
Depressive Symptoms and Cognitive Impairment in Older Users of Community Home Care Services in Low-Resource Settings: A Real-World Clinical Study [Geo-CoDe Study]

 ,
,  , ,
, ,  ,
,  ,
,  on behalf of the Geo-CoDe Study Group
on behalf of the Geo-CoDe Study Group
Abstract
1. Introduction
1.1. Background
1.2. Study Aims
2. Materials and Methods
2.1. Participants
2.2. Setting
2.3. Training of Healthcare Professionals of Municipal Home Care Services
2.4. Sociodemographic and Somatic Clinical Data Collection
2.5. Procedures for Detecting Depressive Symptoms and Cognitive Deficits
- The short version of the Geriatric Depression Scale (GDS-15);
- The Mini Mental State Examination (MMSE);
- The Clock Drawing Test (CDT).
2.6. Data Collection Regarding Further Neuropsychiatric Evaluation
2.7. Statistical Analysis
3. Results
3.1. Sociodemographic and Clinical Characteristics
3.2. Cognitive Performance and Depressive Symptoms
3.3. Seeking Further Neuropsychiatric Diagnostic Workup
4. Discussion
4.1. Frequency and Co-Existence of Depressive Symptoms and Cognitive Impairment in Users of Municipal Home Care Services
4.2. Underdiagnosis of Depression and Cognitive Decline in Users of Municipal Home Care Services
4.3. Factors Influencing the Decision on Seeking Further Neuropsychiatric Diagnostic Workup
5. Limitations
6. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Overend, K.; Bosanquet, K.; Bailey, D.; Foster, D.; Gascoyne, S.; Lewis, H.; Nutbrown, S.; Woodhouse, R.; Gilbody, S.; Chew-Graham, C. Revealing hidden depression in older people: A qualitative study within a randomised controlled trial. BMC Family Practice 2015, 16, 142. [Google Scholar] [CrossRef] [PubMed]
- Panagiotopoulos, G.; Kaliampakos, D. Accessibility and Spatial Inequalities in Greece. Appl. Spat. Anal. Policy 2019, 12, 567–586. [Google Scholar] [CrossRef]
- Rahman, M.; White, E.M.; Mills, C.; Thomas, K.S.; Jutkowitz, E. Rural-urban differences in diagnostic incidence and prevalence of Alzheimer’s disease and related dementias. Alzheimer’s Dement. 2021, 17, 1213–1230. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Demnitz, N.; Yamamoto, S.; Yaffe, K.; Lawlor, B.; Leroi, I. Defining brain health: A concept analysis. Int. J. Geriatr. Psychiatry 2022, 37, gps.5564. [Google Scholar] [CrossRef]
- Eyre, H.A.; Stirland, L.E.; Jeste, D.V.; Reynolds, C.F.; Berk, M.; Ibanez, A.; Dawson, W.D.; Lawlor, B.; Leroi, I.; Yaffe, K.; et al. Life-Course Brain Health as a Determinant of Late-Life Mental Health: American Association for Geriatric Psychiatry Expert Panel Recommendations. Am. J. Geriatr. Psychiatry 2023, 31, 1017–1031. [Google Scholar] [CrossRef] [PubMed]
- Zenebe, Y.; Akele, B.; Selassie, M.; Necho, M. Prevalence and determinants of depression among old age: A systematic review and meta-analysis. Ann. Gen. Psychiatry 2021, 20, 55. [Google Scholar] [CrossRef]
