Effect of the Type and Number of Adverse Childhood Experiences and the Timing of Adverse Experiences on Clinical Outcomes in Individuals with Bipolar Disorder


Abstract
1. Introduction
2. Methods
2.1. Participants
2.2. Diagnostic Interview for Genetic Studies and Childhood Life Events Scale
2.3. Statistical Analyses
3. Results
3.1. Relationship between the Number of Adverse Childhood Experiences and the Clinical Outcomes of Bipolar Disorder
3.2. Effect of the Type of Adverse Childhood Experiences and the Timing of Adverse Experiences on the Clinical Outcomes of Bipolar Disorder
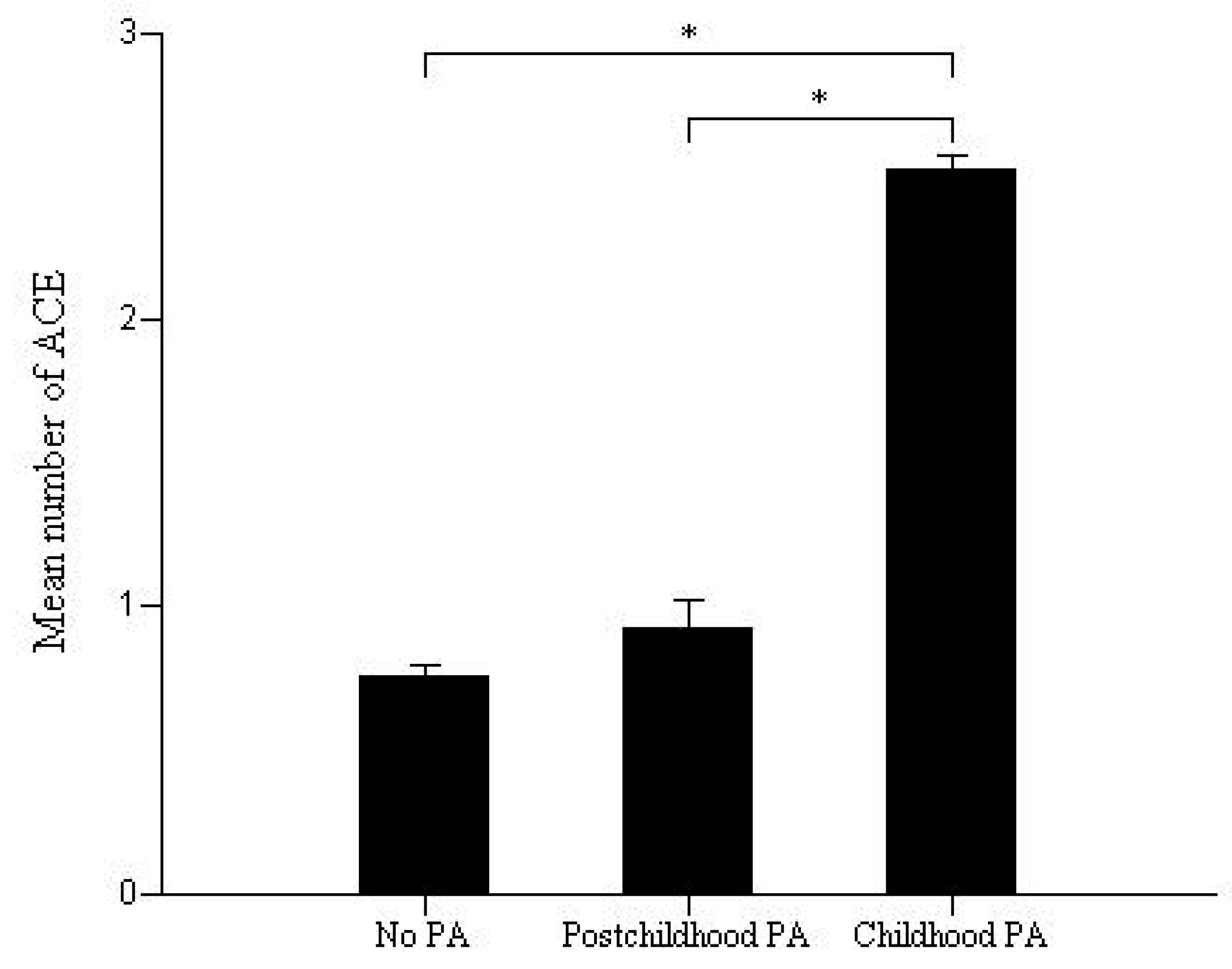
3.3. Effect of Physical Abuse and the Number of Adverse Childhood Experiences on the Clinical Outcomes of Bipolar Disorder
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Koss, M.P.; Marks, J.S. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The adverse childhood experiences (ace) study. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [PubMed]
- Aas, M.; Henry, C.; Andreassen, O.A.; Bellivier, F.; Melle, I.; Etain, B. The role of childhood trauma in bipolar disorders. Int. J. Bipolar Disord. 2016, 4, 2. [Google Scholar] [PubMed]
- Bernstein, D.P.; Fink, L.; Handelsman, L.; Foote, J.; Lovejoy, M.; Wenzel, K.; Sapareto, E.; Ruggiero, J. Initial reliability and validity of a new retrospective measure of child abuse and neglect. Am. J. Psychiatry 1994, 151, 1132–1136. [Google Scholar]
- Garno, J.L.; Goldberg, J.F.; Ramirez, P.M.; Ritzler, B.A. Impact of childhood abuse on the clinical course of bipolar disorder. Br. J. Psychiatry 2005, 186, 121–125. [Google Scholar] [PubMed]
- Janssen, I.; Krabbendam, L.; Bak, M.; Hanssen, M.; Vollebergh, W.; de Graaf, R.; van Os, J. Childhood abuse as a risk factor for psychotic experiences. Acta Psychiatr. Scand. 2004, 109, 38–45. [Google Scholar]
- Etain, B.; Aas, M.; Andreassen, O.A.; Lorentzen, S.; Dieset, I.; Gard, S.; Kahn, J.P.; Bellivier, F.; Leboyer, M.; Melle, I.; et al. Childhood trauma is associated with severe clinical characteristics of bipolar disorders. J. Clin. Psychiatry 2013, 74, 991–998. [Google Scholar]
- Beyer, J.L.; Weisler, R.H. Suicide behaviors in bipolar disorder: A review and update for the clinician. Psychiatr. Clin. North Am. 2016, 39, 111–123. [Google Scholar]
- Daruy-Filho, L.; Brietzke, E.; Lafer, B.; Grassi-Oliveira, R. Childhood maltreatment and clinical outcomes of bipolar disorder. Acta Psychiatr. Scand. 2011, 124, 427–434. [Google Scholar]
- Anand, A.; Koller, D.L.; Lawson, W.B.; Gershon, E.S.; Nurnberger, J.I. Genetic and childhood trauma interaction effect on age of onset in bipolar disorder: An exploratory analysis. J. Affect. Disord. 2015, 179, 1–5. [Google Scholar]
