

Longitudinal Coupling between Eating Disorder Psychopathology and Depression in Patients with Anorexia Nervosa and Bulimia Nervosa Treated with Enhanced Cognitive Behavior Therapy: A One-Year Follow-Up Study

 , , , , , ,
, , , , , ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Assessment
2.3. Treatment
2.4. Statistics
3. Results
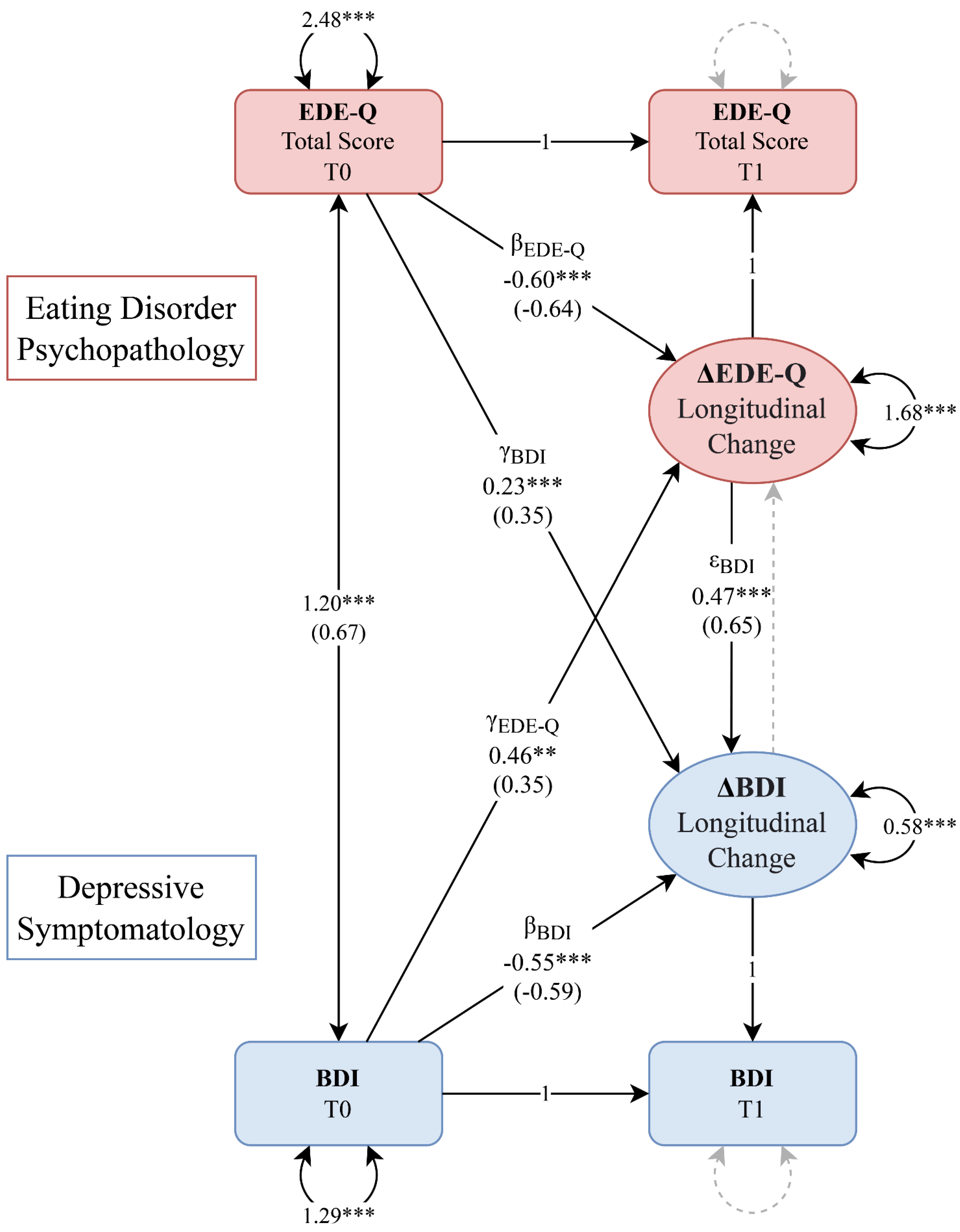
Structural Equation Model
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fairburn, C.G. Cognitive Behavior Therapy and Eating Disorders; Guilford Press: New York, NY, USA, 2008; ISBN 9781593857097. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013; ISBN 089042554X. [Google Scholar]
- Keski-Rahkonen, A.; Mustelin, L. Epidemiology of Eating Disorders in Europe. Curr. Opin. Psychiatry 2016, 29, 340–345. [Google Scholar] [CrossRef] [PubMed]
- Ulfvebrand, S.; Birgegård, A.; Norring, C.; Högdahl, L.; von Hausswolff-Juhlin, Y. Psychiatric Comorbidity in Women and Men with Eating Disorders Results from a Large Clinical Database. Psychiatry Res. 2015, 230, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Vall, E.; Wade, T.D. Predictors of Treatment Outcome in Individuals with Eating Disorders: A Systematic Review and Meta-Analysis. Int. J. Eat. Disord. 2015, 48, 946–971. [Google Scholar] [CrossRef] [PubMed]
- Berkman, N.D.; Lohr, K.N.; Bulik, C.M. Outcomes of Eating Disorders: A Systematic Review of the Literature. Int. J. Eat. Disord. 2007, 40, 293–309. [Google Scholar] [CrossRef] [PubMed]
- Löwe, B.; Zipfel, S.; Buchholz, C.; Dupont, Y.; Reas, D.L.; Herzog, W. Long-Term Outcome of Anorexia Nervosa in a Prospective 21-Year Follow-up Study. Psychol. Med. 2001, 31, 881–890. [Google Scholar] [CrossRef] [PubMed]
- Crow, S.J.; Peterson, C.B.; Swanson, S.A.; Raymond, N.C.; Specker, S.; Eckert, E.D.; Mitchell, J.E. Increased Mortality in Bulimia Nervosa and Other Eating Disorders. Am. J. Psychiatry 2009, 166, 1342–1346. [Google Scholar] [CrossRef]
- Forcano, L.; Fernández-Aranda, F.; Álvarez-Moya, E.; Bulik, C.; Granero, R.; Gratacòs, M.; Jiménez-Murcia, S.; Krug, I.; Mercader, J.M.; Riesco, N.; et al. Suicide Attempts in Bulimia Nervosa: Personality and Psychopathological Correlates. Eur. Psychiatry 2009, 24, 91–97. [Google Scholar] [CrossRef]
- Bulik, C.M.; Thornton, L.; Pinheiro, A.P.; Plotnicov, K.; Klump, K.L.; Brandt, H.; Crawford, S.; Fichter, M.M.; Halmi, K.A.; Johnson, C.; et al. Suicide Attempts in Anorexia Nervosa. Psychosom. Med. 2008, 70, 378–383. [Google Scholar] [CrossRef]
- Franko, D.L.; Keel, P.K.; Dorer, D.J.; Blais, M.A.; Delinsky, S.S.; Eddy, K.T.; Charat, V.; Renn, R.; Herzog, D.B. What Predicts Suicide Attempts in Women with Eating Disorders? Psychol. Med. 2004, 34, 843–853. [Google Scholar] [CrossRef]
