
An Unconventional Case Study of Neoadjuvant Oncolytic Virotherapy for Recurrent Breast Cancer

 , and
, and {kind=link}
{kind=link}
Abstract
1. Introduction
2. Results
2.1. Patient and Case History
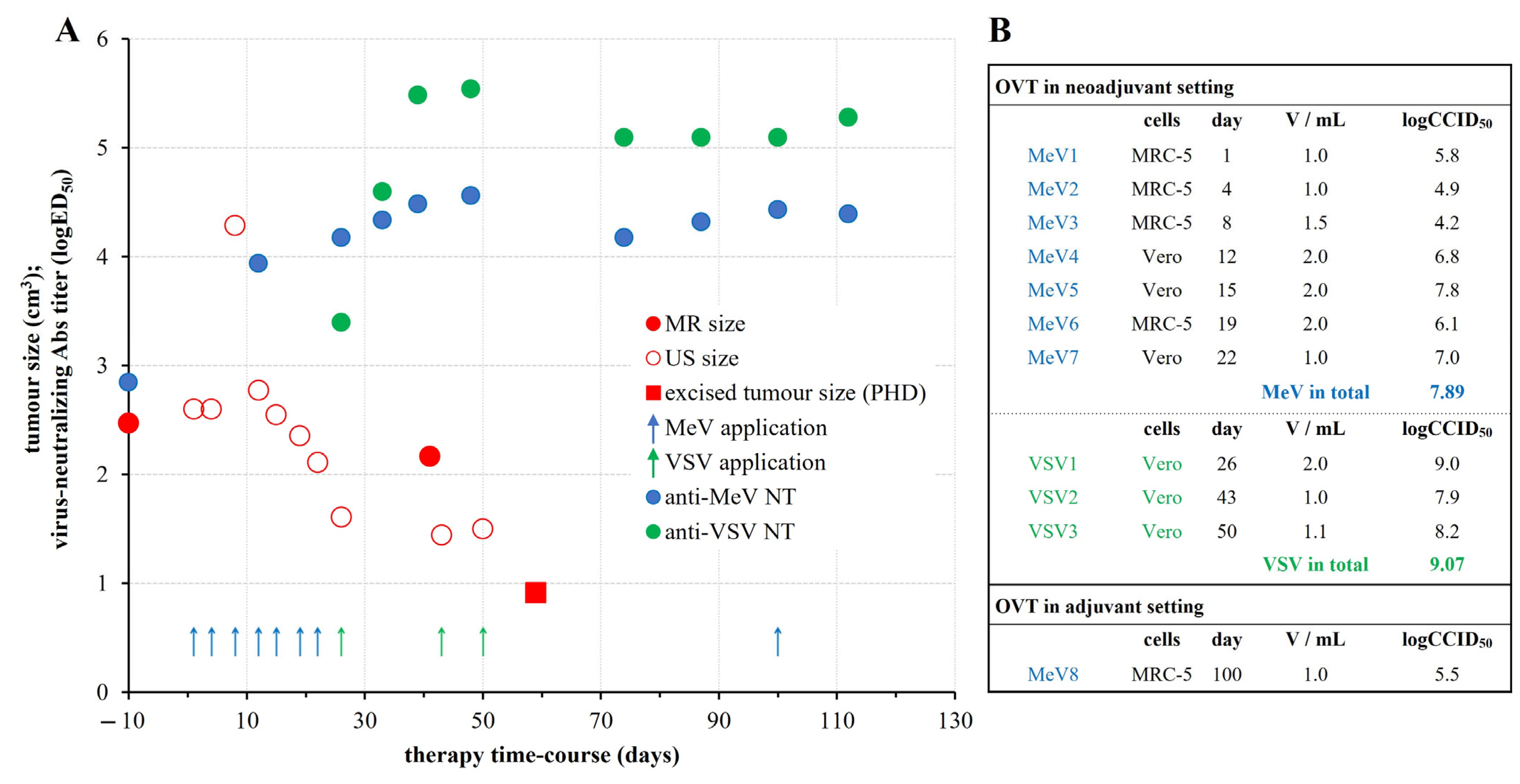
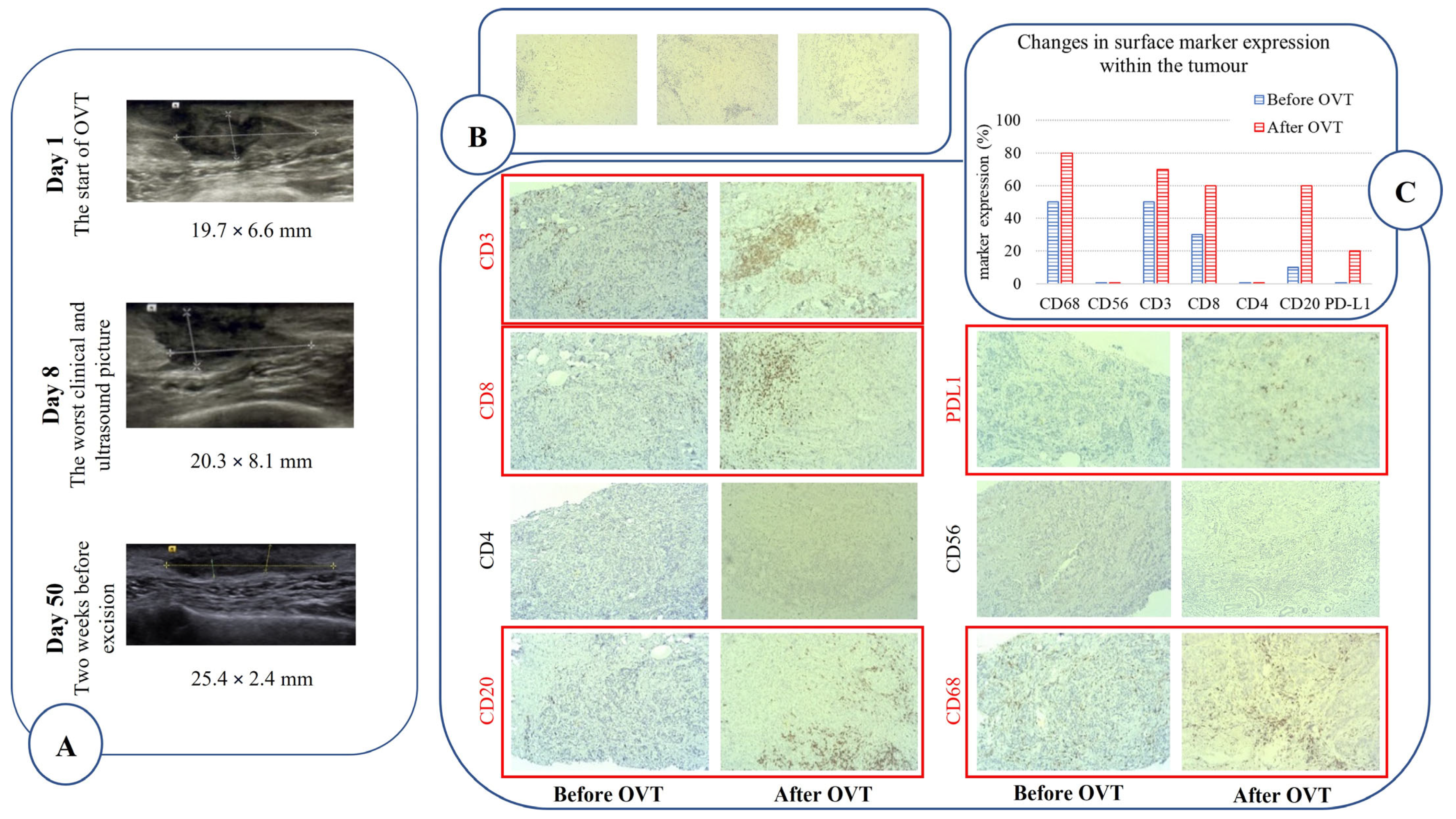
2.2. Oncolytic Virotherapy Protocol and Outcomes
3. Discussion
4. Materials and Methods
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lukasiewicz, S.; Czeczelewski, M.; Forma, A.; Baj, J.; Sitarz, R.; Stanisławek, A. Breast Cancer—Epidemiology, Risk Factors, Classification, Prognostic Markers, and Current Treatment Strategies—An Updated Review. Cancers 2021, 13, 4287. [Google Scholar] [CrossRef] [PubMed]
- Harrington, K.; Freeman, D.J.; Kelly, B.; Harper, J.; Soria, J.C. Optimizing oncolytic virotherapy in cancer treatment. Nat. Rev. Drug Discov. 2019, 18, 689–706. [Google Scholar] [CrossRef] [PubMed]
- Russell, S.J.; Peng, K.W.; Bell, J.C. Oncolytic virotherapy. Nat. Biotechnol. 2014, 30, 658–670. [Google Scholar] [CrossRef] [PubMed]
- Chaurasiya, S.; Fong, Y. Viroimmunotherapy for breast cancer: Promises, problems and future directions. Cancer Gene Ther. 2021, 28, 757–768. [Google Scholar] [CrossRef]
- Martini, V.; D’Avanzo, F.; Maggiora, P.M.; Varughese, F.M.; Sica, A.; Gennari, A. Oncolytic virotherapy: New weapon for breast cancer treatment. Ecancermedicalscience 2020, 14, 1149. [Google Scholar] [CrossRef]
- Msaouel, P.; Opyrchal, M.; Dispenzieri, A.; Whye Peng, K.; Federspiel, M.J.; Russell, S.J.; Galanis, E. Clinical trials with oncolytic mealses virus: Current status and future prospects. Curr. Cancer Drug Targets 2018, 18, 177–187. [Google Scholar] [CrossRef] [PubMed]
- Russell, S.J.; Bell, J.C.; Engeland, C.E.; McFadden, G. Advances in oncolytic virotherapy. Commun. Med. 2022, 2, 4–6. [Google Scholar] [CrossRef]
