



Artificial Intelligence Algorithms in Asthma Management: A Review of Data Engineering, Predictive Models, and Future Implications



Abstract
1. Introduction
1.1. Impact of Artificial Intelligence on Healthcare
1.2. Artificial Intelligence in Asthma Management
1.3. Review Assessment
1.3.1. Strengths
- The included literature identifies recent trends in AI algorithms for asthma diagnosis using diverse data types, such as signals, cough sounds, weather, environment, and EHRs.
- Presents the performance achieved so far in asthma diagnosis with multi-modal data and essential pre-processing techniques.
- Explores latest technology, i.e., ChatGPT’s role in asthma management and administration, focusing on its effectiveness as a support tool for physicians.
- Highlights the challenges and opportunities of implementing AI models in this context and suggests possible future directions.
- Proposes a framework for asthma management based on the existing literature techniques.
1.3.2. Limitations
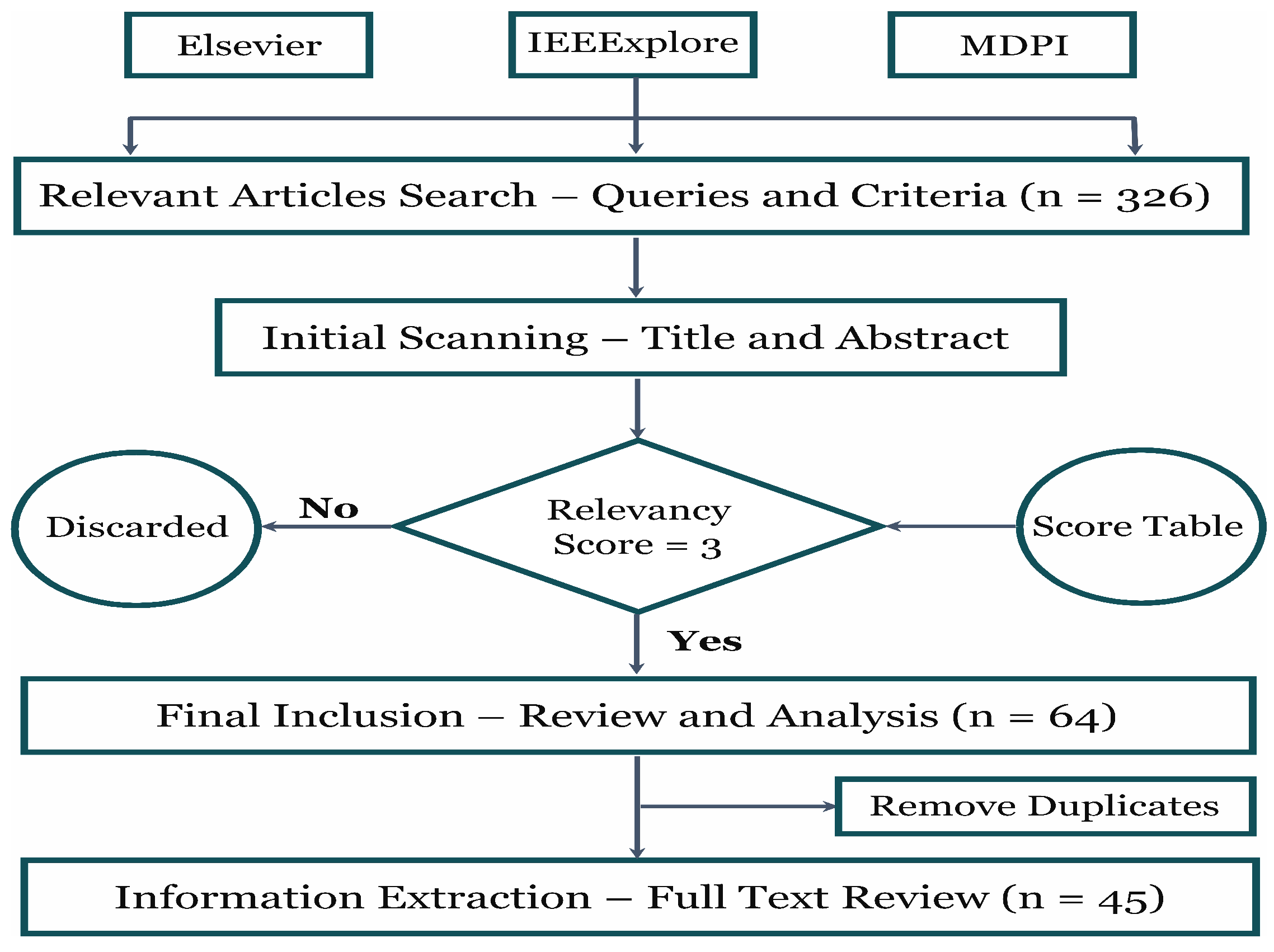
- This review considered articles from selected databases, including Elsevier, IEEE, and MDPI, which are mostly indexed in Scopus. However, Scopus itself was not directly searched, which may have limited access to additional journals, such as those from Springer.
- The model comparison primarily focuses on accuracy, as not all of the included literature reported the same evaluation metrics, making direct comparisons difficult.
- The included literature reveals a limitation in the detailed analysis of deep learning model architectures for asthma classification using imaging data, since the primary focus was on structured medical data.
- The review does not extensively cover synthetic data generation or augmentation techniques, such as the Synthetic Minority Oversampling Technique, as these methods require a separate in-depth discussion.