- Denslow, S.; Wingert, J.R.; Hanchate, A.D.; Rote, A.; Westreich, D.; Sexton, L.; Cheng, K.; Curtis, J.; Jones, W.S.; Lanou, A.J.; et al. Rural-urban outcome differences associated with COVID-19 hospitalizations in North Carolina. PLoS ONE 2022, 17, e0271755. [Google Scholar] [CrossRef]
- Saha, A.; Mandal, B.; Muhammad, T.; Ali, W. Decomposing the rural–urban differences in depression among multimorbid older patients in India: Evidence from a cross-sectional study. BMC Psychiatry 2024, 24, 60. [Google Scholar] [CrossRef]
- Griffiths, K.M.; Christensen, H.; Jorm, A.F. Mental health literacy as a function of remoteness of residence: An Australian national study. BMC Public Health 2019, 9, 92. [Google Scholar] [CrossRef]
- Kumar, S.; Chauhan, S.; Patel, R.; Kumar, M.; Simon, D.J. Urban-rural and gender differential in depressive symptoms among elderly in India. Dialogues Health 2023, 2, 100114. [Google Scholar] [CrossRef]
- Politis, A.; Vorvolakos, T.; Kontogianni, E.; Alexaki, M.; Georgiou, E.-Z.; Aggeletaki, E.; Gkampra, M.; Delatola, M.; Delatolas, A.; Efkarpidis, A.; et al. Old-age mental telehealth services at primary healthcare centers in low- resource areas in Greece: Design, iterative development and single-site pilot study findings. BMC Health Serv. Res. 2023, 23, 626. [Google Scholar] [CrossRef] [PubMed]
- Stewart, H.; Jameson, J.P.; Curtin, L. The relationship between stigma and self-reported willingness to use mental health services among rural and urban older adults. Psychol. Serv. 2015, 12, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Bucciardini, R.; Zetterquist, P.; Rotko, T.; Putatti, V.; Mattioli, B.; De Castro, P.; Napolitani, F.; Giammarioli, A.M.; Kumar, B.N.; Nordström, C.; et al. Addressing health inequalities in Europe: Key messages from the Joint Action Health Equity Europe (JAHEE). Arch. Public Health 2023, 81, 89. [Google Scholar] [CrossRef] [PubMed]
- Panagiotopoulos, G.; Kaliampakos, D. Location quotient-based travel costs for determining accessibility changes. J. Transp. Geogr. 2021, 91, 102951. [Google Scholar] [CrossRef]
- Fountoulakis, K.N.; Tsolaki, M.; Iacovides, A.; Yesavage, J.; O’Hara, R.; Kazis, A.; Ierodiakonou, C. The validation of the short form of the Geriatric Depression Scale (GDS) in Greece. Aging Clin. Exp. Res. 1999, 11, 367–372. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Bird, V.; Rizzo, M.; Meader, N. Diagnostic validity and added value of the Geriatric Depression Scale for depression in primary care: A meta-analysis of GDS30 and GDS15. J. Affect. Disord. 2010, 125, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. Mini-mental state. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Chun, C.T.; Seward, K.; Patterson, A.; Melton, A.; MacDonald-Wicks, L. Evaluation of Available Cognitive Tools Used to Measure Mild Cognitive Decline: A Scoping Review. Nutrients 2021, 13, 3974. [Google Scholar] [CrossRef] [PubMed]
