



Establishing Reference Data for Electromyographic Activity in Gait: Age and Gender Variations


Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics Statement
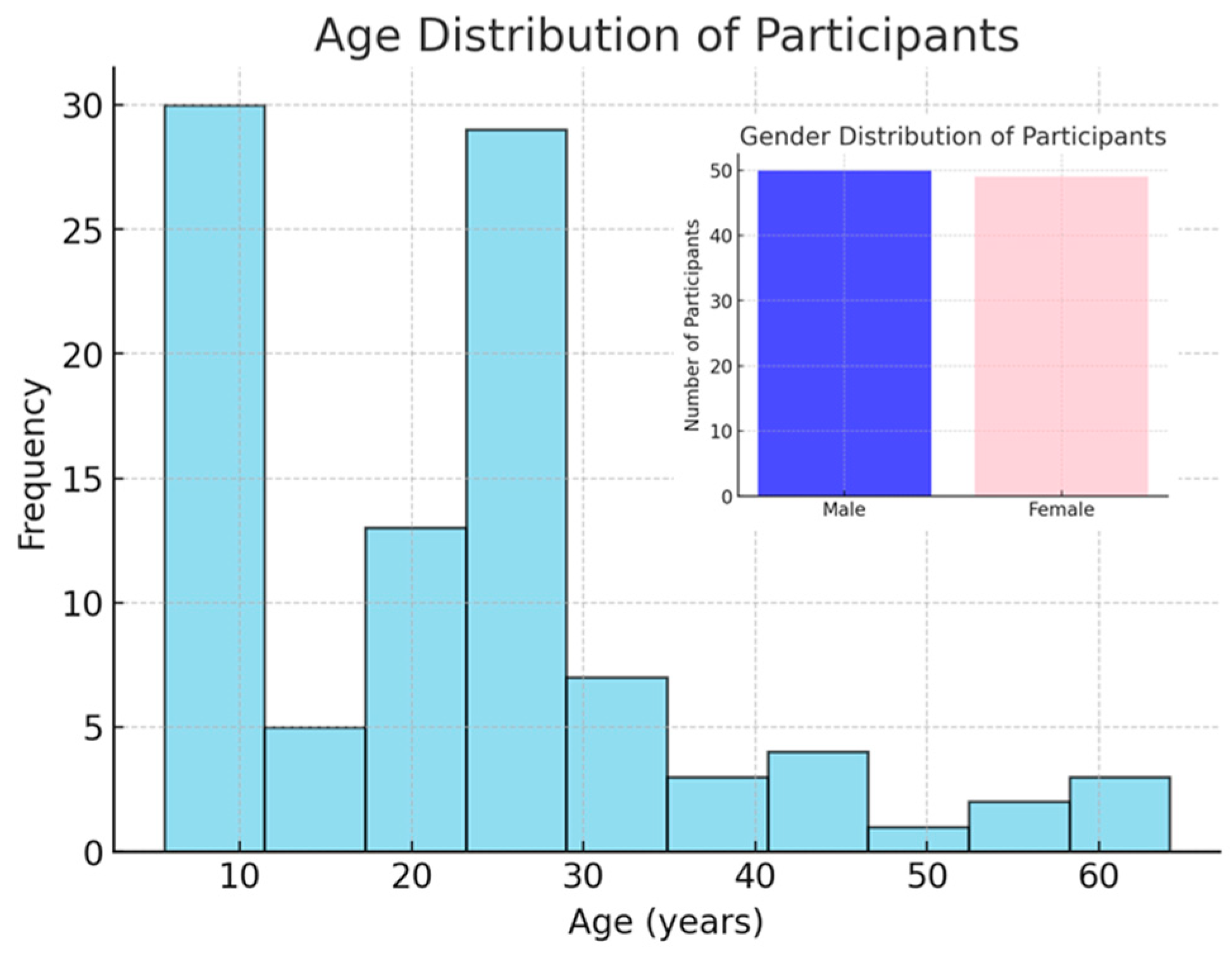
2.2. Participants
2.3. Instrumentation and Protocol
2.4. Signal Processing
2.5. Statistical Analysis
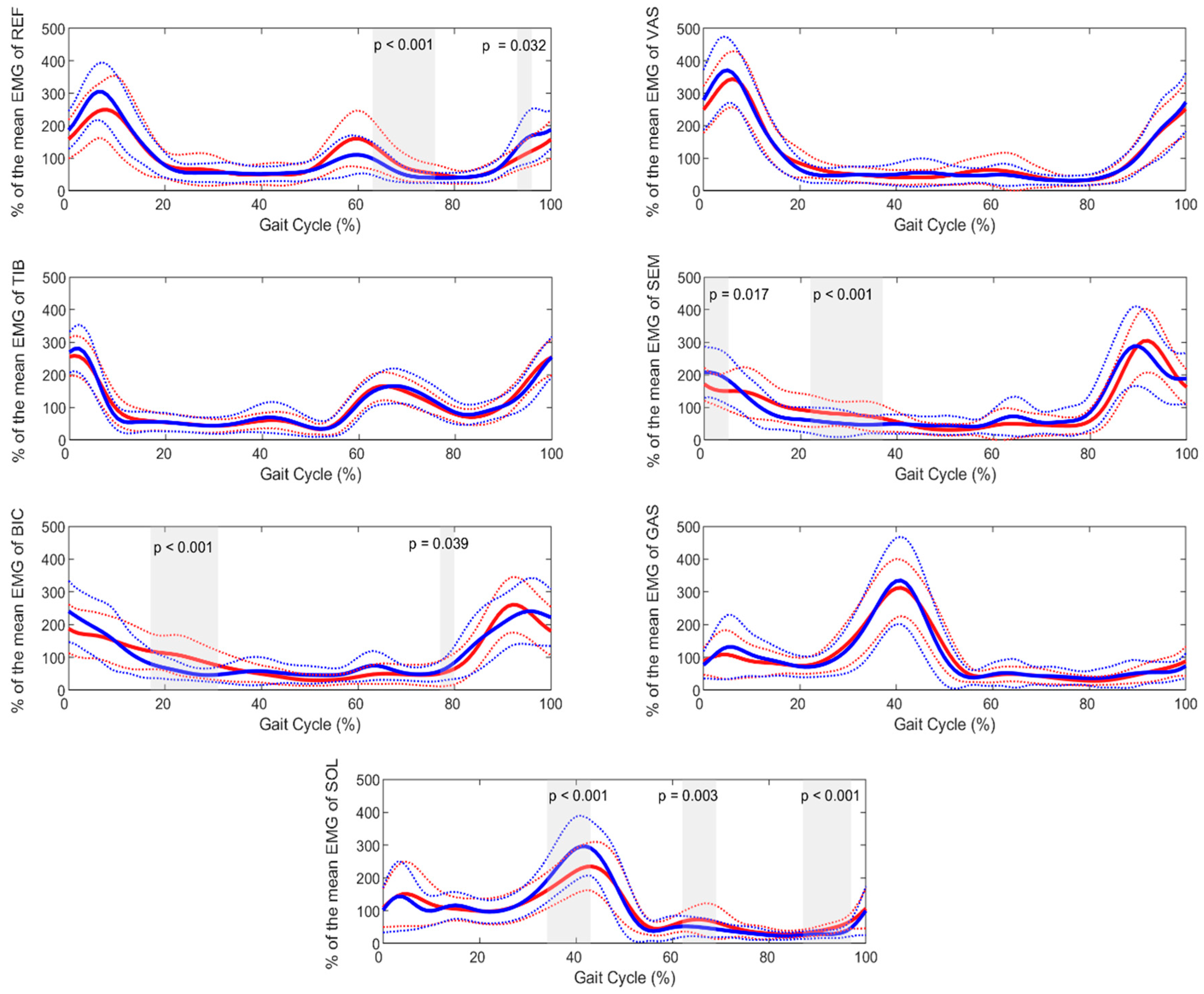
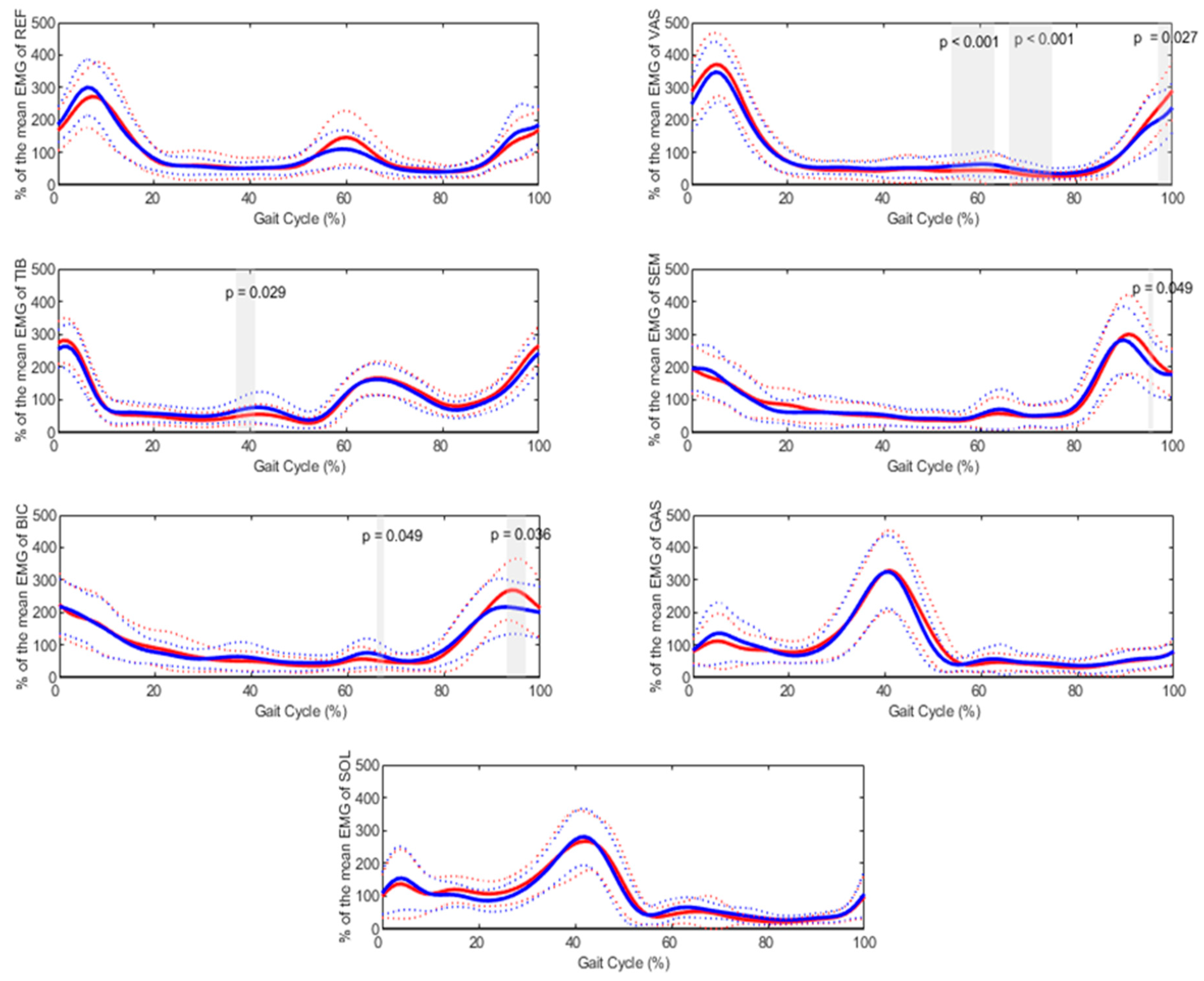
3. Results
4. Discussion
5. Limitations and Future Studies
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Davoudi, M.; Salami, F.; Reisig, R.; Patikas, D.A.; Beckmann, N.A.; Gather, K.S.; Wolf, S.I. Are Electromyography Data a Fingerprint for Patients with Cerebral Palsy (CP)? Appl. Sci. 2025, 15, 766. [Google Scholar] [CrossRef]
- Davoudi, M.; Salami, F.; Reisig, R.; Gather, K.S.; Wolf, S.I. Gluteus medius muscle activation patterns during gait with Cerebral Palsy (CP): A hierarchical clustering analysis. PLoS ONE 2025, 20, e0309582. [Google Scholar]
- Davoudi, M.; Salami, F.; Reisig, R.; Patikas, D.A.; Wolf, S.I. Rectus femoris electromyography signal clustering: Data-driven management of crouch gait in patients with cerebral palsy. PLoS ONE 2024, 19, e0298945. [Google Scholar] [CrossRef]
- Dreher, T.; Wolf, S.I.; Maier, M.; Hagmann, S.; Vegvari, D.; Gantz, S.; Heitzmann, D.; Wenz, W.; Braatz, F. Long-term results after distal rectus femoris transfer as a part of multilevel surgery for the correction of stiff-knee gait in spastic diplegic cerebral palsy. J. Bone Jt. Surg. 2012, 94, e142. [Google Scholar] [CrossRef]
- Agostini, V.; Ghislieri, M.; Rosati, S.; Balestra, G.; Knaflitz, M. Surface electromyography applied to gait analysis: How to improve its impact in clinics? Front. Neurol. 2020, 11, 994. [Google Scholar]
- Reisig, R.; Alexander, N.; Armand, S.; Barton, G.J.; Böhm, H.; Boulay, C.; Brunner, R.; Castagna, A.; Davoudi, M.; Desailly, E. Status of surface electromyography assessment as part of clinical gait analysis in the management of patients with cerebral palsy–Outcomes of a Delphi process. Gait Posture 2025, 117, 72–77. [Google Scholar]