- Castellini, G.; Lo Sauro, C.; Mannucci, E.; Ravaldi, C.; Rotella, C.M.; Faravelli, C.; Ricca, V. Diagnostic Crossover and Outcome Predictors in Eating Disorders According to DSM-IV and DSM-V Proposed Criteria: A 6-Year Follow-up Study. Psychosom. Med. 2011, 73, 270–279. [Google Scholar] [CrossRef]
- Monteleone, A.M.; Cascino, G. A Systematic Review of Network Analysis Studies in Eating Disorders: Is Time to Broaden the Core Psychopathology to Non Specific Symptoms. Eur. Eat. Disord. Rev. 2021, 29, 531–547. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.E.; Mason, T.B.; Crosby, R.D.; Cao, L.; Leonard, R.C.; Wetterneck, C.T.; Smith, B.E.R.; Farrell, N.R.; Riemann, B.C.; Wonderlich, S.A.; et al. A Comparative Network Analysis of Eating Disorder Psychopathology and Co-Occurring Depression and Anxiety Symptoms before and after Treatment. Psychol. Med. 2019, 49, 314–324. [Google Scholar] [CrossRef] [PubMed]
- Voderholzer, U.; Hessler-Kaufmann, J.B.; Lustig, L.; Läge, D. Comparing Severity and Qualitative Facets of Depression between Eating Disorders and Depressive Disorders: Analysis of Routine Data. J. Affect. Disord. 2019, 257, 758–764. [Google Scholar] [CrossRef] [PubMed]
- Bulik, C.M. Anxiety, Depression and Eating Disorders. In Eating Disorders and Obesity: A Comprehensive Handbook; Guilford Press: New York, NY, USA, 2002; pp. 193–198. [Google Scholar]
- Brietzke, E.; Moreira, C.L.R.; Toniolo, R.A.; Lafer, B. Clinical Correlates of Eating Disorder Comorbidity in Women with Bipolar Disorder Type I. J. Affect. Disord. 2011, 130, 162–165. [Google Scholar] [CrossRef]
- Tseng, M.C.M.; Chang, C.H.; Chen, K.Y.; Liao, S.C.; Chen, H.C. Prevalence and Correlates of Bipolar Disorders in Patients with Eating Disorders. J. Affect. Disord. 2016, 190, 599–606. [Google Scholar] [CrossRef]
- McElroy, S.L.; Kotwal, R.; Keck, P.E.; Akiskal, H.S. Comorbidity of Bipolar and Eating Disorders: Distinct or Related Disorders with Shared Dysregulations? J. Affect. Disord. 2005, 86, 107–127. [Google Scholar] [CrossRef]
- de Almeida, J.R.C.; Phillips, M.L. Distinguishing between Unipolar Depression and Bipolar Depression: Current and Future Clinical and Neuroimaging Perspectives. Biol. Psychiatry 2013, 73, 111–118. [Google Scholar] [CrossRef]
- Rodgers, R.F.; DuBois, R.; Thiebaut, S.; Jaussent, I.; Maimoun, L.; Seneque, M.; Lefebvre, P.; Renard, E.; Courtet, P.; Guillaume, S. Structural Differences in Eating Disorder Psychopathology after History of Childhood Abuse: Insights from a Bayesian Network Analysis. J. Abnorm. Psychol. 2019, 128, 795–805. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence Eating Disorders: Recognition and Treatment (NICE Guideline [NG69]). Available online: https://www.nice.org.uk/guidance/ng69 (accessed on 15 October 2021).
