Increased Time Difference between Imagined and Physical Walking in Older Adults at a High Risk of Falling


{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measurement
2.3. Statistics Analysis
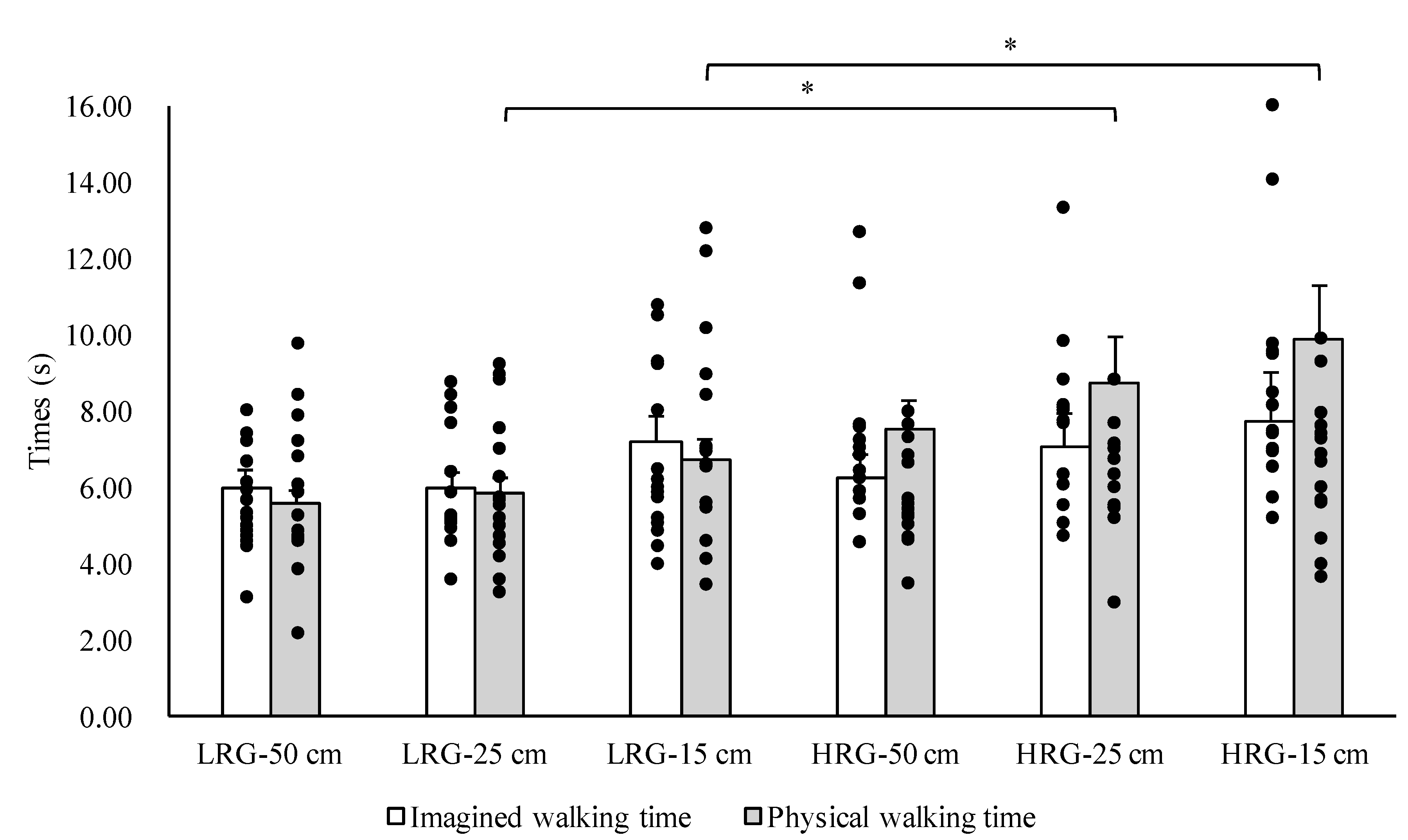
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Jeannerod, M. The representing brain: Neural correlates of motor intention and imagery. Behav. Brain Sci. 1994, 17, 187–245. [Google Scholar] [CrossRef]
- Grush, R. The emulation theory of representation: Motor control, imagery, and perception. Behav. Brain Sci. 2004, 27, 377–396. [Google Scholar] [CrossRef]
- Glover, S.; Baran, M. The motor-cognitive model of motor imagery: Evidence from timing errors in simulated reaching and grasping. J. Exp. Psychol. Hum. Percept. Perform. 2017, 43, 1359–1375. [Google Scholar] [CrossRef] [PubMed]
- Jeannerod, M. Neural simulation of action: A unifying mechanism for motor cognition. Neuroimage 2001, 14, 103–109. [Google Scholar] [CrossRef]
- Hardwick, R.M.; Caspers, S.; Eickhoff, S.B.; Swinnen, S.P. Neural correlates of action: Comparing meta-analyses of imagery, observation, and execution. Neurosci. Biobehav. Rev. 2018, 94, 31–44. [Google Scholar] [CrossRef]
- Guillot, A.; Hoyek, N.; Louis, M.; Collet, C. Understanding the timing of motor imagery: Recent findings and future directions. Int. Rev. Sport Exerc. Psychol. 2012, 5, 3–22. [Google Scholar] [CrossRef]
- Decety, J.; Jeannerod, M.; Prablanc, C. The timing of mentally represented actions. Behav. Brain Res. 1989, 34, 35–42. [Google Scholar] [CrossRef]
- Collet, C.; Guillot, A.; Lebon, F.; MacIntyre, T.; Moran, A. Measuring motor imagery using psychometric, behavioral, and psychophysiological tools. Exerc. Sport Sci. Rev. 2011, 39, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Malouin, F.; Richards, C.L.; Durand, A.; Doyon, J. Reliability of mental chronometry for assessing motor imagery ability after stroke. Arch. Phys. Med. Rehabil. 2008, 89, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Saimpont, A.; Malouin, F.; Tousignant, B.; Jackson, P.L. Motor imagery and aging. J. Mot. Behav. 2013, 45, 21–28. [Google Scholar] [CrossRef]
