

Efficacy of Transcranial Direct Current Stimulation (tDCS) on Cognition, Anxiety, and Mobility in Community-Dwelling Older Individuals: A Controlled Clinical Trial
 , , , ,
, , , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
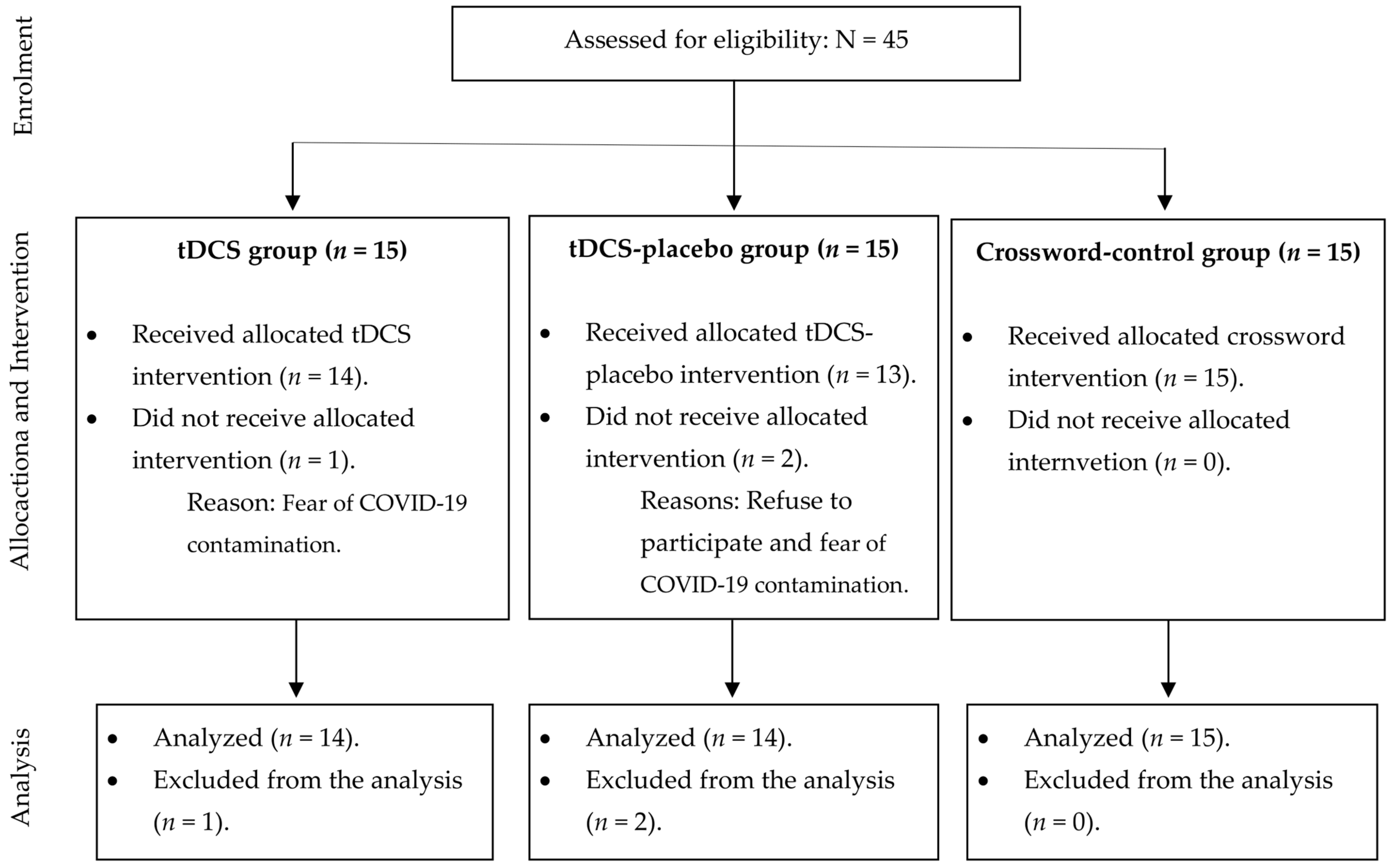
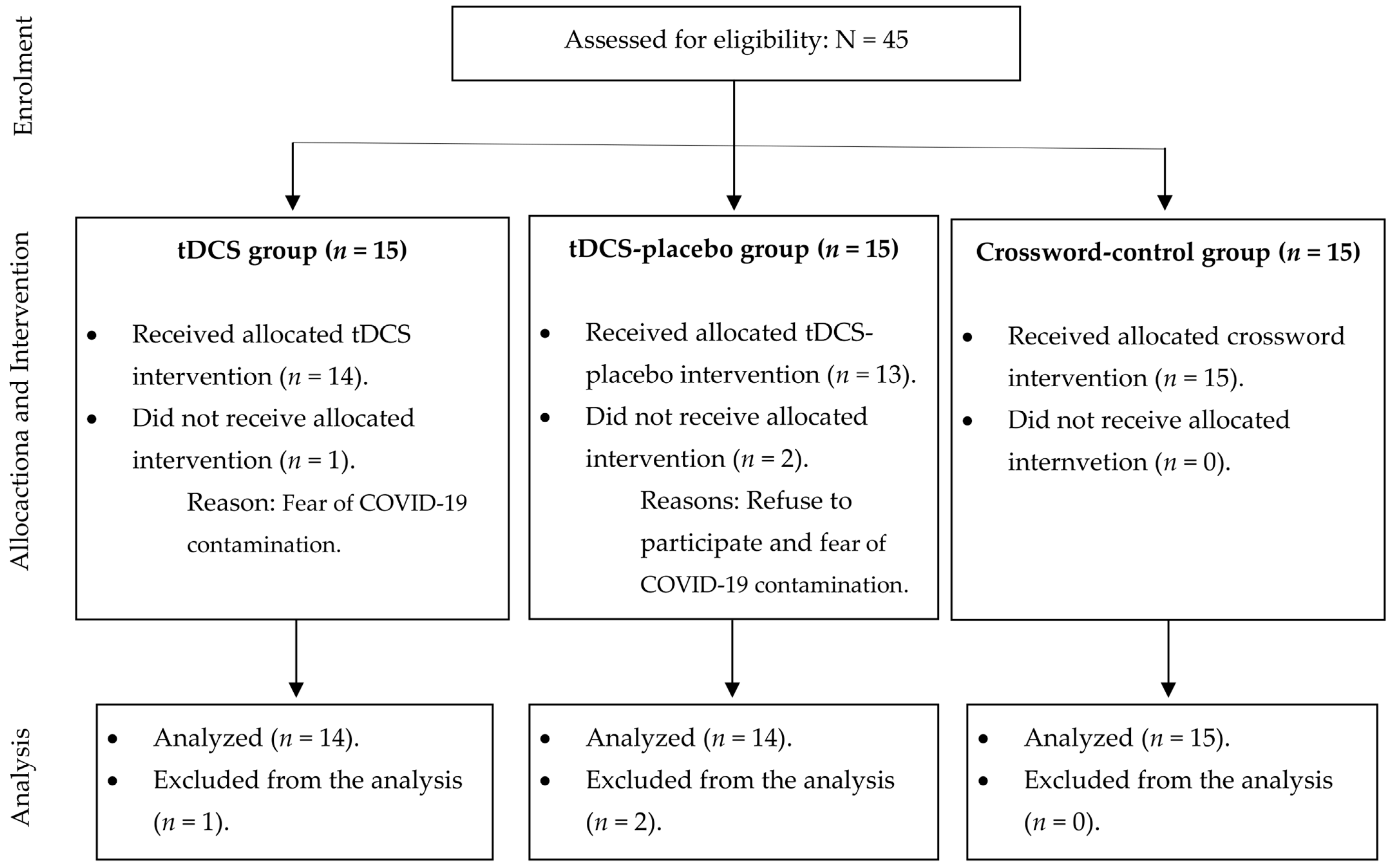
2.1. Sample Size, Blinding, and Randomization
2.2. Outcomes
2.3. tDCS Protocol
2.4. Statistical Analysis
3. Results
3.1. Efficacy of tDCS on Cognition
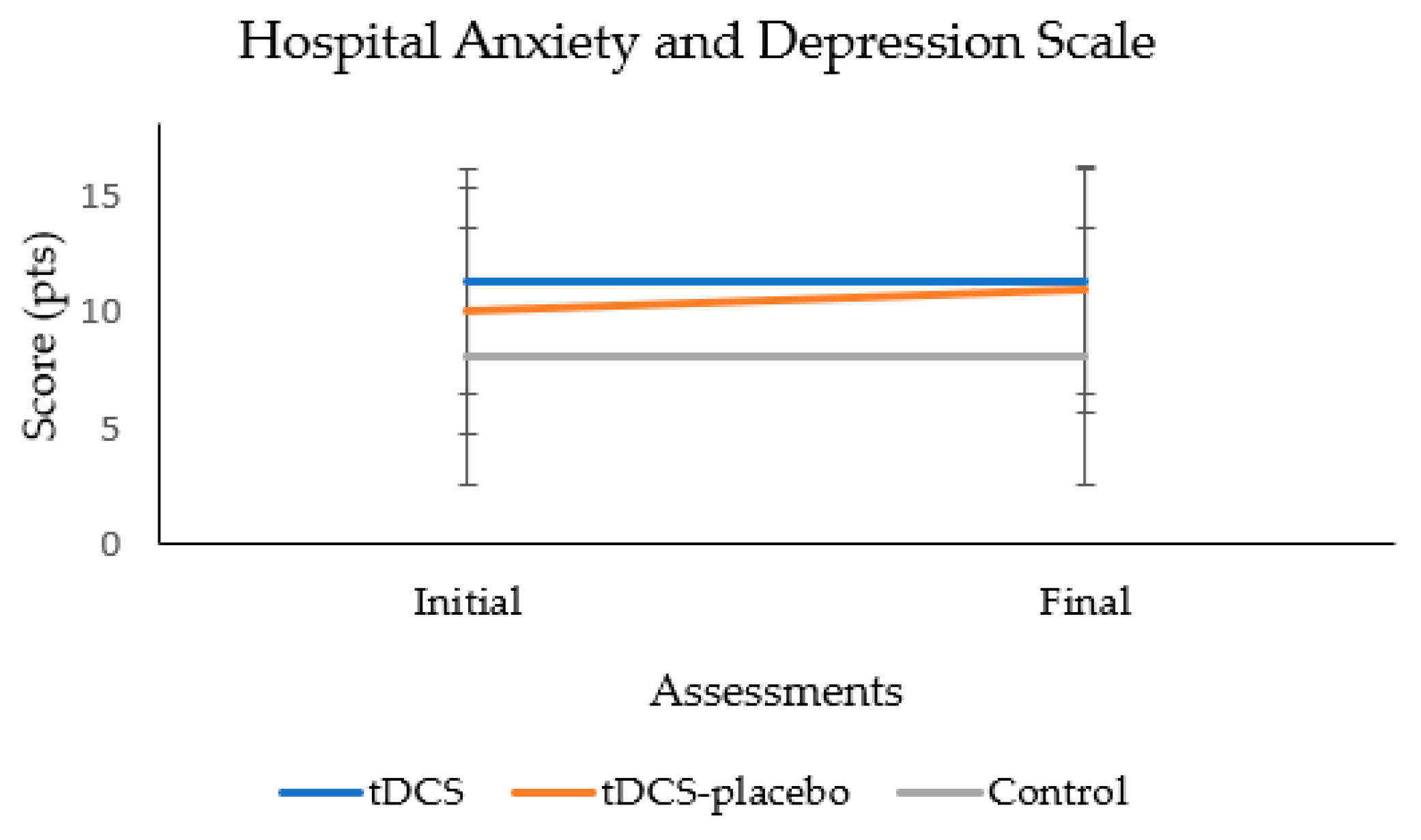
3.2. Efficacy of tDCS on Anxiety
3.3. Efficacy of tDCS on Mobility
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harada, C.N.; Natelson Love, M.C.; Triebel, K.L. Normal cognitive aging. Clin. Geriatr. Med. 2013, 29, 737–752. [Google Scholar] [CrossRef]
- Jayakody, O.; Breslin, M.; Ayers, E.; Verghese, J.; Barzilai, N.; Milman, S.; Weiss, E.; Blumen, H.M.N. Relative trajectories of gait and cognitive decline in aging. J. Gerontol. A Biol. Sci. Med. Sci. 2022, 77, 1230–1238. [Google Scholar] [CrossRef]
- Cruz-Jimenez, M. Normal changes in gait and mobility problems in the elderly. Phys. Med. Rehabil. Clin. N. Am. 2017, 28, 713–725. [Google Scholar] [CrossRef]
- Klimova, B.; Valis, M.; Kuca, K. Cognitive decline in normal aging and its prevention: A review on non-pharmacological lifestyle strategies. Clin. Interv. Aging 2017, 12, 903–910. [Google Scholar] [CrossRef]
- Norouzi, E.; Vaezmosavi, M.; Gerber, M.; Pühse, U.; Brand, S. Dual-task training on cognition and resistance training improved both balance and working memory in older people. Phys. Sportsmed. 2019, 47, 471–478. [Google Scholar] [CrossRef]
- Lo, O.Y.; van Donkelaar, P.; Chou, L.S. Effects of transcranial direct current stimulation over right posterior parietal cortex on attention function in healthy young adults. Eur. J. Neurosci. 2019, 49, 1623–1631. [Google Scholar] [CrossRef]
