
Smart App and Wearable Device-Based Approaches for Contactless Public Healthcare for Adolescents in Korea



Abstract
1. Introduction
2. Methods
2.1. Participation
2.2. Procedures
2.3. Body Composition
2.4. Physical Fitness
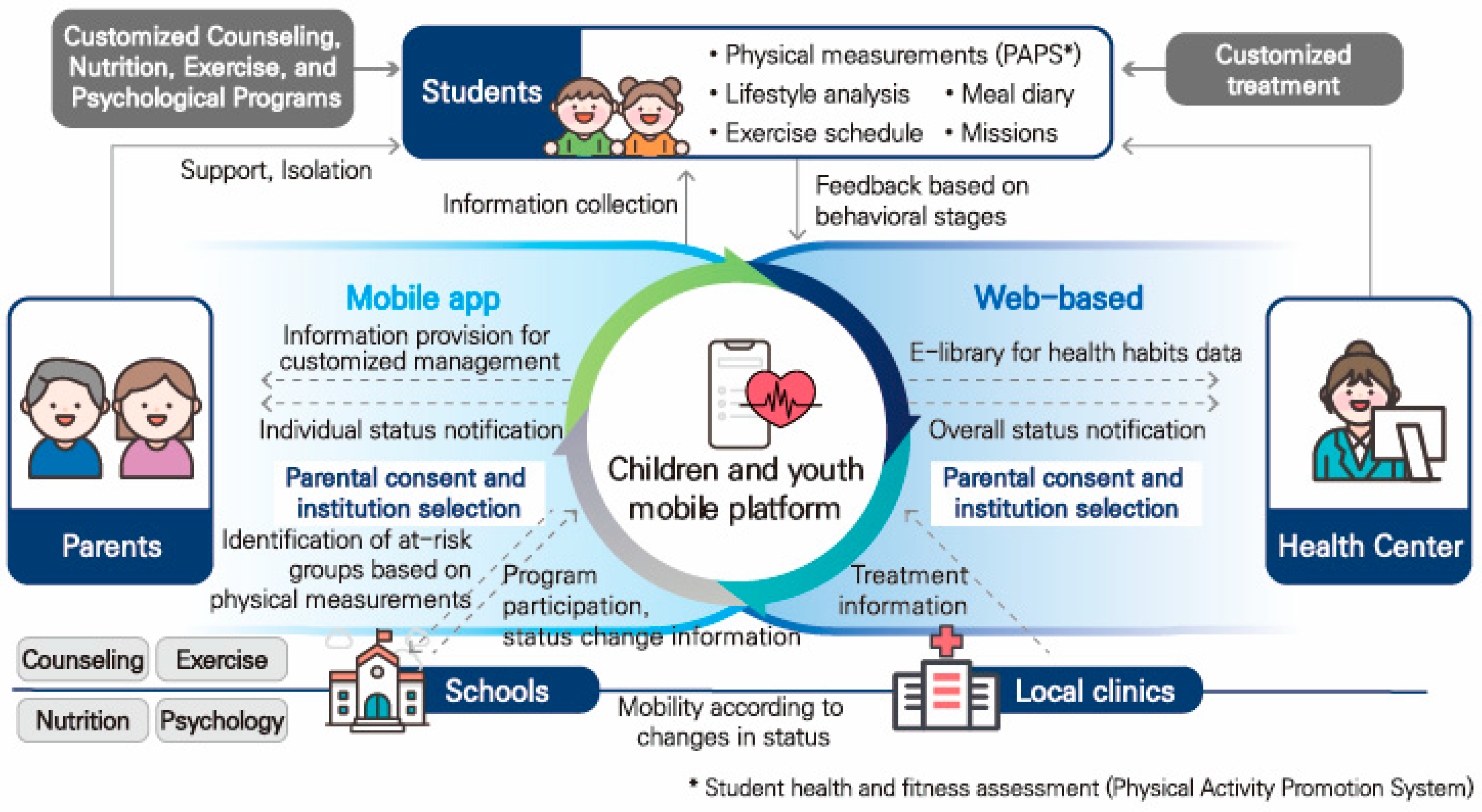
2.5. Smartphone-Based Healthcare APP; Future Health
2.6. The International Physical Activity Questionnaire (IPAQ)
2.7. Statistical Analysis
3. Results
3.1. Changes Before and After 24 Weeks Wearing the Smart Band
3.2. Changes in Adolescents Relative to Urban or Rural Regions
3.3. Changes in Female Adolescents Relative to Urban or Rural Regions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Obesity. Available online: https://www.who.int/health-topics/obesity#tab=tab_1 (accessed on 10 October 2023).