- Schott, N.; Munzert, J. Temporal accuracy of motor imagery in older women. Int. J. Sport Psychol. 2007, 38, 304–320. [Google Scholar]
- Schott, N. Age-related differences in motor imagery: Working memory as a mediator. Exp. Aging Res. 2012, 38, 559–583. [Google Scholar] [CrossRef] [PubMed]
- Personnier, P.; Kubicki, A.; Laroche, D.; Papaxanthis, C. Temporal features of imagined locomotion in normal aging. Neurosci. Lett. 2010, 476, 146–149. [Google Scholar] [CrossRef] [PubMed]
- Nakano, H.; Murata, S.; Shiraiwa, K.; Iwase, H.; Kodama, T. Temporal characteristics of imagined and actual walking in frail older adults. Aging Clin. Exp. Res. 2018, 30, 1453–1457. [Google Scholar] [CrossRef]
- Beauchet, O.; Annweiler, C.; Assal, F.; Bridenbaugh, S.; Herrmann, F.R.; Kressig, R.W.; Allali, G. Imagined Timed Up & Go test: A new tool to assess higher-level gait and balance disorders in older adults? J. Neurol. Sci. 2010, 294, 102–106. [Google Scholar] [PubMed]
- Grenier, S.; Richard-Devantoy, S.; Nadeau, A.; Payette, M.C.; Benyebdri, F.; Duhaime, M.B.; Gunther, B.; Beauchet, O. The association between fear of falling and motor imagery abilities in older community-dwelling individuals. Maturitas 2018, 110, 18–20. [Google Scholar] [CrossRef]
- Sakurai, R.; Fujiwara, Y.; Yasunaga, M.; Suzuki, H.; Sakuma, N.; Imanaka, K.; Montero-Odasso, M. Older adults with fear of falling show deficits in motor imagery of gait. J. Nutr. Health Aging 2017, 21, 721–726. [Google Scholar] [CrossRef]
- Greenberg, S.A. Analysis of measurement tools of fear of falling for high-risk, community-dwelling older adults. Clin. Nurs. Res. 2012, 21, 113–130. [Google Scholar] [CrossRef]
- Sakurai, R.; Fujiwara, Y.; Yasunaga, M.; Suzuki, H.; Murayama, Y.; Imanaka, K.; Kanosue, K.; Ishii, K. Neural correlates of older adults’ self-overestimation of stepping-over ability. Age 2016, 38, 351–361. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. Health and Welfare Services for the Elderly. Available online: https://www.mhlw.go.jp/english/wp/wp-hw11/dl/10e.pdf (accessed on 8 January 2020).
