
Development of a Machine Learning Model to Discriminate Mild Cognitive Impairment Subjects from Normal Controls in Community Screening

 , and
, and 
Abstract
:1. Introduction
2. MCI Prediction Algorithms
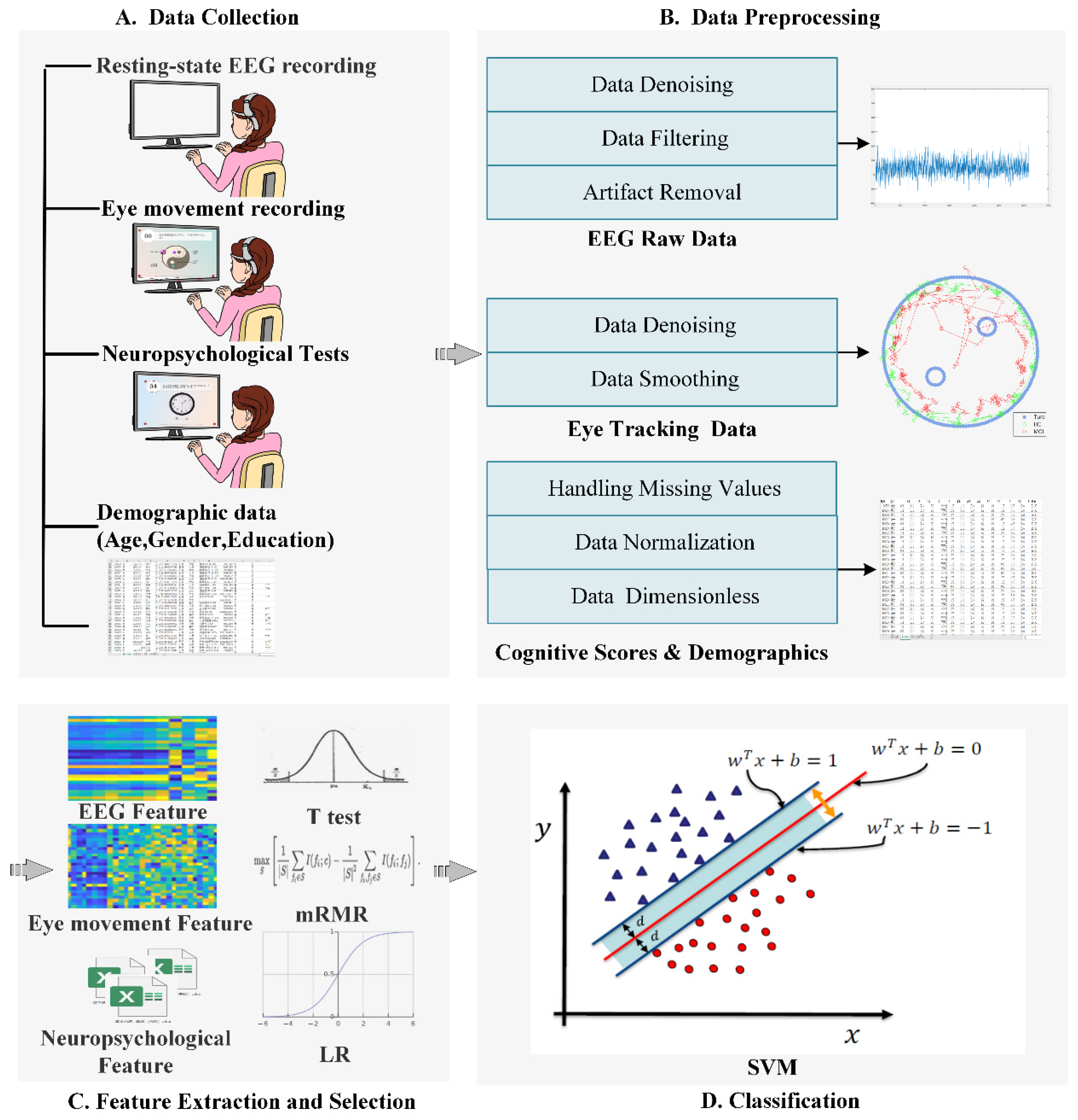
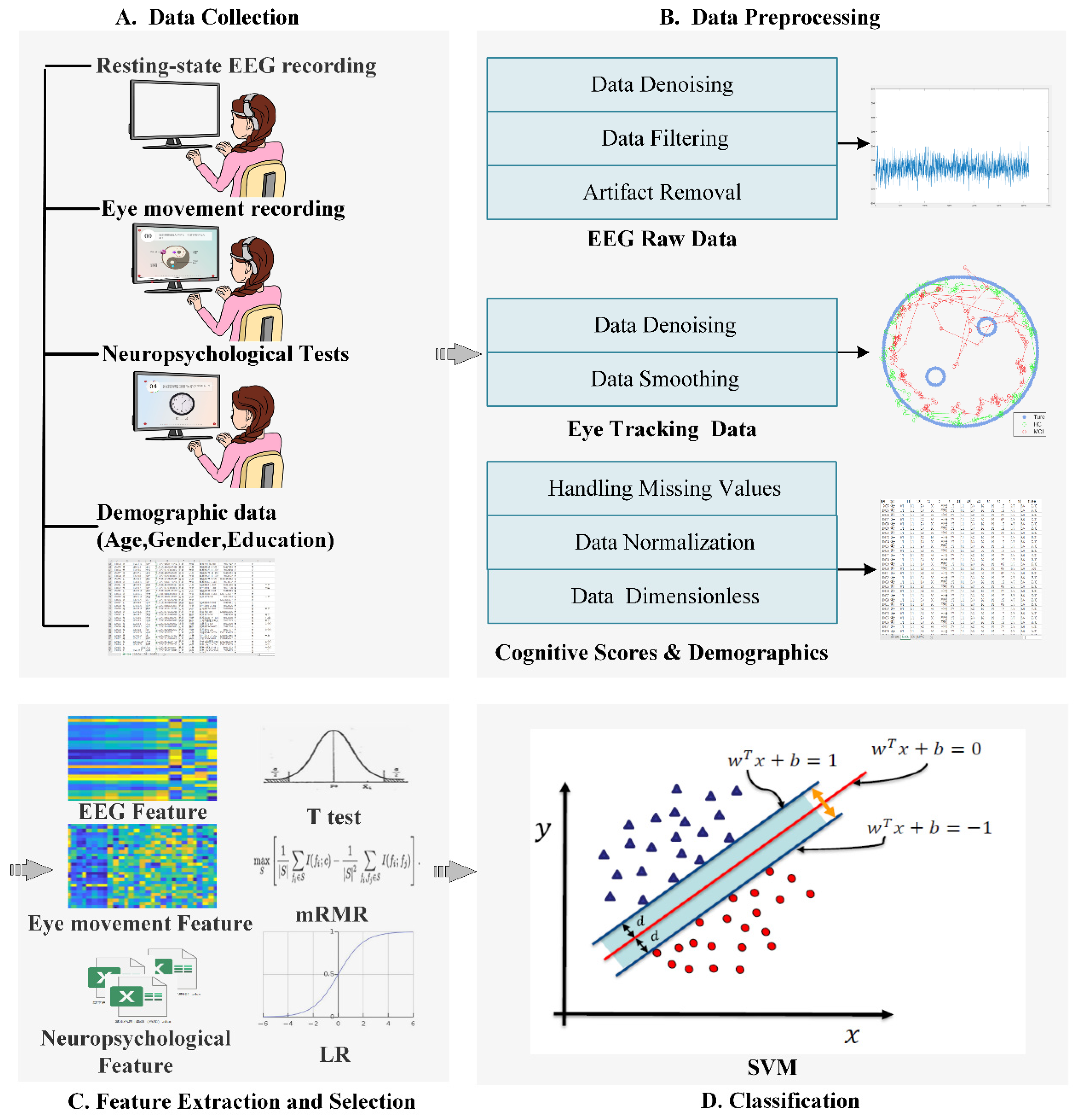
2.1. Data Collection
2.2. Data Preprocessing
2.2.1. EEG Preprocessing
2.2.2. ET Preprocessing
2.2.3. NTB Data Preprocessing
2.3. Feature Extraction
2.3.1. EEG Data
2.3.2. ET Data
2.3.3. NTB Data
2.4. Feature Selection
2.5. Classification
3. Materials and Methods
3.1. Subjects
3.2. Data Acquisition
3.3. Validation Experiments for Optimal Parameters of the Classifier
3.4. Discriminative Analysis
3.5. Statistical Analysis
4. Results
4.1. Demographic and Clinical Characteristics
4.2. Validation Experiments for Optimal Parameters of Classifier
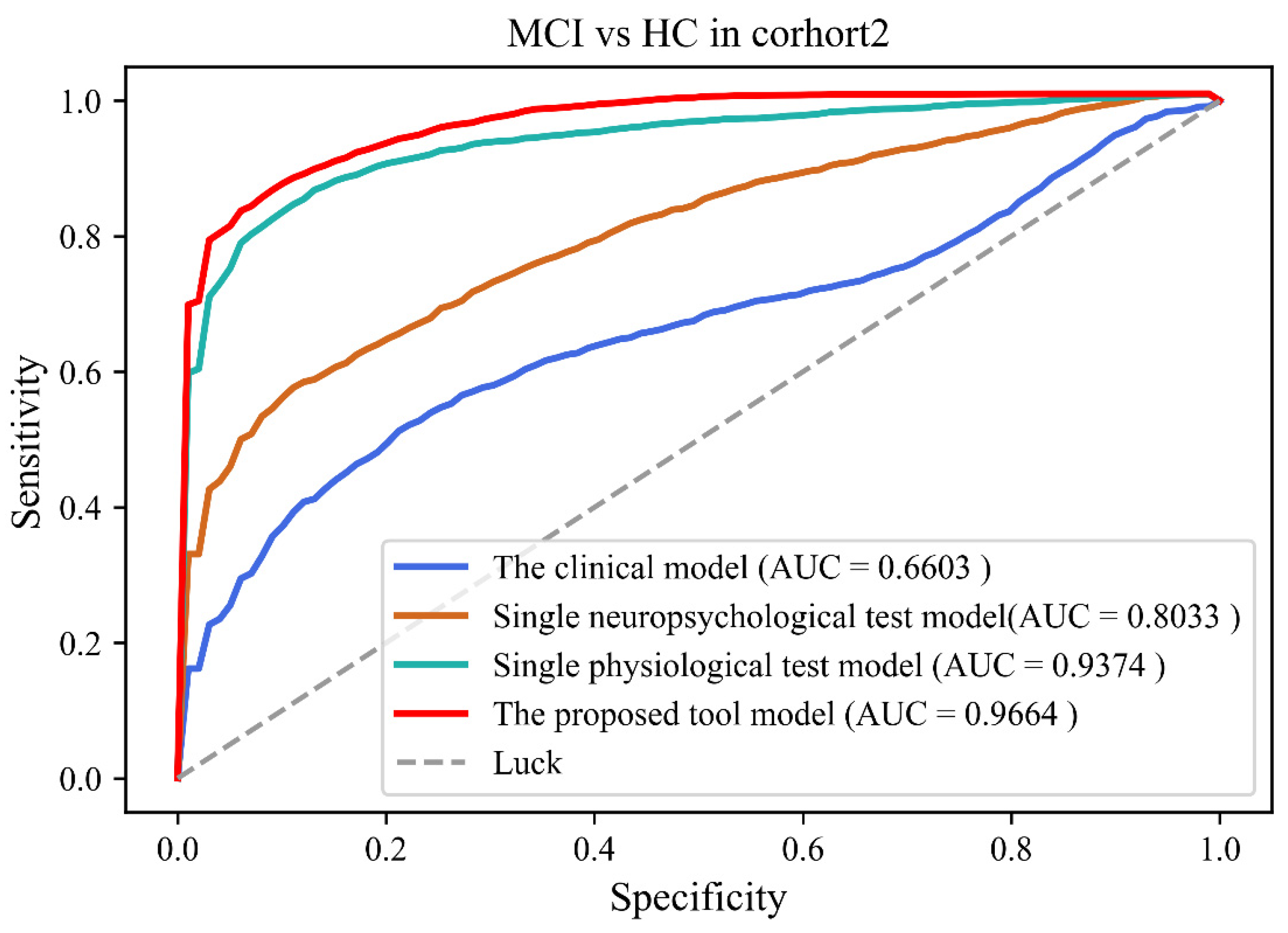
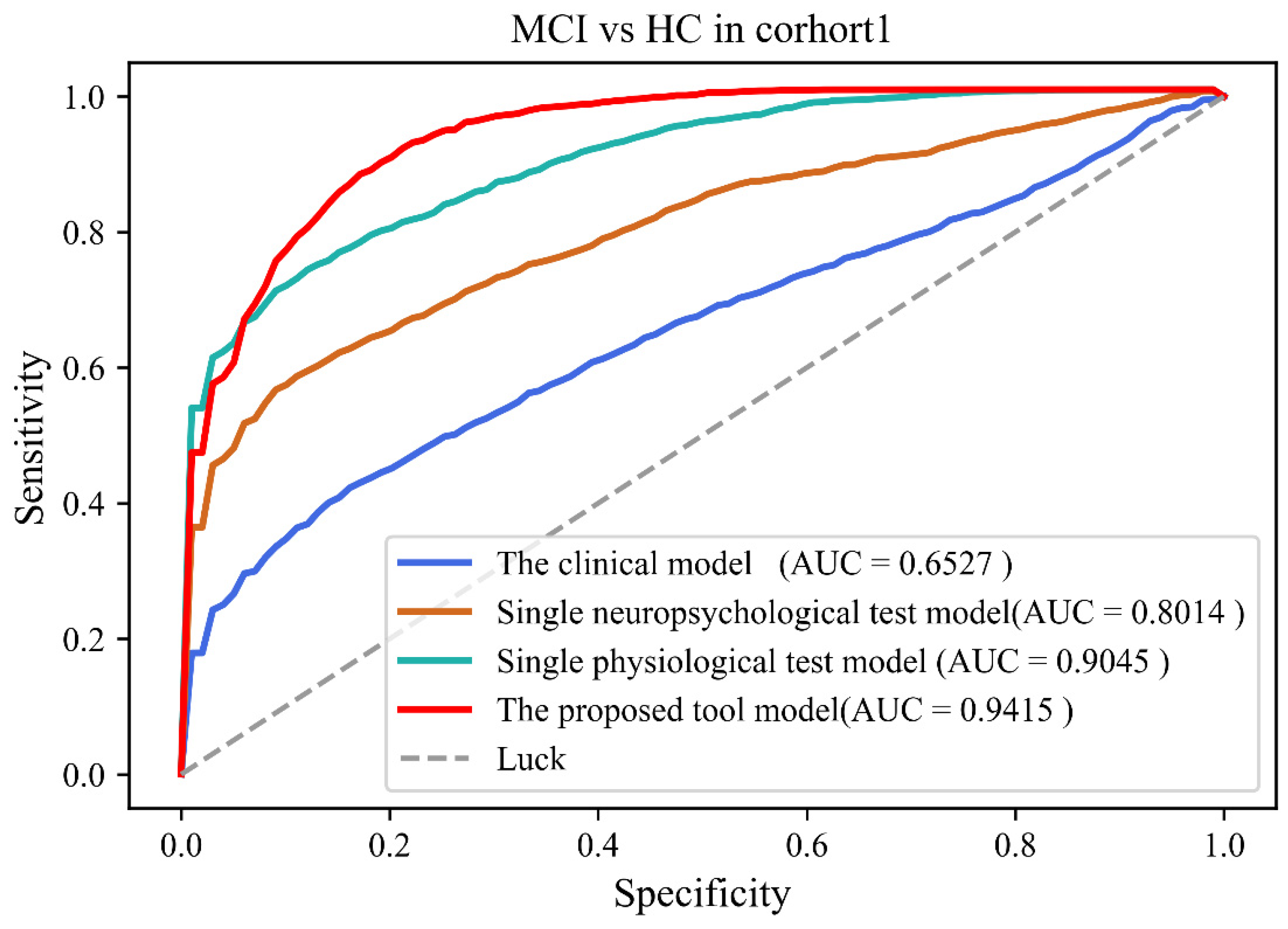
4.3. Discriminative Analysis
5. Discussion
- (1)
- In terms of feature extraction, the linear and nonlinear feature analysis has been successfully used to identify the powerful biomarkers of neurophysiological diseases, such as Alzheimer’s disease (AD). In this study, we applied both linear and nonlinear methods to extract EEG and eye movement features. For EEG, complexity analysis as a nonlinear dynamic method can represent the rate of new patterns appearing in a time series, and to a certain extent, details of the signal can be presented in the binarized sequence.
- (2)
- In terms of feature selection and classification, the SVM model was selected. As a ML model, the SVM is suitable for classifying the features obtained from neuropsychological assessments.
- (3)
- In terms of the clinical setting, we depicted a machine learning framework for automated cognitive assessment data analysis for the precise classification of healthy and mild cognitive impairment individuals. Our work opens the possibility for automated assessment of cognitive function in community screening.