- Elsner, B.; Kwakkel, G.; Kugler, J.; Mehrholz, J. Transcranial direct current stimulation (tDCS) for improving capacity in activities and arm function after stroke: A network meta-analysis of randomised controlled trials. J. Neuroeng. Rehabil. 2017, 14, 95. [Google Scholar] [CrossRef]
- Begemann, M.J.; Brand, B.A.; Ćurčić-Blake, B.; Aleman, A.; Sommer, I.E. Efficacy of non-invasive brain stimulation on cognitive functioning in brain disorders: A meta-analysis. Psychol. Med. 2020, 50, 2465–2486. [Google Scholar] [CrossRef]
- Emonson, M.R.L.; Fitzgerald, P.B.; Rogasch, N.C.; Hoy, K.E. Neurobiological effects of transcranial direct current stimulation in younger adults, older adults and mild cognitive impairment. Neuropsychologia 2019, 125, 51–61. [Google Scholar] [CrossRef]
- Guo, Z.; Bao, D.; Manor, B.; Zhou, J. The effects of transcranial direct current stimulation (tDCS) on balance control in older adults: A systematic review and meta-analysis. Front. Aging. Neurosci. 2020, 12, 275. [Google Scholar] [CrossRef]
- Chase, H.W.; Boudewyn, M.A.; Carter, C.S.; Phillips, M.L. Transcranial direct current stimulation: A roadmap for research, from mechanism of action to clinical implementation. Mol. Psychiatry 2020, 25, 397–407. [Google Scholar] [CrossRef]
- Tononi, G.; Sporns, O.; Edelman, G.M. Measures of degeneracy and redundancy in biological networks. Proc. Natl. Acad. Sci. USA 1999, 96, 3257–3262. [Google Scholar] [CrossRef]
- Baharlouei, H.; Saba, M.A.; Yazdi, M.J.S.; Jaberzadeh, S. The effect of transcranial direct current stimulation on balance in healthy young and older adults: A systematic review of the literature. Neurophysiol. Clin. 2020, 50, 119–131. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Brucki, S.M.; Nitrini, R.; Caramelli, P.; Bertolucci, P.H.F.; Okamoto, I.H. Suggestions for utilization of the mini-mental state examination in Brazil. Arq. Neuropsiquiatr. 2003, 61, 777–781. [Google Scholar] [CrossRef]
- Hsu, W.Y.; Ku, Y.; Zanto, T.P.; Gazzaley, A. Effects of noninvasive brain stimulation on cognitive function in healthy aging and Alzheimer’s disease: A systematic review and meta-analysis. Neurobiol. Aging. 2015, 36, 2348–2359. [Google Scholar] [CrossRef]