1.4. Review Eligibility Criteria
2. History of Artificial Intelligence in Asthma
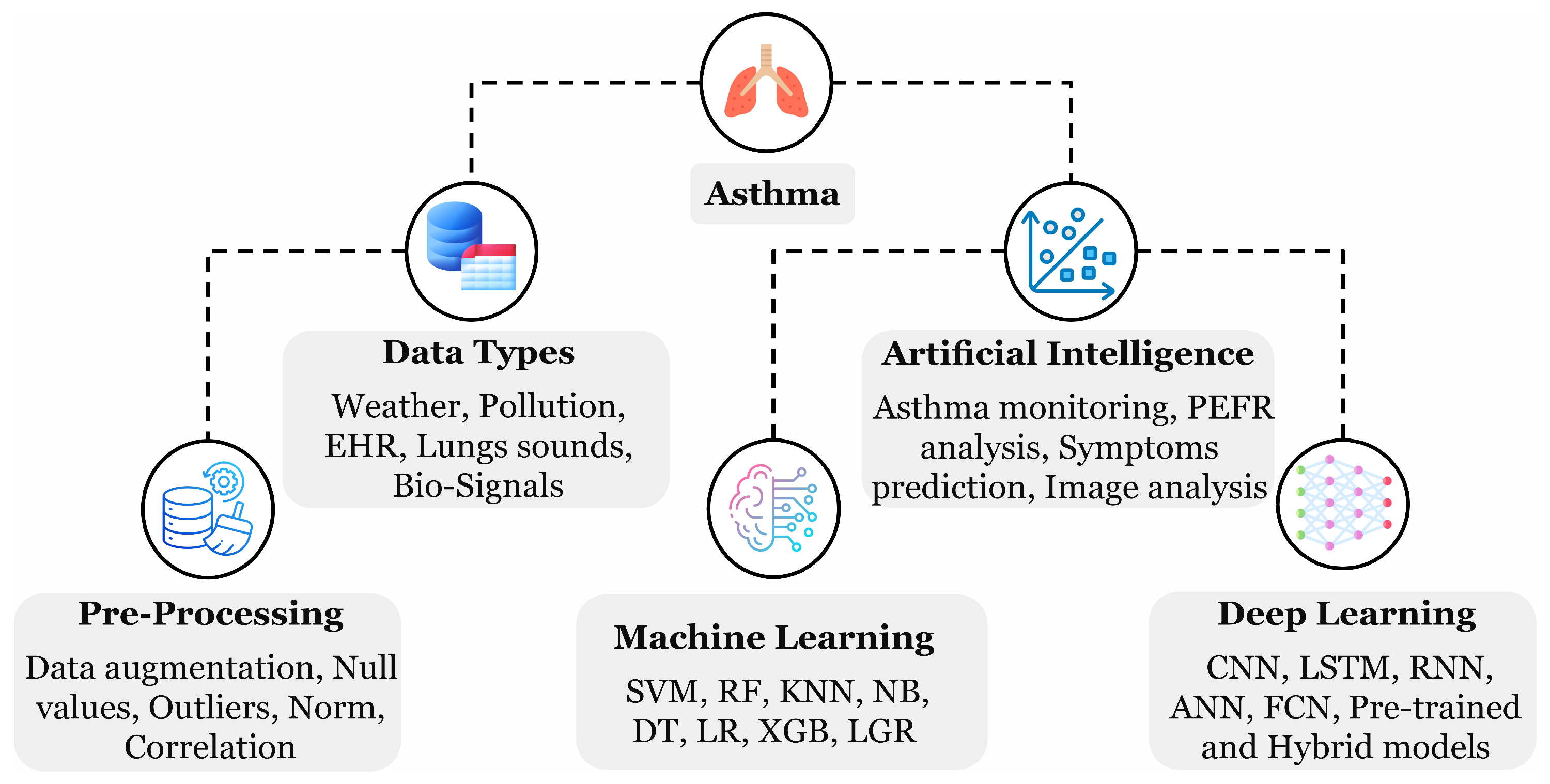
3. Asthma Data Sources
3.1. Data Types
3.1.1. Electronic Health Record
3.1.2. Environmental and Weather Data
3.2. Benchmark Datasets
3.2.1. Diseases Symptoms
3.2.2. Weather Data
3.2.3. Pollution Data
3.2.4. Hospital Databases
3.2.5. Lung X-Ray Radiographs
3.2.6. Cough Sounds
4. Pre-Processing and Classification
4.1. Pre-Processing
4.2. Classification and Regression Models
5. ChatGPT in Asthma Care
6. Challenges and Opportunities
- Classifying cough sounds into binary classes, as performed in the study by [35] using time-frequency analysis, can be extended to recommend relatively safer travel routes. Similarly, the binary classification of asthma vs. normal samples [43] uses relatively small datasets, which may impact model generalization.This review suggests that leveraging a high-volume dataset, such as the Kaggle 2018 free sound dataset with around 18,000 samples across 41 categories (including ‘Cough’), could provide significant benefits. It could be useful for pre-training and transfer learning, for example, by training a base model on the entire dataset and then fine-tuning it with ‘cough’ samples. Additionally, analyzing samples using efficient pre-processing techniques like Fourier or wavelet transforms could further enhance model performance.
- Since ML and DL algorithms are often viewed as black-box models for classification and regression tasks, analyzing the results can be challenging, making it difficult to identify strong and weak performance. Explainable AI techniques like ‘Shapley Additive Explanations’ can improve understanding of the decision-making processes of ML and DL models in asthma analysis, especially for regression and forecasting tasks. These methods can enhance model reliability by revealing how clinical and environmental factors influence predictions, helping to better predict asthma outcomes.
- AI models typically focus on maximizing intra-class similarity and minimizing inter-class similarity to improve performance. However, individual-based asthma classification presents a challenge, as it involves variation in classification labels, such as healthy vs. sick, or categorizing into the three asthma zones—green, yellow, and red for each individual dataset—requiring a more efficient approach to deal with the issue.This review suggests a step-by-step methodology to improve model generalization and performance: first, develop a generalized model that predicts asthma zones based on population-level data rather than individual cases. Then, perform reliable zone transitions to help enhance outcomes when addressing individual-based asthma conditions. This approach could lead to more accurate and consistent predictions for individuals.
- Asthma classification using respiratory sounds collected from stethoscopes or smartphone devices is a relatively new area, in contrast to the more established use of EHR data. Weather and environmental factors also play a crucial role in predicting asthma triggers. Therefore, combining respiratory sounds with weather and environmental data could enhance prediction accuracy, mainly through bagging and ensemble classifier approaches. Interpreting the results by ChatGPT can further improve patient feedback.
- The review highlighted the use of standalone ML, DL, and hybrid models to achieve satisfactory performance. However, transformer models, particularly in NLP, such as ChatGPT-based models, are gaining popularity. Therefore, evaluating GPT prompts with linguistic forms of EHR, pollution, and weather data for LLMs is worth considering.