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rocaspana-García, M.; Blanco-Blanco, J.; Arias-Pastor, A.; Gea-Sánchez, M.; Piñol-Ripoll, G.J.P. Study of community-living Alzheimer’s patients’ adherence to the Mediterranean diet and risks of malnutrition at different disease stages. PeerJ 2018, 6, e5150. [Google Scholar] [CrossRef] [PubMed]
- Jia, L.; Quan, M.; Fu, Y.; Zhao, T.; Li, Y.; Wei, C.; Tang, Y.; Qin, Q.; Wang, F.; Qiao, Y.; et al. Dementia in China: Epidemiology, clinical management, and research advances. Lancet Neurol. 2020, 19, 81–92. [Google Scholar] [CrossRef]
- Jia, L.; Du, Y.; Chu, L.; Zhang, Z.; Li, F.; Lyu, D.; Li, Y.; Li, Y.; Zhu, M.; Jiao, H.; et al. Prevalence, risk factors, and management of dementia and mild cognitive impairment in adults aged 60 years or older in China: A cross-sectional study. Lancet Public Health 2020, 5, e661–e671. [Google Scholar] [CrossRef]
- Petersen, R.C.; Roberts, R.O.; Knopman, D.S.; Boeve, B.F.; Geda, Y.E.; Ivnik, R.J.; Smith, G.E.; Jack, C.R., Jr. Mild cognitive impairment: Ten years later. Arch. Neurol. 2009, 66, 1447–1455. [Google Scholar] [CrossRef]
- Petersen, R.C.; Smith, G.E.; Waring, S.C.; Ivnik, R.J.; Tangalos, E.G.; Kokmen, E. Mild cognitive impairment: Clinical characterization and outcome. Arch. Neurol. 1999, 56, 303–308. [Google Scholar] [CrossRef]
- Wang, M.; Jiang, J.; Yan, Z.; Alberts, I.L.; Ge, J.; Zhang, H.; Zuo, C.; Yu, J.; Rominger, A.; Shi, K.; et al. Individual brain metabolic connectome indicator based on Kullback-Leibler Divergence Similarity Estimation predicts progression from mild cognitive impairment to Alzheimer’s dementia. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 2753–2764. [Google Scholar] [CrossRef]