- Kvitting, A.S.; Fällman, K.; Wressle, E.; Marcusson, J. Age-Normative MMSE Data for Older Persons Aged 85 to 93 in a Longitudinal Swedish Cohort. J. Am. Geriatr. Soc. 2019, 67, 534–538. [Google Scholar] [CrossRef]
- Salis, F.; Costaggiu, D.; Mandas, A. Mini-Mental State Examination: Optimal Cut-Off Levels for Mild and Severe Cognitive Impairment. Geriatrics 2023, 8, 12. [Google Scholar] [CrossRef]
- Aprahamian, I.; Martinelli, J.E.; Neri, A.L.; Yassuda, M.S. The Clock Drawing Test: A review of its accuracy in screening for dementia. Dement. Neuropsychol. 2009, 3, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Jahng, S.; Yu, K.-H.; Lee, B.-C.; Kang, Y. Usefulness of the Clock Drawing Test as a Cognitive Screening Instrument for Mild Cognitive Impairment and Mild Dementia: An Evaluation Using Three Scoring Systems. Dement. Neurocognitive Disord. 2018, 17, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Çorbacıoğlu, Ş.K.; Aksel, G. Receiver operating characteristic curve analysis in diagnostic accuracy studies: A guide to interpreting the area under the curve value. Turk. J. Emerg. Med. 2023, 23, 195–198. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.-T. Introduction to Geographic Information Systems, 9th ed.; McGraw-Hill Education: New York, NY, USA, 2019. [Google Scholar]
- Hodson, T.O.; DeCicco, L.A.; Hariharan, J.A.; Stanish, L.F.; Black, S.; Horsburgh, J.S. Reproducibility Starts at the Source: R, Python, and Julia Packages for Retrieving USGS Hydrologic Data. Water 2023, 15, 4236. [Google Scholar] [CrossRef]
- Hauke, J.; Kossowski, T. Comparison of Values of Pearson’s and Spearman’s Correlation Coefficients on the Same Sets of Data. QUAGEO 2011, 30, 87–93. [Google Scholar] [CrossRef]
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation Coefficients: Appropriate Use and Interpretation. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef]
- Banerjee, A.; Duflo, E.; Grela, E.; McKelway, M.; Schilbach, F.; Sharma, G.; Vaidyanathan, G. Depression and Loneliness Among the Elderly Poor; National Bureau of Economic Research: Cambridge, MA, USA, 2022. [Google Scholar] [CrossRef]
- Evangelopoulou, E.; Alimani, G.; Apotsos, P.; Simou, G.; Kiritsi, E.; Mathioudakis, A.G.; Mathioudakis, G.A. An epidemiological study of multimorbidity in Greece. Arch. Hell. Med. 2019, 36, 754. [Google Scholar]
- Agustini, B.; Lotfaliany, M.; Woods, R.L.; McNeil, J.J.; Nelson, M.R.; Shah, R.C.; Murray, A.M.; Ernst, M.E.; Reid, C.M.; Tonkin, A.; et al. Patterns of Association between Depressive Symptoms and Chronic Medical Morbidities in Older Adults. J. Am. Geriatr. Soc. 2020, 68, 1834–1841. [Google Scholar] [CrossRef]
