
Altered Visual Attention at 12 Months Predicts Joint Attention Ability and Socio-Communicative Development at 24 Months: A Single-Center Eye-Tracking Study on Infants at Elevated Likelihood to Develop Autism

 ,
,  ,
,
Abstract
1. Introduction
2. Methods
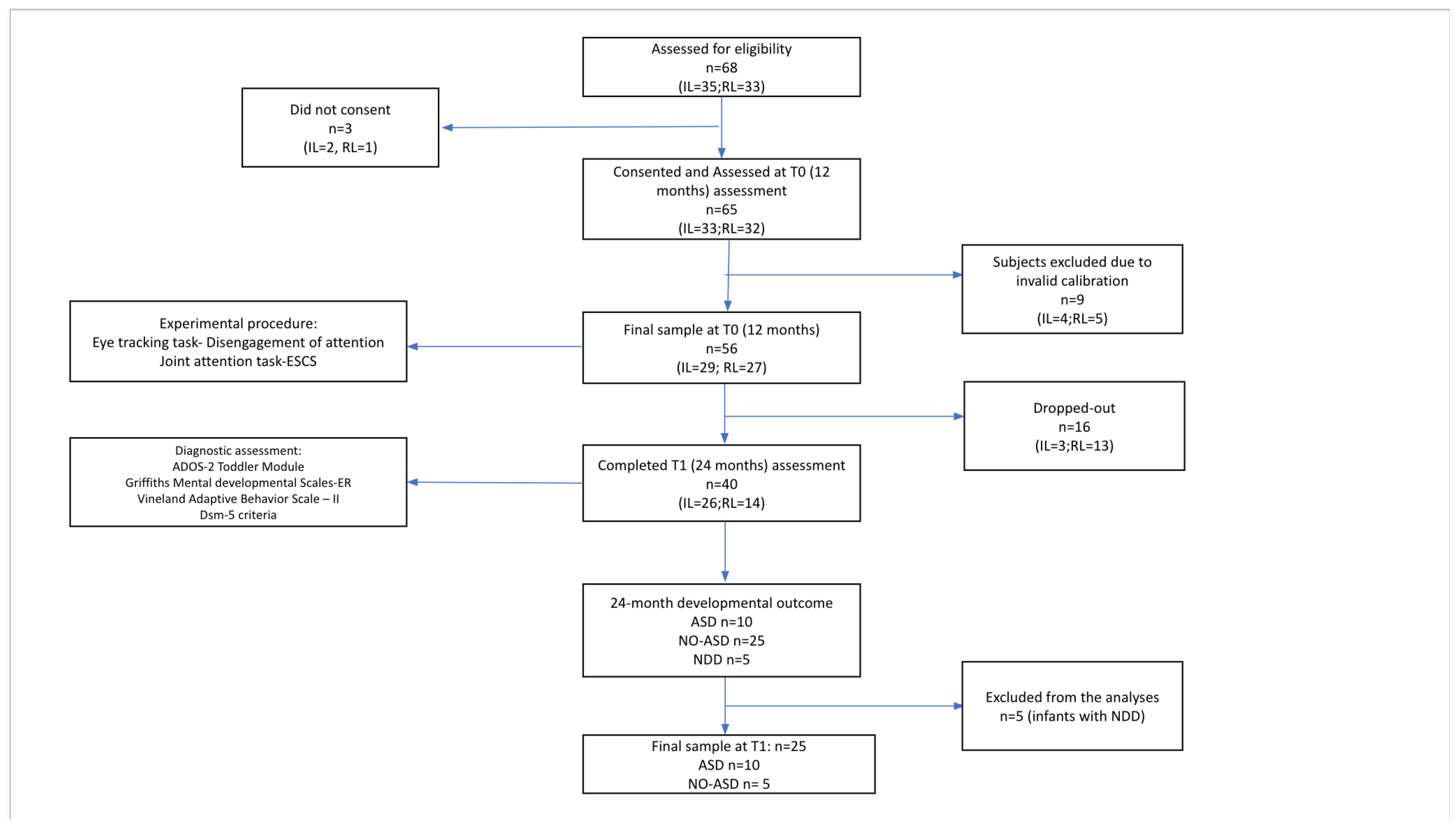
2.1. Participants
2.2. Procedure
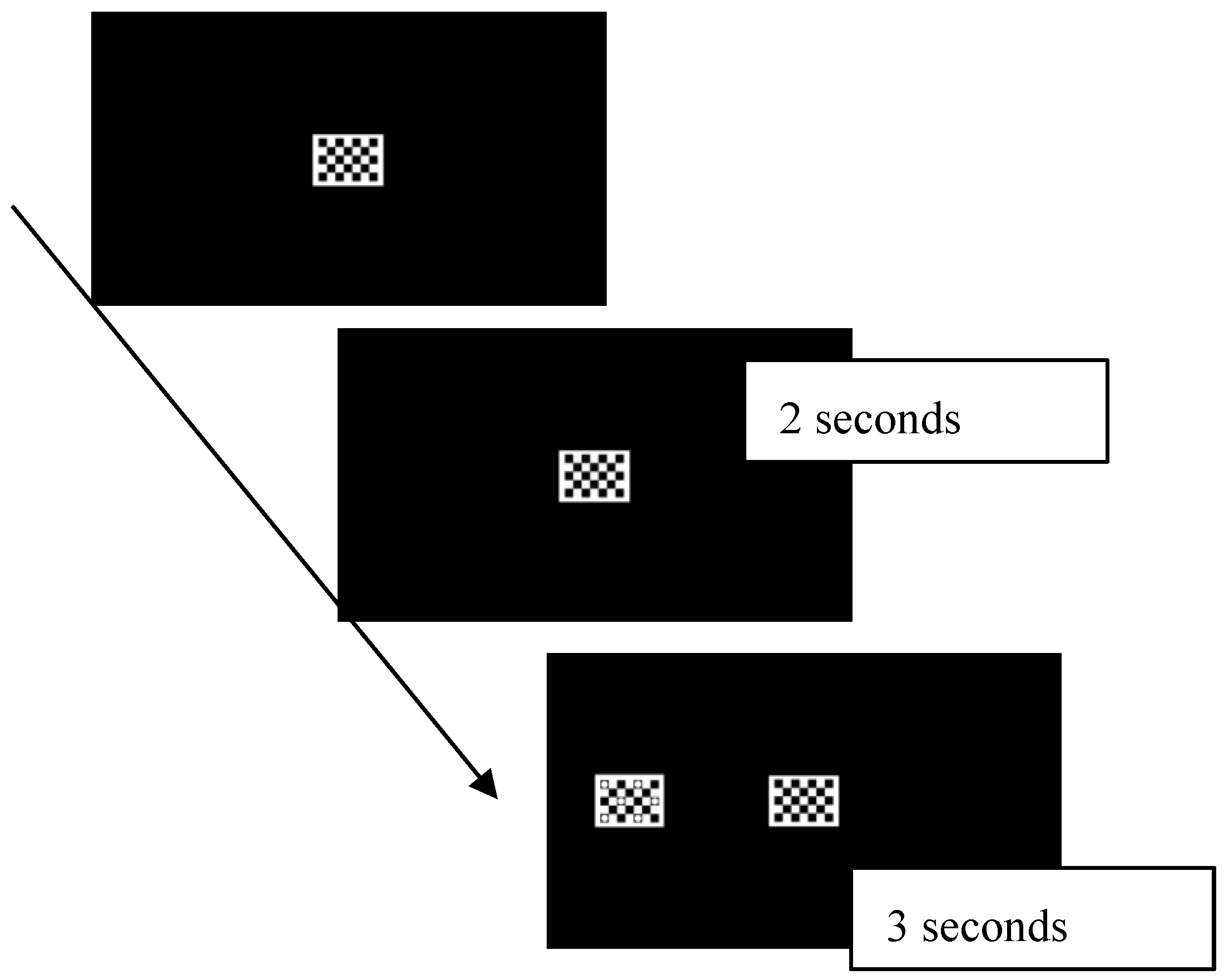
2.3. Attention Disengagement
2.4. Joint Attention
- Object Spectacle Task: In this task, the examiner activates mechanical toys, and the child’s response to the activation of a toy is assessed (a total of 4 trials).
- Book Presentation Task: In this task, the examiner presents images to the child (a total of 6 images), evaluating the child’s ability to follow proximal pointing and any initiation of joint attention or requesting behaviors.
- Gaze-Following Task: This task assesses the child’s ability to follow distal pointing and shift their gaze toward a distant object (a total of 5 trials).
