

Role of Oxidative Stress and Lipid Peroxidation in the Pathophysiology of NAFLD

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Liver Histology
2.3. Biochemical Parameters
2.4. Oxidative Stress Determinations
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics
3.2. Oxidative Stress Levels in NAFLD
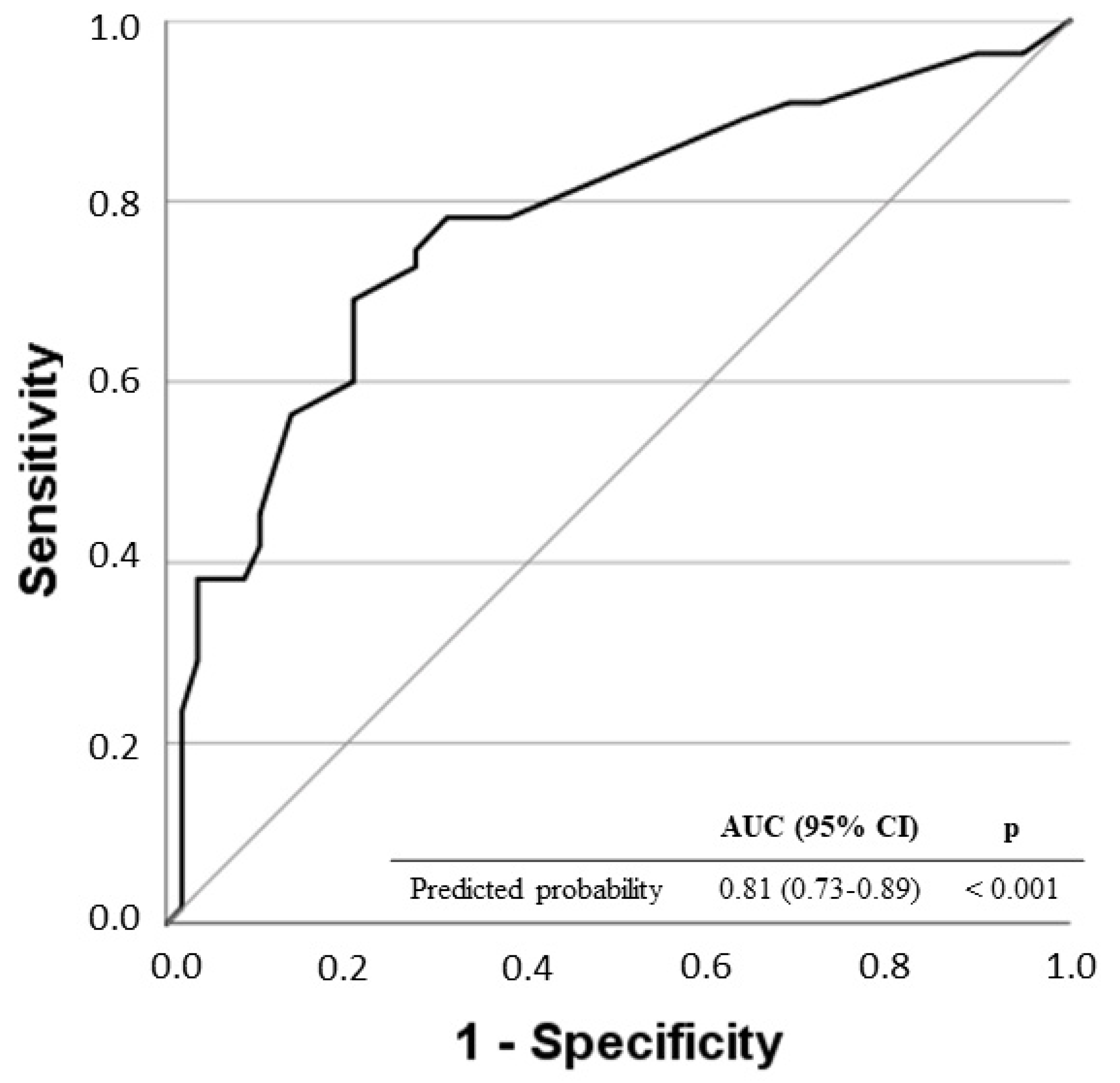
3.3. Evaluation of the Risk of NASH Score Depending on LPO Levels
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global Epidemiology of Nonalcoholic Fatty Liver Disease-Meta-Analytic Assessment of Prevalence, Incidence, and Outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diehl, A.M.; Day, C. Cause, Pathogenesis, and Treatment of Nonalcoholic Steatohepatitis. N. Engl. J. Med. 2017, 377, 2063–2072. [Google Scholar] [CrossRef] [PubMed]
- Lazo, M.; Clark, J.M. The Epidemiology of Nonalcoholic Fatty Liver Disease: A Global Perspective. Semin. Liver Dis. 2008, 28, 339–350. [Google Scholar] [CrossRef] [PubMed]
- Vuppalanchi, R.; Unalp, A.; Van Natta, M.L.; Cummings, O.W.; Sandrasegaran, K.E.; Hameed, T.; Tonascia, J.; Chalasani, N. Effects of Liver Biopsy Sample Length and Number of Readings on Sampling Variability in Nonalcoholic Fatty Liver Disease. Clin. Gastroenterol. Hepatol. 2009, 7, 481–486. [Google Scholar] [CrossRef] [Green Version]
- Angulo, P.; Hui, J.M.; Marchesini, G.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P.; et al. The NAFLD Fibrosis Score: A Noninvasive System That Identifies Liver Fibrosis in Patients with NAFLD. Hepatology 2007, 45, 846–854. [Google Scholar] [CrossRef]
- Wong, V.W.-S.; Adams, L.A.; de Lédinghen, V.; Wong, G.L.-H.; Sookoian, S. Noninvasive Biomarkers in NAFLD and NASH—Current Progress and Future Promise. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 461–478. [Google Scholar] [CrossRef]
- Mofrad, P.; Contos, M.J.; Haque, M.; Sargeant, C.; Fisher, R.A.; Luketic, V.A.; Sterling, R.K.; Shiffman, M.L.; Stravitz, R.T.; Sanyal, A.J. Clinical and Histologic Spectrum of Nonalcoholic Fatty Liver Disease Associated with Normal ALT Values. Hepatology 2003, 37, 1286–1292. [Google Scholar] [CrossRef]
- Oseini, A.M.; Sanyal, A.J. Therapies in Non-Alcoholic Steatohepatitis (NASH). Liver Int. 2017, 37, 97–103. [Google Scholar] [CrossRef] [Green Version]
- Caballería, L.; Torán, P.; Caballería, J. Markers of Hepatic Fibrosis. Med. Clin. 2018, 150, 310–316. [Google Scholar] [CrossRef]
- Tacke, F.; Weiskirchen, R. Non-Alcoholic Fatty Liver Disease (NAFLD)/Non-Alcoholic Steatohepatitis (NASH)-Related Liver Fibrosis: Mechanisms, Treatment and Prevention. Ann. Transl. Med. 2021, 9, 729. [Google Scholar] [CrossRef]