- Kim, J.H.; Moon, J.S. Secular trends in pediatric overweight and obesity in Korea. J. Obes. Metab. Syndr. 2020, 29, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Park, H.K.; Seo, J.Y.; Jung, H.W.; Lim, J.S. Prevalence and trends in obesity and severe obesity in Korean children and adolescents, 2007–2020: A population-based study. Pediatr. Int. 2023, 65, e15472. [Google Scholar] [CrossRef] [PubMed]
- Faienza, M.F.; Chiarito, M.; Molina-Molina, E.; Shanmugam, H.; Lammert, F.; Krawczyk, M.; D’aMato, G.; Portincasa, P. Childhood obesity, cardiovascular, and liver health: A growing epidemic with age. World J. Pediatr. 2020, 16, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Fruh, S.; Williams, S.; Hayes, K.; Hauff, C.; Hudson, G.M.; Sittig, S.; Graves, R.J.P.; Hall, H.P.; Barinas, J.M.S. A practical approach to obesity prevention: Healthy home habits. J. Am. Assoc. Nurse Pract. 2021, 33, 1055–1065. [Google Scholar] [CrossRef] [PubMed]
- Son, W.M.; Sung, K.D.; Bharath, L.P.; Choi, K.J.; Park, S.Y. Combined exercise training reduces blood pressure, arterial stiffness, and insulin resistance in obese prehypertensive adolescent girls. Clin. Exp. Hypertens. 2017, 39, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Júdice, P.B.; Silva, A.M.; Berria, J.; Petroski, E.L.; Ekelund, U.; Sardinha, L.B. Sedentary patterns, physical activity and health-related physical fitness in youth: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 25. [Google Scholar] [CrossRef] [PubMed]
- Alves, J.G.B.; Alves, G.V. Effects of physical activity on children’s growth. J. Pediatr. Rio. J. 2019, 95, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Rossi, L.; Behme, N.; Breuer, C. Physical Activity of Children and Adolescents during the COVID-19 Pandemic-A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 11440. [Google Scholar] [CrossRef] [PubMed]
- The Lancet Child Adolescent Health. Promoting physical activity in children and adolescents. Lancet Child. Adolesc. Health 2020, 6, 829. [Google Scholar]
- Katanic, B.; Bjelica, D.; Stankovic, M.; Milosevic, Z.; Vukovic, J.; Mekic, A. Anthropometric Characteristics and Weight Status of Early Adolescents (Aged 12–14) in Montenegro; Urban–Rural and Regional Differences. Children 2023, 10, 1664. [Google Scholar] [CrossRef] [PubMed]
- Katanic, B.; Bjelica, D.; Stankovic, M.; Vukovic, J.; Milosevic, Z.; Đorđević, D.; Curic, M. Association of Weight Status with Geographic Region, Residential Status and Sex of 8th Grade School Children: The Prevalence of Overweight and Obesity in Montenegro. Sport Mont 2024, 22, 55–60. [Google Scholar] [CrossRef]
- Cho, J.H.; Kim, D.J.; Lim, S.T. Health Promotion Management of Adolescence Based on Digital Healthcare: ICT Health Monitoring. Indian J. Pediatr. 2024, 91, 307. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Education. Physical Activity Promotion System Measurement Manual; Ministry of Education: Seoul, Republic of Korea, 2009. [Google Scholar]
- Kim, D.J.; Kim, I.K.; Oh, Y.S.; Shin, Y.J. Development of Web-based Personal Exercise Prescription System for Health Management. Asian J. Kinesiol. 2021, 12, 73–82. [Google Scholar]