- Jiang, J.; Sun, X.-M.; Alberts, I.L.; Wang, M.; Rominger, A.; Zuo, C.; Han, Y.; Shi, K.; Initiative, F.T.A.D.N. Using radiomics-based modelling to predict individual progression from mild cognitive impairment to Alzheimer’s disease. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 2163–2173. [Google Scholar] [CrossRef]
- Jack, C.R., Jr.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Dunn, B.; Haeberlein, S.B.; Holtzman, D.M.; Jagust, W.; Jessen, F.; Karlawish, J.; et al. NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. Alzheimers Dement. 2018, 14, 535–562. [Google Scholar] [CrossRef]
- Petersen, R.C.; Yaffe, K. Issues and Questions Surrounding Screening for Cognitive Impairment in Older Patients. JAMA 2020, 323, 722–724. [Google Scholar] [CrossRef]
- Marcucci, V.; Kleiman, J.D. Biomarkers and Their Implications in Alzheimer’s Disease: A Literature Review. Explor. Res. Hypothesis Med. 2021, 6, 164–176. [Google Scholar] [CrossRef]
- Chandra, A.; Dervenoulas, G.; Politis, M. Magnetic resonance imaging in Alzheimer’s disease and mild cognitive impairment. J. Neurol. 2018, 266, 1293–1302. [Google Scholar] [CrossRef] [PubMed]
- Arbizu, J.; Festari, C.; Altomare, D.; Walker, Z.; Bouwman, F.H.; Rivolta, J.; Orini, S.; Barthel, H.; Agosta, F.; Drzezga, A.; et al. Clinical utility of FDG-PET for the clinical diagnosis in MCI. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 1497–1508. [Google Scholar] [CrossRef] [PubMed]
- Alberdi, A.; Aztiria, A.; Basarab, A. On the early diagnosis of Alzheimer’s Disease from multimodal signals: A survey. Artif. Intell. Med. 2016, 71, 1–29. [Google Scholar] [CrossRef] [PubMed]
- Laske, C.; Sohrabi, H.R.; Frost, S.; Lopez-de-Ipina, K.; Garrard, P.; Buscema, M.; Dauwels, J.; Soekadar, S.R.; Mueller, S.; Linnemann, C.; et al. Innovative diagnostic tools for early detection of Alzheimer’s disease. Alzheimer’s Dement. 2015, 11, 561–578. [Google Scholar] [CrossRef]