- Schwartz, M.H.; Rozumalski, A.; Trost, J.P. The effect of walking speed on the gait of typically developing children. J. Biomech. 2008, 41, 1639–1650. [Google Scholar]
- Bovi, G.; Rabuffetti, M.; Mazzoleni, P.; Ferrarin, M. A multiple-task gait analysis approach: Kinematic, kinetic and EMG reference data for healthy young and adult subjects. Gait Posture 2011, 33, 6–13. [Google Scholar] [PubMed]
- Cho, S.-H.; Park, J.M.; Kwon, O.Y. Gender differences in three dimensional gait analysis data from 98 healthy Korean adults. Clin. Biomech. 2004, 19, 145–152. [Google Scholar]
- Kerrigan, D.C.; Todd, M.K.; Croce, U.D. Gender differences in joint biomechanics during walking normative study in young adults. Am. J. Phys. Med. Rehabil. 1998, 77, 2–7. [Google Scholar]
- Santuz, A.; Janshen, L.; Brüll, L.; Munoz-Martel, V.; Taborri, J.; Rossi, S.; Arampatzis, A. Sex-specific tuning of modular muscle activation patterns for locomotion in young and older adults. PLoS ONE 2022, 17, e0269417. [Google Scholar]
- Bailey, C.A.; Corona, F.; Pilloni, G.; Porta, M.; Fastame, M.C.; Hitchcott, P.K.; Penna, M.P.; Pau, M.; Côté, J.N. Sex-dependent and sex-independent muscle activation patterns in adult gait as a function of age. Exp. Gerontol. 2018, 110, 1–8. [Google Scholar] [PubMed]
- Sloot, L.H.; Malheiros, S.; Truijen, S.; Saeys, W.; Mombaur, K.; Hallemans, A.; Van Criekinge, T. Decline in gait propulsion in older adults over age decades. Gait Posture 2021, 90, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, Y.; Hobara, H.; Heldoorn, T.A.; Kouchi, M.; Mochimaru, M. Age-independent and age-dependent sex differences in gait pattern determined by principal component analysis. Gait Posture 2016, 46, 11–17. [Google Scholar] [CrossRef]