7. Addressing Research Questions
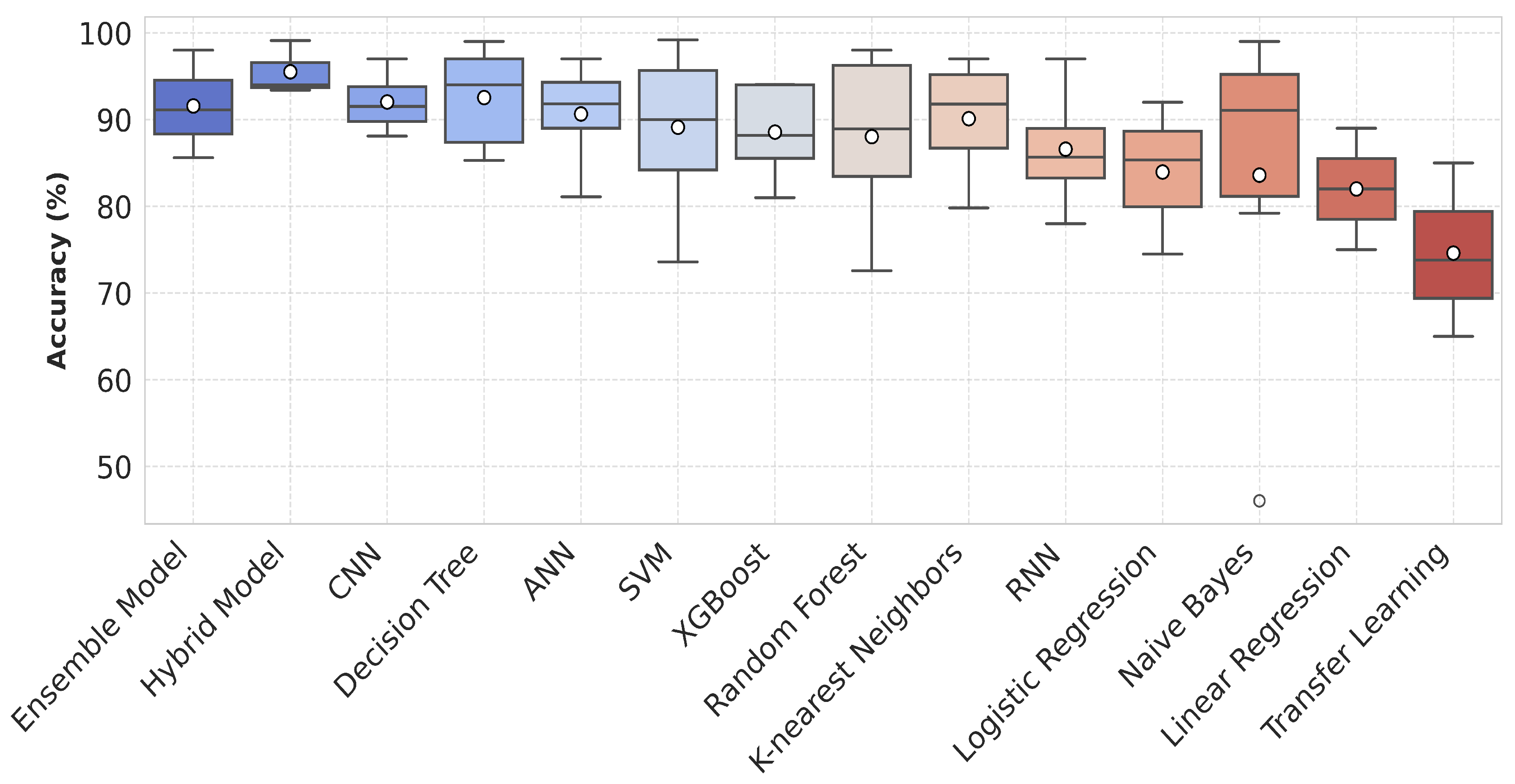
- How effectively can machine learning and deep learning models diagnose asthma compared to traditional diagnostic methods?The application of ML has demonstrated significant improvements in asthma prediction compared to both DL and traditional statistical methods. Notably, ensemble and hybrid ML models, along with DT, SVM, RF, and KNN, have shown predictive performance well when compared to DL approaches such as the RNN and CNN, as illustrated in Figure 7. Additionally, asthma analysis primarily relies on air quality and EHR data, as depicted in Figure 6b. Since these datasets are often presented in numerical form, ML techniques are particularly well suited for handling and analyzing them with greater precision.
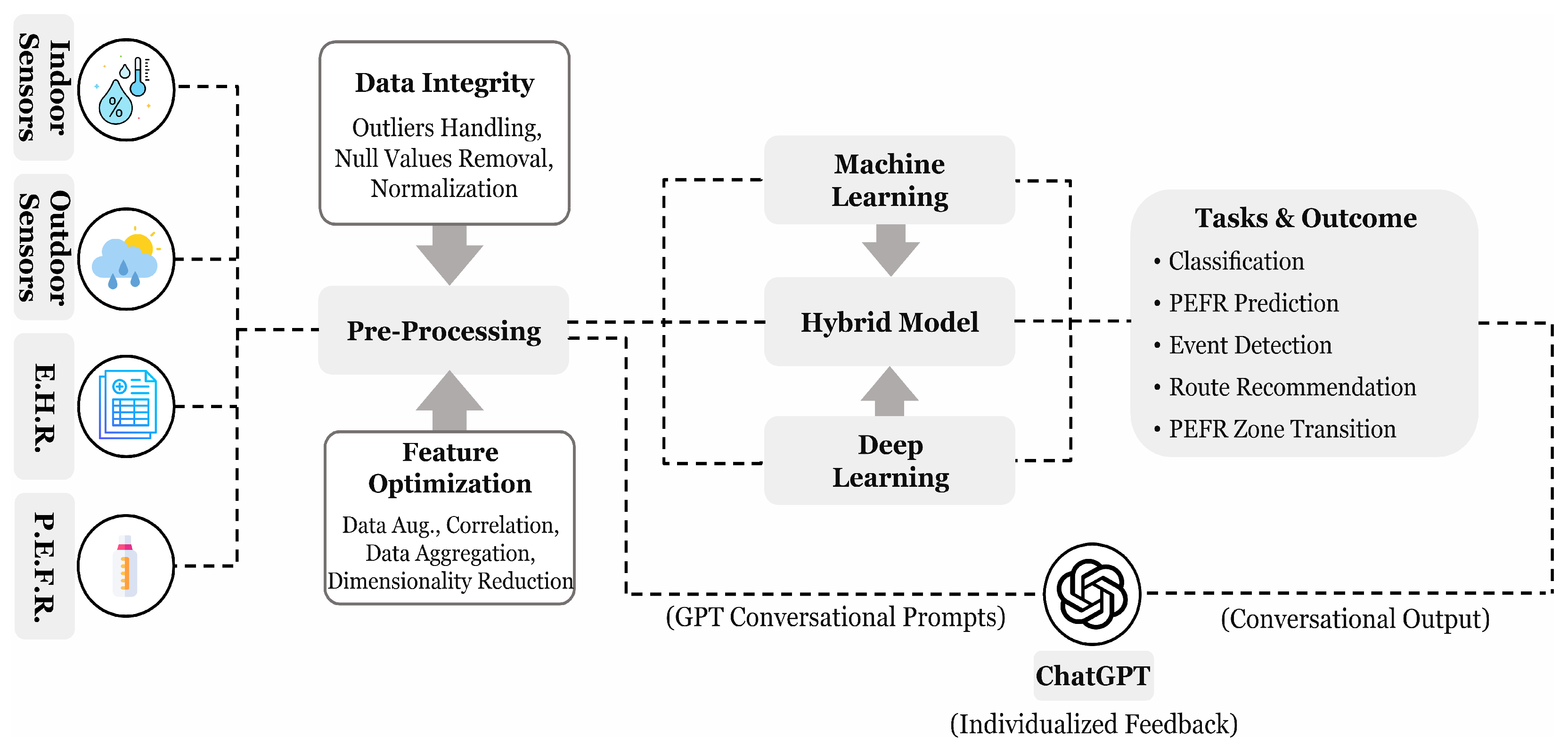
- How do different feature selection and data pre-processing techniques impact the performance of AI-based asthma prediction models?In numerical data analysis, pre-processing and feature selection techniques play a crucial role in enhancing asthma model performance, as discussed in Section 4.1 and illustrated in Figure 8. Eliminating null values and identifying outliers, which can introduce distortions in predictive analysis, are essential steps to prevent performance decline in AI models. Moreover, techniques such as correlation matrix analysis and principal component analysis help identify key features while reducing the influence of irrelevant variables. Additionally, data augmentation strategies like SMOTE contribute to improving model generalization by addressing class imbalance, ultimately leading to more reliable predictions.