- Smith, E.N.; Bloss, C.S.; Badner, J.A.; Barrett, T.; Belmonte, P.L.; Berrettini, W.; Byerley, W.; Coryell, W.; Craig, D.; Edenberg, H.J.; et al. Genome-wide association study of bipolar disorder in european american and african american individuals. Mol. Psychiatry 2009, 14, 755–763. [Google Scholar]
- Nurnberger, J.I., Jr.; Blehar, M.C.; Kaufmann, C.A.; York-Cooler, C.; Simpson, S.G.; Harkavy-Friedman, J.; Severe, J.B.; Malaspina, D.; Reich, T. Diagnostic interview for genetic studies. Rationale, unique features, and training. Nimh genetics initiative. Arch. Gen. Psychiatry 1994, 51, 849–859. [Google Scholar] [PubMed]
- Preisig, M.; Fenton, B.T.; Matthey, M.L.; Berney, A.; Ferrero, F. Diagnostic interview for genetic studies (digs): Inter-rater and test-retest reliability of the french version. Eur. Arch. Psychiatry Clin. Neurosci. 1999, 249, 174–179. [Google Scholar] [PubMed]
- Dualibe, A.L.; Osorio, F.L. Bipolar disorder and early emotional trauma: A critical literature review on indicators of prevalence rates and clinical outcomes. Harv. Rev. Psychiatry 2017, 25, 198–208. [Google Scholar] [PubMed]
- Bebbington, P.E.; Bhugra, D.; Brugha, T.; Singleton, N.; Farrell, M.; Jenkins, R.; Lewis, G.; Meltzer, H. Psychosis, victimisation and childhood disadvantage: Evidence from the second British National Survey of Psychiatric Morbidity. Br. J. Psychiatry 2004, 185, 220–226. [Google Scholar] [PubMed]
- Hammersley, P.; Dias, A.; Todd, G.; Bowen-Jones, K.; Reilly, B.; Bentall, R.P. Childhood trauma and hallucinations in bipolar affective disorder: Preliminary investigation. Br. J. Psychiatry 2003, 182, 543–547. [Google Scholar]
- Li, X.B.; Liu, J.T.; Zhu, X.Z.; Zhang, L.; Tang, Y.L.; Wang, C.Y. Childhood trauma associates with clinical features of bipolar disorder in a sample of chinese patients. J. Affect. Disord. 2014, 168, 58–63. [Google Scholar]
- Leverich, G.S.; Post, R.M. Course of bipolar illness after history of childhood trauma. Lancet 2006, 367, 1040–1042. [Google Scholar]
- Leverich, G.S.; McElroy, S.L.; Suppes, T.; Keck, P.E., Jr.; Denicoff, K.D.; Nolen, W.A.; Altshuler, L.L.; Rush, A.J.; Kupka, R.; Frye, M.A.; et al. Early physical and sexual abuse associated with an adverse course of bipolar illness. Biol. Psychiatry 2002, 51, 288–297. [Google Scholar]
- Weber, S.; Jud, A.; Landolt, M.A. Quality of life in maltreated children and adult survivors of child maltreatment: A systematic review. Qual. Life Res. 2016, 25, 237–255. [Google Scholar]
- Shevlin, M.; Dorahy, M.J.; Adamson, G. Trauma and psychosis: An analysis of the national comorbidity survey. Am. J. Psychiatry 2007, 164, 166–169. [Google Scholar]