- American College of Sports Medicine (ACSM). ACSM’s Guidelines for Exercise Testing and Prescription, 11th ed.; Wolters Kluwer Health: Philadelphia, PA, USA, 2021. [Google Scholar]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O’Brien, W.L.; Bassett, D.R., Jr.; Schmitz, K.H.; Emplaincourt, P.O.; et al. Compendium of physical activities: An update of activity codes and MET intensities. Med. Sci. Sports Exerc. 2000, 32, 498–504. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.T.; Jung, Y.Z.; Akama, T.; Lee, E. Physical Activity Amount and Cognitive Impairment in Korean Elderly Population. Brain Sci. 2020, 10, 804. [Google Scholar] [CrossRef] [PubMed]
- Jang, W.H.; Lee, S.B.; Kim, D.W.; Lee, Y.H.; Uhm, Y.J.; Yang, S.W.; Kim, J.-H.; Kim, J.-B. ICT-Based Health Care Services for Individuals with Spinal Cord Injuries: A Feasibility Study. Sensors 2020, 20, 2491. [Google Scholar] [CrossRef] [PubMed]
- Elliott, T.R.; Brossart, D.; Berry, J.W.; Fine, P.R. Problem-solving training via videoconferencing for family caregivers of persons with spinal cord injuries: A randomized controlled trial. Behav. Res. Ther. 2008, 46, 1220–1229. [Google Scholar] [CrossRef] [PubMed]
- Sarbadhikari, S.; Sarbadhikari, S.N. The global experience of digital health interventions in COVID-19 management. Indian J. Public Health 2020, 64, S117–S124. [Google Scholar] [CrossRef] [PubMed]
- Reddy, P.; Dukhi, N.; Sewpaul, R.; Ellahebokus, M.A.A.; Kambaran, N.S.; Jobe, W. Mobile Health Interventions Addressing Childhood and Adolescent Obesity in Sub-Saharan Africa and Europe: Current Landscape and Potential for Future Research. Front. Public Health 2021, 9, 604439. [Google Scholar] [CrossRef] [PubMed]
- Stasinaki, A.; Büchter, D.; Shih, C.I.; Heldt, K.; Güsewell, S.; Brogle, B.; Farpour-Lambert, N.; Kowatsch, T.; l’Allemand, D. Effects of a novel mobile health intervention compared to a multi-component behaviour changing program on body mass index, physical capacities and stress parameters in adolescents with obesity: A randomized controlled trial. BMC Pediatr. 2021, 21, 308. [Google Scholar] [CrossRef] [PubMed]
- Trukeschitz, B.; Eisenberg, S.; Schneider, C.; Schneider, U. Exploring the effectiveness of a fitness-app prototype for home care service users in Austria and Italy. Health Soc. Care Community 2020, 30, e2884–e2895. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Moseson, H.; Uppal, J.; Juusola, J.L. A Diabetes Mobile App with In-App Coaching from a Certified Diabetes Educator Reduces A1C for Individuals with Type 2 Diabetes. Diabetes Educ. 2018, 44, 226–236. [Google Scholar] [CrossRef] [PubMed]
- Kang, E.; Park, S.M.; Lee, K.; Lee, E.B.; Yim, J.J.; Lee, J.; Kim, S.; Rhee, Y.E.; Yun, Y.H. Efficacy of Health Coaching and an Electronic Health Management Program: Randomized Controlled Trial. J. Gen. Intern. Med. 2021, 36, 2692–2699. [Google Scholar] [CrossRef] [PubMed]
- Lau, P.W.; Lau, E.Y.; Wong del, P.; Ransdell, L. A systematic review of information and communication technology-based interventions for promoting physical activity behavior change in children and adolescents. J. Med. Internet Res. 2011, 13, e48. [Google Scholar] [CrossRef] [PubMed]
