Brain Abscess Masquerading as Brain Infarction


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
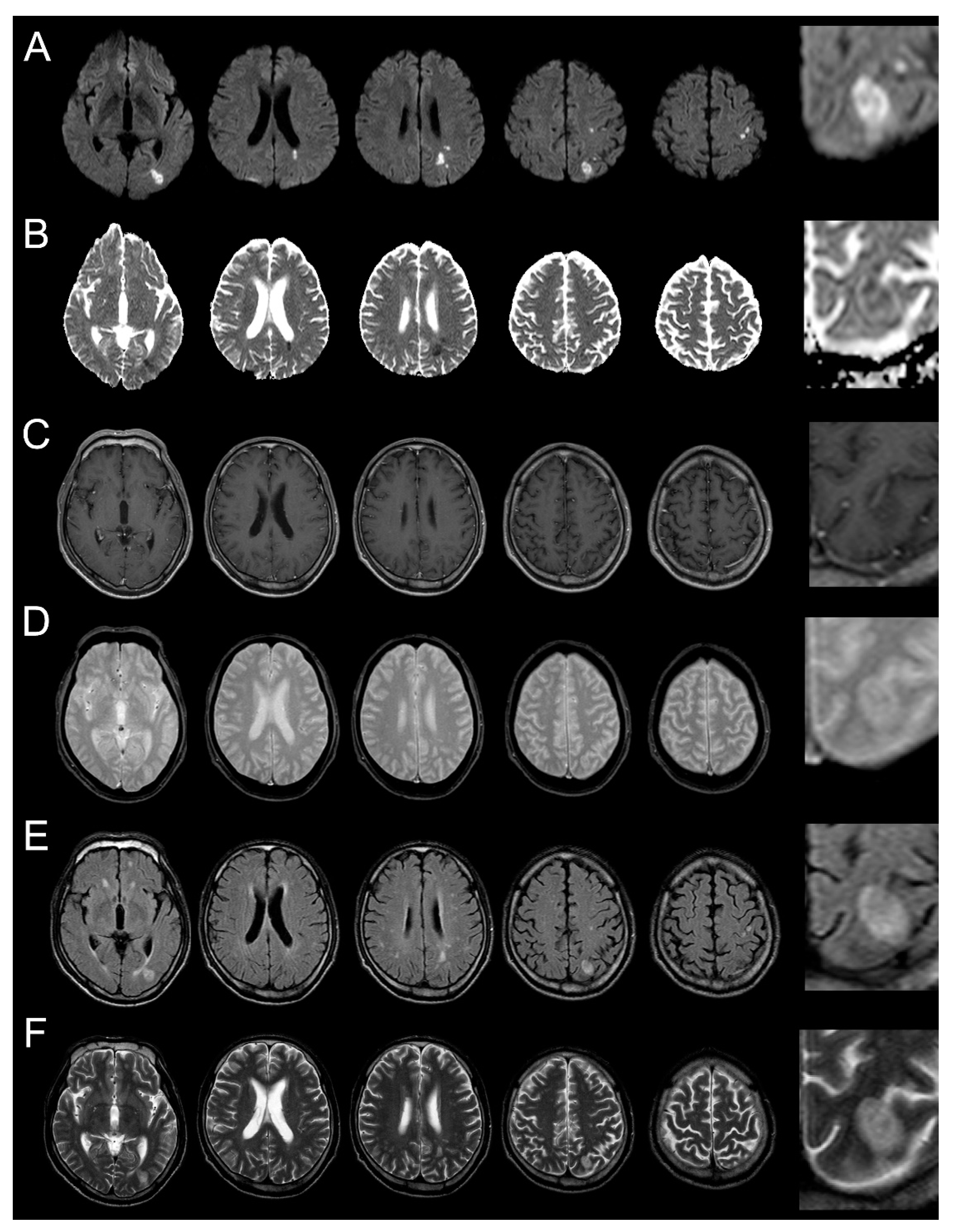
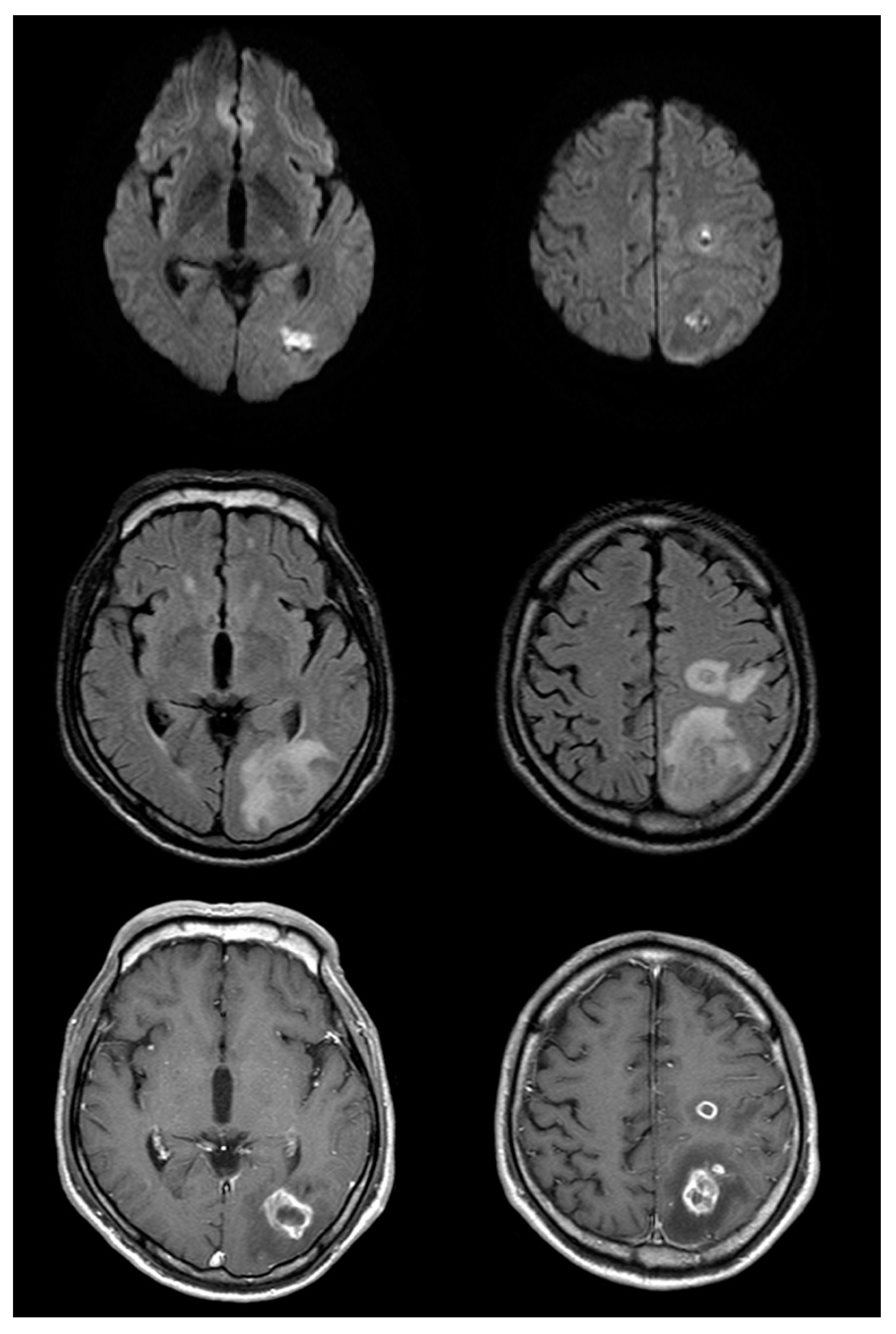
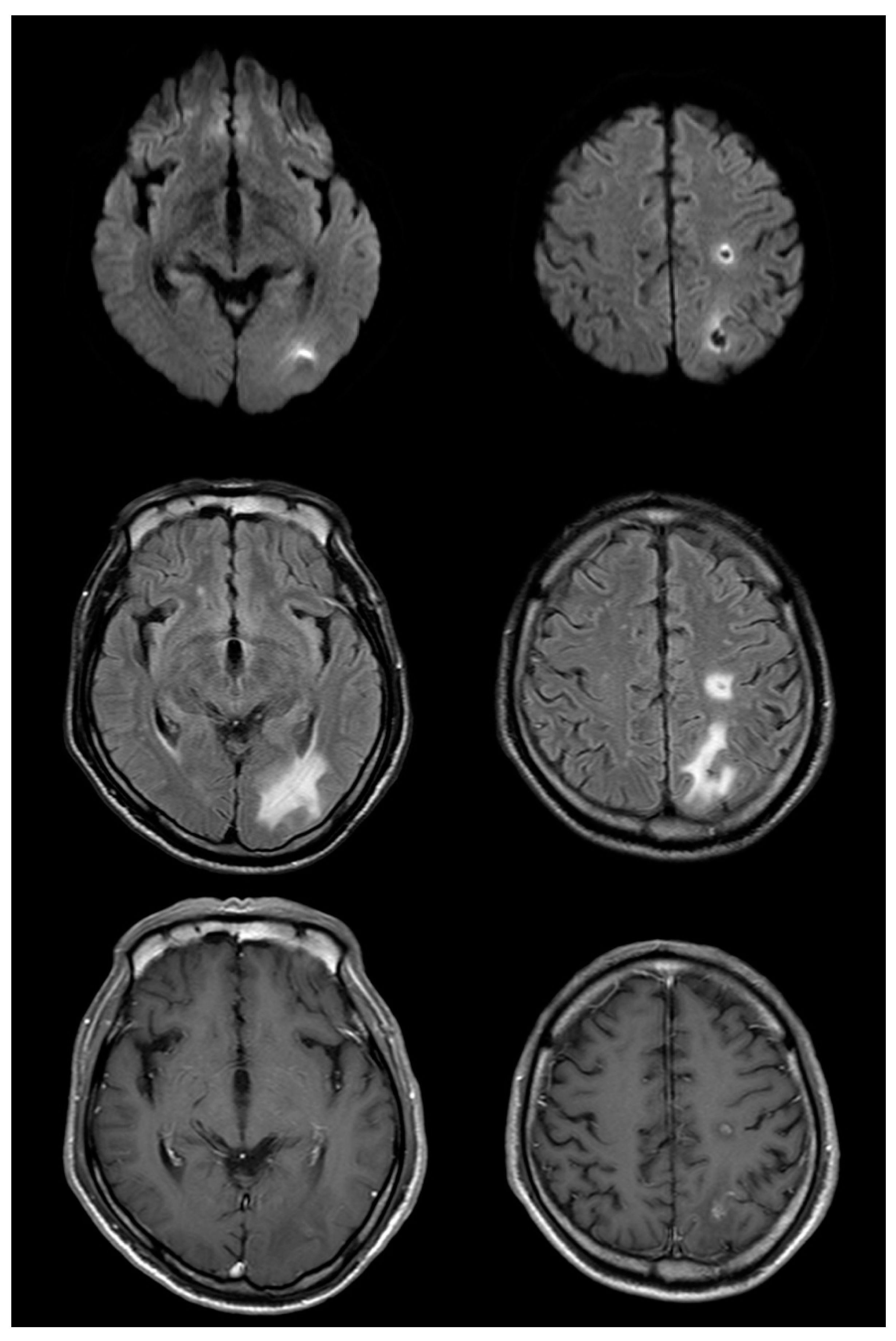
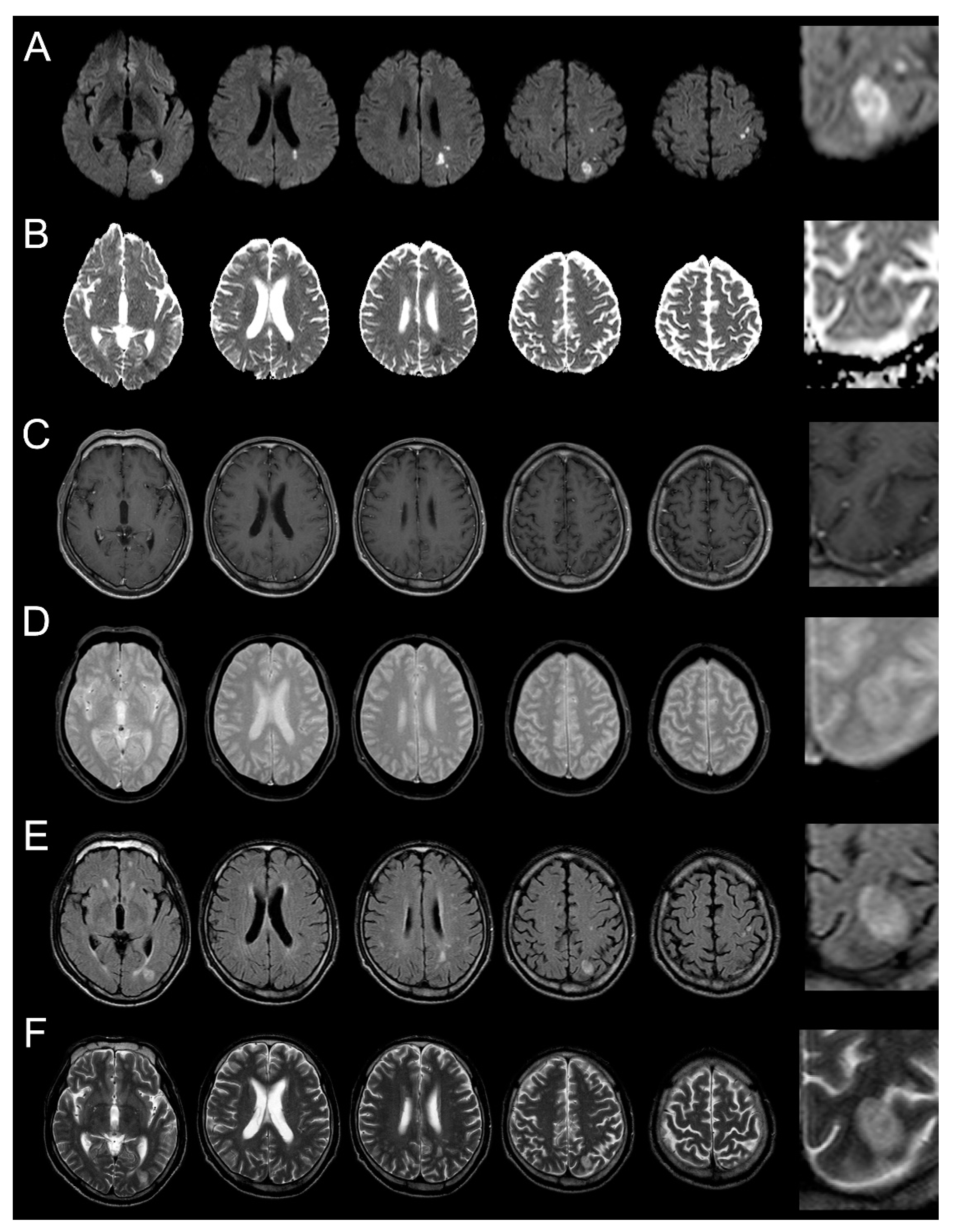
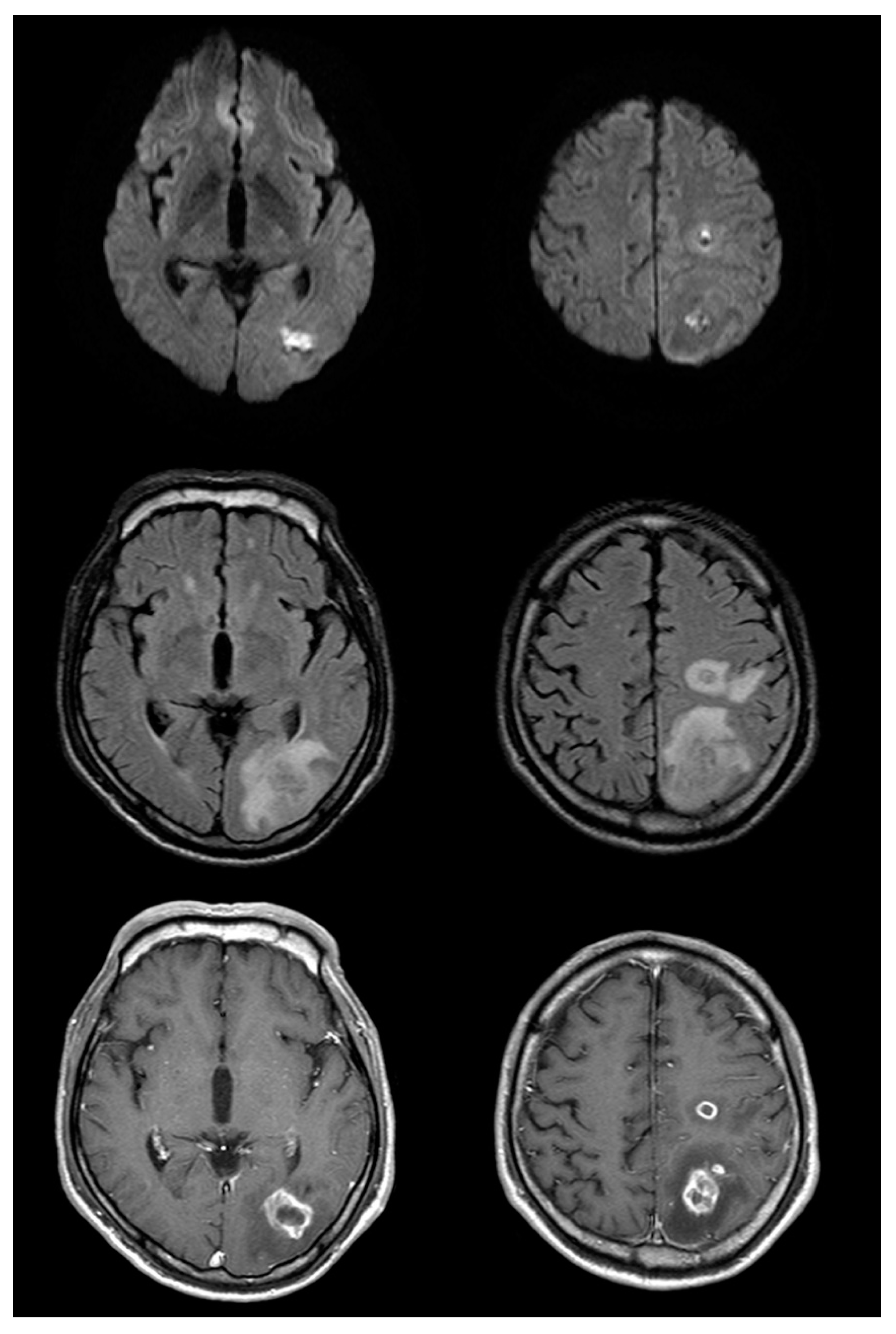
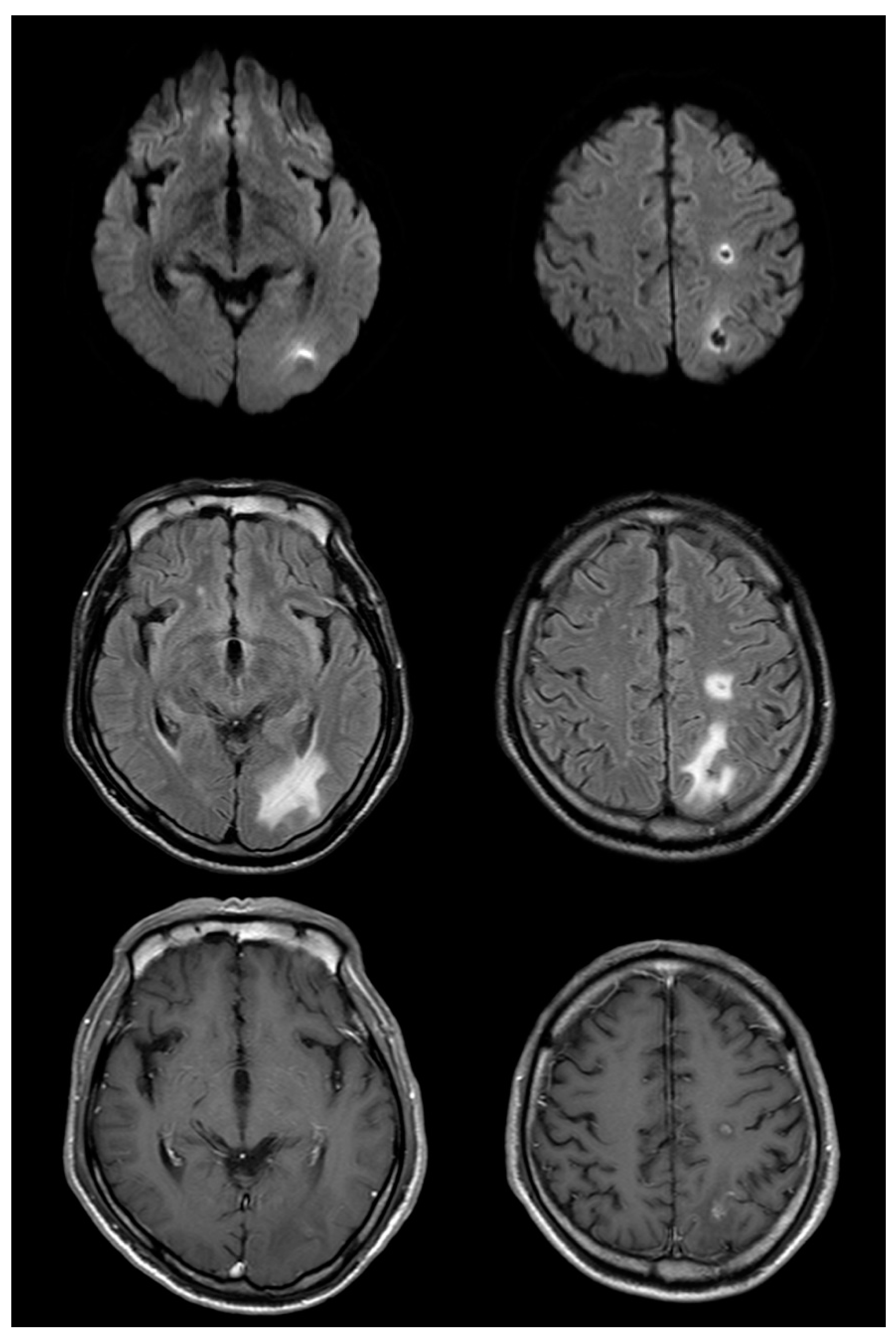
2. Case Presentation
3. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Verma, A. Infections of the nervous system. In