- Mello, M.F.; Faria, A.A.; Mello, A.F.; Carpenter, L.L.; Tyrka, A.R.; Price, L.H. Childhood maltreatment and adult psychopathology: Pathways to hypothalamic-pituitary-adrenal axis dysfunction. Braz. J. Psychiatry 2009, 31, S41–S48. [Google Scholar] [PubMed]
- Chen, Y.; Baram, T.Z. Toward understanding how early-life stress reprograms cognitive and emotional brain networks. Neuropsychopharmacology 2016, 41, 197–206. [Google Scholar] [PubMed]
- Paquola, C.; Bennett, M.R.; Lagopoulos, J. Understanding heterogeneity in grey matter research of adults with childhood maltreatment-a meta-analysis and review. Neurosci. Biobehav. Rev. 2016, 69, 299–312. [Google Scholar] [PubMed]
- Carballedo, A.; Lisiecka, D.; Fagan, A.; Saleh, K.; Ferguson, Y.; Connolly, G.; Meaney, J.; Frodl, T. Early life adversity is associated with brain changes in subjects at family risk for depression. World J. Biol. Psychiatry 2012, 13, 569–578. [Google Scholar]
- Jaworska-Andryszewska, P.; Rybakowski, J.K. Childhood trauma in mood disorders: Neurobiological mechanisms and implications for treatment. Pharmacol. Rep. 2019, 71, 112–120. [Google Scholar] [PubMed]
- Romero, S.; Birmaher, B.; Axelson, D.; Goldstein, T.; Goldstein, B.I.; Gill, M.K.; Iosif, A.M.; Strober, M.A.; Hunt, J.; Esposito-Smythers, C.; et al. Prevalence and correlates of physical and sexual abuse in children and adolescents with bipolar disorder. J. Affect. Disord. 2009, 112, 144–150. [Google Scholar] [PubMed]
- Schaffer, A.; Isometsa, E.T.; Tondo, L.; D, H.M.; Turecki, G.; Reis, C.; Cassidy, F.; Sinyor, M.; Azorin, J.M.; Kessing, L.V.; et al. International society for bipolar disorders task force on suicide: Meta-analyses and meta-regression of correlates of suicide attempts and suicide deaths in bipolar disorder. Bipolar Disord. 2015, 17, 1–16. [Google Scholar]


{kind=link}
| Score | Chronicity | Psychotic Symptoms | Mixed Symptoms | Suicidality | General Impact of Illness on Life Functioning | Substance Misuse |
|---|---|---|---|---|---|---|
| 0 | never | never | never | never | never | never |
| 1 | duration < 2 years | fleeting | mixed symptoms | passive death wishes | employment | no dependence |
| 2 | duration ≥ 2 years | one episode | ≥ a mixed episode | thought about suicide | employment but not disabled | brief usage |
| 3 | frequent symptoms | ≥2 episodes | acted on ambivalently | disabled but living independently | relapsing | |
| 4 | all episodes | acted on seriously | disabled & not living independently | chronic usage | ||
| 5 | chronic psychosis |
| Variable | Value |