- Sies, H. Oxidative Stress: From Basic Research to Clinical Application. Am. J. Med. 1991, 91, 31S–38S. [Google Scholar] [CrossRef]
- Phaniendra, A.; Jestadi, D.B.; Periyasamy, L. Free Radicals: Properties, Sources, Targets, and Their Implication in Various Diseases. Indian J. Clin. Biochem. 2015, 30, 11–26. [Google Scholar] [CrossRef] [Green Version]
- Polimeni, L.; Del Ben, M.; Baratta, F.; Perri, L.; Albanese, F.; Pastori, D.; Violi, F.; Angelico, F. Oxidative Stress: New Insights on the Association of Non-Alcoholic Fatty Liver Disease and Atherosclerosis. World J. Hepatol. 2015, 7, 1325–1336. [Google Scholar] [CrossRef] [PubMed]
- Benzie, I.F. Lipid Peroxidation: A Review of Causes, Consequences, Measurement and Dietary Influences. Int. J. Food Sci. Nutr. 1996, 47, 233–261. [Google Scholar] [CrossRef] [PubMed]
- James, O.F.; Day, C.P. Non-Alcoholic Steatohepatitis (NASH): A Disease of Emerging Identity and Importance. J. Hepatol. 1998, 29, 495–501. [Google Scholar] [CrossRef]
- Koek, G.H.; Liedorp, P.R.; Bast, A. The Role of Oxidative Stress in Non-Alcoholic Steatohepatitis. Clin. Chim. Acta 2011, 412, 1297–1305. [Google Scholar] [CrossRef] [PubMed]
- Ampuero, J.; Aller, R.; Gallego-Durán, R.; Crespo, J.; Abad, J.; González-Rodríguez, Á.; Gómez-Camarero, J.; Caballería, J.; Lo Iacono, O.; Ibañez, L.; et al. Definite and Indeterminate Nonalcoholic Steatohepatitis Share Similar Clinical Features and Prognosis: A Longitudinal Study of 1893 Biopsy-Proven Nonalcoholic Fatty Liver Disease Subjects. Liver Int. 2021, 41, 2076–2086. [Google Scholar] [CrossRef]
- Bedossa, P. Pathology of Non-Alcoholic Fatty Liver Disease. Liver Int. 2017, 37, 85–89. [Google Scholar] [CrossRef] [Green Version]
- Ratziu, V.; Bellentani, S.; Cortez-Pinto, H.; Day, C.; Marchesini, G. A Position Statement on NAFLD Based on the EASL 2009 Special Conference. J. Hepatol. 2010, 53, 372–384. [Google Scholar] [CrossRef] [Green Version]
- Duart Duart, M.J.; Arroyo, C.O.; Moreno Frígols, J.L. Validation of a Kinetic Model for the Reactions in RIA. Clin. Chem. Lab Med. 2002, 40, 1161–1167. [Google Scholar] [CrossRef]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the Concentration of Low-Density Lipoprotein Cholesterol in Plasma, without Use of the Preparative Ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Martín-Fernández, M.; Aller, R.; Heredia-Rodríguez, M.; Gómez-Sánchez, E.; Martínez-Paz, P.; Gonzalo-Benito, H.; Sánchez-de Prada, L.; Gorgojo, Ó.; Carnicero-Frutos, I.; Tamayo, E.; et al. Lipid Peroxidation as a Hallmark of Severity in COVID-19 Patients. Redox Biol. 2021, 48, 102181. [Google Scholar] [CrossRef] [PubMed]