- Cassioli, E.; Sensi, C.; Mannucci, E.; Ricca, V.; Rotella, F. Pharmacological Treatment of Acute-Phase Anorexia Nervosa: Evidence from Randomized Controlled Trials. J. Psychopharmacol. 2020, 34, 864–873. [Google Scholar] [CrossRef]
- Mischoulon, D.; Eddy, K.T.; Keshaviah, A.; Dinescu, D.; Ross, S.L.; Kass, A.E.; Franko, D.L.; Herzog, D.B. Depression and Eating Disorders: Treatment and Course. J. Affect. Disord. 2011, 130, 470–477. [Google Scholar] [CrossRef]
- Garner, D.M. Pathogenesis of Anorexia Nervosa. Lancet 1993, 341, 1631–1635. [Google Scholar] [CrossRef] [PubMed]
- Mattar, L.; Thiébaud, M.-R.; Huas, C.; Cebula, C.; Godart, N. Depression, Anxiety and Obsessive–Compulsive Symptoms in Relation to Nutritional Status and Outcome in Severe Anorexia Nervosa. Psychiatry Res. 2012, 200, 513–517. [Google Scholar] [CrossRef] [PubMed]
- Calugi, S.; El Ghoch, M.; Conti, M.; Dalle Grave, R. Depression and Treatment Outcome in Anorexia Nervosa. Psychiatry Res. 2014, 218, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Santini, Z.I.; Koyanagi, A.; Tyrovolas, S.; Mason, C.; Haro, J.M. The Association between Social Relationships and Depression: A Systematic Review. J. Affect. Disord. 2015, 175, 53–65. [Google Scholar] [CrossRef]
- Leigh-Hunt, N.; Bagguley, D.; Bash, K.; Turner, V.; Turnbull, S.; Valtorta, N.; Caan, W. An Overview of Systematic Reviews on the Public Health Consequences of Social Isolation and Loneliness. Public Health 2017, 152, 157–171. [Google Scholar] [CrossRef]
- Rossi, E.; Castellini, G.; Cassioli, E.; Sensi, C.; Mancini, M.; Stanghellini, G.; Ricca, V. The Role of Embodiment in the Treatment of Patients with Anorexia and Bulimia Nervosa: A 2-Year Follow-up Study Proposing an Integration between Enhanced Cognitive Behavioural Therapy and a Phenomenological Model of Eating Disorders. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2021, 1, 3. [Google Scholar] [CrossRef]
- Bardone-Cone, A.M.; Harney, M.B.; Maldonado, C.R.; Lawson, M.A.; Robinson, D.P.; Smith, R.; Tosh, A. Defining Recovery from an Eating Disorder: Conceptualization, Validation, and Examination of Psychosocial Functioning and Psychiatric Comorbidity. Behav. Res. Ther. 2010, 48, 194–202. [Google Scholar] [CrossRef]
- Junne, F.; Zipfel, S.; Martus, P.; Giel, K.; Resmark, G.; Teufel, M.; Dinkel, A.; Burgmer, M.; Rothermund, E.; Ziser, K.; et al. The Relationship of Body Image with Symptoms of Depression and Anxiety in Patients with Anorexia Nervosa during Outpatient Psychotherapy: Results of the ANTOP Study. Psychotherapy 2016, 53, 141–151. [Google Scholar] [CrossRef]
- Jones, H.; McIntosh, V.V.W.; Britt, E.; Carter, J.D.; Jordan, J.; Bulik, C.M. The Effect of Temperament and Character on Body Dissatisfaction in Women with Bulimia Nervosa: The Role of Low Self-Esteem and Depression. Eur. Eat. Disord. Rev. 2022, 30, 388–400. [Google Scholar] [CrossRef]