3. Statistical Analyses
4. Results
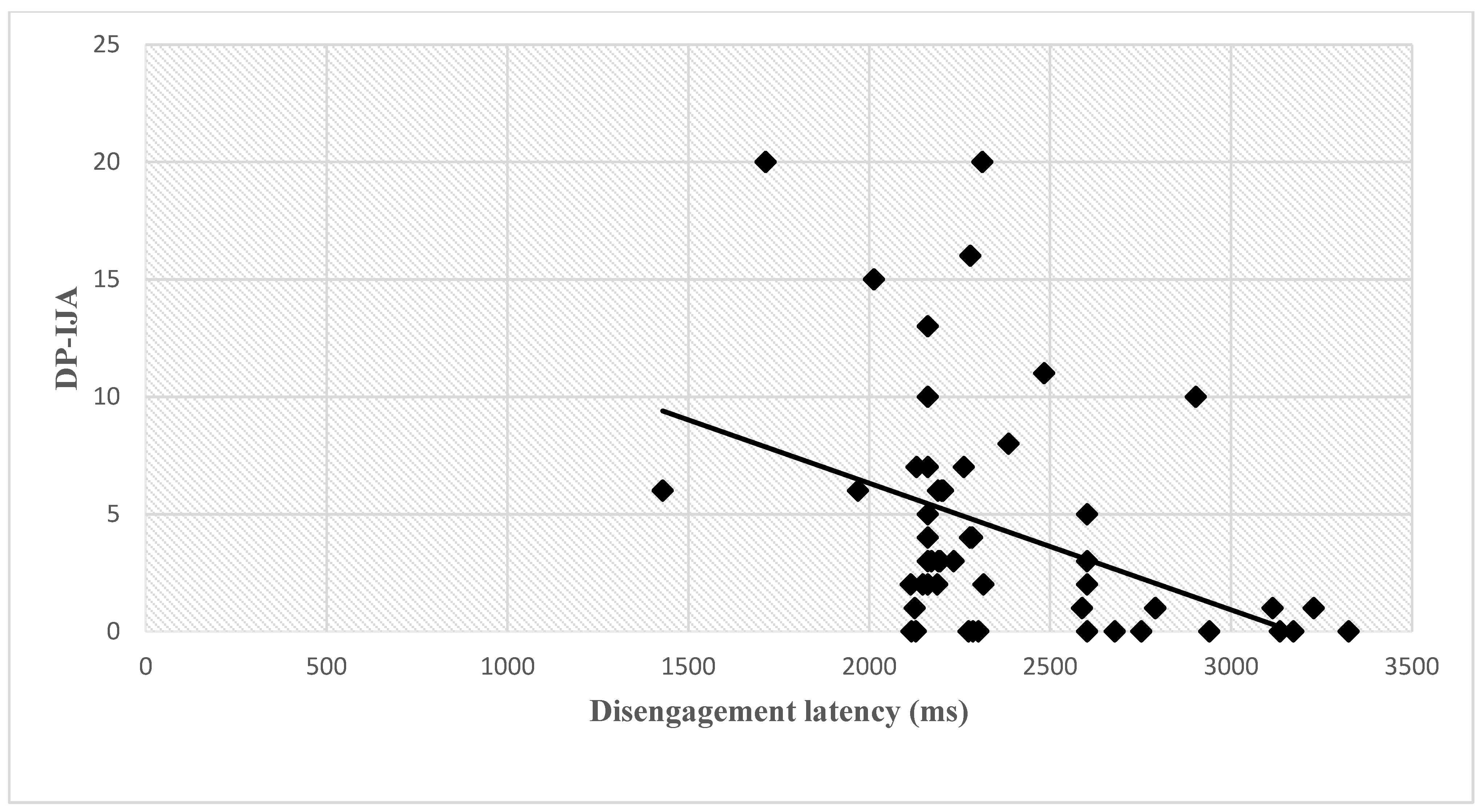
4.1. Correlation Between Disengagement Latency and Joint Attention Behaviors at 12 Months
4.2. T0 Predictors of Outcome at T1 (Table 1)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 12-Month Predictors | ASD and NO-ASD | ADOS-2 JA (Item b13) | ADOS-2 SA | ADOS-2 RRB | ADOS-2 Total | GMDS-ER DQ |
|---|---|---|---|---|---|---|
| Disengagement latency (ms) | p = 0.015 * B = 1.003 | F = 5.037 β = 0.397 p = 0.033 * | F = 4.187 β = 0.345 p = 0.049 * | ns | F = 4.237, β = 0.347 p = 0.048 * | F = 5.870 β = −0.399 p = 0.021 * |
| AG-IJA | p = 0.019 * B = −0.746 | ns | ns | ns | ns | F = 5.525, β = 0.394, p = 0.026 |
5. Discussion
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Variables | IL (n = 29) | RL (n = 27) | ||
|---|---|---|---|---|
| Mean | Sd | Mean | Sd | |
| Disengagement latency (ms) | 2554.64 | 302.7 | 2157.45 | 147.8 |
| AG-IJA | 10.12 | 4.81 | 19 | 7.86 |
| DP-IJA | 3.25 | 5.15 | 6.71 | 6.03 |
| FPP-RJA | 3.96 | 2.56 | 6.21 | 1.31 |
| FDP-RJA | 1.83 | 1.4 | 3.57 | 0.75 |
| Variables | ASD (n = 10) | NO-ASD (n = 25) | ||
|---|---|---|---|---|
| Mean | Sd | Mean | Sd | |
| SA—Ados-2 Toddler Module | 11.70 | 3.77 | 3.65 | 2.98 |
| RRB—Ados-2 Toddler Module | 4.20 | 1.93 | 1.91 | 1.81 |
| Total ADOS-2 score | 15.90 | 4.77 | 5.57 | 4.05 |
| DQ-GMDS-ER | 89.17 | 17.22 | 105.95 | 11.86 |
References
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5-TR®; American Psychiatric Association: Washington, DC, USA, 2022. [Google Scholar]
- Frazier, T.W.; Klingemier, E.W.; Anderson, C.J.; Gengoux, G.W.; Youngstrom, E.A.; Hardan, A.Y. A longitudinal study of language trajectories and treatment outcomes of early intensive behavioral intervention for autism. J. Autism Dev. Disord. 2021, 51, 4534–4550. [Google Scholar] [CrossRef] [PubMed]
