
The Link Between Physical Function, β-Amyloid, and Cognitive Aging in Women



Abstract
1. Introduction
2. Materials and Methods
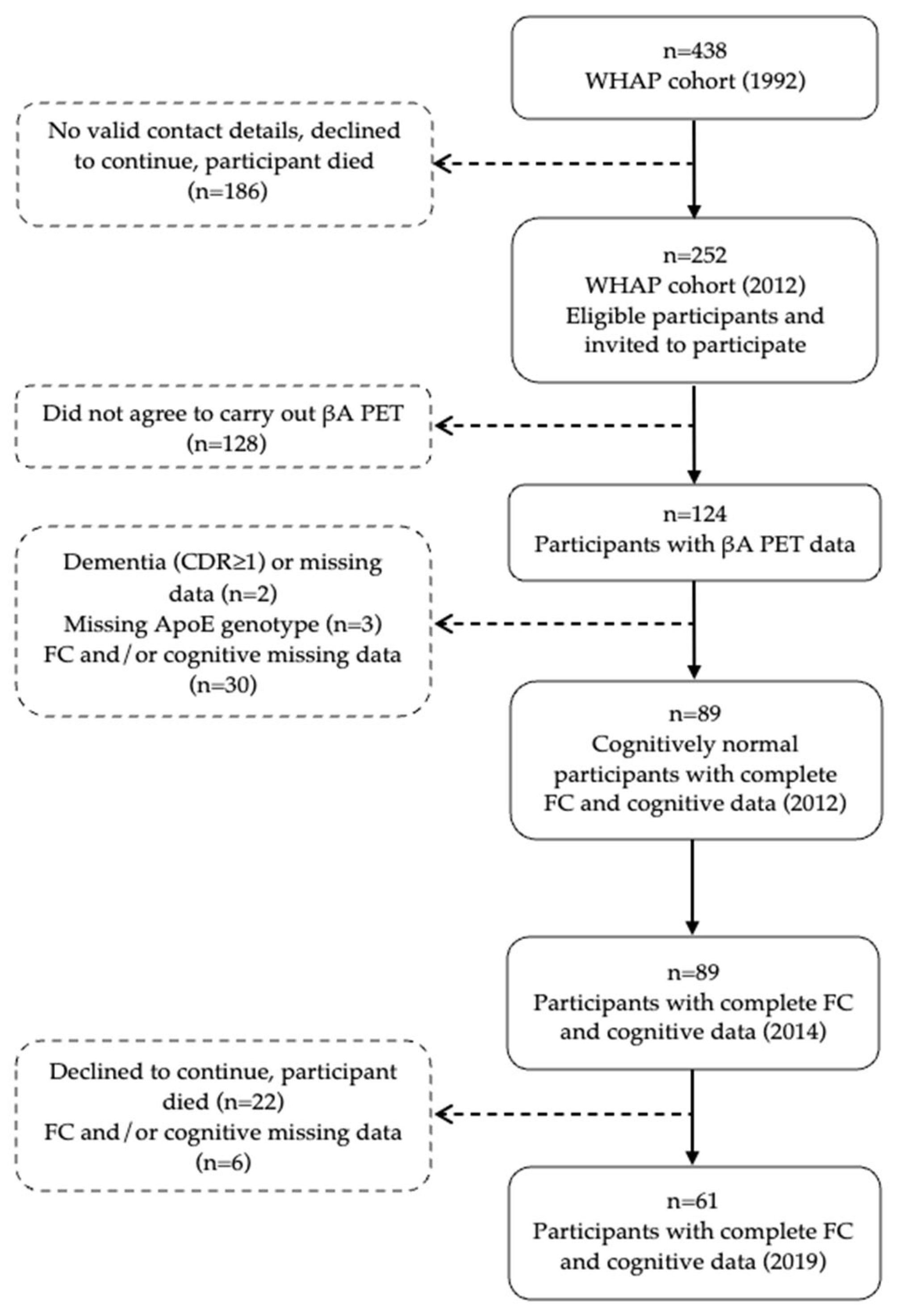
2.1. Participants
2.2. PET Imaging
2.3. Evaluation of Physical Functional Capacity
2.4. Cognitive Measures
2.5. Covariates
2.6. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Association Between FC and Brain βA Load with Cognition
3.3. Factors Associated with Cognitive Performance over Time
3.4. Mediation Analysis
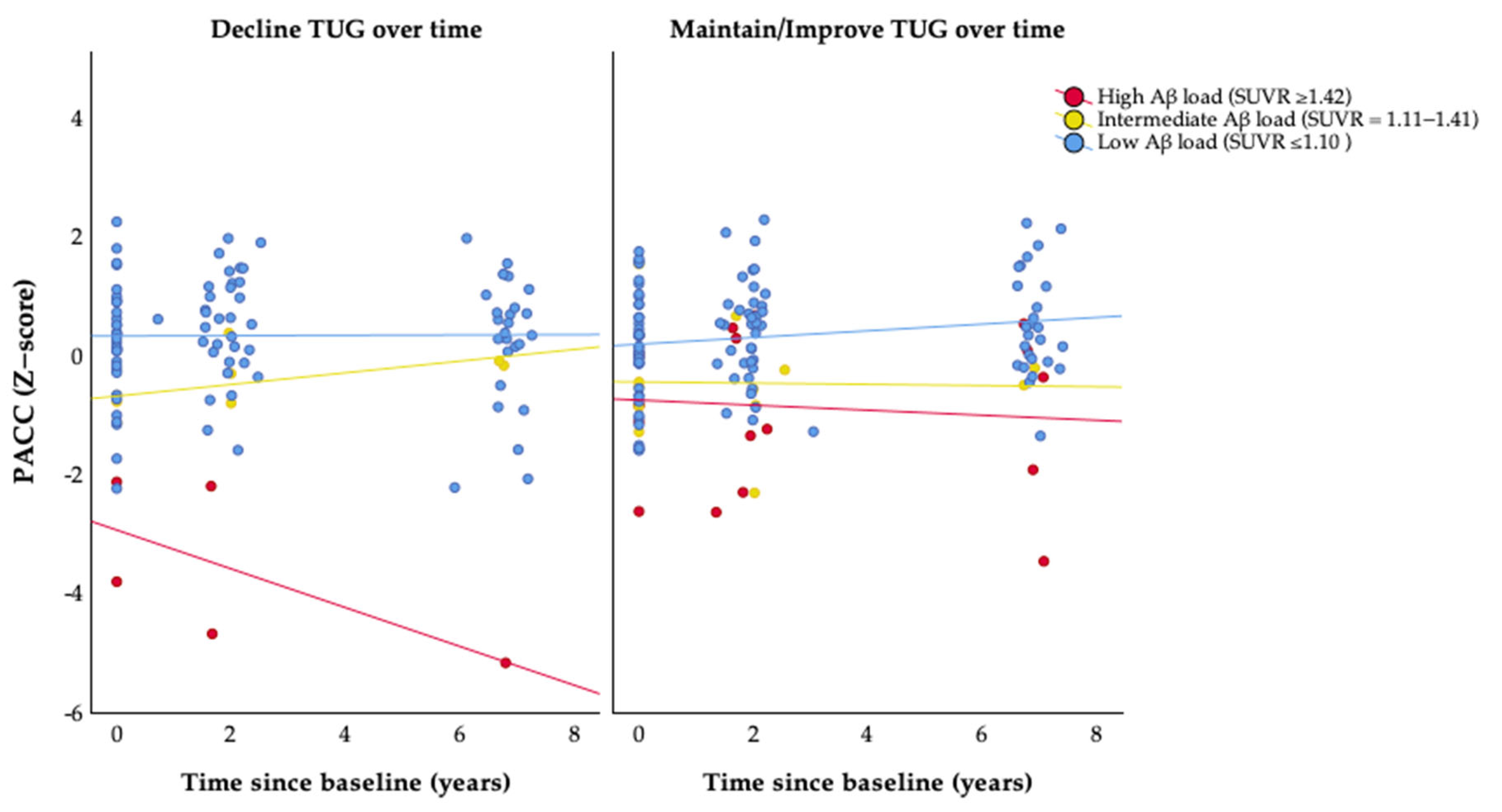
3.5. Association of FC Deterioration with Longitudinal Cognitive Function
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nandi, A.; Counts, N.; Chen, S.; Seligman, B.; Tortorice, D.; Vigo, D.; Bloom, D.E. Global and Regional Projections of the Economic Burden of Alzheimer’s Disease and Related Dementias from 2019 to 2050: A Value of Statistical Life Approach. EClinicalMedicine 2022, 51, 101580. [Google Scholar] [CrossRef] [PubMed]
- Skaria, A.P. The Economic and Societal Burden of Alzheimer Disease: Managed Care Considerations. Am. J. Manag. Care 2022, 28, S188–S196. [Google Scholar] [CrossRef] [PubMed]
- Gauthier, S.; Rosa-Neto, P.; Morais, J.A.; Webster, C. World Alzheimer Report: Journey Through the Diagnosis of Dementia. Alzheimer’s Dis. Int. 2021, 30, 19. [Google Scholar]
- Thal, D.R.; Capetillo-Zarate, E.; Del Tredici, K.; Braak, H. The Development of Amyloid Beta Protein Deposits in the Aged Brain. Sci. Aging Knowl. Environ. 2006, 2006, re1. [Google Scholar] [CrossRef]