- Junne, F.; Wild, B.; Resmark, G.; Giel, K.E.; Teufel, M.; Martus, P.; Ziser, K.; Friederich, H.; Zwaan, M.; Löwe, B.; et al. The Importance of Body Image Disturbances for the Outcome of Outpatient Psychotherapy in Patients with Anorexia Nervosa: Results of the ANTOP-study. Eur. Eat. Disord. Rev. 2019, 27, 49–58. [Google Scholar] [CrossRef]
- First, M.B.; Williams, J.B.W.; Karg, R.S.; Spitzer, R.L. Structured Clinical Interview for DSM-5 Disorders, Clinician Version (SCID-5-CV); American Psychiatric Association: Arlington, VA, USA, 2016. [Google Scholar]
- World Health Organization. Child Maltreatment. Available online: https://www.who.int/news-room/fact-sheets/detail/child-maltreatment (accessed on 21 April 2022).
- Bernstein, D.P.; Stein, J.A.; Newcomb, M.D.; Walker, E.; Pogge, D.; Ahluvalia, T.; Stokes, J.; Handelsman, L.; Medrano, M.; Desmond, D.; et al. Development and Validation of a Brief Screening Version of the Childhood Trauma Questionnaire. Child Abus. Negl. 2003, 27, 169–190. [Google Scholar] [CrossRef] [PubMed]
- Calugi, S.; Milanese, C.; Sartirana, M.; el Ghoch, M.; Sartori, F.; Geccherle, E.; Coppini, A.; Franchini, C.; Dalle Grave, R. The Eating Disorder Examination Questionnaire: Reliability and Validity of the Italian Version. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2016, 22, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Rø, Ø.; Reas, D.L.; Stedal, K. Eating Disorder Examination Questionnaire (EDE-Q) in Norwegian Adults: Discrimination between Female Controls and Eating Disorder Patients. Eur. Eat. Disord. Rev. 2015, 23, 408–412. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory-II; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Sica, C.; Ghisi, M. The Italian Versions of the Beck Anxiety Inventory and the Beck Depression Inventory: II. Psychometric Properties and Discriminant Power. In Leading-Edge Psychological Tests and Testing Research; Lange, A.M., Ed.; Nova Science Publishers: Hauppauge, NY, USA, 2007. [Google Scholar]
- Derogatis, L.R. Symptom Checklist-90-R: Administration, Scoring, and Procedures Manual; Clinical Psychometric Research: Towson, MD, USA, 1994. [Google Scholar]
- Prunas, A.; Sarno, I.; Preti, E.; Madeddu, F.; Perugini, M. Psychometric Properties of the Italian Version of the SCL-90-R: A Study on a Large Community Sample. Eur. Psychiatry 2012, 27, 591–597. [Google Scholar] [CrossRef] [PubMed]
- American Psychological Association. Clinical Practice Guideline for the Treatment of Depression across Three Age Cohorts. Available online: https://www.apa.org/depression-guideline (accessed on 22 April 2022).