- How can multi-modal data integration (EHR, environmental, and physiological data) improve asthma forecasting and early intervention strategies?The review findings indicate that most studies have focused either on EHR and environmental data or separately on physiological signals. However, integrating these diverse data sources into a multi-modal framework can offer a more comprehensive understanding of asthma triggers. Combining environmental factors, patient medical history, and real-time physiological signals enhances feature representation, providing a more broad view of asthma progression. These enriched data merging can lead to improved predictive accuracy, enabling early intervention strategies and more personalized asthma management.
- How can large language models (LLMs) like ChatGPT enhance asthma management, patient education, and decision support for physicians?With the growing prominence of LLMs in processing natural language and extracting meaningful insights, their integration into asthma care presents significant advantages. By transforming the outputs of traditional ML or DL models into conversational prompts, ChatGPT can provide personalized feedback, offering patients a clearer understanding of their health status, as illustrated in Figure 8. Additionally, preliminary studies, discussed in Section 5, highlight the potential of ChatGPT in assisting physicians with decision support and improving patient education, hence enhancing asthma management strategies.
8. Conclusions
Study Limitations
- Most of the articles in the review work were extracted from the Elsevier database rather than MDPI and IEEExplore due to the highly matched relevancy criteria described in Table 1.
- The reported accuracies in Figure 7 are based on the models’ appearances across various studies rather than their actual performance in identical conditions. These accuracies may be influenced by variations in datasets and methodologies used in each study.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AI | Artificial Intelligence |
| DL | Deep Learning |
| ML | Machine Learning |
| PM | Particulate Material |
| GPT | Generative Pre-trained Transformer |
| EHR | Electronic Health Records |
| LR | Linear Regression |
| SVM | Support Vector Machine |
| COPD | Chronic Obstructive Pulmonary Disease |
| CNN | Convolutional Neural Network |
| RF | Random Forest |
| NB | Naive Bayes |
| RMSE | Root Mean Squared Error |
| MSE | Mean Squared Error |
| MAE | Mean Absolute Error |
| SMOTE | Synthetic Minority Oversampling Technique |
References
- Exarchos, K.P.; Beltsiou, M.; Votti, C.A.; Kostikas, K. Artificial intelligence techniques in asthma: A systematic review and critical appraisal of the existing literature. Eur. Respir. J. 2020, 56, 2000521. [Google Scholar] [CrossRef] [PubMed]
- Gater, A.; Nelsen, L.; Fleming, S.; Lundy, J.J.; Bonner, N.; Hall, R.; Marshall, C.; Staunton, H.; Krishnan, J.A.; Stoloff, S.; et al. Assessing asthma symptoms in adolescents and adults: Qualitative research supporting development of the asthma daily symptom diary. Value Health 2016, 19, 440–450. [Google Scholar] [CrossRef]
- Yu, G.; Li, Z.; Li, S.; Liu, J.; Sun, M.; Liu, X.; Sun, F.; Zheng, J.; Li, Y.; Yu, Y.; et al. The role of artificial intelligence in identifying asthma in pediatric inpatient setting. Ann. Transl. Med. 2020, 8, 1367. [Google Scholar] [CrossRef]
- Kharaba, Z.; Feghali, E.; El Husseini, F.; Sacre, H.; Abou Selwan, C.; Saadeh, S.; Hallit, S.; Jirjees, F.; AlObaidi, H.; Salameh, P.; et al. An assessment of quality of life in patients with asthma through physical, emotional, social, and occupational aspects. A cross-sectional study. Front. Public Health 2022, 10, 883784. [Google Scholar] [CrossRef] [PubMed]
- Borna, E.; Nwaru, B.I.; Bjerg, A.; Mincheva, R.; Rådinger, M.; Lundbäck, B.; Ekerljung, L. Changes in the prevalence of asthma and respiratory symptoms in western Sweden between 2008 and 2016. Allergy 2019, 74, 1703–1715. [Google Scholar] [CrossRef]
- Hafke-Dys, H.; Kuźnar-Kamińska, B.; Grzywalski, T.; Maciaszek, A.; Szarzyński, K.; Kociński, J. Artificial intelligence approach to the monitoring of respiratory sounds in asthmatic patients. Front. Physiol. 2021, 12, 745635. [Google Scholar] [CrossRef]
- Al Kuwaiti, A.; Nazer, K.; Al-Reedy, A.; Al-Shehri, S.; Al-Muhanna, A.; Subbarayalu, A.V.; Al Muhanna, D.; Al-Muhanna, F.A. A review of the role of artificial intelligence in healthcare. J. Pers. Med. 2023, 13, 951. [Google Scholar] [CrossRef] [PubMed]
- Gulshan, V.; Peng, L.; Coram, M.; Stumpe, M.C.; Wu, D.; Narayanaswamy, A.; Venugopalan, S.; Widner, K.; Madams, T.; Cuadros, J.; et al. Development and validation of a deep learning algorithm for detection of diabetic retinopathy in retinal fundus photographs. JAMA 2016, 316, 2402–2410. [Google Scholar] [CrossRef]
- Meedeniya, D.; Kumarasinghe, H.; Kolonne, S.; Fernando, C.; De la Torre Díez, I.; Marques, G. Chest X-ray analysis empowered with deep learning: A systematic review. Appl. Soft Comput. 2022, 126, 109319. [Google Scholar] [CrossRef]