- Gonzalo, H.; Nogueras, L.; Gil-Sánchez, A.; Hervás, J.V.; Valcheva, P.; González-Mingot, C.; Martin-Gari, M.; Canudes, M.; Peralta, S.; Solana, M.J.; et al. Impairment of Mitochondrial Redox Status in Peripheral Lymphocytes of Multiple Sclerosis Patients. Front. Neurosci. 2019, 13, 938. [Google Scholar] [CrossRef] [PubMed]
- Brunt, E.M.; Kleiner, D.E.; Wilson, L.A.; Belt, P.; Neuschwander-Tetri, B.A.; NASH Clinical Research Network (CRN). Nonalcoholic Fatty Liver Disease (NAFLD) Activity Score and the Histopathologic Diagnosis in NAFLD: Distinct Clinicopathologic Meanings. Hepatology 2011, 53, 810–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleiner, D.E.; Brunt, E.M.; Van Natta, M.; Behling, C.; Contos, M.J.; Cummings, O.W.; Ferrell, L.D.; Liu, Y.-C.; Torbenson, M.S.; Unalp-Arida, A.; et al. Design and Validation of a Histological Scoring System for Nonalcoholic Fatty Liver Disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef] [PubMed]
- Notarnicola, M.; Osella, A.R.; Caruso, M.G.; Pesole, P.L.; Lippolis, A.; Tutino, V.; Bonfiglio, C.; De Nunzio, V.; Scavo, M.P.; Mirizzi, A.; et al. Nonalcoholic Fatty Liver Disease: Focus on New Biomarkers and Lifestyle Interventions. Int. J. Mol. Sci. 2021, 22, 3899. [Google Scholar] [CrossRef]
- Sayiner, M.; Koenig, A.; Henry, L.; Younossi, Z.M. Epidemiology of Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis in the United States and the Rest of the World. Clin. Liver Dis. 2016, 20, 205–214. [Google Scholar] [CrossRef]
- Svegliati-Baroni, G.; Pierantonelli, I.; Torquato, P.; Marinelli, R.; Ferreri, C.; Chatgilialoglu, C.; Bartolini, D.; Galli, F. Lipidomic Biomarkers and Mechanisms of Lipotoxicity in Non-Alcoholic Fatty Liver Disease. Free Radic. Biol. Med. 2019, 144, 293–309. [Google Scholar] [CrossRef]
- Yang, S.Q.; Lin, H.Z.; Lane, M.D.; Clemens, M.; Diehl, A.M. Obesity Increases Sensitivity to Endotoxin Liver Injury: Implications for the Pathogenesis of Steatohepatitis. Proc. Natl. Acad. Sci. USA 1997, 94, 2557–2562. [Google Scholar] [CrossRef] [Green Version]
- Marra, F.; Svegliati-Baroni, G. Lipotoxicity and the Gut-Liver Axis in NASH Pathogenesis. J. Hepatol. 2018, 68, 280–295. [Google Scholar] [CrossRef]
- Almeda-Valdes, P.; Altamirano-Barrera, A.; Méndez-Sánchez, N. Insights in Non-Alcoholic Fatty Liver Disease Pathophysiology with Lipidomic Analyses. Ann. Hepatol. 2015, 14, 567–569. [Google Scholar] [CrossRef]