- Zijlmans, J.L.; Vernooij, M.W.; Ikram, M.A.; Luik, A.I. The role of cognitive and brain reserve in late-life depressive events: The Rotterdam Study. J. Affect. Disord. 2023, 320, 211–217. [Google Scholar] [CrossRef]
- Gamble, L.D.; Clare, L.; Opdebeeck, C.; Martyr, A.; Jones, R.W.; Rusted, J.M.; Pentecost, C.; Thom, J.M.; Matthews, F.E. Cognitive reserve and its impact on cognitive and functional abilities, physical activity and quality of life following a diagnosis of dementia: Longitudinal findings from the Improving the experience of Dementia and Enhancing Active Life (IDEAL) study. Age Ageing 2025, 54, afae284. [Google Scholar] [CrossRef]
- Alexopoulos, P.; Leroi, I.; Kinchin, I.; Canty, A.J.; Dasgupta, J.; Furlano, J.A.; Haas, A.N. Relevance and Premises of Values-Based Practice for Decision Making in Brain Health. Brain Sci. 2024, 14, 718. [Google Scholar] [CrossRef] [PubMed]
- Luchetti, M.; Aschwanden, D.; Sesker, A.A.; Zhu, X.; O’Súilleabháin, P.S.; Stephan, Y.; Terracciano, A.; Sutin, A.R. A meta-analysis of loneliness and risk of dementia using longitudinal data from >600,000 individuals. Nat. Ment. Health 2024, 2, 1350–1361. [Google Scholar] [CrossRef] [PubMed]
- Raichlen, D.A.; Aslan, D.H.; Sayre, M.K.; Bharadwaj, P.K.; Ally, M.; Maltagliati, S.; Lai, M.H.C.; Wilcox, R.R.; Klimentidis, Y.C.; Alexander, G.E. Sedentary Behavior and Incident Dementia Among Older Adults. JAMA 2023, 330, 934. [Google Scholar] [CrossRef]
- Dafsari, F.S.; Jessen, F. Depression—An underrecognized target for prevention of dementia in Alzheimer’s disease. Transl. Psychiatry 2020, 10, 160. [Google Scholar] [CrossRef] [PubMed]
- Coelho, E. Eurostat Database. In Encyclopedia of Quality of Life and Well-Being Research; Maggino, F., Ed.; Springer International Publishing: Cham, Switzerland, 2023; pp. 2255–2257. [Google Scholar] [CrossRef]
- Aliberti, M.J.R.; Suemoto, C.K. Empowering older adults and their communities to cope with depression in resource-limited settings. Lancet Healthy Longev. 2022, 3, e643–e644. [Google Scholar] [CrossRef] [PubMed]
- Xu, D.; Samu, G.C.; Chen, J. Advancing mental health service delivery in low-resource settings. Lancet Glob. Health 2024, 12, e543–e545. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.; Wang, Q.; Zhang, J.; Wang, Q.; Hou, F.; Han, X.; Hu, S.; Shen, G.; Zhang, Y. Depressive Symptoms and Cognitive Decline Among Chinese Rural Elderly Individuals: A Longitudinal Study With 2-Year Follow-Up. Front. Public Health 2022, 10, 939150. [Google Scholar] [CrossRef]