- Gassenmaier, S.; Küstner, T.; Nickel, D.; Herrmann, J.; Hoffmann, R.; Almansour, H.; Afat, S.; Nikolaou, K.; Othman, A.E. Deep learning applications in magnetic resonance imaging: Has the future become present? Diagnostics 2021, 11, 2181. [Google Scholar] [CrossRef]
- Safdar, M.F.; Alkobaisi, S.S.; Zahra, F.T. A comparative analysis of data augmentation approaches for magnetic resonance imaging (MRI) scan images of brain tumor. Acta Inform. Medica 2020, 28, 29. [Google Scholar] [CrossRef] [PubMed]
- Snider, E.J.; Hernandez-Torres, S.I.; Boice, E.N. An image classification deep-learning algorithm for shrapnel detection from ultrasound images. Sci. Rep. 2022, 12, 8427. [Google Scholar] [CrossRef]
- Ong, M.S.; Sordillo, J.E.; Dahlin, A.; McGeachie, M.; Tantisira, K.; Wang, A.L.; Lasky-Su, J.; Brilliant, M.; Kitchner, T.; Roden, D.M.; et al. Machine Learning Prediction of Treatment Response to Inhaled Corticosteroids in Asthma. J. Pers. Med. 2024, 14, 246. [Google Scholar] [CrossRef]
- Thafar, M.A.; Olayan, R.S.; Ashoor, H.; Albaradei, S.; Bajic, V.B.; Gao, X.; Gojobori, T.; Essack, M. DTiGEMS+: Drug–target interaction prediction using graph embedding, graph mining, and similarity-based techniques. J. Cheminformatics 2020, 12, 44. [Google Scholar] [CrossRef]
- Matsuzaka, Y.; Uesawa, Y. Prediction model with high-performance constitutive androstane receptor (car) using deepsnap-deep learning approach from the Tox21 10K compound library. Int. J. Mol. Sci. 2019, 20, 4855. [Google Scholar] [CrossRef] [PubMed]
- Asaad, C.; Ghogho, M. AsthmaKGxE: An asthma–environment interaction knowledge graph leveraging public databases and scientific literature. Comput. Biol. Med. 2022, 148, 105933. [Google Scholar] [CrossRef] [PubMed]
- Mittal, K.; Dhar, M. Use of ChatGPT by physicians to build rehabilitation plans for the elderly: A mini-review of case studies. J. Indian Acad. Geriatr. 2023, 19, 86–93. [Google Scholar] [CrossRef]
- Al Meslamani, A.Z. How AI is advancing asthma management? Insights into economic and clinical aspects. J. Med. Econ. 2023, 26, 1489–1494. [Google Scholar] [CrossRef]
- Gunasinghe, A.D.; Aponso, A.C.; Thirimanna, H. Early prediction of lung diseases. In Proceedings of the 2019 IEEE 5th International Conference for Convergence in Technology (I2CT), Bombay, India, 29–31 March 2019; pp. 1227–1230. [Google Scholar]
- Abirami, S.; Chitra, P.; Madhumitha, R.; Kesavan, S.R. Hybrid spatio-temporal deep learning framework for particulate matter (pm 2.5) concentration forecasting. In Proceedings of the 2020 International Conference on Innovative Trends in Information Technology (ICITIIT), Kottayam, India, 13–14 February 2020; pp. 11–16. [Google Scholar]
- Kim, M.S.; Lee, J.H.; Jang, Y.J.; Lee, C.H.; Choi, J.H.; Sung, T.E. Hybrid deep learning algorithm with open innovation perspective: A prediction model of asthmatic occurrence. Sustainability 2020, 12, 6143. [Google Scholar] [CrossRef]
- Ibrahim, M.A.; Çamur, H.; Savaş, M.A.; Sabo, A.K.; Mustapha, M.; Abba, S.I. Hybrid artificial intelligence models with multi objective optimization for prediction of tribological behavior of polytetrafluoroethylene matrix composites. Appl. Sci. 2022, 12, 8671. [Google Scholar] [CrossRef]
- Li, M.; Waheed, R.; Kirikkaleli, D.; Aziz, G. Relevance of hybrid artificial intelligence for improving the forecasting accuracy of natural resource prices. Geosci. Front. 2024, 15, 101670. [Google Scholar] [CrossRef]
- Manocha, A.; Bhatia, M.; Kumar, G. Dew computing-inspired health-meteorological factor analysis for early prediction of bronchial asthma. J. Netw. Comput. Appl. 2021, 179, 102995. [Google Scholar] [CrossRef]
- Khasha, R.; Sepehri, M.M.; Taherkhani, N. Detecting asthma control level using feature-based time series classification. Appl. Soft Comput. 2021, 111, 107694. [Google Scholar] [CrossRef]
- Yahyaoui, A.; Yumuşak, N. Deep and machine learning towards pneumonia and asthma detection. In Proceedings of the 2021 International Conference on Innovation and Intelligence for Informatics, Computing, and Technologies (3ICT), Virtual, 29–30 September 2021; pp. 494–497. [Google Scholar]
- Jeddi, Z.; Gryech, I.; Ghogho, M.; El Hammoumi, M.; Mahraoui, C. Machine learning for predicting the risk for childhood asthma using prenatal, perinatal, postnatal and environmental factors. Healthcare 2021, 9, 1464. [Google Scholar] [CrossRef]
- Tong, Y.; Lin, B.; Chen, G.; Zhang, Z. Predicting continuity of asthma care using a machine learning model: Retrospective cohort study. Int. J. Environ. Res. Public Health 2022, 19, 1237. [Google Scholar] [CrossRef]
- Alharbi, E.; Nadeem, F.; Cherif, A. Smart healthcare framework for asthma attack prediction and prevention. In Proceedings of the 2021 National Computing Colleges Conference (NCCC), Taif, Saudi Arabia, 27–28 March 2021; pp. 1–6. [Google Scholar]