- Efird, J. Blocked randomization with randomly selected block sizes. Int. J. Environ. Res. Public. Health 2011, 8, 15–20. [Google Scholar] [CrossRef]
- Pfeffer, R.I.; Kurosaki, T.T.; Harrah, C.H., Jr.; Chance, J.M.; Filos, S. Measurement of functional activities in older adults in the community. J. Gerontol. 1982, 37, 323–329. [Google Scholar] [CrossRef]
- Dubois, B.; Slachevsky, A.; Litvan, I.; Pillon, B. The FAB: A Frontal Assessment Battery at bedside. Neurology 2000, 55, 1621–1626. [Google Scholar] [CrossRef]
- Lezak, M.D. Neuropsychological Assessment, 3rd ed.; Oxford University Press: Oxford, UK, 1995. [Google Scholar]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Gandiga, P.C.; Hummel, F.C.; Coehn, L.G. Transcranial DC stimulation (tDCS): A tool for double-blind sham-controlled clinical studies in brain stimulation. Clin. Neurophysiol. 2006, 117, 845–850. [Google Scholar] [CrossRef]
- Vonk, J.M.J.; Higby, E.; Nikolaev, A.; Cahana-Amitay, D.; Spiro, A.; Albert, M.L.; Pbler, L.K. Demographic effects on longitudinal semantic processing, working memory, and cognitive speed. J. Gerontol. B. Psychol. Sci. Soc. Sci. 2020, 75, 1850–1862. [Google Scholar] [CrossRef]
- Idowu, M.I.; Szameitat, A.J. Executive function abilities in cognitively healthy young and older adults-A cross-sectional study. Front. Aging Neurosci. 2023, 15, 976915. [Google Scholar] [CrossRef]
- Li, Q.; Fu, Y.; Liu, C.; Meng, Z. Transcranial direct current stimulation of the dorsolateral prefrontal cortex for treatment of neuropsychiatric disorders. Front. Behav. Neurosci. 2022, 16, 893955. [Google Scholar] [CrossRef]
- Lee, J.H.; Lee, T.L.; Kang, N. Transcranial direct current stimulation decreased cognition-related reaction time in older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2021, 70, 101377. [Google Scholar] [CrossRef]