- Spahis, S.; Delvin, E.; Borys, J.-M.; Levy, E. Oxidative Stress as a Critical Factor in Nonalcoholic Fatty Liver Disease Pathogenesis. Antioxid. Redox Signal. 2017, 26, 519–541. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.-P.; Mao, X.-L.; Chen, Y.-H.; Yan, L.-L.; Ye, L.-P.; Li, S.-W. Reactive Oxygen Species Induce Fatty Liver and Ischemia-Reperfusion Injury by Promoting Inflammation and Cell Death. Front. Immunol. 2022, 13, 870239. [Google Scholar] [CrossRef] [PubMed]
- Reiniers, M.J.; van Golen, R.F.; van Gulik, T.M.; Heger, M. Reactive Oxygen and Nitrogen Species in Steatotic Hepatocytes: A Molecular Perspective on the Pathophysiology of Ischemia-Reperfusion Injury in the Fatty Liver. Antioxid. Redox Signal. 2014, 21, 1119–1142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Llacuna, L.; Fernández, A.; Montfort, C.V.; Matías, N.; Martínez, L.; Caballero, F.; Rimola, A.; Elena, M.; Morales, A.; Fernández-Checa, J.C.; et al. Targeting Cholesterol at Different Levels in the Mevalonate Pathway Protects Fatty Liver against Ischemia-Reperfusion Injury. J. Hepatol. 2011, 54, 1002–1010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poli, G.; Schaur, R.J.; Siems, W.G.; Leonarduzzi, G. 4-Hydroxynonenal: A Membrane Lipid Oxidation Product of Medicinal Interest. Med. Res. Rev. 2008, 28, 569–631. [Google Scholar] [CrossRef]
- Malaguarnera, L.; Madeddu, R.; Palio, E.; Arena, N.; Malaguarnera, M. Heme Oxygenase-1 Levels and Oxidative Stress-Related Parameters in Non-Alcoholic Fatty Liver Disease Patients. J. Hepatol. 2005, 42, 585–591. [Google Scholar] [CrossRef]
- Puri, P.; Baillie, R.A.; Wiest, M.M.; Mirshahi, F.; Choudhury, J.; Cheung, O.; Sargeant, C.; Contos, M.J.; Sanyal, A.J. A Lipidomic Analysis of Nonalcoholic Fatty Liver Disease. Hepatology 2007, 46, 1081–1090. [Google Scholar] [CrossRef]
- Pelusi, S.; Cespiati, A.; Rametta, R.; Pennisi, G.; Mannisto, V.; Rosso, C.; Baselli, G.; Dongiovanni, P.; Fracanzani, A.L.; Badiali, S.; et al. Prevalence and Risk Factors of Significant Fibrosis in Patients with Nonalcoholic Fatty Liver Without Steatohepatitis. Clin. Gastroenterol. Hepatol. 2019, 17, 2310–2319.e6. [Google Scholar] [CrossRef] [Green Version]
- Sanyal, A.J.; Shankar, S.S.; Calle, R.A.; Samir, A.E.; Sirlin, C.B.; Sherlock, S.P.; Loomba, R.; Fowler, K.J.; Dehn, C.A.; Heymann, H.; et al. Non-Invasive Biomarkers of Nonalcoholic Steatohepatitis: The FNIH NIMBLE Project. Nat. Med. 2022, 28, 430–432. [Google Scholar] [CrossRef]
