
Executive Function Improves Following Acute Exercise in Adults with Down Syndrome


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Baseline
2.3. Interventions
2.4. Resistance Training (RT)
2.5. Assisted Cycle Therapy (ACT)
2.6. No Training (NT) or Control
2.7. Dependent Measures
2.7.1. Ericksen Flanker Task
2.7.2. Tower of London Test (TOL)
2.8. Data Analysis
3. Results
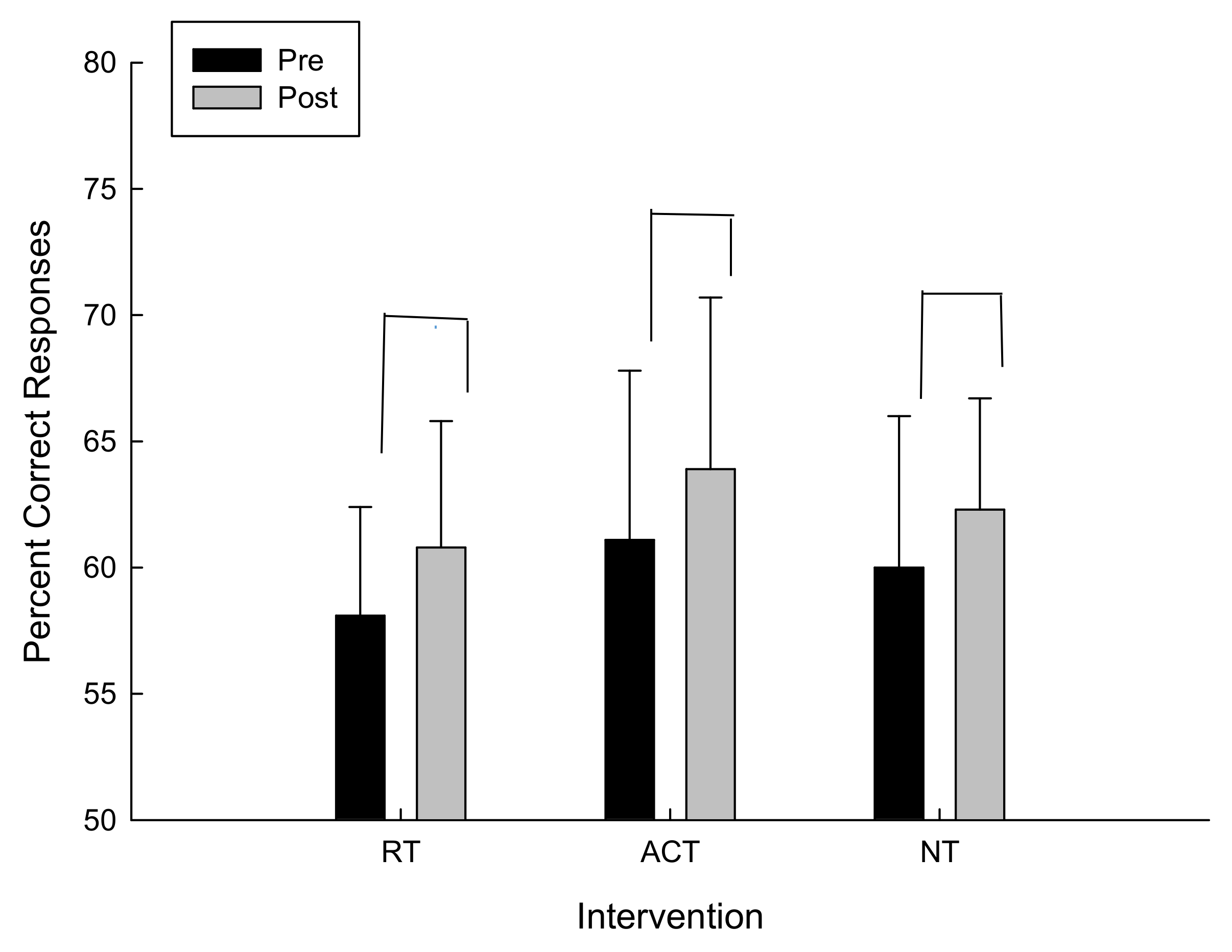
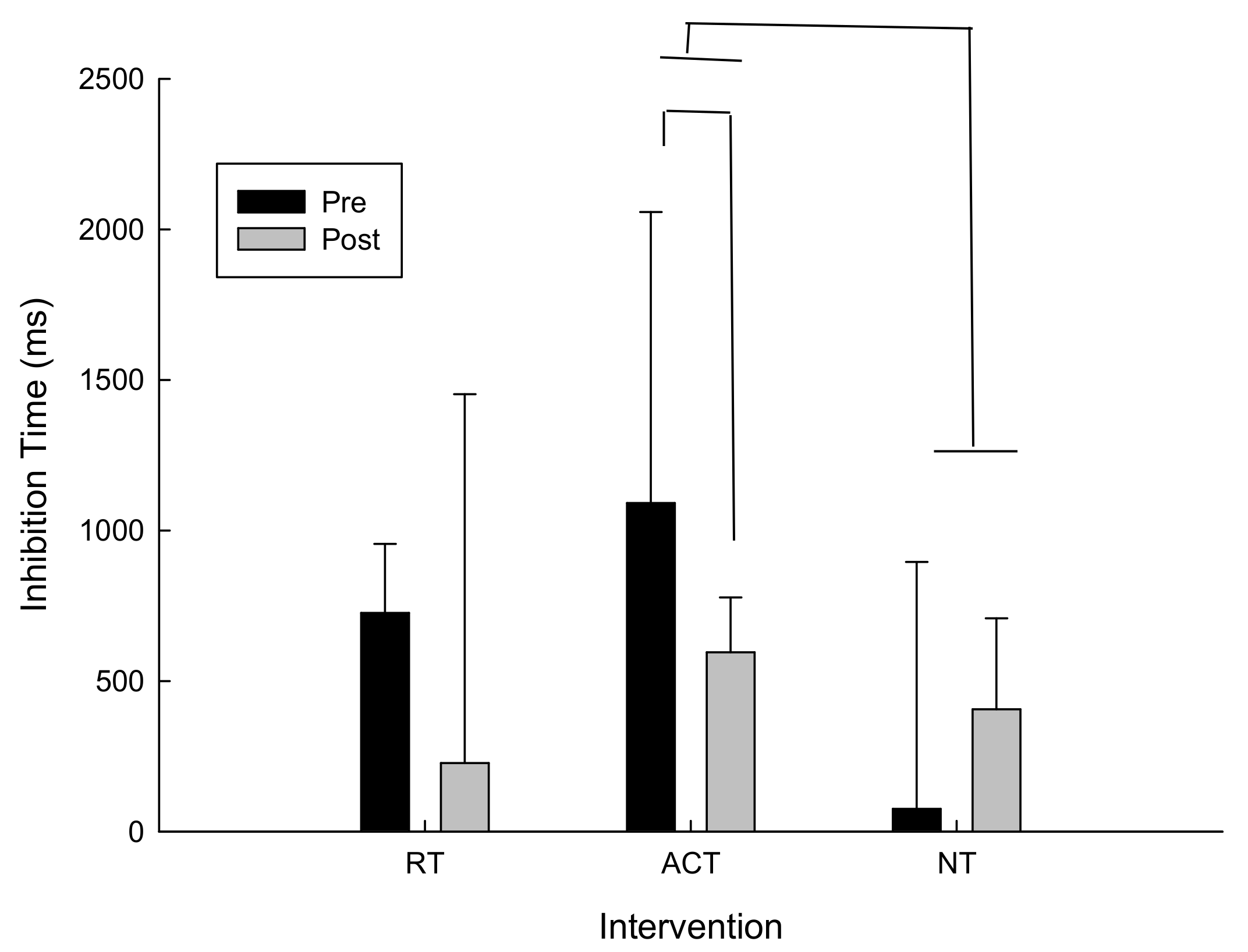
3.1. Inhibition
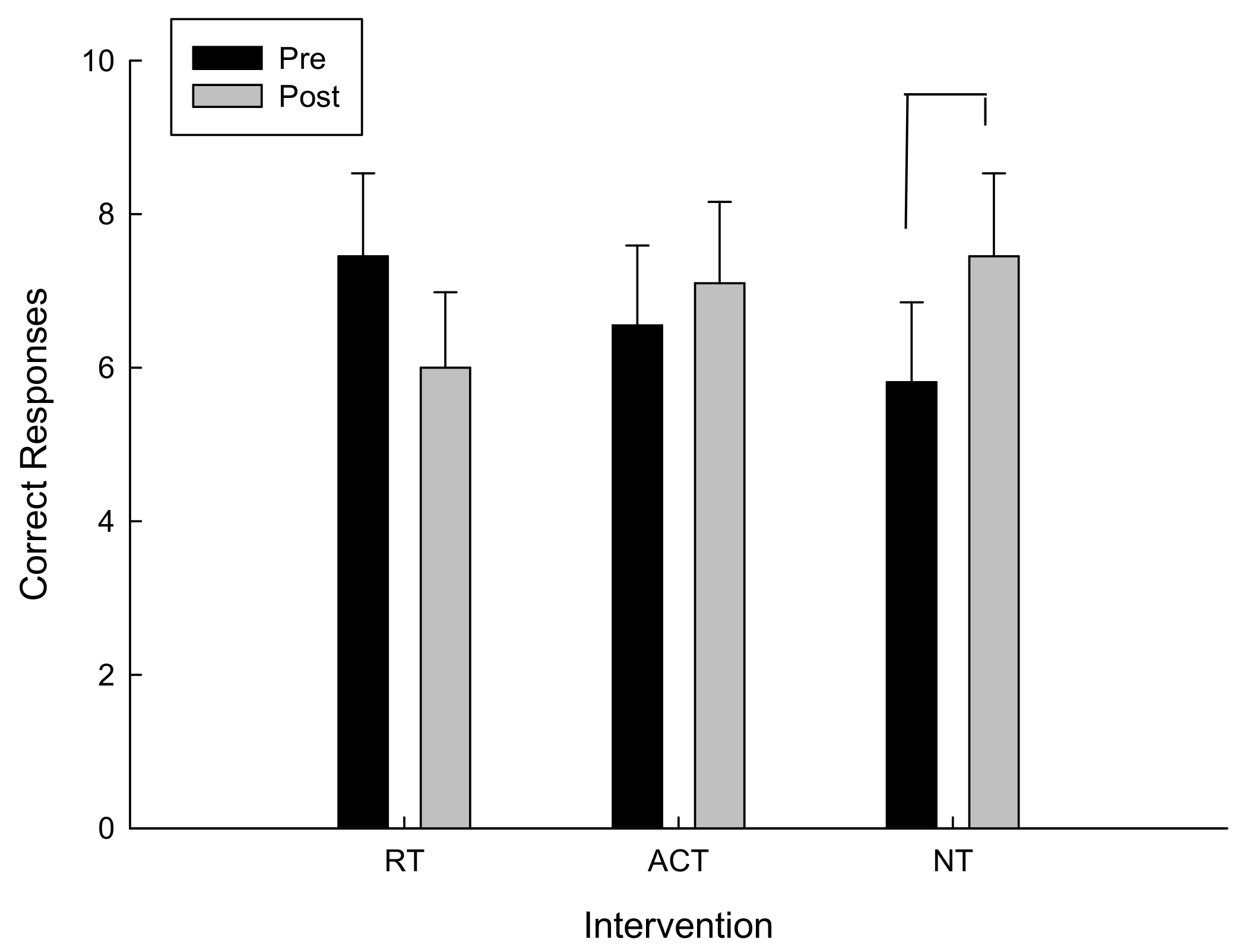
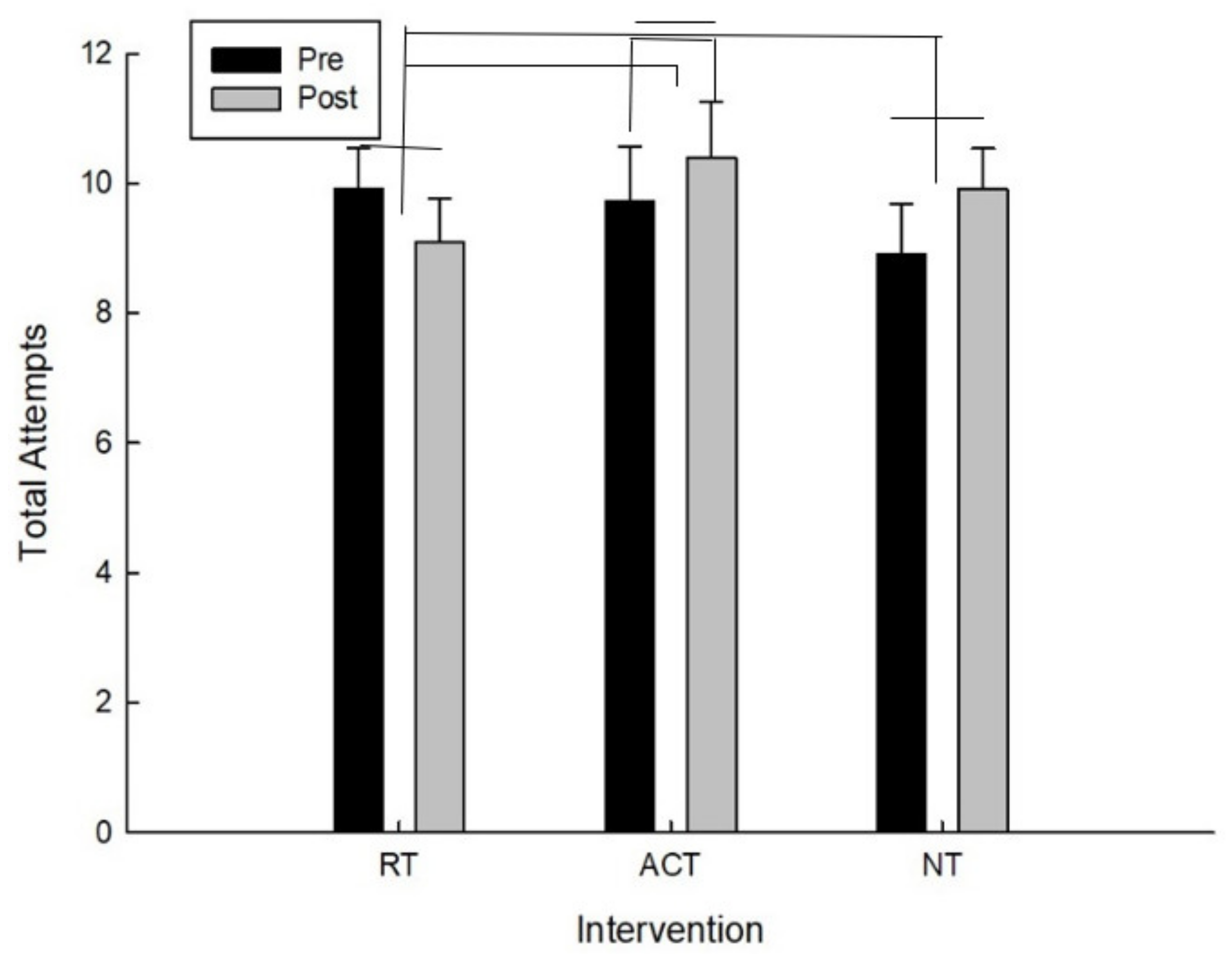
3.2. Cognitive Planning
4. Discussion
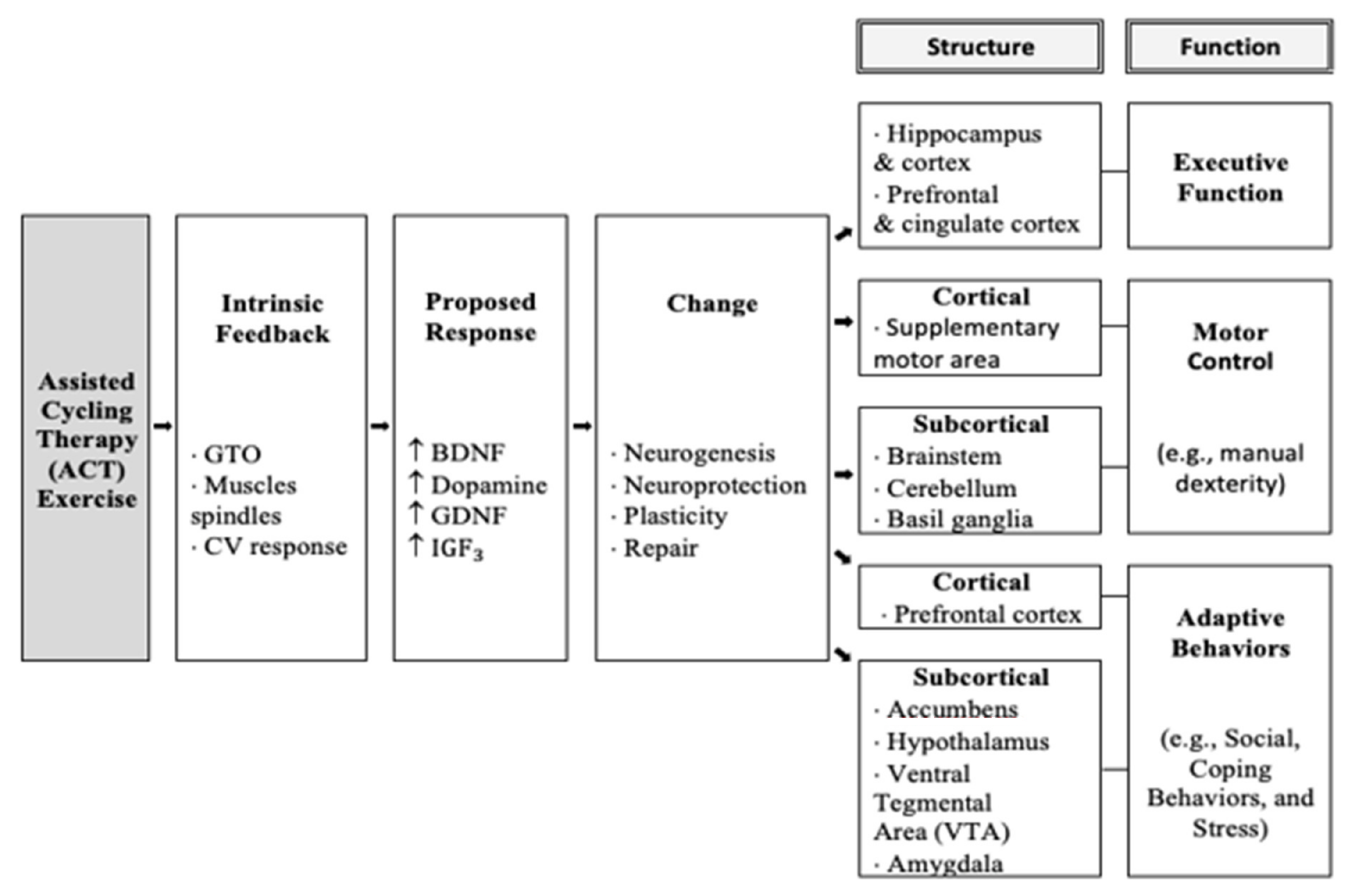
4.1. Neural Hypothesis
4.2. Cognitive Stimulation Hypothesis
4.3. Intensity Hypothesis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Parker, S.E.; Kirby, R.S.; Correa, A.; Mai, C.T.; Canfield, M.A.; Rickard, R. National Birth Defects Prevention Network. Updated national birth prevalence estimates for selected birth defects in the United States, 2004–2006. Birth Defects Research. Part A Clin. Mol. Terat. 2010, 88, 1008. [Google Scholar]
- Angulo-Barroso, R.; Burghardt, A.R.; Lloyd, M.; Ulrich, D.A. Physical activity in infants with Down syndrome receiving a treadmill intervention. Infant. Behav. Dev. 2008, 31, 255–269. [Google Scholar] [CrossRef] [PubMed]