Neurology in Clinical Practice, 5th ed.; Bradley, W., Daroff, R., Fenichel, G., Jankovic, J., Eds.; Butterworth-Heinemann: Oxford, UK, 2007; pp. 1428–1431. [Google Scholar]
- Hogan, R.E. Sudden ‘stroke-like’ onset of hemiparesis due to bacterial brain abscess. Neurology 1994, 44, 569–570. [Google Scholar] [CrossRef] [PubMed]
- Shintani, S.; Tsuruoka, S.; Koumo, Y.; Shiigai, T. Sudden ‘stroke-like’ onset of homonymous hemianopsia due to bacterial brain abscess. J. Neurol. Sci. 1996, 143, 190–194. [Google Scholar] [CrossRef]
- Mori, K.; Miwa, K.; Hara, S.; Nakashima, T.; Ueda, T.; Yokoyama, K.; Sakai, N. A case of a bacterial brain abscess presenting as symptoms of ‘sudden stroke-like’ onset. No Shinkei Geka 2003, 31, 443–448. [Google Scholar] [PubMed]
- Borm, W.; Gleixner, M. Nocardia brain abscess misinterpreted as cerebral infarction. J. Clin. Neurosci. 2003, 10, 130–132. [Google Scholar] [CrossRef]
- Bhatt, A.; Masih, A.; Grothous, H.F.; Farooq, M.U.; Naravetla, B.; Kassab, M.Y. Diffusion-weighted imaging: Not all that glitters is gold. South. Med. J. 2009, 102, 923–928. [Google Scholar] [CrossRef] [PubMed]
- Han, K.-T.; Choi, D.S.; Ryoo, J.W.; Cho, J.M.; Jeon, K.N.; Bae, K.S.; You, J.J.; Chung, S.H.; Koh, E.H.; Park, K.-J. Diffusion-weighted MR imaging of pyogenic intraventricular empyema. Neuroradiology 2007, 49, 813–818. [Google Scholar] [CrossRef] [PubMed]