- Di Nardo, F.; Mengarelli, A.; Maranesi, E.; Burattini, L.; Fioretti, S. Gender differences in the myoelectric activity of lower limb muscles in young healthy subjects during walking. Biomed. Signal Process. Control 2015, 19, 14–22. [Google Scholar]
- Di Nardo, F.; Laureati, G.; Strazza, A.; Mengarelli, A.; Burattini, L.; Agostini, V.; Nascimbeni, A.; Knaflitz, M.; Fioretti, S. Is child walking conditioned by gender? Surface EMG patterns in female and male children. Gait Posture 2017, 53, 254–259. [Google Scholar]
- Schmitz, A.; Silder, A.; Heiderscheit, B.; Mahoney, J.; Thelen, D.G. Differences in lower-extremity muscular activation during walking between healthy older and young adults. J. Electromyogr. Kinesiol. 2009, 19, 1085–1091. [Google Scholar]
- Pataky, T.C. Generalized n-dimensional biomechanical field analysis using statistical parametric mapping. J. Biomech. 2010, 43, 1976–1982. [Google Scholar]
- Kadaba, M.P.; Ramakrishnan, H.K.; Wootten, M.E. Measurement of lower extremity kinematics during level walking. J. Orthop. Res. 1990, 8, 383–392. [Google Scholar] [CrossRef]
- Hermens, H.J.; Freriks, B.; Merletti, R.; Stegeman, D.; Blok, J.; Rau, G.; Disselhorst-Klug, C.; Hägg, G. European recommendations for surface electromyography. Roessingh Res. Dev. 1999, 8, 13–54. [Google Scholar]
- Patikas, D.; Wolf, S.I.; Schuster, W.; Armbrust, P.; Dreher, T.; Döderlein, L. Electromyographic patterns in children with cerebral palsy: Do they change after surgery? Gait Posture 2007, 26, 362–371. [Google Scholar] [CrossRef]
- Wolf, S.I.; Mikut, R.; Kranzl, A.; Dreher, T. Which functional impairments are the main contributors to pelvic anterior tilt during gait in individuals with cerebral palsy? Gait Posture 2014, 39, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Wolf, S.; Loose, T.; Schablowski, M.; Döderlein, L.; Rupp, R.; Gerner, H.J.; Bretthauer, G.; Mikut, R. Automated feature assessment in instrumented gait analysis. Gait Posture 2006, 23, 331–338. [Google Scholar] [CrossRef]