- Rowe, J.; Lavender, A.; Turk, V. Cognitive executive function in Down’s syndrome. Br. J. Clin. Psychol. 2006, 45, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Tomaszewski, B.; Fidler, D.; Talapatra, D.; Riley, K. Adaptive behaviour, executive function and employment in adults with Down syndrome. J. Intellect. Disabil Res. 2018, 62, 41–52. [Google Scholar] [CrossRef]
- Diamond, A. Executive functions. Ann. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef]
- Lanfranchi, S.; Jerman, O.; Dal Pont, E.; Alberti, A.; Vianello, R. Executive function in adolescents with Down Syndrome. J. Intellect. Disabil. Res. 2010, 54, 308–319. [Google Scholar] [CrossRef]
- Traverso, L.; Fontana, M.; Usai, M.C.; Passolunghi, M.C. Response Inhibition and Interference Suppression in Individuals With Down Syndrome Compared to Typically Developing Children. Front. Psychol. 2018, 9, 660. [Google Scholar] [CrossRef] [PubMed]
- Pennington, B.; Bennetto, L. Towards a neuropsychology of mental retardation. In Handbook of Mental Retardation; Burack, J.A., Hodapp, R.M., Eds.; Cambridge University Press: New York, NY, USA, 1998; pp. 80–114. [Google Scholar]
- Crnic, L.S.; Pennington, B.F. Down syndrome: Neuropsychology and animal models. In Progress in Infancy Research; Rovee-Collier, C., Lipsitt, L.P., Eds.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 2000; Volume 1, pp. 69–111. [Google Scholar]
- Ringenbach, S.D.R.; Albert, A.R.; Chen, C.C.; Alberts, J.L. Acute bouts of assisted cycling improves cognitive and upper extremity movement functions in adolescents with Down syndrome. Intellect. Dev. Disabil. 2014, 52, 124–135. [Google Scholar] [CrossRef]