- Yim, D.; Yeo, T.Y.; Park, M.H. Mild cognitive impairment, dementia, and cognitive dysfunction screening using machine learning. J. Int. Med. Res. 2020, 48, 7. [Google Scholar] [CrossRef]
- Schmid, N.S.; Taylor, K.I.; Foldi, N.S.; Berres, M.; Monsch, A.U. Neuropsychological signs of Alzheimer’s disease 8 years prior to diagnosis. J. Alzheimer’s Dis. 2013, 34, 537–546. [Google Scholar] [CrossRef]
- Paúl, C.; Sousa, S.; Santos, P.; O’Caoimh, R.; Molloy, W. Screening Neurocognitive Disorders in Primary Care Services: The Quick Mild Cognitive Impairment Approach. Innov. Aging 2020, 4, 158. [Google Scholar] [CrossRef]
- Murty, D.V.P.S.; Manikandan, K.; Kumar, W.S.; Ramesh, R.G.; Purokayastha, S.; Nagendra, B.; Ml, A.; Balakrishnan, A.; Javali, M.; Rao, N.P.; et al. Stimulus-induced gamma rhythms are weaker in human elderly with mild cognitive impairment and Alzheimer’s disease. eLife 2021, 10, e61666. [Google Scholar] [CrossRef]
- Oyama, A.; Takeda, S.; Ito, Y.; Nakajima, T.; Takami, Y.; Takeya, Y.; Yamamoto, K.; Sugimoto, K.; Shimizu, H.; Shimamura, M.; et al. Novel Method for Rapid Assessment of Cognitive Impairment Using High-Performance Eye-Tracking Technology. Sci. Rep. 2019, 9, 12932. [Google Scholar] [CrossRef]
- Nie, J.; Qiu, Q.; Phillips, M.; Sun, L.; Yan, F.; Lin, X.; Xiao, S.; Li, X. Early Diagnosis of Mild Cognitive Impairment Based on Eye Movement Parameters in an Aging Chinese Population. Front. Aging Neurosci. 2020, 12, 221. [Google Scholar] [CrossRef]
- Choi, J.; Lim, E.; Park, M.G.; Cha, W. Assessing the Retest Reliability of Prefrontal EEG Markers of Brain Rhythm Slowing in the Eyes-Closed Resting State. Clin. EEG Neurosci. 2020, 51, 348–356. [Google Scholar] [CrossRef]