- Saito, T.; Izawa, K.P.; Watanabe, S. The relative and absolute reliability of the Functional Independence and Difficulty Scale in community-dwelling frail elderly Japanese people using long-term care insurance services. Aging Clin. Exp. Res. 2017, 29, 549–556. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G * Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Ogawa, M.; Loenneke, J.P.; Thiebaud, R.S.; Loftin, M.; Mitsukawa, N. Association between site-specific muscle loss of lower body and one-leg standing balance in active women: The HIREGASAKI study. Geriatr. Gerontol. Int. 2014, 14, 381–387. [Google Scholar] [PubMed]
- Vellas, B.J.; Wayne, S.J.; Romero, L.; Baumgartner, R.N.; Rubenstein, L.Z.; Garry, P.J. One-leg balance is an important predictor of injurious falls in older persons. J. Am. Geriatr. Soc. 1997, 45, 735–738. [Google Scholar] [CrossRef]
- American Geriatrics Society; British Geriatrics Society; American Academy of Orthopaedic Surgeons Panel on Falls Prevention. Guideline for the prevention of falls in older persons. J. Am. Geriatr. Soc. 2001, 49, 664–672. [Google Scholar] [CrossRef]
- Allali, G.; van der Meulen, M.; Beauchet, O.; Rieger, S.W.; Vuilleumier, P.; Assal, F. The neural basis of age-related changes in motor imagery of gait: An fMRI study. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 1389–1398. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: London, UK, 1988. [Google Scholar]
- Kalicinski, M.; Kempe, M.; Bock, O. Motor imagery: Effects of age, task complexity, and task setting. Exp. Aging Res. 2015, 41, 25–38. [Google Scholar] [CrossRef]
- Boyle, P.A.; Buchman, A.S.; Wilson, R.S.; Leurgans, S.E.; Bennett, D.A. Physical frailty is associated with incident mild cognitive impairment in community-based older persons. J. Am. Geriatr. Soc. 2010, 58, 248–255. [Google Scholar] [CrossRef]
- Sakurai, R.; Fujiwara, Y.; Yasunaga, M.; Suzuki, H.; Kanosue, K.; Montero-Odasso, M.; Ishii, K. Association between hypometabolism in the supplementary motor area and fear of falling in older adults. Front. Aging Neurosci. 2017, 9, 251. [Google Scholar] [CrossRef]
- Sakurai, R.; Fujiwara, Y.; Sakuma, N.; Suzuki, H.; Ishihara, M.; Higuchi, T.; Imanaka, K. Influential factors affecting age-related self-overestimation of step-over ability: Focusing on frequency of going outdoors and executive function. Arch. Gerontol. Geriatr. 2014, 59, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, A.; Hori, H.; Tamura, T.; Hirai, T.; Umemura, T.; Iguchi, F.; Sawa, S.; Ogawa, K.; Sato, K.; Kusaka, Y. Relationships between estimation errors and falls in healthy aged dwellers. Gerontology 2015, 61, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Ridderinkhof, K.R.; Ullsperger, M.; Crone, E.A.; Nieuwenhuis, S. The role of the medial frontal cortex in cognitive control. Science 2004, 306, 443–447. [Google Scholar] [PubMed]
- Shany-Ur, T.; Lin, N.; Rosen, H.J.; Sollberger, M.; Miller, B.L.; Rankin, K.P. Self-awareness in neurodegenerative disease relies on neural structures mediating reward-driven attention. Brain 2014, 137, 2368–2381. [Google Scholar] [PubMed]
- O’Shea, H.; Moran, A. Does Motor Simulation Theory Explain the Cognitive Mechanisms Underlying Motor Imagery? A Critical Review. Front. Hum. Neurosci. 2017, 11, 72. [Google Scholar] [CrossRef]



© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakano, H.; Murata, S.; Shiraiwa, K.; Nonaka, K. Increased Time Difference between Imagined and Physical Walking in Older Adults at a High Risk of Falling. Brain Sci. 2020, 10, 332. https://doi.org/10.3390/brainsci10060332
Nakano H, Murata S, Shiraiwa K, Nonaka K. Increased Time Difference between Imagined and Physical Walking in Older Adults at a High Risk of Falling. Brain Sciences. 2020; 10(6):332. https://doi.org/10.3390/brainsci10060332
Chicago/Turabian StyleNakano, Hideki, Shin Murata, Kayoko Shiraiwa, and Koji Nonaka. 2020. "Increased Time Difference between Imagined and Physical Walking in Older Adults at a High Risk of Falling" Brain Sciences 10, no. 6: 332. https://doi.org/10.3390/brainsci10060332
APA StyleNakano, H., Murata, S., Shiraiwa, K., & Nonaka, K. (2020). Increased Time Difference between Imagined and Physical Walking in Older Adults at a High Risk of Falling. Brain Sciences, 10(6), 332. https://doi.org/10.3390/brainsci10060332