- Pitetti, K.; Agiovlasitis, T. Children and adolescents with Down syndrome, physical fitness and physical activity. J. Sport Health Sci. 2013, 2, 47–57. [Google Scholar] [CrossRef]
- Alberts, J.L.; Linder, S.M.; Penko, A.L.; Lowe, M.J.; Phillips, M. It is not about the bike, it is about the pedaling: Forced exercise and Parkinson’s disease. Ex. Sport Sci. Rev. 2011, 39, 177–186. [Google Scholar] [CrossRef]
- Fisher, B.E.; Petzinger, G.M.; Nixon, K. Exercise-induced behavioral recovery and neuroplasticity in the 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine-leasioned mouse basal ganglia. J. Neurosci. Res. 2004, 77, 378–390. [Google Scholar] [CrossRef]
- Ridgel, A.L.; Kim, C.; Fickes, E.J.; Muller, M.D.; Alberts, J.L. Changes in executive function after acute bouts of passive cycling in Parkinson’s disease. J. Aging Phys. Activ. 2011, 19, 87–98. [Google Scholar] [CrossRef]
- Ringenbach, S.D.R.; Holzapfel, S.D.; Mulvey, G.M.; Jimenez, A.; Benson, A.; Richter, M. The effects of assisted cycling therapy (ACT) and voluntary cycling on reaction time and measures of executive function in adolescents with Down syndrome. J. Intellect. Disabil. Res. 2016, 60, 1073–1085. [Google Scholar] [CrossRef]
- Ringenbach, S.D.R.; Lichtsinn, K.C.; Holzapfel, S.D. Assisted cycle therapy (ACT) improves inhibition in adolescents with autism spectrum disorder. J. Intellect. Dev. Disabil. 2015, 40, 376–387. [Google Scholar] [CrossRef]