- Bocker, E.; Glasser, M.; Nielsen, K.; Weidenbacher-Hoper, V. Rural older adults’ mental health: Status and challenges in care delivery. Rural. Remote Health 2012, 12, 1–13. [Google Scholar] [CrossRef]
- Devita, M.; De Salvo, R.; Ravelli, A.; De Rui, M.; Coin, A.; Sergi, G.; Mapelli, D. Recognizing Depression in the Elderly: Practical Guidance and Challenges for Clinical Management. Neuropsychiatr. Dis. Treat. 2022, 18, 2867–2880. [Google Scholar] [CrossRef]
- Pacifico, D.; Fiordelli, M.; Fadda, M.; Serena, S.; Piumatti, G.; Carlevaro, F.; Magno, F.; Franscella, G.; Albanese, E. Dementia is (not) a natural part of ageing: A cross-sectional study on dementia knowledge and misconceptions in Swiss and Italian young adults, adults, and older adults. BMC Public Health 2022, 22, 2176. [Google Scholar] [CrossRef]
- CHP 2 Depression Group; Shajan, A.M.; Guttikonda, A.; Hephzibah, A.; Jones, A.S.; Susanna, J.; Neethu, S.; Poornima, S.; Jala, S.M.; Arputharaj, D.; et al. Perceived Stigma Regarding Mental Illnesses among Rural Adults in Vellore, Tamil Nadu, South India. Indian J. Psychol. Med. 2019, 41, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Pujolar, G.; Oliver-Anglès, A.; Vargas, I.; Vázquez, M.L. Changes in Access to Health Services during the COVID-19 Pandemic: A Scoping Review. Int. J. Env. Res. Public Health 2022, 19, 1749. [Google Scholar] [CrossRef]
- Mseke, E.P.; Jessup, B.; Barnett, T. Impact of distance and/or travel time on healthcare service access in rural and remote areas: A scoping review. J. Transp. Health 2024, 37, 101819. [Google Scholar] [CrossRef]
- Parsons, M.; Qiu, L.; Levis, B.; Fan, S.; Sun, Y.; Amiri, L.S.N.; Harel, D.; Markham, S.; Vigod, S.N.; Ziegelstein, R.C.; et al. Depression prevalence of the Geriatric Depression Scale-15 was compared to Structured Clinical Interview for DSM using individual participant data meta-analysis. Scientific Reports 2024, 14, 17430. [Google Scholar] [CrossRef] [PubMed]
- Alexopoulos, P.; Novotni, A.; Novotni, G.; Vorvolakos, T.; Vratsista, A.; Konsta, A.; Kaprinis, S.; Konstantinou, A.; Bonotis, K.; Katirtzoglou, E.; et al. Old age mental health services in Southern Balkans: Features, geospatial distribution, current needs, and future perspectives. Eur. Psychiatry 2020, 63, e88. [Google Scholar] [CrossRef] [PubMed]
- Aggeletaki, E.; Stamos, V.; Konidari, E.; Efkarpidis, A.; Petrou, A.; Savvopoulou, K.; Kontogianni, E.; Tsimpanis, K.; Vorvolakos, T.; Politis, A.; et al. Telehealth memory clinics in primary healthcare: Real-world experiences from low-resource settings in Greece. Front. Dement. 2024, 3, 1477242. [Google Scholar] [CrossRef]
- Allana, A.; Kuluski, K.; Tavares, W.; Pinto, A.D. Building integrated, adaptive and responsive healthcare systems—Lessons from paramedicine in Ontario, Canada. BMC Health Serv. Res. 2022, 22, 595. [Google Scholar] [CrossRef]