- Jack, C.R.; Knopman, D.S.; Jagust, W.J.; Petersen, R.C.; Weiner, M.W.; Aisen, P.S.; Shaw, L.M.; Vemuri, P.; Wiste, H.J.; Weigand, S.D.; et al. Tracking Pathophysiological Processes in Alzheimer’s Disease: An Updated Hypothetical Model of Dynamic Biomarkers. Lancet Neurol. 2013, 12, 207–216. [Google Scholar] [CrossRef]
- Peters, R.; Booth, A.; Rockwood, K.; Peters, J.; D’Este, C.; Anstey, K.J. Combining Modifiable Risk Factors and Risk of Dementia: A Systematic Review and Meta-Analysis. BMJ Open 2019, 9, e022846. [Google Scholar] [CrossRef]
- Ebrahimi, K.; Majdi, A.; Baghaiee, B.; Hosseini, S.H.; Sadigh-Eteghad, S. Physical Activity and Beta-Amyloid Pathology in Alzheimer’s Disease: A Sound Mind in a Sound Body. EXCLI J. 2017, 16, 959–972. [Google Scholar]
- De la Rosa, A.; Olaso-Gonzalez, G.; Arc-Chagnaud, C.; Millan, F.; Salvador-Pascual, A.; García-Lucerga, C.; Blasco-Lafarga, C.; Garcia-Dominguez, E.; Carretero, A.; Correas, A.G.; et al. Physical Exercise in the Prevention and Treatment of Alzheimer’s Disease. J. Sport Health Sci. 2020, 9, 394–404. [Google Scholar] [CrossRef]
- Rabin, J.S.; Klein, H.; Kirn, D.R.; Schultz, A.P.; Yang, H.S.; Hampton, O.; Jiang, S.; Buckley, R.F.; Viswanathan, A.; Hedden, T.; et al. Associations of Physical Activity and β-Amyloid with Longitudinal Cognition and Neurodegeneration in Clinically Normal Older Adults. JAMA Neurol. 2019, 76, 1203–1210. [Google Scholar] [CrossRef]
- Erickson, K.I.; Leckie, R.L.; Weinstein, A.M. Physical Activity, Fitness, and Gray Matter Volume. Neurobiol. Aging 2014, 35, S20–S28. [Google Scholar] [CrossRef]
- Pedrero-Chamizo, R.; Szoeke, C.; Dennerstein, L.; Campbell, S. Influence of Physical Activity Levels and Functional Capacity on Brain β-Amyloid Deposition in Older Women. Front. Aging Neurosci. 2021, 13, 697528. [Google Scholar] [CrossRef] [PubMed]