- Mayo, R.; Crespo, J.; Martínez-Arranz, I.; Banales, J.M.; Arias, M.; Mincholé, I.; Aller de la Fuente, R.; Jimenez-Agüero, R.; Alonso, C.; de Luis, D.A.; et al. Metabolomic-Based Noninvasive Serum Test to Diagnose Nonalcoholic Steatohepatitis: Results from Discovery and Validation Cohorts. Hepatol. Commun. 2018, 2, 807–820. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, W.M.C.; Voelker, M.; Thiel, R.; Becka, M.; Burt, A.; Schuppan, D.; Hubscher, S.; Roskams, T.; Pinzani, M.; Arthur, M.J.P. Serum Markers Detect the Presence of Liver Fibrosis: A Cohort Study. Gastroenterology 2004, 127, 1704–1713. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| NASH Score < 4 (N = 82) | NASH Score ≥ 4 (N = 70) | p | |
|---|---|---|---|
| -Demographic | |||
| Age [years, median (IQR)] | 49 (18.50) | 51.50 (23) | 0.93 |
| Male [%(n)] | 69.5 (57) | 48.6 (34) | 0.009 |
| -Comorbidities, [%(n)] | |||
| Diabetes | 11.3 (7) | 28.6 (18) | 0.016 |
| Hypercholesterolemia | 49.4 (39) | 47.8 (33) | 0.85 |
| Hypertriglyceridemia | 34.2 (26) | 38.5 (25) | 0.60 |
| Obesity | 61.7 (50) | 68.6 (48) | 0.38 |
| -Liver biopsy, [%(n)] | |||
| Mild Steatosis (<33%) | 73.2 (60) | 12.9 (9) | <0.001 |
| Moderate/Severe Steatosis (≥33%) | 26.8 (22) | 87.1 (61) | <0.001 |
| NASH (Inflammation + Ballooning) | 20.7 (17) | 88.6 (62) | <0.001 |
| Advanced/Severe Fibrosis (≥F3) | 9.8 (8) | 25.7 (18) | 0.009 |
| Cirrhosis (F4) | 3.7 (3) | 11.4 (8) | 0.06 |
| -Laboratory measurements, [median (IQR)] | |||
| Height (m) | 1.67 (0.13) | 1.62 (0.17) | 0.09 |
| Weight (kg) | 86.3 (21.95) | 87.6 (29.35) | 0.88 |
| Body Index Mass (BMI) | 31.05 (36.91) | 32.30 (16.02) | 0.24 |
| Waist (cm) | 104 (19.50) | 105 (20.65) | 0.67 |
| Hip (cm) | 107 (16.38) | 108.25 (15.65) | 0.90 |
| Systolic Blood Pressure (mmHg) | 120 (35) | 140 (28.75) | <0.001 |
| Diastolic Blood Pressure (mmHg) | 75 (30) | 90 (16) | <0.001 |
| Fibroscan * (KPa) | 8.1 (6.4) | 10.35 (7.55) | 0.033 |
| AST (U/L) | 30 (17.50) | 41 (27) | <0.001 |
| ALT (U/L) | 52.50 (29) | 65 (51) | 0.002 |
| GGT (U/L) | 82.50 (97.25) | 68 (73) | 0.45 |
| HOMA-IR score | 3.42 (4.44) | 5.37 (5.08) | <0.001 |
| Total Cholesterol (mg/dL) | 183 (50) | 192 (59.25) | 0.58 |
| HDL Cholesterol (mg/dL) | 43.50 (12.15) | 46.70 (12.80) | 0.59 |
| LDL Cholesterol (mg/dL) | 106.60 (31.38) | 116 (51) | 0.49 |
| Triglycerides (mg/dL) | 134 (96.75) | 133 (99) | 0.62 |
| Glycaemia (mg/dL) | 103 (25) | 109 (32.50) | 0.011 |
| Creatinine (mg/dL) | 0.90 (0.28) | 0.80 (0.28) | 0.003 |
| Uric acid (mg/dL) | 5.90 (1.50) | 5.80 (2.03) | 0.55 |
| Total bilirubin (mg/dL) | 0.62 (0.50) | 0.60 (0.40) | 0.37 |