- Liu, Z.; Yang, Z.; Gu, Y.; Liu, H.; Wang, P. The effectiveness of eye tracking in the diagnosis of cognitive disorders: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0254059. [Google Scholar] [CrossRef]
- Jiang, J.; Yan, Z.; Sheng, C.; Wang, M.; Guan, Q.; Yu, Z.; Han, Y.; Jiang, J. A Novel Detection Tool for Mild Cognitive Impairment Patients Based on Eye Movement and Electroencephalogram. J. Alzheimer’s Dis. 2019, 72, 389–399. [Google Scholar] [CrossRef]
- Lv, S.; Wang, X.; Cui, Y.; Jin, J.; Sun, Y.L.; Tang, Y.; Bai, Y.; Wang, Y.; Zhou, L. Application of attention network test and demographic information to detect mild cognitive impairment via combining feature selection with support vector machine. Comput. Methods Programs Biomed. 2010, 97, 11–18. [Google Scholar] [CrossRef]
- Lin, M.; Gong, P.; Yang, T.; Ye, J.; Albin, R.L.; Dodge, H.H.; Disorders, A. Big Data Analytical Approaches to the NACC Dataset: Aiding Preclinical Trial Enrichment. Alzheimer Dis. Assoc. Disord. 2018, 32, 18–27. [Google Scholar] [CrossRef]
- Abásolo, D.E.; Hornero, R.; Espino, P.; Poza, J.; Sánchez, C.I.; Rosa, R. Analysis of regularity in the EEG background activity of Alzheimer’s disease patients with Approximate Entropy. Clin. Neurophysiol. 2005, 116, 1826–1834. [Google Scholar] [CrossRef]
- Costa, M.; Goldberger, A.L.; Peng, C.-K. Multiscale entropy analysis of complex physiologic time series. Phys. Rev. Lett. 2002, 89, 068102. [Google Scholar] [CrossRef]
- Lempel, A.; Ziv, J. On the Complexity of Finite Sequences. IEEE Trans. Inf. Theory 1976, 22, 75–81. [Google Scholar] [CrossRef]
- Peng, H.; Long, F.; Ding, C.; Intelligence, M. Feature selection based on mutual information criteria of max-dependency, max-relevance, and min-redundancy. IEEE Trans. Pattern Anal. Mach. Intell. 2005, 27, 1226–1238. [Google Scholar] [CrossRef]