- McArdle, J.J. Latent Variable Modeling of Differences and Changes with Longitudinal Data. Annu. Rev. Psychol. 2009, 60, 577–605. [Google Scholar] [CrossRef] [PubMed]
- Grimm, K.J.; Ram, N.; Estabrook, R. Growth Modeling: Structural Equation and Multilevel Modeling Approaches; The Guilford Press: New York, NY, USA, 2016; ISBN 9781462526062. [Google Scholar]
- Enders, C.; Bandalos, D. The Relative Performance of Full Information Maximum Likelihood Estimation for Missing Data in Structural Equation Models. Struct. Equ. Model. Multidiscip. J. 2001, 8, 430–457. [Google Scholar] [CrossRef]
- Schreiber, J.B.; Stage, F.K.; King, J.; Nora, A.; Barlow, E.A. Reporting Structural Equation Modeling and Confirmatory Factor Analysis Results: A Review. J. Educ. Res. 2006, 99, 323–338. [Google Scholar] [CrossRef]
- Claeskens, G.; Hjort, N.L. Model Selection and Model Averaging; Cambridge University Press: Cambridge, UK, 2008. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Wickham, H.; François, R.; Henry, L.; Müller, K. Dplyr: A Grammar of Data Manipulation. Available online: https://cran.r-project.org/package=dplyr (accessed on 1 March 2023).
- Rosseel, Y. Lavaan: An R Package for Structural Equation Modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef]
- Pinheiro, J.; Bates, D.; DebRoy, S.; Sarkar, D.; R Core Team. nlme: Linear and Nonlinear Mixed Effects Models. Available online: https://cran.r-project.org/package=nlme (accessed on 1 March 2023).
- Atwood, M.E.; Friedman, A. A Systematic Review of Enhanced Cognitive Behavioral Therapy (CBT-E) for Eating Disorders. Int. J. Eat. Disord. 2020, 53, 311–330. [Google Scholar] [CrossRef]
- Cassioli, E.; Rossi, E.; D’Anna, G.; Martelli, M.; Hazzard, V.M.; Crosby, R.D.; Wonderlich, S.A.; Ricca, V.; Castellini, G. A 1-year Follow-up Study of the Longitudinal Interplay between Emotion Dysregulation and Childhood Trauma in the Treatment of Anorexia Nervosa. Int. J. Eat. Disord. 2022, 55, 98–107. [Google Scholar] [CrossRef]
- Signorini, R.; Sheffield, J.; Rhodes, N.; Fleming, C.; Ward, W. The Effectiveness of Enhanced Cognitive Behavioural Therapy (CBT-E): A Naturalistic Study within an Out-Patient Eating Disorder Service. Behav. Cogn. Psychother. 2018, 46, 21–34. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, D.J.; Wilson, M.G.; Ascroft, R.C.; Al-Banna, M. Effectiveness of Fluoxetine Therapy in Bulimia Nervosa Regardless of Comorbid Depression. Int. J. Eat. Disord. 1999, 25, 19–27. [Google Scholar] [CrossRef]
- Bacaltchuk, J.; Hay, P.; Mari, J.J. Antidepressants Versus Placebo for the Treatment of Bulimia Nervosa: A Systematic Review. Aust. N. Z. J. Psychiatry 2000, 34, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Kohn, M.R.; Ashtari, M.; Golden, N.H.; Schebendach, J.; Patel, M.; Jacobson, M.S.; Shenker, I.R. Structural Brain Changes and Malnutrition in Anorexia Nervosa. Ann. N. Y. Acad. Sci. 1997, 817, 398–399. [Google Scholar] [CrossRef]