|---|---|
| Age, years (mean ± SD) (age range) | 44.1 ± 13.0 (17–83) |
| Sex ratio, males/females (%) | 36.3/63.7 |
| Race (%) | |
| White | 80.9 |
| Other | 19.1 |
| Illness subtype (%) | |
| Bipolar I | 94.9 |
| Bipolar II | 3.4 |
| Bipolar NOS | 1.7 |
| Mean number of ACEs (CLES score) (mean ± SD) | 1.4 ± 1.5 |
| AAO, years (mean ± SD) | 18.5 ± 9.4 |
| Presence of psychotic episodes (%) | 69.4 |
| History of suicide attempts (%) | 50.9 |
| Presence of substance misuse (%) | 59.3 |
| Presence of mixed symptoms or episodes (%) | 49.6 |
| Mean number of manic episodes (per year) (mean ± SD) | 0.5 ± 1.2 |
| Mean number of depressive episodes (per year) (mean ± SD) | 0.9 ± 2.2 |
| History of physical abuse (%) | 39.3 |
| Frequency of the number of ACEs (%) | |
| 0 | 36.9 |
| 1 | 23.8 |
| 2 | 17.8 |
| ≥3 | 21.5 |
| Variable | Group without ACE | Group with ACE | P |
|---|---|---|---|
| AAO, years (mean ± SD) | 20.1 ± 9.7 | 17.5 ± 9.0 | <0.01a |
| Age at assessment, years (mean ± SD) | 43.7 ± 14.1 | 44.3 ± 12.1 | 0.28b |
| Sex ratio, males/females (%) | 42.5/57.5 | 32.3/67.7 | <0.01c |
| Number of manic episodes* (mean ± SD) | 0.5 ± 0.9 | 0.6 ± 1.4 | 0.30b |
| Number of depressive episodes* (mean ± SD) | 1.0 ± 2.8 | 0.9 ± 1.7 | 0.21b |
| History of psychotic episodes (mean ± SD) | 47.5 | 82.4 | <0.01c |
| History of suicide attempts (%) | 75.7 | 82.4 | <0.01c |
| History of mixed symptoms or episodes (%) | 44.9 | 52.4 | <0.01c |
| Presence of substance misuse (%) | 54.3 | 62.2 | <0.01c |
| Presence of worsening in life functioning (%) | 81.7 | 86.7 | <0.01c |
| Variable | No ACE (n = 987) | One Type of ACE (n = 637) | Two Types of ACE (n = 477) | Three and More Types of ACE (n = 574) | P | Pd |
|---|---|---|---|---|---|---|
| AAO, years (mean ± SD) | 20.1 ± 9.7 | 18.9 ± 9.1 | 17.1 ± 9.1 | 16.3 ± 8.7 | <0.01a | <0.01 |
| Age at assessment, years (mean ± SD) | 43.7 ± 14.1 | 43.0 ± 12.9 | 45.0 ± 11.7 | 45.3 ± 11.3 | 0.057b | NA |
| Sex ratio, males/females (%) | 42.5/57.5 | 31.0/69.0 | 32.3/67.7 | 34.0/66.0 | <0.01c | NA |
| Mean episodes per year (mean ± SD) | 1.5 ± 3.0 | 1.3 ± 2.3 | 1.5 ± 3.1 | 1.5 ± 1.9 | <0.05c | <0.05 |
| History of psychotic episodes (%) | 47.5 | 55.2 | 98.6 | 99.8 | <0.01c | <0.01 |
| History of suicide attempts (%) | 75.7 | 79.8 | 84.1 | 83.9 | <0.01c | <0.01 |
| History of mixed symptoms (%) | 44.9 | 51.8 | 51.5 | 53.8 | <0.01c | <0.01 |
| Presence of substance misuse (%) | 54.3 | 57.2 | 60.3 | 69.6 | <0.01c | <0.01 |
| Presence of worsening in life functioning (%) | 81.7 | 84.0 | 85.3 | 91.4 | <0.01c | <0.01 |
| Variable (Categorical Variables) | Coefficient | SE | Wald | P | OR (95% CI) |