- Shields, N.; Taylor, N.F.; Wee, E.; Wollersheim, D.; O’Shea, S.D.; Fernhall, B. A community-based strength training programme increases muscle strength and physical activity in young people with Down syndrome: A randomised controlled trial. Res. Develop. Disabil. 2013, 34, 4385–4394. [Google Scholar] [CrossRef] [PubMed]
- Cowley, P.M.; Ploutz-Snyder, L.L.; Baynard, T.; Heffernan, K.S.; Young Jae, S.; Hsu, S.; Fernhall, B. The effect of progressive resistance training on leg strength, aerobic capacity and functional tasks of daily living in persons with Down syndrome. Disabil. Rehab. 2011, 33, 2229–2236. [Google Scholar] [CrossRef] [PubMed]
- Shields, N.; Taylor, N.F.; Dodd, K.J. Effects of a community-based progressive resistance training program on muscle performance and physical function in adults with Down syndrome: A randomized controlled trial. Arch. Phys. Med. Rehab. 2008, 89, 1215–1220. [Google Scholar] [CrossRef]
- Dunsky, A.; Abu-Rukun, M.; Tsuk, S.; Dwolatzky, T.; Carasso, R.; Netz, Y. The effects of a resistance vs. an aerobic single session on attention and executive functioning in adults. PLoS ONE 2017, 12, e0179799. [Google Scholar] [CrossRef] [PubMed]