- Collantoni, E.; Meneguzzo, P.; Tenconi, E.; Meregalli, V.; Manara, R.; Favaro, A. Shift Toward Randomness in Brain Networks of Patients With Anorexia Nervosa: The Role of Malnutrition. Front. Neurosci. 2021, 15, 210. [Google Scholar] [CrossRef]
- Gauthier, C.; Hassler, C.; Mattar, L.; Launay, J.-M.; Callebert, J.; Steiger, H.; Melchior, J.-C.; Falissard, B.; Berthoz, S.; Mourier-Soleillant, V.; et al. Symptoms of Depression and Anxiety in Anorexia Nervosa: Links with Plasma Tryptophan and Serotonin Metabolism. Psychoneuroendocrinology 2014, 39, 170–178. [Google Scholar] [CrossRef]
- Cuthbert, B.N.; Insel, T.R. Toward the Future of Psychiatric Diagnosis: The Seven Pillars of RDoC. BMC Med. 2013, 11, 126. [Google Scholar] [CrossRef]
- Kotov, R.; Krueger, R.F.; Watson, D.; Achenbach, T.M.; Althoff, R.R.; Bagby, R.M.; Brown, T.A.; Carpenter, W.T.; Caspi, A.; Clark, L.A.; et al. The Hierarchical Taxonomy of Psychopathology (HiTOP): A Dimensional Alternative to Traditional Nosologies. J. Abnorm. Psychol. 2017, 126, 454–477. [Google Scholar] [CrossRef]
- Castellini, G.; Lelli, L.; Cassioli, E.; Ciampi, E.; Zamponi, F.; Campone, B.; Monteleone, A.M.; Ricca, V. Different Outcomes, Psychopathological Features, and Comorbidities in Patients with Eating Disorders Reporting Childhood Abuse: A 3-Year Follow-up Study. Eur. Eat. Disord. Rev. 2018, 26, 217–229. [Google Scholar] [CrossRef]
- Castellini, G.; Rossi, E.; Cassioli, E.; Giardinelli, L.; Fanelli, A.; Fisher, A.D.; Vignozzi, L.; Ricca, V. Predictors of Resumption of Menses in Anorexia Nervosa. Psychosom. Med. 2020, 82, 782–786. [Google Scholar] [CrossRef]
- Castellini, G.; D’Anna, G.; Rossi, E.; Cassioli, E.; Appignanesi, C.; Monteleone, A.M.; Rellini, A.H.; Ricca, V. Dysregulated Sexuality in Women with Eating Disorders: The Role of Childhood Traumatic Experiences. J. Sex Marital 2020, 46, 793–806. [Google Scholar] [CrossRef] [PubMed]
- Rossi, E.; Cassioli, E.; Gironi, V.; Idrizaj, E.; Garella, R.; Squecco, R.; Baccari, M.C.; Maggi, M.; Vignozzi, L.; Comeglio, P.; et al. Ghrelin as a Possible Biomarker and Maintaining Factor in Patients with Eating Disorders Reporting Childhood Traumatic Experiences. Eur. Eat. Disord. Rev. 2021, 29, 588–599. [Google Scholar] [CrossRef] [PubMed]
- Monteleone, A.M.; Cascino, G.; Ruzzi, V.; Pellegrino, F.; Patriciello, G.; Barone, E.; Carfagno, M.; Monteleone, P.; Maj, M. Emotional Traumatic Experiences Significantly Contribute to Identify a Maltreated Ecophenotype Sub-group in Eating Disorders: Experimental Evidence. Eur. Eat. Disord. Rev. 2021, 29, 269–280. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Baseline T0 (n = 157) | Follow-Up T1 (n = 121) | Time Effect (b) | |
|---|---|---|---|
| Age (years) | 25.52 ± 9.94 | - | |
| Education (years) | 12.88 ± 2.98 | - | |
| Age of onset (years) | 17.72 ± 5.19 | - | |
| BMI (kg/m2) | 19.33 ± 5.63 | 19.62 ± 4.63 | 0.62 * |
| EDE-Q Restraint | 3.45 ± 1.87 | 2.25 ± 1.78 | −1.31 *** |
| EDE-Q Eating Concern | 2.97 ± 1.61 | 1.93 ± 1.60 | −1.08 *** |
| EDE-Q Weight Concern | 3.41 ± 1.72 | 2.63 ± 1.89 | −0.84 *** |
| EDE-Q Shape Concern | 3.87 ± 1.78 | 3.07 ± 1.94 | −0.86 *** |
