients, to protect colleagues (−3 to 3) †† | 3.0 [2.0; 3.0] | 1.95 [1.76; 2.16] | <0.001 | 1.38 [1.22; 1.57] | <0.001 |
| It is a solution to collectively get out of this crisis †† | |||||
| Not important or this reason does not apply to me | 83 (7.4) | 0.12 [0.07; 0.20] | <0.001 | 0.23 [0.13; 0.39] | <0.001 |
| Moderately important | 188 (16.8) | 1.00 | 1.00 | ||
| Very important | 851 (75.8) | 6.06 [4.45; 8.28] | <0.001 | 3.21 [2.25; 4.57] | <0.001 |
| HBM—Cues to action | |||||
| Score for perception of being sufficiently informed about vaccine efficacy, side effects and safety, and development process (−3 to 3) ‡ | −1 [−3; 1] | 1.46 [1.38; 1.55] | <0.001 | 1.22 [1.13; 1.32] | <0.001 |
| Knowledge about COVID-19 vaccine | |||||
| Score for knowledge about COVID-19 vaccine (0 to 4) ‡‡ | 1.0 [1.0; 2.0] | 1.74 [1.55; 1.96] | <0.001 | 1.12 [0.96; 1.30] | 0.139 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spinewine, A.; Pétein, C.; Evrard, P.; Vastrade, C.; Laurent, C.; Delaere, B.; Henrard, S. Attitudes towards COVID-19 Vaccination among Hospital Staff—Understanding What Matters to Hesitant People. Vaccines 2021, 9, 469. https://doi.org/10.3390/vaccines9050469
Spinewine A, Pétein C, Evrard P, Vastrade C, Laurent C, Delaere B, Henrard S. Attitudes towards COVID-19 Vaccination among Hospital Staff—Understanding What Matters to Hesitant People. Vaccines. 2021; 9(5):469. https://doi.org/10.3390/vaccines9050469
Chicago/Turabian StyleSpinewine, Anne, Catherine Pétein, Perrine Evrard, Christelle Vastrade, Christine Laurent, Bénédicte Delaere, and Séverine Henrard. 2021. "Attitudes towards COVID-19 Vaccination among Hospital Staff—Understanding What Matters to Hesitant People" Vaccines 9, no. 5: 469. https://doi.org/10.3390/vaccines9050469
APA StyleSpinewine, A., Pétein, C., Evrard, P., Vastrade, C., Laurent, C., Delaere, B., & Henrard, S. (2021). Attitudes towards COVID-19 Vaccination among Hospital Staff—Understanding What Matters to Hesitant People. Vaccines, 9(5), 469. https://doi.org/10.3390/vaccines9050469