- Indahlastari, A.; Hardcastle, C.; Albizu, A.; Alvarez-Alvarado, S.; Boutzoukasm, E.M.; Evangelista, N.S.; Hausman, H.K.; Kraft, J.; Langer, K.; Woods, A.J. A systematic review and meta-analysis of transcranial direct current stimulation to remediate age-related cognitive decline in healthy older adults. Neuropsychiatr. Dis. Treat. 2021, 17, 971–990. [Google Scholar] [CrossRef]
- Meléndez, J.C.; Satorres, E.; Pitarque, A.; Delhom, I.; Real, E.; Escudero, J. Effectiveness of tDCS at improving recognition and reducing false memories in older adults. Int. J. Environ. Res. Public Health 2021, 18, 1317. [Google Scholar] [CrossRef]
- Furubayashi, T.; Terao, Y.; Arai, N.; Okabe, S.; Mochizuki, H.; Hanajima, R.; Hamada, M.; Yugeta, A.; Inomata-Terada, S.; Ugawa, Y. Short and long duration transcranial direct current stimulation (tDCS) over the human hand motor area. Exp. Brain Res. 2008, 185, 279–286. [Google Scholar] [CrossRef]
- Loo, C.K.; Husain, M.M.; McDonald, W.M.; Aaronson, S.; O’Reardon, J.P.; Alonzo, A.; Shannon Weickert, C.; Martin, D.M.; McClintock, S.M.; Mohan, A.; et al. International randomized-controlled trial of transcranial direct current stimulation in depression. Brain Stimul. 2018, 11, 125–133. [Google Scholar] [CrossRef]
- Chen, J.; Wang, Z.; Chen, Q.; Fu, Y.; Zheng, K. Transcranial direct current stimulation enhances cognitive function in patients with mild cognitive impairment and early/mid Alzheimer’s disease: A systematic review and meta-analysis. Brain Sci. 2022, 12, 562. [Google Scholar] [CrossRef]
- Alonzo, A.; Brassil, J.; Taylor, J.L.; Martin, D.; Loo, C.K. Daily transcranial direct current stimulation (tDCS) leads to greater increases in cortical excitability than second daily transcranial direct current stimulation. Brain Stimul. 2012, 5, 208–213. [Google Scholar] [CrossRef]
- Teselink, J.; Bawa, K.K.; Koo Ky, G.; Sankhe, K.; Liu, C.S.; Rapoport, M.; Ph, P.; Marzolini, S.; Gallagher, D.; Swardfager, W.; et al. Efficacy of non-invasive brain stimulation on global cognition and neuropsychiatric symptoms in Alzheimer’s disease and mild cognitive impairment: A meta-analysis and systematic review. Ageing Res. Rev. 2021, 72, 101499. [Google Scholar] [CrossRef]