- Steenkamer, B.; Drewes, H.; Putters, K.; Van Oers, H.; Baan, C. Reorganizing and integrating public health, health care, social care and wider public services: A theory-based framework for collaborative adaptive health networks to achieve the triple aim. J. Health Serv. Res. Policy 2020, 25, 187–201. [Google Scholar] [CrossRef] [PubMed]
- Thiam, Y.; Allaire, J.-F.; Morin, P.; Hyppolite, S.-R.; Doré, C.; Zomahoun, H.T.V.; Garon, S. A Conceptual Framework for Integrated Community Care. Int. J. Integr. Care 2021, 21, 5. [Google Scholar] [CrossRef]
- Elkind, M.S.V.; Albert, M.A.; Lloyd-Jones, D.M. Road to Equity in Brain Health. Circulation 2022, 145, e869–e871. [Google Scholar] [CrossRef]
- Steele Gray, C.; Grudniewicz, A.; Armas, A.; Mold, J.; Im, J.; Boeckxstaens, P. Goal-Oriented Care: A Catalyst for Person-Centred System Integration. Int. J. Integr. Care 2020, 20, 8. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Sample Characteristics | |
| N | 406 |
| Age, years * | 81.03 (7.71) [58.0–97.0] |
| Education, years * | 4.00 (3.30) [0.0–22.0] |
| Marital status [N = 402] N (%) | Single: 22 (0.056) Married: 138 (0.339) Widow: 219 (0.538) Divorced: 12 (0.029) |
| Occupation [N = 332] N (%) | Unemployed: 60 (0.181) Farmer: 191 (0.575) Office employee: 35 (0.105) Workers: 8 (0.024) Other: 38 (0.114) |
| Neurological disorders diagnosed prior to enrollment (N) [%] | 42 [10.76] |
| Psychiatric disorders diagnosed prior to enrollment (N) [%] | 40 [10.25] |
| Test results—N = 406 | |
| Cognitive performance calculated as % of the highest score the examinee could receive based on all items that were administered on Mini Mental State Examination * [N = 406] | 78.11 (15.55) [20.0–100.0] |
| Clock Drawing Test score * [N = 402] | 1.77 (1.07) [0.0–3.0] |
| Geriatric Depression Scale-15 score * [N = 405] | 5.38 (3.67) [0.0–15.0] |
| Somatic diseases—N = 335 | |
| Sum of comorbidities * | 3.71 (1.59) [0.0–8.0] |
| Medication Number * | 6.11 (2.70) [0.0–16.0] |
| Hypertension (%) | 84 |
| Dyslipidemia (%) | 52.5 |
| Coronary artery disease (%) | 5.2 |
| Heart failure (%) | 25.9 |
| Atrial fibrillation/arrhythmia (%) | 17.3 |
| Diabetes mellitus (%) | 26.5 |
| Stroke (%) | 6.5 |
| Chronic obstructive pulmonary disease, asthma (%) | 13.9 |
| Thyroidopathy (%) | 10.2 |
| Other endocrinological conditions (e.g., osteoporosis) (%) | 26.9 |
| Rheumatological conditions (%) | 14.8 |
| Hematological diseases (%) | 11.1 |
| Neurological disorders (%) | 11.7 |
| Gastrointestinal diseases (%) | 29.6 |
| Urological/nephrological diseases (%) | 17.9 |
| Chronic pain syndrome (%) | 13.3 |
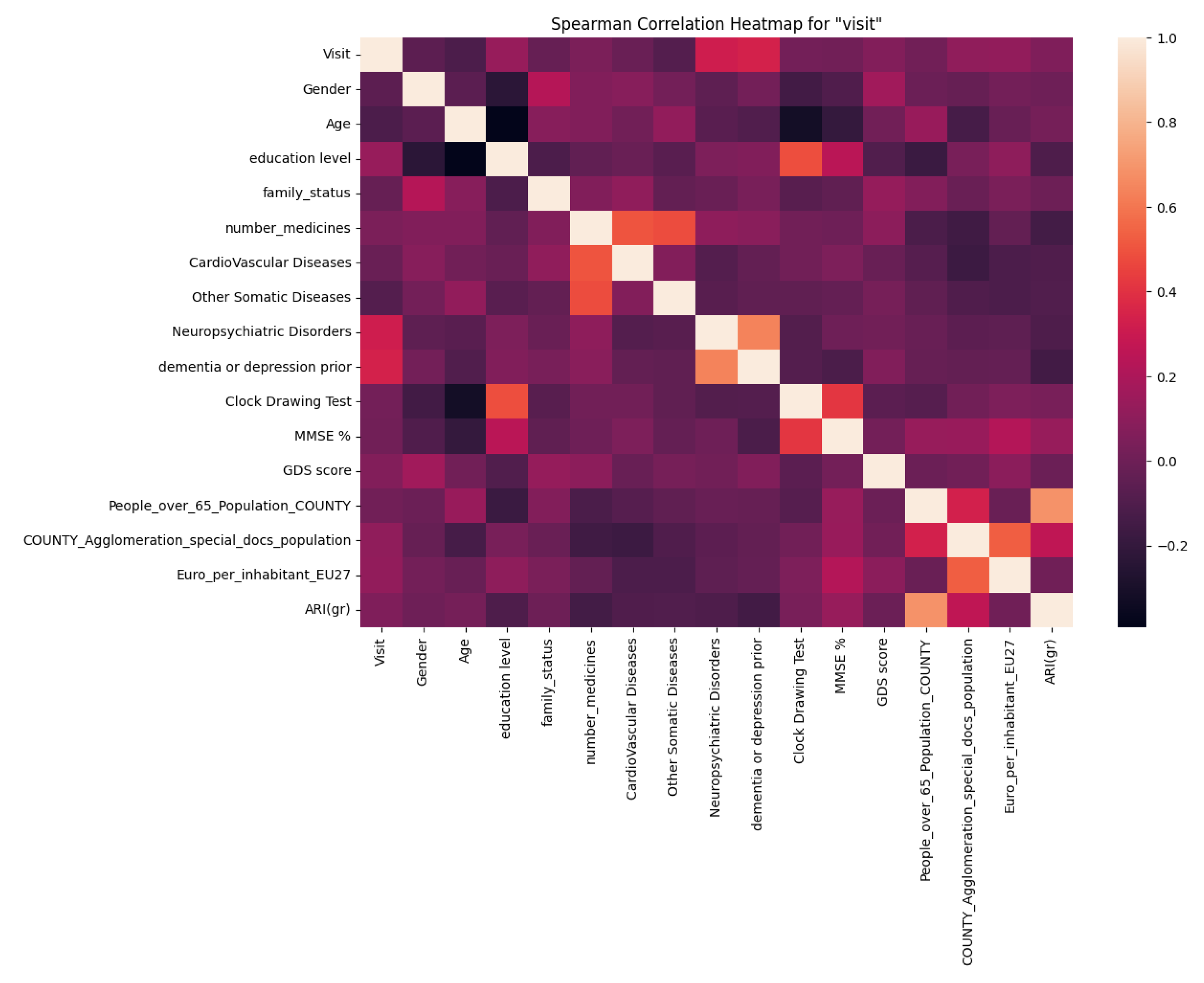
| Parameter | Spearman Rank-Order Correlation Coefficient | p-Value | N |
|---|---|---|---|
| Visit | 1 | 0 | 335 |