- Thomas, R.J.; Bartee, E. The use of oncolytic virotherapy in the neoadjuvant setting. J. Immunother. Cancer 2022, 10, e004462. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.F.; Chen, P.J.; Sze, D.Y.; Reid, T.; Bartlett, D.; Kirn, D.H.; Liu, T.C. Oncolytic virotherapy for advanced liver tumours. J. Cell. Mol. Med. 2009, 13, 1238–1247. [Google Scholar] [CrossRef]
- Park, B.H.; Hwang, T.; Liu, T.C.; Sze, D.Y.; Kim, J.S.; Kwon, H.C.; Oh, S.Y.; Han, S.Y.; Yoon, J.H.; Hong, S.H.; et al. Use of a targeted oncolytic poxvirus, JX-594, in patients with refractory primary or metastatic liver cancer: A phase I trial. Lancet Oncol. 2008, 9, 533–542. [Google Scholar] [CrossRef]
- Lievano, F.; Galea, S.A.; Thornton, M.; Wiedmann, R.T.; Manoff, S.B.; Tran, T.N.; Amin, M.A.; Seminack, M.M.; Vagie, K.A.; Dana, A.; et al. Measles, mumps, and rubella virus vaccine (M-M-RTMII): A review of 32 years of clinical and postmarketing experience. Vaccine 2012, 30, 6918–6926. [Google Scholar] [CrossRef] [PubMed]
- Baldo, A.; Galanis, E.; Tangy, F.; Herman, P. Biosafety considerations for attenuated measles virus vectors used in virotherapy and vaccination. Hum. Vaccines Immunother. 2016, 12, 1102–1116. [Google Scholar] [CrossRef] [PubMed]
- Matveeva, O.V.; Shabalina, S.A. Prospects for using expression patterns of paramyxovirus receptors as biomarkers for oncolytic virotherapy. Cancers 2020, 12, 3659. [Google Scholar] [CrossRef] [PubMed]
- Aref, S.; Bailey, K.; Fielding, A. Measles to the rescue: A review of oncolytic measles virus. Viruses 2016, 8, 294. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Nagalo, B.M. Immunovirotherapy Based on Recombinant Vesicular Stomatitis Virus: Where Are We? Front. Immunol. 2022, 13, 898631. [Google Scholar] [CrossRef]