- Bhat, G.S.; Shankar, N.; Kim, D.; Song, D.J.; Seo, S.; Panahi, I.M.; Tamil, L. Machine learning-based asthma risk prediction using IoT and smartphone applications. IEEE Access 2021, 9, 118708–118715. [Google Scholar] [CrossRef]
- Bae, W.D.; Alkobaisi, S.; Horak, M.; Park, C.S.; Kim, S.; Davidson, J. Predicting health risks of adult asthmatics susceptible to indoor air quality using improved logistic and quantile regression models. Life 2022, 12, 1631. [Google Scholar] [CrossRef]
- Barrera-Animas, A.Y.; Oyedele, L.O.; Bilal, M.; Akinosho, T.D.; Delgado, J.M.D.; Akanbi, L.A. Rainfall prediction: A comparative analysis of modern machine learning algorithms for time-series forecasting. Mach. Learn. Appl. 2022, 7, 100204. [Google Scholar] [CrossRef]
- Bhattacharjee, S.; Saha, B.; Bhattacharyya, P.; Saha, S. Classification of obstructive and non-obstructive pulmonary diseases on the basis of spirometry using machine learning techniques. J. Comput. Sci. 2022, 63, 101768. [Google Scholar] [CrossRef]
- Azim, A.; Rezwan, F.I.; Barber, C.; Harvey, M.; Kurukulaaratchy, R.J.; Holloway, J.W.; Howarth, P.H. Measurement of exhaled volatile organic compounds as a biomarker for personalised medicine: Assessment of short-term repeatability in severe asthma. J. Pers. Med. 2022, 12, 1635. [Google Scholar] [CrossRef]
- Bhowmik, R.T.; Most, S.P. A personalized respiratory disease exacerbation prediction technique based on a novel spatio-temporal machine learning architecture and local environmental sensor networks. Electronics 2022, 11, 2562. [Google Scholar] [CrossRef]
- Akinosho, T.D.; Bilal, M.; Hayes, E.T.; Ajayi, A.; Ahmed, A.; Khan, Z. Deep learning-based multi-target regression for traffic-related air pollution forecasting. Mach. Learn. Appl. 2023, 12, 100474. [Google Scholar] [CrossRef]
- Lu, X.; Zhou, W.; Ly, H.B.; Qi, C.; Nguyen, T.A.; Nguyen, M.H.; Huang, J.; Pham, B.T. Optimization of neural network parameters in improvement of particulate matter concentration prediction of open-pit mining. Appl. Soft Comput. 2023, 147, 110769. [Google Scholar] [CrossRef]
- Topaloglu, I.; Barua, P.D.; Yildiz, A.M.; Keles, T.; Dogan, S.; Baygin, M.; Gul, H.F.; Tuncer, T.; Tan, R.S.; Acharya, U.R. Explainable attention ResNet18-based model for asthma detection using stethoscope lung sounds. Eng. Appl. Artif. Intell. 2023, 126, 106887. [Google Scholar] [CrossRef]
- Alharbi, E.; Cherif, A.; Nadeem, F. Adaptive Smart eHealth Framework for Personalized Asthma Attack Prediction and Safe Route Recommendation. Smart Cities 2023, 6, 2910–2931. [Google Scholar] [CrossRef]
- Nasarudin, N.A.; Al Jasmi, F.; Sinnott, R.O.; Zaki, N.; Al Ashwal, H.; Mohamed, E.A.; Mohamad, M.S. A review of deep learning models and online healthcare databases for electronic health records and their use for health prediction. Artif. Intell. Rev. 2024, 57, 249. [Google Scholar] [CrossRef]
- Lan, B.; Haaland, P.; Krishnamurthy, A.; Peden, D.B.; Schmitt, P.L.; Sharma, P.; Sinha, M.; Xu, H.; Fecho, K. Open application of statistical and machine learning models to explore the impact of environmental exposures on health and disease: An asthma use case. Int. J. Environ. Res. Public Health 2021, 18, 11398. [Google Scholar] [CrossRef]
- Tomita, K.; Yamasaki, A.; Katou, R.; Ikeuchi, T.; Touge, H.; Sano, H.; Tohda, Y. Construction of a Diagnostic Algorithm for Diagnosis of Adult Asthma Using Machine Learning with Random Forest and XGBoost. Diagnostics 2023, 13, 3069. [Google Scholar] [CrossRef]
- Hee, H.I.; Balamurali, B.; Karunakaran, A.; Herremans, D.; Teoh, O.H.; Lee, K.P.; Teng, S.S.; Lui, S.; Chen, J.M. Development of machine learning for asthmatic and healthy voluntary cough sounds: A proof of concept study. Appl. Sci. 2019, 9, 2833. [Google Scholar] [CrossRef]
- Sharma, R.; Zang, W.; Zhou, M.; Schafer, N.; Begley, L.A.; Huang, Y.J.; Fan, X. Real time breath analysis using portable gas chromatography for adult asthma phenotypes. Metabolites 2021, 11, 265. [Google Scholar] [CrossRef]
- Sridhar, A.; Mawia, A.; Amutha, A. Mobile application development for disease diagnosis based on symptoms using machine learning techniques. Procedia Comput. Sci. 2023, 218, 2594–2603. [Google Scholar] [CrossRef]
- OpenWeather. Open Weather API Dataset. 2024. Available online: https://openweathermap.org/ (accessed on 15 August 2024).
- CPCB. Weather Pollution Dataset. 2024. Available online: https://cpcb.nic.in/ (accessed on 15 August 2024).
- Imam, M.; Adam, S.; Dev, S.; Nesa, N. Air quality monitoring using statistical learning models for sustainable environment. Intell. Syst. Appl. 2024, 22, 200333. [Google Scholar] [CrossRef]
- Jayamini, W.K.D.; Mirza, F.; Naeem, M.A.; Chan, A.H.Y. State of asthma-related hospital admissions in New Zealand and predicting length of stay using machine learning. Appl. Sci. 2022, 12, 9890. [Google Scholar] [CrossRef]
- Kaggle-NIH. NIH Chest X-Ray Images. 2024. Available online: https://www.kaggle.com/datasets/nih-chest-xrays/data (accessed on 15 August 2024).