- Iso-Markku, P.; Kujala, U.M.; Knittle, K.; Polet, J.; Vuoksimaa, E.; Waller, K. Physical Activity as a Protective Factor for Dementia and Alzheimer’s Disease: Systematic Review, Meta-Analysis and Quality Assessment of Cohort and Case-Control Studies. Br. J. Sports Med. 2022, 56, 701–709. [Google Scholar] [CrossRef] [PubMed]
- Szoeke, C.; Coulson, M.; Campbell, S.; Dennerstein, L. Cohort Profile: Women’s Healthy Ageing Project (WHAP)—A Longitudinal Prospective Study of Australian Women since 1990. Womens Midlife Health 2016, 2, 5. [Google Scholar] [CrossRef] [PubMed]
- Duara, R.; Loewenstein, D.A.; Lizarraga, G.; Adjouadi, M.; Barker, W.W.; Greig-Custo, M.T.; Rosselli, M.; Penate, A.; Shea, Y.F.; Behar, R.; et al. Effect of Age, Ethnicity, Sex, Cognitive Status and APOE Genotype on Amyloid Load and the Threshold for Amyloid Positivity. Neuroimage Clin. 2019, 22, 101800. [Google Scholar] [CrossRef]
- Villemagne, V.L.; Ong, K.; Mulligan, R.S.; Holl, G.; Pejoska, S.; Jones, G.; O’Keefe, G.; Ackerman, U.; Tochon-Danguy, H.; Chan, J.G.; et al. Amyloid Imaging with 18F-Florbetaben in Alzheimer Disease and Other Dementias. J. Nucl. Med. 2011, 52, 1210–1217. [Google Scholar] [CrossRef]
- Bullich, S.; Roé-Vellvé, N.; Marquié, M.; Landau, S.M.; Barthel, H.; Villemagne, V.L.; Sanabria, Á.; Tartari, J.P.; Sotolongo-Grau, O.; Doré, V.; et al. Early Detection of Amyloid Load Using 18F-Florbetaben PET. Alzheimers Res. Ther. 2021, 13, 67. [Google Scholar] [CrossRef]
- Richardson, S. The Timed “Up & Go”: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef]