- Martin, N.T.; Roy, D.G.; Workenhe, S.T.; van Den Wollenberg, D.J.; Hoeben, R.C.; Mossman, K.L.; Bell, J.C.; Bourgeois-Daigneault, M.C. Pre-surgical neoadjuvant oncolytic virotherapy confers protection against rechallenge in a murine model of breast cancer. Sci. Rep. 2019, 9, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Muik, A.; Stubbert, L.J.; Jahedi, R.Z.; Geiβ, Y.; Kimpel, J.; Dold, C.; Tober, R.; Volk, A.; Klein, S.; Dietrich, U.; et al. Re-engineering vesicular stomatitis virus to abrogate neurotoxicity, circumvent humoral immunity, and enhance oncolytic potency. Cancer Res. 2014, 74, 3567–3578. [Google Scholar] [CrossRef]
- van den Pol, A.N.; Dalton, K.P.; Rose, J.K. van den Pol J Virol 2002.pdf. J. Virol. 2002, 76, 1309–1327. [Google Scholar] [CrossRef]
- Johnson, J.E.; Nasar, F.; Coleman, J.W.; Price, R.E.; Javadian, A.; Draper, K.; Lee, M.; Reilly, P.A.; Clarke, D.K.; Hendry, R.M.; et al. Neurovirulence properties of recombinant vesicular stomatitis virus vectors in non-human primates. Virology 2007, 360, 36–49. [Google Scholar] [CrossRef]
- Rodrigues, A.F.; Soares, H.R.; Guerreiro, M.R.; Alves, P.M.; Coroadinha, A.S. Viral vaccines and their manufacturing cell substrates: New trends and designs in modern vaccinology. Biotechnol. J. 2015, 10, 1329–1344. [Google Scholar] [CrossRef]
- Tysome, J.R.; Li, X.; Wang, S.; Wang, P.; Gao, D.; Du, P.; Chen, D.; Gangeswaran, R.; Chard, L.S.; Yuan, M.; et al. A novel therapeutic regimen to eradicate established solid tumors with an effective induction of tumor-specific immunity. Clin. Cancer Res. 2012, 18, 6679–6689. [Google Scholar] [CrossRef]
- Thorne, S.H. Methods of Treating Cancer. International Patent Application WO2020/146411A1, 16 July 2020. 69p. [Google Scholar]
- Bell, J.C.; Stojdl, D.F. Oncolytic Rhabdovirus. U.S. Patent US9896664B2, 20 February 2018. 89p. [Google Scholar]
- Nielsen, J.S.; Sahota, R.A.; Milne, K.; Kost, S.E.; Nesslinger, N.J.; Watson, P.H.; Nelson, B.H. CD20+ tumor-infiltrating lymphocytes have an atypical CD27—Memory phenotype and together with CD8+ T cells promote favorable prognosis in ovarian cancer. Clin. Cancer Res. 2012, 18, 3281–3292. [Google Scholar] [CrossRef] [PubMed]