- Lai, P.-H.; Hsu, S.-S.; Ding, S.-W.; Ko, C.-W.; Fu, J.-H.; Weng, M.-J.; Yeh, L.-R.; Wu, M.-T.; Liang, H.-L.; Chen, C.-K.; et al. Proton magnetic resonance spectroscopy and diffusion-weighted imaging in intracranial cystic mass lesions. Surg. Neurol. 2007, 68 (Suppl. 1), S25–S36. [Google Scholar] [CrossRef] [PubMed]
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeong, D.-E.; Lee, J. Brain Abscess Masquerading as Brain Infarction. Brain Sci. 2020, 10, 440. https://doi.org/10.3390/brainsci10070440
Jeong D-E, Lee J. Brain Abscess Masquerading as Brain Infarction. Brain Sciences. 2020; 10(7):440. https://doi.org/10.3390/brainsci10070440
Chicago/Turabian StyleJeong, Da-Eun, and Jun Lee. 2020. "Brain Abscess Masquerading as Brain Infarction" Brain Sciences 10, no. 7: 440. https://doi.org/10.3390/brainsci10070440
APA StyleJeong, D.-E., & Lee, J. (2020). Brain Abscess Masquerading as Brain Infarction. Brain Sciences, 10(7), 440. https://doi.org/10.3390/brainsci10070440