- Donoghue, O.A.; Savva, G.M.; Börsch-Supan, A.; Kenny, R.A. Reliability, Measurement Error and Minimum Detectable Change in Mobility Measures: A Cohort Study of Community-Dwelling Adults Aged 50 Years and over in Ireland. BMJ Open 2019, 9, e030475. [Google Scholar] [CrossRef]
- Insel, P.S.; Weiner, M.; Scott MacKin, R.; Mormino, E.; Lim, Y.Y.; Stomrud, E.; Palmqvist, S.; Masters, C.L.; Maruff, P.T.; Hansson, O.; et al. Determining Clinically Meaningful Decline in Preclinical Alzheimer Disease. Neurology 2019, 93, E322–E333. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E. Mini-Mental State. A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiat. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Delis, D.; Kramer, J.; Kaplan, E.; Ober, B.A. CVLT-II Adult Version; Harcourt-Brace: San Antonio, CA, USA, 2000. [Google Scholar]
- Wechsler, D.A. Wechsler Adult Intelligence Scale-Third Edition; Psychological Corporation: New York, NY, USA, 1997. [Google Scholar]
- Wechsler, D.A. Wechsler Memory Scale-Revised (WMS-R); Psychological Corporation: San Antonio, TX, USA, 1987. [Google Scholar]
- D’Agostino, R.B.; Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.M.; Kannel, W.B. General Cardiovascular Risk Profile for Use in Primary Care: The Framingham Heart Study. Circulation 2008, 117, 743–753. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F. PROCESS: A Versatile Computational Tool for Observed Variable Mediation, Moderation, and Conditional Process Modeling [White Paper]. 2012. Available online: http://www.afhayes.com/public/process2012.pdf (accessed on 26 April 2025).