- Labree, B.; Hoare, D.J.; Gascoyne, L.E.; Scutt, P.; Del Giovane, C.; Sereda, M. Determining the effects of transcranial direct current stimulation on tinnitus, depression, and anxiety: A systematic review. Brain Sci. 2022, 12, 484. [Google Scholar] [CrossRef]
- Wen, Y.R.; Shi, J.; Hu, Z.Y.; Lin, Y.Y.; Lin, Y.T.; Jiang, X.; Wang, R.; Wang, X.Q.; Wang, Y.L. Is transcranial direct current stimulation beneficial for treating pain, depression, and anxiety symptoms in patients with chronic pain? A systematic review and meta-analysis. Front. Mol. Neurosci. 2022, 15, 1056966. [Google Scholar] [CrossRef]
- Scarmagnan, G.S.; Mello, S.C.M.; Lino, T.B.; Barbieri, F.A.; Christofoletti, G. Negative effect of task complexity on the balance and mobility of healthy older adults. Rev. Bras. Geriatr. Gerontol. 2021, 24, e200120. [Google Scholar] [CrossRef]
- Schneider, N.; Dagan, M.; Katz, R.; Thumm, P.C.; Brozgol, M.; Giladi, N.; Manor, B.; Mirelman, A.; Hausdorff, J.M. Combining transcranial direct current stimulation with a motor-cognitive task: The impact on dual-task walking costs in older adults. J. Neuroeng. Rehabil. 2021, 18, 23. [Google Scholar] [CrossRef]
- Belur, P.; Hsiao, D.; Myers, P.S.; Earhart, G.M.; Rawson, K.S. Dual-task costs of texting while walking forward and backward are greater for older adults than younger adults. Hum. Mov. Sci. 2020, 71, 102619. [Google Scholar] [CrossRef]
- Lino, T.B.; Scarmagnan, G.S.; Sobrinho-Junior, S.A.; Tessari, G.M.F.; Gonçalves, G.H.; Pereira, H.M.; Christofoletti, G. Impact of using smartphone while walking or standing: A study focused on age and cognition. Brain Sci. 2023, 13, 987. [Google Scholar] [CrossRef]
- Montori, V.M.; Guyatt, G.H. Intention-to-treat principle. CMAJ 2001, 165, 1339–1341. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Groups | p | ||