- Kamijo, K.; Takeda, Y. Regular physical activity improves executive function during task switching in young adults. Intern. J. Psychophys. 2010, 75, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Guarino, A.; Forte, G.; Giovannoli, J.; Casagrande, M. Executive functions in the elderly with mild cognitive impairment: A systematic review on motor and cognitive inhibition, conflict control and cognitive flexibility. Aging Mental Health 2020, 24, 1028–1045. [Google Scholar] [CrossRef]
- Chang, Y.-K.; Tsai, Y.-J.; Chen, T.-T.; Hung, T.-M. The impacts of coordinative exercise on executive function in kindergarten children: An ERP study. Exp. Brain Res. 2013, 225, 187–196. [Google Scholar] [CrossRef]
- Korkman, M.; Kirk, U.; Kemp, S. NEPSY: A Developmental Neuropsychological Assessment; The Psychological Corporation: San Antonio, TX, USA, 1998. [Google Scholar]
- García-Alba, J.; Esteba-Castillo, S.; Castellanos-López, M.; Rodríguez-Hidalgo, E.; Ribas-Vidal, N.; Moldenhauer-Díaz, F.; Novell-Alsina, R. Validation and normalization of the Tower of London-Drexel University Test 2nd Edition in an adult population with intellectual disability. Span. J. Psychol. 2017, 20, E32. [Google Scholar] [CrossRef]
- Holzapfel, S.D.; Ringenbach, S.D.; Mulvey, G.M.; Sandoval-Menendez, A.M.; Cook, M.R.; Ganger, R.O.; Bennett, K. Improvements in manual dexterity relate to improvements in cognitive planning after assisted cycling therapy (ACT) in adolescents with down syndrome. Res. Dev. Disabil. 2015, 45, 261–270. [Google Scholar] [CrossRef]