- Chae, M.; Han, K. Differences in Health Behavior Profiles of Adolescents in Urban and Rural Areas in a Korean City. Healthcare 2021, 9, 282. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Liu, L.; Wang, X.; Zhang, X.; Zhai, Y.; Wang, K.; Liu, J. Urban-Rural Differences in Physical Fitness and Out-of-School Physical Activity for Primary School Students: A County-Level Comparison in Western China. Int. J. Environ. Res. Public Health 2021, 18, 10813. [Google Scholar] [CrossRef] [PubMed]
- Boraita, R.J.; Alsina, D.A.; Ibort, E.G.; Torres, J.M.D. Quality of life related to health and habits: Differences between adolescents in rural and urban environments. An. Pediatr. 2022, 96, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Q.; Huang, X.; Cui, D. Rural-Urban Differences in Physical Fitness and Overweight Prevalence of Children and Adolescents from Central South China. Int. J. Environ. Res. Public Health 2023, 20, 2390. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.Y.; Um, Y.J. Factors Affecting Obesity in Urban and Rural Adolescents: Demographic, Socioeconomic Characteristics, Health Behavior and Health Education. Int. J. Environ. Res. Public Health 2021, 18, 2405. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 1261) | Male (n = 660) | Female (n = 601) |
|---|---|---|---|
| Age (years) | 13.45 ± 1.18 | 13.40 ± 1.14 | 13.51 ± 1.23 |
| Height (cm) | 155.33 ± 9.27 | 156.12 ± 10.59 | 154.45 ± 7.48 |
| Weight (kg) | 53.75 ± 18.41 | 56.34 ± 17.13 | 50.90 ± 19.35 |
| BMI (kg/m2) | 21.97 ± 6.42 | 22.72 ± 4.90 | 21.14 ± 7.66 |
| (a) | |||
| Variable | Pre | Post | p-Value |
| Height (cm) | 156.12 ± 10.59 | 158.76 ± 9.97 | <0.001 |
| Weight (kg) | 56.34 ± 17.13 | 58.61 ± 17.50 | 0.060 |
| BMI (kg/m2) | 22.72 ± 4.90 | 22.89 ± 5.00 | 0.640 |
| 20m shuttle run (rep) | 53.45 ± 30.96 | 58.81 ± 30.72 | 0.023 |
| Sit-and-reach (cm) | 6.07 ± 9.40 | 5.56 ± 8.03 | 0.351 |
| Grip strength (kg) | 23.39 ± 8.69 | 26.91 ± 10.26 | <0.001 |
| Sit-ups (rep) | 49.08 ± 44.24 | 52.88 ± 42.75 | 0.596 |
| Long jump (cm) | 149.41 ± 40.92 | 150.16 ± 29.35 | <0.001 |
| 50m run (sec) | 10.31 ± 4.00 | 9.39 ± 1.30 | 0.230 |
| (b) | |||
| Variable | Pre | Post | p-Value |
| Height (cm) | 154.45 ± 7.48 | 156.55 ± 6.93 | <0.001 |
| Weight (kg) | 50.90 ± 19.35 | 52.06 ± 12.32 | 0.241 |
| BMI (kg/m2) | 21.14 ± 7.66 | 21.11 ± 4.14 | 0.984 |
| 20m shuttle run (rep) | 35.67 ± 17.36 | 58.69 ± 26.04 | <0.001 |
| Sit-and-reach (cm) | 11.98 ± 9.01 | 12.14 ± 9.24 | 0.776 |
| Grip strength (kg) | 22.41 ± 6.70 | 24.03 ± 7.25 | 0.003 |
| Sit-ups (rep) | 27.74 ± 16.74 | 40.47 ± 38.30 | 0.022 |
| Long jump (cm) | 142.00 ± 31.60 | 146.15 ± 27.19 | 0.033 |
| 50m run (sec) | 9.87 ± 1.43 | 9.62 ± 1.40 | 0.076 |
| Variables | Urban (n = 384) | Rural (n = 276) | p-Value | Post-Hoc | ||
|---|---|---|---|---|---|---|
| Pre (a) | Post (b) | Pre (c) | Post (d) | |||
| Height (cm) | 153.14 ± 9.31 | 157.66 ± 10.40 | 158.25 ± 13.70 | 159.53 ± 9.60 | <0.001 | a < b, c, d |
| Weight (kg) | 51.87 ± 15.11 | 56.94 ± 18.00 | 60.10 ± 18.18 | 59.77 ± 17.07 | <0.001 | a < b, c, d |
| BMI (kg/m2) | 21.81 ± 4.73 | 22.51 ± 5.09 | 23.48 ± 5.12 | 23.16 ± 4.92 | <0.001 | a < c, d |