|---|---|---|---|---|
| tDCS | tDCS-Placebo | Control | ||
| Sex (men:women), n | 6:8 | 3:10 | 5:10 | 0.552 |
| Age, years | 71.3 (7.6) | 70.9 (7.6) | 72.6 (7.8) | 0.830 |
| Pfeffer Questionnaire, pts | 0.4 (0.8) | 0.5 (0.9) | 0.3 (0.8) | 0.815 |
| Mini-Mental State Examination, pts | 27.6 (1.7) | 26.1 (2.2) | 26.4 (1.9) | 0.126 |
| Frontal Assessment Battery, pts | 13.1 (2.0) | 12.9 (2.3) | 12.1 (2.7) | 0.510 |
| Semantic Verbal fluency, animals/minute | 13.1 (2.1) | 14.4 (4.6) | 12.3 (4.9) | 0.401 |
| Hospital Anxiety and Depression Scale, pts | 11.3 (4.7) | 10.0 (5.1) | 8.1 (5.2) | 0.246 |
| Timed Get Up and Go test, secs | 11.8 (1.7) | 12.2 (3.2) | 12.1 (3.2) | 0.938 |
| Cognition | Groups | MANOVA Main Effect | ||||||
|---|---|---|---|---|---|---|---|---|
| tDCS | tDCS-Placebo | Control | ||||||
| Assessment | Assessment | Assessment | ||||||
| Initial | Final | Initial | Final | Initial | Final | |||
| Mini-Mental State Examination, pts | 27.6 (1.7) | 28.6 (1.1) | 26.1 (2.2) | 27.1 (2.0) | 26.4 (1.9) | 26.9 (2.2) | Group | p = 0.101 |
| Frontal Assessment Battery, pts | 13.1 (2.0) | 14.3 (2.0) | 12.9 (2.3) | 13.4 (2.8) | 12.1 (2.7) | 12.6 (2.5) | Time | p = 0.001 |
| Semantic Verbal Fluency test, animals/min. | 13.1 (2.1) | 13.2 (2.2) | 14.4 (4.6) | 15.7 (4.6) | 12.3 (4.9) | 13.0 (4.9) | Interaction | p = 0.557 |
| Anxiety | Groups | ANOVA Main Effect | ||||||
|---|---|---|---|---|---|---|---|---|
| tDCS | tDCS-Placebo | Control | ||||||
| Assessment | Assessment | Assessment | ||||||
| Initial | Final | Initial | Final | Initial | Final | |||
| Hospital Anxiety and Depression Scale, pts | 11.3 (4.7) | 11.3 (4.8) | 10.0 (5.1) | 10.9 (5.4) | 8.1 (5.2) | 8.1 (6.0) | Group | p = 0.237 |
| Time | p = 0.355 | |||||||
| Interaction | p = 0.356 | |||||||
| Mobility | Groups | MANOVA Main Effect | ||||||
|---|---|---|---|---|---|---|---|---|
| tDCS | tDCS-Placebo | Control | ||||||
| Assessment | Assessment | Assessment | ||||||