- Kaggle-Audio. Audio Sounds Dataset. 2024. Available online: https://www.kaggle.com/c/freesound-audio-tagging (accessed on 15 August 2024).
- Alqudaihi, K.S.; Aslam, N.; Khan, I.U.; Almuhaideb, A.M.; Alsunaidi, S.J.; Ibrahim, N.M.A.R.; Alhaidari, F.A.; Shaikh, F.S.; Alsenbel, Y.M.; Alalharith, D.M.; et al. Cough sound detection and diagnosis using artificial intelligence techniques: Challenges and opportunities. IEEE Access 2021, 9, 102327–102344. [Google Scholar] [CrossRef]
- Majdi, A.; Alrubaie, A.J.; Al-Wardy, A.H.; Baili, J.; Panchal, H. A novel method for Indoor Air Quality Control of Smart Homes using a Machine learning model. Adv. Eng. Softw. 2022, 173, 103253. [Google Scholar] [CrossRef]
- Lee, Z.J.; Yang, M.R.; Hwang, B.J. A Sustainable Approach to Asthma Diagnosis: Classification with Data Augmentation, Feature Selection, and Boosting Algorithm. Diagnostics 2024, 14, 723. [Google Scholar] [CrossRef]
- Mahammad, A.B.; Kumar, R. Machine Learning Approach to Predict Asthma Prevalence with Decision Trees. In Proceedings of the 2022 2nd International Conference on Technological Advancements in Computational Sciences (ICTACS), Tashkent, Uzbekistan, 10–12 October 2022; pp. 263–267. [Google Scholar]
- Raj, M.K.; Malardhas, J.P.; Devapriya, I. Machine Learning Approach To Predict Multiple Diseases Based On Symptoms. In Proceedings of the 2024 10th International Conference on Communication and Signal Processing (ICCSP), Melmaruvathur, India, 12–14 April 2024; pp. 1195–1199. [Google Scholar]
- Vyas, N.; Das, P.; Mahajan, Y. The Impact of Air Pollution on Respiratory Health Results: An Analysis of Asthma and COPD in a Population Study. In Proceedings of the 2023 International Conference on Computing, Communication, and Intelligent Systems (ICCCIS), Greater Noida, India, 3–4 November 2023; pp. 141–146. [Google Scholar]
- Lu, Y.; Wang, J.; Wang, D.; Yoo, C.; Liu, H. Incorporating temporal multi-head self-attention convolutional networks and LightGBM for indoor air quality prediction. Appl. Soft Comput. 2024, 157, 111569. [Google Scholar] [CrossRef]
- Arias, J.; Ramos, M.I.; Cubillas, J.J. Predicting emergency health care demands due to respiratory diseases. Int. J. Med. Inform. 2023, 177, 105163. [Google Scholar] [CrossRef]
- Yadav, P.; Rastogi, V.; Yadav, A.; Parashar, P. Artificial Intelligence: A Promising Tool in Diagnosis of Respiratory Diseases. Intell. Pharm. 2024, 2, 784–791. [Google Scholar] [CrossRef]
- Pyingkodi, M.; Thenmozhi, K.; NR, W.B.; Selvaraj, P.; Kumar, K.; Aadarsh, V. Asthma Disease Risk Prediction Using Machine Learning Techniques. In Proceedings of the 2023 International Conference on Computer Communication and Informatics (ICCCI), Coimbatore, India, 23–25 January 2023; pp. 1766–1771. [Google Scholar]
- Jothi, E.S.J.; Justin, J.; Vanithamani, R.; Varsha, R. On-mask sensor network for lung disease monitoring. Biomed. Signal Process. Control 2023, 83, 104655. [Google Scholar]
- Huang, C.H.; Chou, K.T.; Perng, D.W.; Hsiao, Y.H.; Huang, C.W. Using Machine Learning with Impulse Oscillometry Data to Develop a Predictive Model for Chronic Obstructive Pulmonary Disease and Asthma. J. Pers. Med. 2024, 14, 398. [Google Scholar] [CrossRef]
- Xie, F.; Yuan, H.; Ning, Y.; Ong, M.E.H.; Feng, M.; Hsu, W.; Chakraborty, B.; Liu, N. Deep learning for temporal data representation in electronic health records: A systematic review of challenges and methodologies. J. Biomed. Inform. 2022, 126, 103980. [Google Scholar] [CrossRef] [PubMed]
- Raj, R.S.; Kusuma, M. A Comprehensive Analysis of Chronic Health Diseases using Big Data. In Proceedings of the 2023 International Conference on Evolutionary Algorithms and Soft Computing Techniques (EASCT), Bengaluru, India, 20–21 October 2023; pp. 1–5. [Google Scholar]
- Xu, S.; Deo, R.C.; Soar, J.; Barua, P.D.; Faust, O.; Homaira, N.; Jaffe, A.; Kabir, A.L.; Acharya, U.R. Automated detection of airflow obstructive diseases: A systematic review of the last decade (2013–2022). Comput. Methods Programs Biomed. 2023, 241, 107746. [Google Scholar] [CrossRef]
- Feng, Y.; Qin, Y.; Zhao, S. Correlation-split and Recombination-sort Interaction Networks for air quality forecasting. Appl. Soft Comput. 2023, 145, 110544. [Google Scholar] [CrossRef]
- Høj, S.; Thomsen, S.F.; Ulrik, C.S.; Meteran, H.; Sigsgaard, T.; Meteran, H. Evaluating the scientific reliability of ChatGPT as a source of information on asthma. J. Allergy Clin. Immunol. Glob. 2024, 3, 100330. [Google Scholar] [CrossRef]
- Alabdulmohsen, D.M.; Almahmudi, M.A.; Alhashim, J.N.; Almahdi, M.H.; Alkishy, E.F.; Almossabeh, M.J.; Alkhalifah, S.A. Is ChatGPT a Reliable Source of Patient Information on Asthma? Cureus 2024, 16, e64114. [Google Scholar] [CrossRef]
- Kernitskyi, V.; Poberezhets, V.; Demchuk, A.; Slepchenko, N.; Konstantynovych, T.; Viltsaniuk, O.; Ovcharuk, M.; Dovhan, A. Assessing the potential of using ChatGPT by patients with asthma. Eur. Respir. J. 2024, 68, PA4377. [Google Scholar]
- Luo, H.; Yan, J.; Zhou, X. Evaluating artificial intelligence responses to respiratory medicine questions. Respirology 2024, 29, 640–643. [Google Scholar] [CrossRef]