- Buchman, A.S.; Boyle, P.A.; Yu, L.; Shah, R.C.; Wilson, R.S.; Bennett, D.A. Total Daily Physical Activity and the Risk of AD and Cognitive Decline in Older Adults. Neurology 2012, 78, 1323–1329. [Google Scholar] [CrossRef] [PubMed]
- Brown, B.M.; Peiffer, J.J.; Taddei, K.; Lui, J.K.; Laws, S.M.; Gupta, V.B.; Taddei, T.; Ward, V.K.; Rodrigues, M.A.; Burnham, S.; et al. Physical Activity and Amyloid-β Plasma and Brain Levels: Results from the Australian Imaging, Biomarkers and Lifestyle Study of Ageing. Mol. Psychiatry 2013, 18, 875–881. [Google Scholar] [CrossRef] [PubMed]
- Stillman, C.M.; Lopez, O.L.; Becker, J.T.; Kuller, L.H.; Mehta, P.D.; Tracy, R.P.; Erickson, K.I. Physical Activity Predicts Reduced Plasma β Amyloid in the Cardiovascular Health Study. Ann. Clin. Transl. Neurol. 2017, 4, 284–291. [Google Scholar] [CrossRef]
- De Souto Barreto, P.; Andrieu, S.; Payoux, P.; Demougeot, L.; Rolland, Y.; Vellas, B. Physical Activity and Amyloid-β Brain Levels in Elderly Adults with Intact Cognition and Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2015, 63, 1634–1639. [Google Scholar] [CrossRef]
- Vemuri, P.; Lesnick, T.G.; Przybelski, S.A.; Knopman, D.S.; Roberts, R.O.; Lowe, V.J.; Kantarci, K.; Senjem, M.L.; Gunter, J.L.; Boeve, B.F.; et al. Effect of Lifestyle Activities on Alzheimer Disease Biomarkers and Cognition. Ann. Neurol. 2012, 72, 730–738. [Google Scholar] [CrossRef]
- Bachmann, D.; Roman, Z.J.; Buchmann, A.; Zuber, I.; Studer, S.; Saake, A.; Rauen, K.; Gruber, E.; Nitsch, R.M.; Hock, C.; et al. Lifestyle Affects Amyloid Burden and Cognition Differently in Men and Women. Ann. Neurol. 2022, 92, 451–463. [Google Scholar] [CrossRef]
- Brown, B.M.; Peiffer, J.J.; Rainey-Smith, S.R. Exploring the Relationship between Physical Activity, Beta-Amyloid and Tau: A Narrative Review. Ageing Res. Rev. 2019, 50, 9–18. [Google Scholar] [CrossRef]
- Raffin, J.; Rolland, Y.; Aggarwal, G.; Nguyen, A.D.; Morley, J.E.; Li, Y.; Bateman, R.J.; Vellas, B.; Barreto, P.D.S. Associations between Physical Activity, Blood-Based Biomarkers of Neurodegeneration, and Cognition in Healthy Older Adults: The MAPT Study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2021, 76, 1382–1390. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Year of Data Collection | |||
|---|---|---|---|
| Variables | 2012 | 2014 | 2019 |
| Age | x | x | x |
| PACC | x | x | x |
| ApoE4 genotype | x | - | - |
| Aβ PET scan | x | - | - |
| Functional capacity (TUG) | x | x | x |
| Years of education | x | x | x |
| FHS-CVD | x | - | - |
| Whole Sample | TUG Performance Groups | ||
|---|---|---|---|
| Maintain/Improve a | Decline b | ||
| Total, n | 89 | 50 (56.2) | 39 (43.8) |
| Age (years) | 70.0 (2.7) | 69.9 (3.0) | 70.1 (2.3) |
| ApoE4 carriers, n (%) | 31 (34.8) | 18 (36.0) | 12 (30.8) |
| SUVR (index) | 1.1 (0.2) | 1.2 (0.2) | 1.1 (0.2) |
| TUG (seconds) | 7.7 (1.5) | 8.2 (1.3) | 7.0 (1.6) * |
| Education (years) | 12.8 (3.8) | 13.0 (3.5) | 12.6 (4.2) |
| FHS-CVD (index) | 0.2 (0.1) | 0.21 (0.1) | 0.32 (0.2) |
| Follow-up time (years) | 3.9 (2.6) | 3.9 (2.5) | 4.0 (2.5) |