- Best, J.R. Effects of physical activity on children’s executive function: Contributions of experimental research on aerobic exercise. Dev. Rev. 2010, 30, 331–351. [Google Scholar] [CrossRef]
- Pesce, C. Shifting the focus from quantitative to qualitative exercise characteristics in exercise and cognition research. J. Sport Exerc. Psychol. 2012, 34, 766–786. [Google Scholar] [CrossRef]
- Wilke, J.; Giesche, F.; Klier, K.; Vogt, L.; Herrmann, E.; Banzer, W. Acute Effects of Resistance Exercise on Cognitive Function in Healthy Adults: A Systematic Review with Multilevel Meta-Analysis. Sports Med. 2019, 49, 905–916. [Google Scholar] [CrossRef]
- Landrigan, J.F.; Bell, T.; Crowe, M.; Clay, O.J.; Mirman, D. Lifting cognition: A meta-analysis of effects of resistance exercise on cognition. Psychol. Res. 2019, 84, 1167–1183. [Google Scholar] [CrossRef]
- Tsuk, S.; Netz, Y.; Dunsky, A.; Zeev, A.; Carasso, R.; Dwolatzky, T.; Salem, R.; Behar, S.; Rotstein, A. The acute effect of exercise on executive function and attention: Resistance versus aerobic exercise. Adv. Cog. Psychol. 2019, 15, 208–215. [Google Scholar] [CrossRef]
- Formenti, D.; Cavaggioni, L.; Duca, M.; Trecroci, A.; Rapelli, M.; Alberti, G.; Komar, J.; Iodice, P. Acute effect of exercise on cognitive performance in middle-aged adults: Aerobic versus balance. J. Phys. Act. Health 2020, 17, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Rogge, A.-K.; Röder, B.; Zech, A.; Nagel, V.; Hollander, K.; Braumann, K.-M.; Hötting, K. Balance training improves memory and spatial cognition in healthy adults. Sci. Rep. 2017, 7. [Google Scholar] [CrossRef]