|---|---|---|---|---|---|
| a Psychotic episodes | |||||
| One type of ACE | 0.35 | 0.14 | 6.65 | <0.05 | 1.42 (1.09–1.86) |
| Two types of ACE | 5.80 | 1.01 | 33.22 | <0.01 | 329.24 (45.86–2363.70) |
| Three or more types of ACE | 12.62 | 29.20 | 0.00 | 0.67 | NA |
| a Mixed symptoms | |||||
| One type of ACE | 0.46 | 0.14 | 10.65 | <0.01 | 1.59 (1.20–2.09) |
| Two types of ACE | 0.45 | 0.16 | 8.10 | <0.01 | 1.52 (1.15–2.12) |
| Three or more types of ACE | 0.42 | 0.15 | 7.68 | <0.01 | 1.52 (1.13–2.06) |
| a Suicide attempts | |||||
| One type of ACE | 0.12 | 0.16 | 0.50 | 0.48 | 1.12 (0.82–1.55) |
| Two types of ACE | 0.49 | 0.20 | 6.18 | <0.05 | 1.64 (1.11–2.42) |
| Three or more types of ACE | 0.61 | 0.20 | 9.59 | <0.01 | 1.84 (1.25–2.71) |
| a Substance misuse | |||||
| One type of ACE | 0.17 | 0.14 | 1.55 | 0.21 | 1.19 (0.91–1.56) |
| Two types of ACE | 0.34 | 0.16 | 4.63 | <0.05 | 1.41 (1.03–1.93) |
| Three or more types of ACE | 0.63 | 0.16 | 16.26 | <0.01 | 1.87 (1.38–2.54) |
| a Worse life functioning | |||||
| One type of ACE | 0.29 | 0.18 | 2.51 | 0.11 | 1.33 (0.93–1.89) |
| Two types of ACE | 0.31 | 0.21 | 2.32 | 0.13 | 1.37 (0.91–2.04) |
| Three or more types of ACE | 1.21 | 0.26 | 21.67 | <0.01 | 3.37 (2.02–5.61) |
| Group According to ACEs Type(Frequency, %) | AAO (Years) | Chronicity | Psychosis | Mixed Symptoms | Suicidality | Worsening Function | Substance Misuse |
|---|---|---|---|---|---|---|---|
| Parental loss (7.8) | 19.57 | 2.53 | 2.34** | 0.84 | 2.40 | 2.61a,b,** | 2.35 |
| Sibling loss (5.3) | 17.44 | 2.54 | 2.19a** | 0.82 | 2.23b,** | 2.56 | 2.30 |
| Chronic illness (10.3) | 16.29a,b,** | 2.55 | 2.28** | 0.87 | 2.44 | 2.51b,** | 2.24 |
| Lengthy hospitalization (10.4) | 16.37a,** | 2.58a,* | 2.39** | 0.79 | 2.40b,** | 2.59a,b,** | 2.39a,** |
| Permanent injury or disability (4.8) | 17.69 | 2.59a,b,** | 2.47a,** | 0.85 | 2.42b,** | 2.86a,b,** | 2.30b,* |
| Physical abuse (39.4) | 16.54a,** | 2.54a,** | 2.16a,c** | 0.87** | 2.60a,b,** | 2.54a,** | 2.39a,** |
| Injury or death threat (21.3) | 16.23a,* | 2.58a,b,** | 2.40a,** | 0.89** | 2.67a,b,** | 2.63a,b,** | 2.46a,** |
| Leaving home unexpectedly (16.0) | 17.09 | 2.57a,b,** | 2.44a,** | 0.81* | 2.47* | 2.53a** | 2.33a,** |
| Serious unexpected life change (36.5) | 17.16 | 2.56a,** | 2.27** | 0.84** | 2.49** | 2.50a** | 2.31a,** |
| Variable (Categorical) | Coefficient | SE | Wald | P | OR (95% CI) |
|---|---|---|---|---|---|
| a Psychotic features | |||||
| Post-childhood PA | 0.23 | 0.27 | 6.65 | 0.38 | 1.26 (0.75–2.13) |
| Childhood PA | 1.65 | 0.15 | 33.22 | <0.01 | 5.19 (3.89–6.92) |
| a Mixed symptoms | |||||