- Wu, M.; Liao, L.; Luo, X.; Ye, X.; Yao, Y.; Chen, P.; Shi, L.; Huang, H.; Wu, Y. Analysis and classification of stride patterns associated with children development using gait signal dynamics parameters and ensemble learning algorithms. BioMed Res. Int. 2016, 2016, 9246280. [Google Scholar] [CrossRef] [PubMed]
- Nene, A.; Mayagoitia, R.; Veltink, P. Assessment of rectus femoris function during initial swing phase. Gait Posture 1999, 9, 1–9. [Google Scholar] [CrossRef]
- Augsburger, S.; White, H.; Iwinski, H. Midstance hamstring length is a better indicator for hamstring lengthening procedures than initial contact length. Gait Posture 2020, 80, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Konrath, J.M.; Saxby, D.J.; Killen, B.A.; Pizzolato, C.; Vertullo, C.J.; Barrett, R.S.; Lloyd, D.G. Muscle contributions to medial tibiofemoral compartment contact loading following ACL reconstruction using semitendinosus and gracilis tendon grafts. PLoS ONE 2017, 12, e0176016. [Google Scholar] [CrossRef]
- DeMont, R.G.; Lephart, S.M. Effect of sex on preactivation of the gastrocnemius and hamstring muscles. Br. J. Sports Med. 2004, 38, 120–124. [Google Scholar] [CrossRef]
- Ko, S.-u.; Tolea, M.I.; Hausdorff, J.M.; Ferrucci, L. Sex-specific differences in gait patterns of healthy older adults: Results from the Baltimore Longitudinal Study of Aging. J. Biomech. 2011, 44, 1974–1979. [Google Scholar] [CrossRef]
- Chappell, J.D.; Creighton, R.A.; Giuliani, C.; Yu, B.; Garrett, W.E. Kinematics and electromyography of landing preparation in vertical stop-jump: Risks for noncontact anterior cruciate ligament injury. Am. J. Sports Med. 2007, 35, 235–241. [Google Scholar] [CrossRef]
- Sigward, S.M.; Powers, C.M. The influence of gender on knee kinematics, kinetics and muscle activation patterns during side-step cutting. Clin. Biomech. 2006, 21, 41–48. [Google Scholar]