| EDE-Q Total Score | 3.43 ± 1.58 | 2.47 ± 1.68 | −1.03 *** |
| BDI | 22.78 ± 11.41 | 13.85 ± 12.23 | −9.28 *** |
| SCL-90-R GSI | 1.52 ± 0.75 | 1.09 ± 0.77 | −0.45 *** |
| Model | χ2 | DF | BIC | CFI | TLI | RMSEA | SRMR | Δχ2 | Model |
|---|---|---|---|---|---|---|---|---|---|
| Final model | 1.15 | 2 | 1711.43 | 1.00 | 1.01 | 0.000 | 0.033 | - | Final model |
| Unconstrained models | |||||||||
| 1→ΔEDE-Q | αEDE-Q ≠ 0 | 0.86 | 1 | 1716.32 | 1.00 | 1.00 | 0.000 | 0.020 | 0.26 |
| 1→ΔBDI | αBDI ≠ 0 | 0.26 | 1 | 1715.89 | 1.00 | 1.01 | 0.000 | 0.017 | 0.86 |
| ΔBDI→ΔEDE-Q | εEDE-Q ≠ 0 | 0.58 | 1 | 1716.49 | 1.00 | 1.01 | 0.000 | 0.033 | 0.00 |
| Constrained models | |||||||||
| EDE-QT0⇻ΔEDE-Q | βEDE-Q = 0 | 40.50 *** | 3 | 1739.12 | 0.88 | 0.76 | 0.257 | 0.139 | 28.12 *** |
| BDIT0⇻ΔBDI | βBDI = 0 | 52.15 *** | 3 | 1740.62 | 0.87 | 0.75 | 0.265 | 0.114 | 49.18 *** |
| BDIT0⇻ΔEDE-Q | γEDE-Q = 0 | 12.45 ** | 3 | 1716.14 | 0.97 | 0.94 | 0.130 | 0.066 | 8.02 ** |
| EDE-QT0⇻ΔBDI | γBDI = 0 | 18.62 *** | 3 | 1718.48 | 0.96 | 0.92 | 0.151 | 0.052 | 16.02 *** |
| ΔEDE-Q⇻ΔBDI | εBDI = 0 | 73.94 *** | 3 | 1765.78 | 0.78 | 0.55 | 0.350 | 0.117 | 52.85 *** |
| cov(EDE-Q T0, BDI T0) = 0 | 102.78 *** | 3 | 1799.41 | 0.65 | 0.30 | 0.440 | 0.248 | 65.49 *** | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cassioli, E.; Rossi, E.; Martelli, M.; Arganini, F.; Giuranno, G.; Siviglia, S.; Tarchi, L.; Faldi, M.; Castellini, G.; Ricca, V. Longitudinal Coupling between Eating Disorder Psychopathology and Depression in Patients with Anorexia Nervosa and Bulimia Nervosa Treated with Enhanced Cognitive Behavior Therapy: A One-Year Follow-Up Study. Brain Sci. 2023, 13, 535. https://doi.org/10.3390/brainsci13040535
Cassioli E, Rossi E, Martelli M, Arganini F, Giuranno G, Siviglia S, Tarchi L, Faldi M, Castellini G, Ricca V. Longitudinal Coupling between Eating Disorder Psychopathology and Depression in Patients with Anorexia Nervosa and Bulimia Nervosa Treated with Enhanced Cognitive Behavior Therapy: A One-Year Follow-Up Study. Brain Sciences. 2023; 13(4):535. https://doi.org/10.3390/brainsci13040535
Chicago/Turabian StyleCassioli, Emanuele, Eleonora Rossi, Michela Martelli, Francesca Arganini, Gabriele Giuranno, Serena Siviglia, Livio Tarchi, Marco Faldi, Giovanni Castellini, and Valdo Ricca. 2023. "Longitudinal Coupling between Eating Disorder Psychopathology and Depression in Patients with Anorexia Nervosa and Bulimia Nervosa Treated with Enhanced Cognitive Behavior Therapy: A One-Year Follow-Up Study" Brain Sciences 13, no. 4: 535. https://doi.org/10.3390/brainsci13040535
APA StyleCassioli, E., Rossi, E., Martelli, M., Arganini, F., Giuranno, G., Siviglia, S., Tarchi, L., Faldi, M., Castellini, G., & Ricca, V. (2023). Longitudinal Coupling between Eating Disorder Psychopathology and Depression in Patients with Anorexia Nervosa and Bulimia Nervosa Treated with Enhanced Cognitive Behavior Therapy: A One-Year Follow-Up Study. Brain Sciences, 13(4), 535. https://doi.org/10.3390/brainsci13040535