| Post-childhood PA | 0.47 | 0.27 | 10.65 | 0.081 | 1.60 (0.94–2.71) |
| Childhood PA | 0.49 | 0.12 | 8.10 | <0.01 | 1.65 (1.30–2.08) |
| a Suicide attempts | |||||
| Post-childhood PA | 0.92 | 0.41 | 0.50 | <0.05 | 2.50 (1.12–5.59) |
| Childhood PA | 0.49 | 0.20 | 6.18 | <0.01 | 1.97 (1.46–2.65) |
| a Substance misuse | |||||
| Post-childhood PA | 0.33 | 0.27 | 1.55 | 0.23 | 1.39 (0.82–2.38) |
| Childhood PA | 0.51 | 0.12 | 4.63 | <0.01 | 1.66 (1.32–2.11) |
| Outcomes (Continuous Variables) | Coefficient | SE | t | P | Goodness of Fit |
|---|---|---|---|---|---|
| a AAO | |||||
| Number of ACE | −0.78 | 0.42 | −4.25 | <0.01 | |
| PA | −2.06 | 0.57 | −3.61 | <0.01 | R2 = 0.043 |
| b Chronicity | |||||
| Number of ACE | 0.038 | 0.013 | 3.05 | <0.01 | |
| PA | 0.03 | 0.037 | 0.81 | 0.42 | R2 = 0.068 |
| b Psychotic episode | |||||
| Number of ACE | 0.42 | 0.025 | 16.92 | <0.01 | |
| PA | 0.11 | 0.074 | 1.42 | 0.16 | R2 = 0.28 |
| b Mixed symptoms | |||||
| Number of ACE | 0.017 | 0.021 | 0.79 | 0.43 | |
| PA | 0.13 | 0.062 | 2.07 | <0.05 | R2 = 0.041 |
| b Suicidality | |||||
| Number of ACE | 0.084 | 0.032 | 2.58 | <0.01 | |
| PA | 0.23 | 0.097 | 2.42 | <0.05 | R2 = 0.072 |
| b Substance misuse | |||||
| Number of ACE | 0.069 | 0.026 | 2.60 | <0.01 | |
| PA | 0.18 | 0.080 | 2.26 | <0.05 | R2 = 0.044 |
| b Worsening function | |||||
| Number of ACE | 0.10 | 0.020 | 5.06 | <0.01 | |
| PA | 0.058 | 0.059 | 0.97 | 0.33 | R2 = 0.075 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, Y.-M.; Shekhtman, T.; Kelsoe, J.R. Effect of the Type and Number of Adverse Childhood Experiences and the Timing of Adverse Experiences on Clinical Outcomes in Individuals with Bipolar Disorder. Brain Sci. 2020, 10, 254. https://doi.org/10.3390/brainsci10050254
Park Y-M, Shekhtman T, Kelsoe JR. Effect of the Type and Number of Adverse Childhood Experiences and the Timing of Adverse Experiences on Clinical Outcomes in Individuals with Bipolar Disorder. Brain Sciences. 2020; 10(5):254. https://doi.org/10.3390/brainsci10050254
Chicago/Turabian StylePark, Young-Min, Tatyana Shekhtman, and John R. Kelsoe. 2020. "Effect of the Type and Number of Adverse Childhood Experiences and the Timing of Adverse Experiences on Clinical Outcomes in Individuals with Bipolar Disorder" Brain Sciences 10, no. 5: 254. https://doi.org/10.3390/brainsci10050254
APA StylePark, Y.-M., Shekhtman, T., & Kelsoe, J. R. (2020). Effect of the Type and Number of Adverse Childhood Experiences and the Timing of Adverse Experiences on Clinical Outcomes in Individuals with Bipolar Disorder. Brain Sciences, 10(5), 254. https://doi.org/10.3390/brainsci10050254