| Alkaline Phosphatase (ALP) | 72 (32.25) | 80 (32) | 0.039 |
| Leukocytes (cells/mL) | 6760 (5750) | 5745 (5170) | 0.28 |
| Platelet (cells/mL) | 254,000 (95,000) | 242,000 (122,250) | 0.35 |
| Ferritin (ng/mL) | 186 (164.20) | 174 (180.20) | 0.93 |
| Albumin (g/dL) | 4.60 (0.70) | 4.40 (0.70) | 0.005 |
| FLI score | 85.26 (84.03) | 81.37 (73.23) | 0.68 |
| HSI score | 42.07 (33.22) | 45.80 (28.73) | 0.033 |
| NFS | −3.59 (3.46) | −2.05 (2.92) | 0.005 |
| FIB4 score | 0.85 (0.64) | 1.06 (1.15) | 0.07 |
| HFS score | 0.019 (0.06) | 0.12 (0.36) | <0.001 |
| APRI score | −3.48 (6.72) | 0.33 (10.55) | 0.001 |
| NASH Score < 4 | NASH Score ≥ 4 | p | |
|---|---|---|---|
| SOD (U/mL) | 0.14 (0.06) | 0.13 (0.06) | 0.518 |
| Catalase (U/μL) | 42.40 (45.84) | 34.02 (39.65) | 0.384 |
| FRAP (μM) | 409.64 (110.65) | 392.71 (130.14) | 0.826 |
| ABTS (μM) | 548.43 (477.99) | 560.09 (556.05) | 0.496 |
| 8-OHdG (pg/mL) | 17710 (24974) | 19395 (33234) | 0.370 |
| MDA + HNE (μM) | 120.48 (280.61) | 230.14 (355.89) | 0.024 |
| OR | 95% CI | p | |
|---|---|---|---|
| HSI | 1.05 | 1.02–1.09 | <0.001 |
| FIB4 | 1.68 | 1.05–2.68 | 0.030 |
| APRI | 1.08 | 1.02–1.13 | 0.005 |
| LPO > 315.39 μM | 4.71 | 1.68–13.19 | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martín-Fernández, M.; Arroyo, V.; Carnicero, C.; Sigüenza, R.; Busta, R.; Mora, N.; Antolín, B.; Tamayo, E.; Aspichueta, P.; Carnicero-Frutos, I.; et al. Role of Oxidative Stress and Lipid Peroxidation in the Pathophysiology of NAFLD. Antioxidants 2022, 11, 2217. https://doi.org/10.3390/antiox11112217
Martín-Fernández M, Arroyo V, Carnicero C, Sigüenza R, Busta R, Mora N, Antolín B, Tamayo E, Aspichueta P, Carnicero-Frutos I, et al. Role of Oxidative Stress and Lipid Peroxidation in the Pathophysiology of NAFLD. Antioxidants. 2022; 11(11):2217. https://doi.org/10.3390/antiox11112217
Chicago/Turabian StyleMartín-Fernández, Marta, Víctor Arroyo, Carmen Carnicero, Rebeca Sigüenza, Reyes Busta, Natalia Mora, Beatriz Antolín, Eduardo Tamayo, Patricia Aspichueta, Irene Carnicero-Frutos, and et al. 2022. "Role of Oxidative Stress and Lipid Peroxidation in the Pathophysiology of NAFLD" Antioxidants 11, no. 11: 2217. https://doi.org/10.3390/antiox11112217
APA StyleMartín-Fernández, M., Arroyo, V., Carnicero, C., Sigüenza, R., Busta, R., Mora, N., Antolín, B., Tamayo, E., Aspichueta, P., Carnicero-Frutos, I., Gonzalo-Benito, H., & Aller, R. (2022). Role of Oxidative Stress and Lipid Peroxidation in the Pathophysiology of NAFLD. Antioxidants, 11(11), 2217. https://doi.org/10.3390/antiox11112217