- Chiu, M.-C.; Wang, M.-J. The effect of gait speed and gender on perceived exertion, muscle activity, joint motion of lower extremity, ground reaction force and heart rate during normal walking. Gait Posture 2007, 25, 385–392. [Google Scholar] [PubMed]
- Cammarata, M.L.; Dhaher, Y.Y. The differential effects of gender, anthropometry, and prior hormonal state on frontal plane knee joint stiffness. Clin. Biomech. 2008, 23, 937–945. [Google Scholar]
- Ko, S.-u.; Hausdorff, J.M.; Ferrucci, L. Age-associated differences in the gait pattern changes of older adults during fast-speed and fatigue conditions: Results from the Baltimore longitudinal study of ageing. Age Ageing 2010, 39, 688–694. [Google Scholar]
- Kimura, T.; Kobayashi, H.; Nakayama, E.; Hanaoka, M. Effects of aging on gait patterns in the healthy elderly. Anthropol. Sci. 2007, 115, 67–72. [Google Scholar]
- Hof, A.L.; Elzinga, H.; Grimmius, W.; Halbertsma, J.P.K. Speed dependence of averaged EMG profiles in walking. Gait Posture 2002, 16, 78–86. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Age Group | Gender Group | No. | Age (Years) | Age Range (Min–Max) | Height (cm) | Body Mass (kg) | |
|---|---|---|---|---|---|---|---|
| Children | Male | 21 | 9.36 (1.77) | 5.7–12.7 | 137.76 (11.89) | 33.02 (88.82) | 17.04 (2.14) |
| Female | 14 | 9.28 (2.19) | 5.6–12.6 | 138.42 (15.16) | 34.37 (13.78) | 17.02 (4.06) | |
| Adults | Male | 29 | 31.42 (10.86) | 21.2–64.1 | 180.55 (7.16) | 77.25 (8.71) | 23.69 (2.33) |
| Female | 33 | 28.7 (11.03) | 18.2–62.6 | 168.84 (11.03) | 62.88 (7.6) | 22.04 (2.17) |
| Variable | Age Group | Mean (SD) | 95% Confidence Interval (Lower–Upper Bound) | p-Value |
|---|---|---|---|---|
| Maximum ankle dorsiflexion moment (N.m/kg) | Children | 1.28 (0.17) | 1.22–1.34 | <0.001 |
| Adults | 1.59 (0.17) | 1.55–1.64 | ||
| Maximum ankle dorsiflexion power (W/kg) | Children | 3.62 (0.86) | 3.32–3.91 | <0.001 |
| Adults | 4.59 (0.95) | 4.34–4.83 | ||
| Maximum ankle plantarflexion power (W/kg) | Children | 0.76 (0.38) | 0.62–0.89 | 0.012 |