- Benzing, V.; Schmidt, M.; Jager, K.; Egger, F.; Conzelmann, A.; Roebers, C. A classroom intervention to improve executive functions in late primary school children: Too ‘old’ for improvements? Br. J. Ed. Psychol. 2019, 89, 225–238. [Google Scholar] [CrossRef]
- Chen, C.; Ringenbach, S. Dose–response relationship between intensity of exercise and cognitive performance in individuals with Down syndrome: A preliminary study. J. Intellect Disabil. Res. 2016, 60, 606–614. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean | Standard Deviation | |||
|---|---|---|---|---|
| Chronological Age | 26 years 3 months | 5 years 2 months | ||
| Mental Age | 6 years 2 months | 4 years 5 months | ||
| BMI | 33.6 | 9.12 | ||
| Sex | Male | Female | ||
| 8 | 6 | |||
| Ethnicity | White | African American | Hispanic | Native American |
| 10 | 1 | 2 | 1 | |
| Resistance Training | ||||||||
|---|---|---|---|---|---|---|---|---|
| Total Repetitions | Percent of Max (%) | Heart Rate (BPM) | RPE | |||||
| M | SD | M | SD | M | SD | M | SD | |
| Leg Press | 16.57 | 1.59 | 70.18 | 5.17 | 100.21 | 15.14 | 1.79 | 0.77 |
| Chest Press | 16.79 | 1.78 | 68.92 | 6.23 | 104.64 | 17.14 | 2.14 | 1.06 |
| Lat Pulldown | 17.14 | 2.47 | 73.04 | 10.78 | 102.93 | 14.63 | 2.43 | 1.12 |
| Seated Row | 17.14 | 1.96 | 67.76 | 7.72 | 104.71 | 17.65 | 2.29 | 0.88 |