- Almuhanna, H.; Alenezi, M.; Abualhasan, M.; Alajmi, S.; Alfadhli, R.; Karar, A.S. AI Asthma Guard: Predictive Wearable Technology for Asthma Management in Vulnerable Populations. Appl. Syst. Innov. 2024, 7, 78. [Google Scholar] [CrossRef]
- Caruccio, L.; Cirillo, S.; Polese, G.; Solimando, G.; Sundaramurthy, S.; Tortora, G. Can ChatGPT provide intelligent diagnoses? A comparative study between predictive models and ChatGPT to define a new medical diagnostic bot. Expert Syst. Appl. 2024, 235, 121186. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Score | Description |
|---|---|
| 1 | Miscellaneous diseases analyzed using ML or DL techniques |
| 2 | Pediatric asthma analyzed with ML or DL models |
| 3 | Environmental or respiratory data with ML or DL techniques |
| 4 | Adult asthma with environmental or EHR data and ML or DL algorithms |
| 5 | Adult asthma with combination of environmental and EHR data using ML or DL methods |
| Data Source | Advantage | Disadvantage | Accessibility | Weblink |
|---|---|---|---|---|
| Disease symptoms | Organized list of diseases including lungs and asthma with associated symptoms | Lack of detail for the patient demographics | Public | https://www.kaggle.com/datasets/dhivyeshrk/diseases-and-symptoms-dataset (accessed on 15 January 2025) |
| OpenWeather map | Provides several weather data parameters useful in asthma-environment prediction | Application programmable interface (API) is required with limited usage | Public | https://openweathermap.org/ (accessed on 15 January 2025) |
| Hospitals’ EHRs | Offers multi-modal data containing laboratory, treatment, clinical and medical history | Management, acquisition, and interpretation is difficult, requiring expertise | Public, Private | MIMIC, eICU collaborative database, TriNetX, Epic Cosmos |
| Chest radiographs | Provides huge amount of chest X-ray images useful in respiratory disease analysis including asthma | Major sampling focus is pneumonia with a lack of other conditions | Public | https://www.kaggle.com/datasets/paultimothymooney/chest-xray-pneumonia (accessed on 15 January 2025) |
| Pollution data | Air quality data access for multiple Indian locations in real time | Data availability and details may be limited with respect to provided regions | Public | https://cpcb.nic.in/real-time-air-qulity-data/ (accessed on 15 January 2025) |
| Respiratory sound | Multiple respiratory audio recordings offering deep analysis including asthma | Data annotations may be needed with careful interpretation | Public | https://www.kaggle.com/datasets/vbookshelf/respiratory-sound-database (accessed on 15 January 2025) |
| Models | Advantage | Disadvantage |
|---|---|---|
| Ensemble |
|
|
| Hybrid |
|
|
| CNN |
|
|
| Decision Tree |
|
|
| ANN |
|
|
| Author | ML/DL Model | Data Type | Pre-Processing | Performance | ||
|---|---|---|---|---|---|---|
| Env. | EHR | Aug. | Data Handling | |||
| Sridhar A. et al. [45] | Bagging (KNN, SVM, DT, RF, NB, ANN) | ✓ | ✓ | Acc: 98.84% | ||
| Topaloglu I. et al. [38] | Hybrid (ResNet-18, SVM) | ✓ | ✓ | Acc: 99.1% | ||
| Sudipto B. et al. [33] | Multi-Layer Perceptron | ✓ | ✓ | Acc: 85.7% | ||
| Khasha R. et al. [25] | Ensemble (SVM, Tree, LR, KNN, NB, RF, XGBoost) | ✓ | ✓ | ✓ | ✓ | Acc: 92.15% |
| Lu Y. et al. [58] | Hybrid (TCN, Gradient Boosting) | ✓ | ✓ | RMSE: 60.2, MAE: 4.36 | ||
| Arias J. et al. [59] | SVM | ✓ | ✓ | ✓ | Error Improved 15% | |
| Yahyaoui A. et al. [26] | KNN | ✓ | Acc: 95% | |||
| Abeda B. et al. [55] | Decision Trees | ✓ | ✓ | ✓ | RMSE: 0.07 | |
| Raj M. et al. [56] | RF | ✓ | ✓ | Acc: 98% | ||
| Bhat G. et al. [30] | CNN | ✓ | ✓ | RMSE: 2.42 | ||
| Abirami S. et al. [20] | Hybrid (CNN-LSTM) | ✓ | ✓ | MAE: 4.16, Rsquare: 0.94 | ||
| Lee Z. et al. [54] | XGBoost | ✓ | ✓ | ✓ | Acc: 94.03% | |
| Alharbi E. et al. [39] | XGBoost | ✓ | ✓ | ✓ | ✓ | Acc: 94% |
| Bhowmik R. et al. [35] | Hybrid (CNN-RNN) | ✓ | ✓ | ✓ | Acc: 93.4% | |
| Hee H. et al. [43] | GMM | ✓ | ✓ | Acc: 83.76% | ||
| Bae W. et al. [31] | Transfer Learning (LR, FcNN) | ✓ | ✓ | ✓ | ✓ | Acc: 73.8% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alkobaisi, S.; Safdar, M.F.; Pałka, P.; Abu Ali, N.A. Artificial Intelligence Algorithms in Asthma Management: A Review of Data Engineering, Predictive Models, and Future Implications. Appl. Sci. 2025, 15, 3609. https://doi.org/10.3390/app15073609
Alkobaisi S, Safdar MF, Pałka P, Abu Ali NA. Artificial Intelligence Algorithms in Asthma Management: A Review of Data Engineering, Predictive Models, and Future Implications. Applied Sciences. 2025; 15(7):3609. https://doi.org/10.3390/app15073609
Chicago/Turabian StyleAlkobaisi, Shayma, Muhammad Farhan Safdar, Piotr Pałka, and Najah Abed Abu Ali. 2025. "Artificial Intelligence Algorithms in Asthma Management: A Review of Data Engineering, Predictive Models, and Future Implications" Applied Sciences 15, no. 7: 3609. https://doi.org/10.3390/app15073609
APA StyleAlkobaisi, S., Safdar, M. F., Pałka, P., & Abu Ali, N. A. (2025). Artificial Intelligence Algorithms in Asthma Management: A Review of Data Engineering, Predictive Models, and Future Implications. Applied Sciences, 15(7), 3609. https://doi.org/10.3390/app15073609