| Sex | −0.06 | 0.23 | 335 |
| Age | −0.11 | 0.04 | 333 |
| Education level | 0.13 | 0.03 | 316 |
| Family status | −0.02 | 0.66 | 329 |
| Total number of medicines | 0.05 | 0.32 | 334 |
| Cardiovascular diseases | −0.02 | 0.77 | 335 |
| Other somatic diseases | −0.08 | 0.13 | 334 |
| Neuropsychiatric disorders | 0.32 | <0.001 | 335 |
| Dementia or depression diagnosed prior enrollment in the study | 0.34 | <0.001 | 335 |
| Clock Drawing Test score | 0.01 | 0.91 | 280 |
| Mini Mental State Examination (MMSE) score | 0.01 | 0.85 | 310 |
| Geriatric depression scale score | 0.08 | 0.18 | 311 |
| Total number of neurologists and psychiatrists in the county of residence of home care service user | 0.01 | 0.81 | 334 |
| COUNTY_Agglomeration_special_docs_population | 0.12 | 0.05 | 335 |
| Population of people aged 65 or over | 0.11 | 0.08 | 335 |
| Accessibility/remoteness index for Greece (ARI(gr)) | 0.05 | 0.32 | 335 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Georgiou, E.-Z.; Thomopoulos, V.; Prapiadou, S.; Brouma, M.; Skondra, M.; Panagiotopoulos, G.; Premtou, K.; Karydas, G.; Markopoulou, G.; Theodoropoulou, A.; et al. Depressive Symptoms and Cognitive Impairment in Older Users of Community Home Care Services in Low-Resource Settings: A Real-World Clinical Study [Geo-CoDe Study]. Appl. Sci. 2025, 15, 6426. https://doi.org/10.3390/app15126426
Georgiou E-Z, Thomopoulos V, Prapiadou S, Brouma M, Skondra M, Panagiotopoulos G, Premtou K, Karydas G, Markopoulou G, Theodoropoulou A, et al. Depressive Symptoms and Cognitive Impairment in Older Users of Community Home Care Services in Low-Resource Settings: A Real-World Clinical Study [Geo-CoDe Study]. Applied Sciences. 2025; 15(12):6426. https://doi.org/10.3390/app15126426
Chicago/Turabian StyleGeorgiou, Eleni-Zacharoula (Eliza), Vasileios Thomopoulos, Savvina Prapiadou, Maria Brouma, Maria Skondra, George Panagiotopoulos, Kyriaki Premtou, Georgios Karydas, Georgia Markopoulou, Afroditi Theodoropoulou, and et al. 2025. "Depressive Symptoms and Cognitive Impairment in Older Users of Community Home Care Services in Low-Resource Settings: A Real-World Clinical Study [Geo-CoDe Study]" Applied Sciences 15, no. 12: 6426. https://doi.org/10.3390/app15126426
APA StyleGeorgiou, E.-Z., Thomopoulos, V., Prapiadou, S., Brouma, M., Skondra, M., Panagiotopoulos, G., Premtou, K., Karydas, G., Markopoulou, G., Theodoropoulou, A., Macha, P., Tatsi, P., Kaliampakos, D., Vantarakis, A., Tsichlas, K., & Alexopoulos, P., on behalf of the Geo-CoDe Study Group. (2025). Depressive Symptoms and Cognitive Impairment in Older Users of Community Home Care Services in Low-Resource Settings: A Real-World Clinical Study [Geo-CoDe Study]. Applied Sciences, 15(12), 6426. https://doi.org/10.3390/app15126426