| Initial | Final | Initial | Final | Initial | Final | |||
| Timed get-up-and-go test, secs | 11.8 (1.7) | 11.7 (1.8) | 12.2 (3.2) | 12.3 (2.8) | 12.1 (3.2) | 12.4 (3.5) | Group | p = 0.846 |
| Timed get-up-and-go test with motor distraction, secs | 12.0 (2.6) | 12.4 (2.6) | 12.9 (3.9) | 13.0 (4.1) | 13.1 (3.8) | 13.5 (2.9) | Time | p = 0.128 |
| Timed get-up-and-go test with cognitive distraction, secs | 13.2 (2.4) | 13.0 (2.4) | 15.2 (3.7) | 14.4 (3.3) | 15.4 (6.8) | 14.5 (5.6) | Interaction | p = 0.871 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodrigues, N.O.; Vidal Bravalhieri, A.A.; Moraes, T.P.d.; Barros, J.A.; Ansai, J.H.; Christofoletti, G. Efficacy of Transcranial Direct Current Stimulation (tDCS) on Cognition, Anxiety, and Mobility in Community-Dwelling Older Individuals: A Controlled Clinical Trial. Brain Sci. 2023, 13, 1614. https://doi.org/10.3390/brainsci13121614
Rodrigues NO, Vidal Bravalhieri AA, Moraes TPd, Barros JA, Ansai JH, Christofoletti G. Efficacy of Transcranial Direct Current Stimulation (tDCS) on Cognition, Anxiety, and Mobility in Community-Dwelling Older Individuals: A Controlled Clinical Trial. Brain Sciences. 2023; 13(12):1614. https://doi.org/10.3390/brainsci13121614
Chicago/Turabian StyleRodrigues, Nathalia Oliveira, Anna Alice Vidal Bravalhieri, Tatiane Pereira de Moraes, Jorge Aparecido Barros, Juliana Hotta Ansai, and Gustavo Christofoletti. 2023. "Efficacy of Transcranial Direct Current Stimulation (tDCS) on Cognition, Anxiety, and Mobility in Community-Dwelling Older Individuals: A Controlled Clinical Trial" Brain Sciences 13, no. 12: 1614. https://doi.org/10.3390/brainsci13121614
APA StyleRodrigues, N. O., Vidal Bravalhieri, A. A., Moraes, T. P. d., Barros, J. A., Ansai, J. H., & Christofoletti, G. (2023). Efficacy of Transcranial Direct Current Stimulation (tDCS) on Cognition, Anxiety, and Mobility in Community-Dwelling Older Individuals: A Controlled Clinical Trial. Brain Sciences, 13(12), 1614. https://doi.org/10.3390/brainsci13121614