| Total of participants at each follow-up, n (2nd, 3rd) | 89, 61 | 50, 33 | 39, 28 |
| Dependent Variable: PACC 2012 | |||||
| F | df | p | R2 | Adjusted R2 | |
| Final Model | 14.290 | 3, 85 | <0.001 | 0.335 | 0.312 |
| Independent Variables | B | SE | β | t | Sig. |
| Baseline SUVR * | −2.064 | 0.461 | −0.403 | −4.481 | <0.001 |
| Education (years) * | 0.081 | 0.025 | 0.286 | 3.200 | 0.002 |
| Age (years) * | −0.077 | 0.036 | −0.193 | −2.161 | 0.033 |
| Dependent Variable: PACC 2014 | |||||
| F | df | p | R2 | Adjusted R2 | |
| Final Model | 22.117 | 3, 84 | <0.001 | 0.441 | 0.421 |
| Independent Variables | B | SE | β | t | Sig. |
| Baseline SUVR * | −2.563 | 0.474 | −0.465 | −5.407 | <0.001 |
| Education (years) * | 0.097 | 0.026 | 0.318 | 3.698 | <0.001 |
| Baseline TUG (seconds) * | −0.200 | 0.070 | −0.251 | −2.859 | 0.005 |
| Dependent Variable: PACC 2019 | |||||
| F | df | p | R2 | Adjusted R2 | |
| Final Model | 15.577 | 3, 57 | <0.001 | 0.450 | 0.422 |
| Independent Variables | B | SE | β | t | Sig. |
| Baseline SUVR * | −4.505 | 0.813 | −0.550 | −5.544 | <0.001 |
| Education (years) * | 0.090 | 0.035 | 0.257 | 2.576 | 0.013 |
| FHS-CVD (index) * | −2.722 | 1.122 | −0.239 | −2.427 | 0.018 |
| Parameter | Estimate | SE | t Statistic | p Value |
|---|---|---|---|---|
| TUG decline × High Aβ load × Time | −0.284 | 0.129 | −2.206 | 0.029 * |
| TUG decline × Intermediate Aβ load × Time | 0.183 | 0.122 | 1.492 | 0.138 |
| TUG decline × Time | −0.044 | 0.033 | −1.346 | 0.180 |
| High Aβ load × Time | −0.103 | 0.060 | −1.712 | 0.089 |
| Intermediate Aβ load × Time | −0.135 | 0.084 | −1.607 | 0.110 |
| TUG decline × High Aβ load | −2.444 | 0.736 | −3.320 | 0.001 * |
| TUG decline × Intermediate Aβ load | −0.268 | 0.679 | −0.395 | 0.694 |
| ApoE4 carrier × Time | 0.056 | 0.034 | 1.643 | 0.102 |
| Age × Time | −0.006 | 0.005 | −1.148 | 0.253 |
| Education × Time | 0.004 | 0.004 | 0.950 | 0.344 |
| FHS-CVD × Time | −0.306 | 0.128 | −2.385 | 0.018 * |
| TUG decline | 0.161 | 0.211 | 0.763 | 0.447 |
| High Aβ load | −0.765 | 0.388 | −1.973 | 0.051 |
| Intermediate Aβ load | −0.654 | 0.423 | −1.548 | 0.125 |
| ApoE4 carrier | −0.122 | 0.218 | −0.561 | 0.576 |
| Age | −0.060 | 0.035 | −1.703 | 0.091 |
| Education | 0.087 | 0.025 | 3.481 | 0.001 * |
| FHS-CVD | 0.230 | 0.774 | 0.298 | 0.766 |
| Time | 0.496 | 0.363 | 1.368 | 0.173 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pedrero-Chamizo, R.; Szoeke, C. The Link Between Physical Function, β-Amyloid, and Cognitive Aging in Women. Appl. Sci. 2025, 15, 5210. https://doi.org/10.3390/app15095210
Pedrero-Chamizo R, Szoeke C. The Link Between Physical Function, β-Amyloid, and Cognitive Aging in Women. Applied Sciences. 2025; 15(9):5210. https://doi.org/10.3390/app15095210
Chicago/Turabian StylePedrero-Chamizo, Raquel, and Cassandra Szoeke. 2025. "The Link Between Physical Function, β-Amyloid, and Cognitive Aging in Women" Applied Sciences 15, no. 9: 5210. https://doi.org/10.3390/app15095210
APA StylePedrero-Chamizo, R., & Szoeke, C. (2025). The Link Between Physical Function, β-Amyloid, and Cognitive Aging in Women. Applied Sciences, 15(9), 5210. https://doi.org/10.3390/app15095210