- Milne, K.; Köbel, M.; Kalloger, S.E.; Barnes, R.O.; Gao, D.; Gilks, C.B.; Watson, P.H.; Nelson, B.H. Systematic analysis of immune infiltrates in high-grade serous ovarian cancer reveals CD20, FoxP3 and TIA-1 as positive prognostic factors. PLoS ONE 2009, 4, e6412. [Google Scholar] [CrossRef] [PubMed]
- Kinker, G.S.; Vitiello, G.A.F.; Ferreira, W.A.S.; Chaves, A.S.; Cordeiro de Lima, V.C.; Medina, T.D.S. B cell orchestration of anti-tumor immune responses: A matter of cell localization and communication. Front. Cell Dev. Biol. 2021, 9, 678127. [Google Scholar] [CrossRef] [PubMed]
- Schumacher, T.N.; Schreiber, R.D. Neoantigens in cancer immunotherapy. Science 2015, 348, 69–74. [Google Scholar] [CrossRef]
- Sautès-Fridman, C.; Petitprez, F.; Calderaro, J.; Fridman, W.H. Tertiary lymphoid structures in the era of cancer immunotherapy. Nat. Rev. Cancer 2019, 19, 307–325. [Google Scholar] [CrossRef] [PubMed]
- Sharonov, G.V.; Serebrovskaya, E.O.; Yuzhakova, D.V.; Britanova, O.V.; Chudakov, D.M. B cells, plasma cells and antibody repertoires in the tumour microenvironment. Nat. Rev. Immunol. 2020, 20, 294–307. [Google Scholar] [CrossRef]
- Shen, M.; Sun, Q.; Wang, J.; Pan, W.; Ren, X. Positive and negative functions of B lymphocytes in tumors. Oncotarget 2016, 7, 55828–55839. [Google Scholar] [CrossRef]
- Cardoso, F.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rubio, I.T.; Zackrisson, S.; Senkus, E. Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019, 30, 1194–1220. [Google Scholar] [CrossRef]
- Baričević, M.; Forčić, D.; Gulija, T.K.; Jug, R.; Mažuran, R. Determination of the coding and non-coding nucleotide sequences of genuine Edmonston-Zagreb master seed and current working seed lot. Vaccine 2005, 23, 1072–1078. [Google Scholar] [CrossRef] [PubMed]