- Bondi, M.W.; Edmonds, E.C.; Jak, A.J.; Clark, L.; Delano-Wood, L.; McDonald, C.R.; Nation, D.A.; Libon, D.J.; Au, R.; Galasko, D.R.; et al. Neuropsychological criteria for mild cognitive impairment improves diagnostic precision, biomarker associations, and progression rates. J. Alzheimer’s Dis. 2014, 42, 275–289. [Google Scholar] [CrossRef] [Green Version]
- Albert, M.S.; DeKosky, S.T.; Dickson, D.W.; Dubois, B.; Feldman, H.H.; Fox, N.C.; Gamst, A.C.; Holtzman, D.M.; Jagust, W.J.; Petersen, R.C.; et al. The Diagnosis of Mild Cognitive Impairment due to Alzheimer’s Disease: Recommendations from the National Institute on Aging-Alzheimer’s Association Workgroups on Diagnostic Guidelines for Alzheimer’s Disease. Focus 2011, 11, 96–106. [Google Scholar] [CrossRef]
- Petersen, R.C. Mild cognitive impairment as a diagnostic entity. Psychology 2011, 11, 96–106. [Google Scholar] [CrossRef]
- Siuly, S.; Alçin, Ö.F.; Kabir, E.; Şengür, A.; Wang, H.; Zhang, Y.; Whittaker, F.; Engineering, R. A New Framework for Automatic Detection of Patients With Mild Cognitive Impairment Using Resting-State EEG Signals. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 1966–1976. [Google Scholar] [CrossRef]
- Lagun, D.; Manzanares, C.; Zola, S.; Buffalo, E.; Agichtein, E. Detecting cognitive impairment by eye movement analysis using automatic classification algorithms. J. Neurosci. Methods 2011, 201, 196–203. [Google Scholar] [CrossRef]
- Wang, J.; Wang, Z.; Liu, N.; Liu, C.; Mao, C.; Dong, L.-L.; Li, J.; Huang, X.; Lei, D.; Chu, S.; et al. Random Forest Model in the Diagnosis of Dementia Patients with Normal Mini-Mental State Examination Scores. J. Pers. Med. 2022, 12, 37. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Cohort 1 | Cohort 2 | |||||
|---|---|---|---|---|---|---|
| NC (184) | MCI (152) | p Value | NC (48) | MCI (44) | p Value | |
| Age (years) | 71.7 ± 4.66 | 71.6 ± 4.15 | 0.875 b | 69.3 ± 17.0 | 76.5 ± 11.3 | 0.783 b |