| Adults | 0.95 (0.33) | 0.86–1.03 | ||
| Maximum knee flexion moment (N.m/kg) | Children | 0.48 (0.16) | 0.42–0.54 | 0.004 |
| Adults | 0.6 (0.2) | 0.55–0.65 | ||
| Maximum hip flexion (degree) | Children | 36.9 (6.3) | 34.7–39.1 | 0.018 |
| Adults | 33.9 (5.4) | 32.5–35.3 | ||
| Maximum hip extension moment (N.m/kg) | Children | 0.88 (0.22) | 0.8–0.95 | <0.001 |
| Adults | 1.08 (0.27) | 1.01–1.15 | ||
| Cadence (strides/min) | Children | 128.1 (10.2) | 124.6–131.6 | <0.001 |
| Adults | 115.2 (8) | 113.2–117.3 | ||
| Speed (m/s) | Children | 1.29 (0.15) | 1.23–1.34 | 0.001 |
| Adults | 1.39 (0.13) | 1.35–1.42 | ||
| Stride time (s) | Children | 0.94 (0.07) | 0.91–0.96 | <0.001 |
| Adults | 1.04 (0.07) | 1.02–1.06 | ||
| Stride length (m) | Children | 1.21 (0.15) | 1.16–1.26 | <0.001 |
| Adults | 1.45 (0.12) | 1.42–1.48 |
| Variable | Gender Group | Mean (SD) | 95% Confidence Interval (Lower–Upper Bound) | p Value |
|---|---|---|---|---|
| Maximum ankle plantarflexion (degree) | Males | 18.4 (5.7) | 16.8–20.1 | 0.023 |
| Females | 21.5 (7.1) | 19.4–37.3 | ||
| Maximum ankle dorsiflexion power (W/kg) | Males | 4.03 (1) | 3.74–4.32 | 0.041 |
| Females | 4.46 (1) | 4.1–4.75 | ||
| Maximum hip flexion (degree) | Males | 33.6 (5.6) | 31.9–35.2 | 0.012 |
| Females | 36.6 (5.9) | 34.8–38.3 | ||
| Maximum hip extension power (W/kg) | Males | 0.97 (0.3) | 0.88–1.05 | 0.042 |
| Females | 1.1 (0.33) | 1–1.2 | ||
| Foot off (% gait cycle) | Males | 61.4 (2.1) | 60.8–62 | 0.024 |
| Females | 60.5 (1.9) | 59.9–61 |
| Dependent Variable | Age Group | Gender Group | Mean (SD) | 95% Confidence Interval (Lower–Upper Bound) | p Value for Pairwise Comparisons | p Value for Interaction Age-Gender | Cohen’s f2 |
|---|---|---|---|---|---|---|---|
| Mean activity of BIC in stance | Children | Male | 90.4 (2.7) | 84.9–95.9 | 0.056 | 0.002 | 0.141 |
| Female | 81.9 (3.3) | 75.2–88.7 | |||||
| Adults | Male | 79.1 (2.3) | 74.3–83.7 | 0.006 | |||
| Female | 88.1 (2.2) | 83.7–92.5 | |||||