- Rammensee, H.G.; Gouttefangeas, C.; Heidu, S.; Klein, R.; Preuß, B.; Walz, J.S.; Nelde, A.; Haen, S.P.; Reth, M.; Yang, J.; et al. Designing a SARS-CoV-2 T-cell-inducing vaccine for high-risk patient groups. Vaccines 2021, 9, 428. [Google Scholar] [CrossRef] [PubMed]
- Hanley, B.P.; Bains, W.; Church, G. Review of scientific self-experimentation: Ethics history, regulation, scenarios, and views among ethics committees and prominent scientists. Rejuvenat. Res. 2019, 22, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Rammensee, H.G.; Wiesmüller, K.H.; Chandran, P.A.; Zelba, H.; Rusch, E.; Gouttefangeas, C.; Kowalewski, D.J.; Di Marco, M.; Haen, S.P.; Walz, J.S.; et al. A new synthetic toll-like receptor 1/2 ligand is an efficient adjuvant for peptide vaccination in a human volunteer. J. Immunother. Cancer 2019, 7, 307. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forčić, D.; Mršić, K.; Perić-Balja, M.; Kurtović, T.; Ramić, S.; Silovski, T.; Pedišić, I.; Milas, I.; Halassy, B. An Unconventional Case Study of Neoadjuvant Oncolytic Virotherapy for Recurrent Breast Cancer. Vaccines 2024, 12, 958. https://doi.org/10.3390/vaccines12090958
Forčić D, Mršić K, Perić-Balja M, Kurtović T, Ramić S, Silovski T, Pedišić I, Milas I, Halassy B. An Unconventional Case Study of Neoadjuvant Oncolytic Virotherapy for Recurrent Breast Cancer. Vaccines. 2024; 12(9):958. https://doi.org/10.3390/vaccines12090958
Chicago/Turabian StyleForčić, Dubravko, Karmen Mršić, Melita Perić-Balja, Tihana Kurtović, Snježana Ramić, Tajana Silovski, Ivo Pedišić, Ivan Milas, and Beata Halassy. 2024. "An Unconventional Case Study of Neoadjuvant Oncolytic Virotherapy for Recurrent Breast Cancer" Vaccines 12, no. 9: 958. https://doi.org/10.3390/vaccines12090958
APA StyleForčić, D., Mršić, K., Perić-Balja, M., Kurtović, T., Ramić, S., Silovski, T., Pedišić, I., Milas, I., & Halassy, B. (2024). An Unconventional Case Study of Neoadjuvant Oncolytic Virotherapy for Recurrent Breast Cancer. Vaccines, 12(9), 958. https://doi.org/10.3390/vaccines12090958