| Education (years) | 9.36 ± 3.47 | 8.16 ± 3.74 | 0.541 a | 13.0 ± 3.87 | 10.8 ± 5.66 | 0.492 a |
| Gender (male/female) | 101/83 | 78/74 | 0.071 c | 18/30 | 16/28 | 0.068 c |
| MoCA-B | 28.3 ± 0.95 | 23.2 ± 3.40 | <0.001 b * | 23.8 ± 3.28 | 16.4 ± 3.84 | <0.001 b * |
| ACE-R | 72.1 ± 7.79 | 63.7 ± 8.53 | <0.001 b * | 71.0 ± 24.9 | 64.2 ± 8.28 | <0.001 b * |
| Kernel Function | C | GAMMA | Accuracy (%) | Sensitivity (%) | Specificity (%) | AUC (95% CI) |
|---|---|---|---|---|---|---|
| Linear | 4.0 | / | 84.3 ± 4.05 | 83.1 ± 7.70 | 85.5 ± 4.97 | 0.906 (0.841–0.969) |
| Poly | 20.0 | 0.02 | 78.1 ± 9.90 | 83.6 ± 10.6 | 71.3 ± 13.6 | 0.851 (0.747–0.954) |
| RBF | 1.1 | 0.001 | 84.5 ± 4.34 | 82.4 ± 7.36 | 86.5 ± 6.51 | 0.934 (0.878–0.977) |
| Sigmoid | 17.0 | 0.01 | 82.1 ± 6.08 | 90.9 ± 8.13 | 71.3 ± 11.7 | 0.851 (0.838–0.964) |
| Comparative Model | Accuracy (%) | Sensitivity (%) | Specificity (%) | AUC (95% CI) |
|---|---|---|---|---|
| The clinical model | 62.6 ± 5.19 | 54.7 ± 6.81 | 71.4 ± 5.56 | 0.653 (0.541–0.783) |
| Single neuropsychological test model | 75.6 ± 4.60 | 55.7 ± 8.15 | 71.2 ± 4.72 | 0.8014 (0.700–0.885) |
| Single physiological test model | 81.4 ± 4.66 | 72.1 ± 8.25 | 89.2 ± 5.42 | 0.9045 (0.819–0.961) |
| The proposed tool model | 84.5 ± 4.43 | 81.9± 7.88 | 86.8 ± 6.19 | 0.9415 (0.893–0.982) |
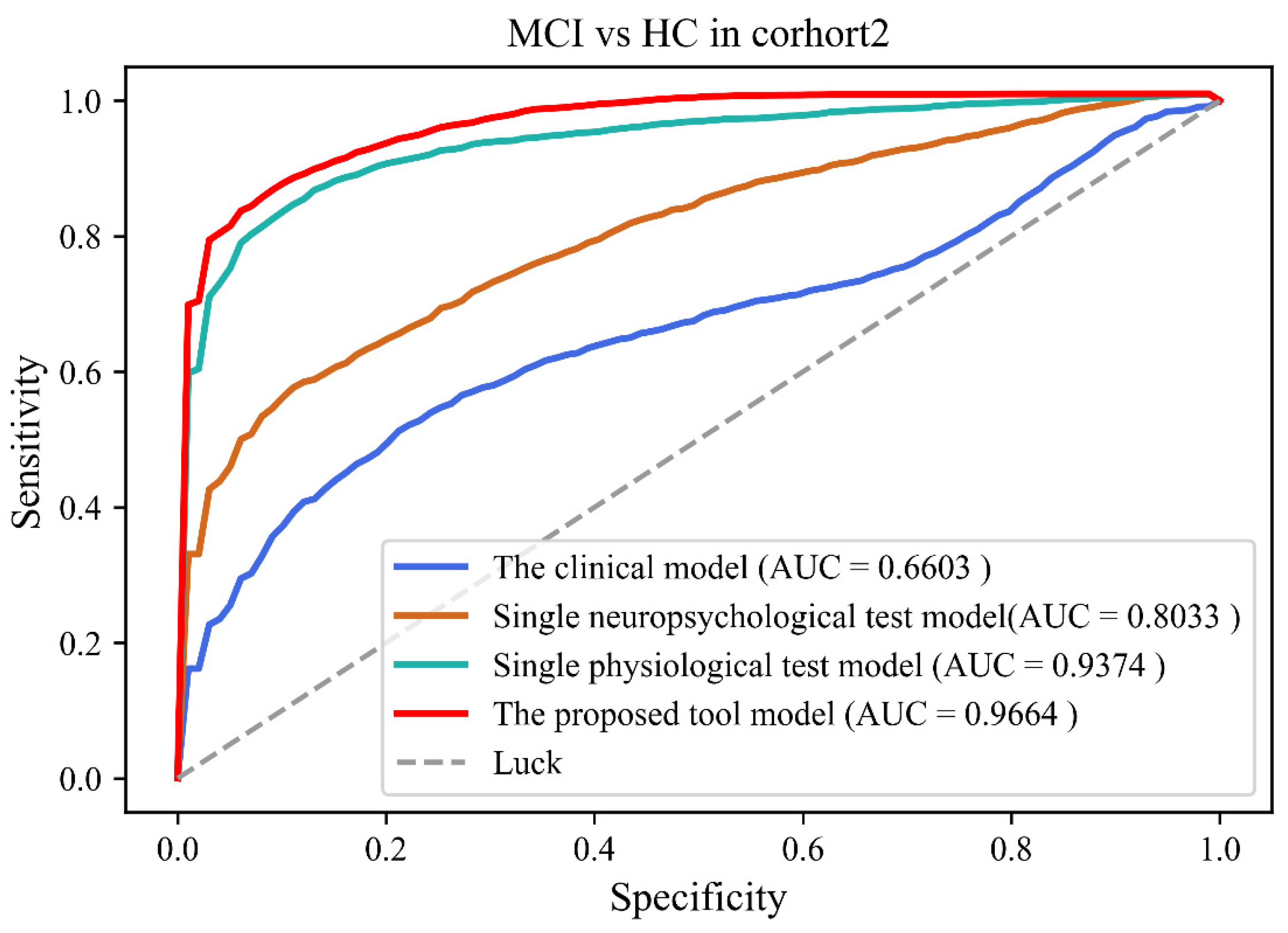
| Comparative Model | Accuracy (%) | Sensitivity (%) | Specificity (%) | AUC (95% CI) |
|---|---|---|---|---|
| The clinical model | 65.7 ± 4.93 | 43.3 ± 10.6 | 90.1 ± 7.94 | 0.660 (0.543–0.789) |
| Single neuropsychological test model | 75.0 ± 5.22 | 54.1 ± 8.63 | 91.5 ± 4.73 | 0.803 (0.681–0.889) |
| Single physiological test model | 87.0 ± 4.27 | 82.4 ± 7.94 | 90.6 ± 5.05 | 0.937 (0.867–0.985) |