| Mean activity of BIC in swing | Children | Male | 116.9 (17.8) | 108.5–125.3 | 0.04 | <0.001 | 0.177 |
| Female | 130.9 (14.6) | 120.6–141.2 | |||||
| Adults | Male | 136.8 (23) | 129.6–144 | 0.002 | |||
| Female | 121 (18.7) | 114.2–127.7 | |||||
| Maximum activity of BIC in swing | Children | Male | 278.5 (61.8) | 247.5–309.3 | 0.151 | <0.001 | 0.199 |
| Female | 314.1 (46.5) | 276.2–351.9 | |||||
| Adults | Male | 340.6 (85.4) | 314.3–366.9 | <0.001 | |||
| Female | 268 (71.7) | 243.3–292.6 | |||||
| Mean activity of SEM in stance | Children | Male | 85.1 (2.9) | 79.2–91 | 0.061 | 0.006 | 0.141 |
| Female | 76.2 (3.6) | 69–83.4 | |||||
| Adults | Male | 71.2 (2.5) | 66.2–76.3 | 0.036 | |||
| Female | 78.6 (2.3) | 73.9–83.3 | |||||
| Mean activity of SEM in swing | Children | Male | 126.1 (4.6) | 116.9–135.4 | 0.093 | 0.006 | 0.151 |
| Female | 138.6 (5.6) | 127.3–149.9 | |||||
| Adults | Male | 148.5 (3.9) | 140.6–156.4 | 0.018 | |||
| Female | 135.4 (3.7) | 128.1–142.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davoudi, M.; Salami, F.; Putz, C.; Wolf, S.I. Establishing Reference Data for Electromyographic Activity in Gait: Age and Gender Variations. Appl. Sci. 2025, 15, 3472. https://doi.org/10.3390/app15073472
Davoudi M, Salami F, Putz C, Wolf SI. Establishing Reference Data for Electromyographic Activity in Gait: Age and Gender Variations. Applied Sciences. 2025; 15(7):3472. https://doi.org/10.3390/app15073472
Chicago/Turabian StyleDavoudi, Mehrdad, Firooz Salami, Cornelia Putz, and Sebastian I. Wolf. 2025. "Establishing Reference Data for Electromyographic Activity in Gait: Age and Gender Variations" Applied Sciences 15, no. 7: 3472. https://doi.org/10.3390/app15073472
APA StyleDavoudi, M., Salami, F., Putz, C., & Wolf, S. I. (2025). Establishing Reference Data for Electromyographic Activity in Gait: Age and Gender Variations. Applied Sciences, 15(7), 3472. https://doi.org/10.3390/app15073472