| 20m shuttle run (rep) | 58.99 ± 32.46 | 62.09 ± 31.07 | 48.27 ± 27.15 | 55.87 ± 30.80 | <0.001 | c < a, b, d |
| Sit-and-reach (cm) | 3.87 ± 9.00 | 5.91 ± 7.83 | 7.44 ± 9.41 | 5.50 ± 8.19 | <0.001 | c > a, b, d |
| Grip strength (kg) | 19.78 ± 6.44 | 26.10 ± 10.26 | 26.72 ± 9.29 | 26.45 ± 9.73 | <0.001 | a < b, c, d |
| Sit-ups (rep) | 25.58 ± 16.41 | 55.19 ± 47.37 | 26.72 ± 47.37 | 51.73 ± 42.40 | <0.001 | a < b, d b > a, c |
| Long jump (cm) | 139.68 ± 49.01 | 162.33 ± 29.79 | 161.78 ± 26.74 | 158.49 ± 27.90 | <0.001 | a < b, c, d |
| 50m run (sec) | 9.69 ± 0.80 | 10.21 ± 4.91 | 10.09 ± 3.97 | 9.90 ± 3.00 | 0.962 | - |
| MPA (min/week) | 185.14 ± 226.7 | 256.80 ± 369.5 | 181.81 ± 210.52 | 252.72 ± 349.0 | 0.008 | c < d |
| VPA (min/week) | 152.22 ± 214.5 | 198.95 ± 359.8 | 141.92 ± 192.9 | 202.63 ± 320.6 | 0.001 | a < b, d b > a, c |
| MVPA (min/week) | 337.35 ± 391.9 | 455.75 ± 650.7 | 323.73 ± 355.7 | 455.35 ± 610.4 | 0.001 | a < d b > c |
| Variables | Urban (n = 264) | Rural (n = 337) | p-Value | Post-Hoc | ||
|---|---|---|---|---|---|---|
| Pre (a) | Post (b) | Pre (c) | Post (d) | |||
| Height (cm) | 152.41 ± 7.26 | 156.95 ± 7.14 | 156.13 ± 7.27 | 156.24 ± 6.75 | <0.001 | a < b, c, d |
| Weight (kg) | 49.95 ± 25.97 | 52.51 ± 13.00 | 52.57 ± 13.03 | 51.70 ± 11.77 | 0.016 | a < c |
| BMI (kg/m2) | 20.93 ± 10.69 | 21.15 ± 4.24 | 21.34 ± 4.57 | 21.07 ± 4.07 | 0.719 | - |
| 20m shuttle run (rep) | 43.97 ± 24.16 | 60.40 ± 25.61 | 36.90 ± 17.97 | 56.47 ± 24.84 | <0.001 | c < a, b, d |
| Sit-and-reach (cm) | 10.65 ± 8.49 | 13.19 ± 9.03 | 13.11 ± 9.32 | 11.33 ± 9.33 | 0.001 | a < b, c b < c |
| Grip strength (kg) | 19.68 ± 5.04 | 23.66 ± 7.02 | 24.18 ± 7.14 | 24.19 ± 7.72 | <0.001 | a < b, c, d |
| Sit-ups (rep) | 23.94 ± 13.33 | 31.82 ± 30.89 | 35.21 ± 21.38 | 32.54 ± 26.45 | 0.001 | a < c, d |
| Long jump (cm) | 133.67 ± 33.15 | 147.95 ± 27.82 | 149.68 ± 28.25 | 143.23 ± 28.37 | <0.001 | a < b, c, d |
| 50m run (sec) | 10.21 ± 1.08 | 9.99 ± 1.06 | 10.34 ± 1.38 | 9.88 ± 1.40 | <0.001 | a > b, c, d |
| MPA (min/week) | 147.34 ± 173.1 | 176.66 ± 258.6 | 143.60 ± 177.5 | 201.0 ± 325.4 | 0.019 | d > a, c |
| VPA (min/week) | 101.06 ± 151.9 | 129.93 ± 241.1 | 79.63 ± 127.3 | 106.04 ± 227.4 | 0.008 | b > c |
| MVPA (min/week) | 248.40 ± 280.9 | 305.60 ± 454.5 | 223.22 ± 259.3 | 307.03 ± 480.9 | 0.009 | d > c |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, J.-H.; Lim, S.-T. Smart App and Wearable Device-Based Approaches for Contactless Public Healthcare for Adolescents in Korea. Appl. Sci. 2025, 15, 8084. https://doi.org/10.3390/app15148084
Cho J-H, Lim S-T. Smart App and Wearable Device-Based Approaches for Contactless Public Healthcare for Adolescents in Korea. Applied Sciences. 2025; 15(14):8084. https://doi.org/10.3390/app15148084
Chicago/Turabian StyleCho, Ji-Hoon, and Seung-Taek Lim. 2025. "Smart App and Wearable Device-Based Approaches for Contactless Public Healthcare for Adolescents in Korea" Applied Sciences 15, no. 14: 8084. https://doi.org/10.3390/app15148084
APA StyleCho, J.-H., & Lim, S.-T. (2025). Smart App and Wearable Device-Based Approaches for Contactless Public Healthcare for Adolescents in Korea. Applied Sciences, 15(14), 8084. https://doi.org/10.3390/app15148084