| The proposed tool model | 88.8 ± 3.59 | 86.2 ± 6.46 | 91.0 ± 5.39 | 0.966 (0.921–0.988) |
| Detection Tools | Modality | Subject | Method | Classifier | Accuracy |
|---|---|---|---|---|---|
| EEG based | Siuly, 2020 [33] EEG (19 Electrodes) | 27 | EEG features | ELM | 98.8% |
| ET based | Lagun, 2011 [34] ET Test | 174 | ET features | SVM | 87% |
| Neuropsychological test based | Yim, 2020 [15] | 614 | The mean total scores of neuropsychological test | GB | 93.5% |
| NTB based | Wang, 2022 [35] Neuropsychological tests battery | 241 | NTB scores | RF | 68% |
| Proposed Method NTB, EEG and Eye tracking | EEG (1 electrode) & ET & Neuropsychological test battery | 336 | EEG & ET features & NTB scores | SVM | 88.8% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, J.; Zhang, J.; Li, C.; Yu, Z.; Yan, Z.; Jiang, J. Development of a Machine Learning Model to Discriminate Mild Cognitive Impairment Subjects from Normal Controls in Community Screening. Brain Sci. 2022, 12, 1149. https://doi.org/10.3390/brainsci12091149
Jiang J, Zhang J, Li C, Yu Z, Yan Z, Jiang J. Development of a Machine Learning Model to Discriminate Mild Cognitive Impairment Subjects from Normal Controls in Community Screening. Brain Sciences. 2022; 12(9):1149. https://doi.org/10.3390/brainsci12091149
Chicago/Turabian StyleJiang, Juanjuan, Jieming Zhang, Chenyang Li, Zhihua Yu, Zhuangzhi Yan, and Jiehui Jiang. 2022. "Development of a Machine Learning Model to Discriminate Mild Cognitive Impairment Subjects from Normal Controls in Community Screening" Brain Sciences 12, no. 9: 1149. https://doi.org/10.3390/brainsci12091149
APA StyleJiang, J., Zhang, J., Li, C., Yu, Z., Yan, Z., & Jiang, J. (2022). Development of a Machine Learning Model to Discriminate Mild Cognitive Impairment Subjects from Normal Controls in Community Screening. Brain Sciences, 12(9), 1149. https://doi.org/10.3390/brainsci12091149