| Leg Curl | 16.71 | 1.79 | 71.12 | 10.42 | 104.93 | 19.19 | 2.43 | 1.12 |
| Shoulder Press | 16.79 | 1.61 | 67.67 | 10.31 | 108.36 | 19.10 | 2.64 | 1.17 |
| Assisted Cycling Therapy | ||||||||
| Average Cadence (RPM) | % of Voluntary Cadence | Heart Rate (BPM) | RPE | |||||
| ACT | 64.36 | 22.53 | 128 | 16 | 91.31 | 17.08 | 1.5 | 0.66 |
| No Training | ||||||||
| Heart Rate (BPM) | RPE | |||||||
| NT | 75.88 * | 9.82 | 1.64 | 0.71 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ringenbach, S.; Arnold, N.; Myer, B.; Hayes, C.; Nam, K.; Chen, C.-C. Executive Function Improves Following Acute Exercise in Adults with Down Syndrome. Brain Sci. 2021, 11, 620. https://doi.org/10.3390/brainsci11050620
Ringenbach S, Arnold N, Myer B, Hayes C, Nam K, Chen C-C. Executive Function Improves Following Acute Exercise in Adults with Down Syndrome. Brain Sciences. 2021; 11(5):620. https://doi.org/10.3390/brainsci11050620
Chicago/Turabian StyleRingenbach, Shannon, Nathanial Arnold, Brandon Myer, Claire Hayes, Kahyun Nam, and Chih-Chia Chen. 2021. "Executive Function Improves Following Acute Exercise in Adults with Down Syndrome" Brain Sciences 11, no. 5: 620. https://doi.org/10.3390/brainsci11050620
APA StyleRingenbach, S., Arnold, N., Myer, B., Hayes, C., Nam, K., & Chen, C.-C. (2021). Executive Function Improves Following Acute Exercise in Adults with Down Syndrome. Brain Sciences, 11(5), 620. https://doi.org/10.3390/brainsci11050620