- Sandbank, M.; Bottema-Beutel, K.; Crowley, S.; Cassidy, M.; Feldman, J.I.; Canihuante, M.; Woynaroski, T. Intervention effects on language in children with autism: A Project AIM meta-analysis. J. Speech Lang. Hear. Res. 2020, 63, 1537–1560. [Google Scholar] [CrossRef] [PubMed]
- McCarty, P.; Frye, R.E. Early detection and diagnosis of autism spectrum disorder: Why is it so difficult? Semin. Pediatr. Neurol. 2020, 35, 100831. [Google Scholar] [CrossRef]
- Zwaigenbaum, L.; Bauman, M.L.; Stone, W.L.; Yirmiya, N.; Estes, A.; Hansen, R.L.; McPartland, J.C.; Natowicz, M.R.; Choueiri, R.; Fein, D. Early Identification of Autism Spectrum Disorder: Recommendations for Practice and Research. Pediatrics 2015, 136 (Suppl. S1), S10–S14. [Google Scholar] [CrossRef]
- Hiremath, C.S.; Sagar, K.J.V.; Yamini, B.K.; Girimaji, A.S.; Kumar, R.; Sravanti, S.L.; Padmanabha, H.; Vykunta Raju, K.N.; Kishore, M.T.; Jacob, P.; et al. Emerging behavioral and neuroimaging biomarkers for early and accurate characterization of autism spectrum disorders: A systematic review. Transl. Psychiatry 2021, 11, 42. [Google Scholar] [CrossRef]
- Franchini, M.; Armstrong, V.L.; Schaer, M.; Smith, I.M. Initiation of joint attention and related visual attention processes in infants with autism spectrum disorder: Literature review. Child Neuropsychol. 2019, 25, 287–317. [Google Scholar] [CrossRef] [PubMed]
- Gliga, T.; Jones, E.J.; Bedford, R.; Charman, T.; Johnson, M.H. From early markers to neuro-developmental mechanisms of autism. Dev. Rev. 2014, 34, 189–207. [Google Scholar] [CrossRef]
- Shen, M.D.; Piven, J. Brain and behavior development in autism from birth through infancy. Dialogues Clin. Neurosci. 2017, 19, 325–333. [Google Scholar] [CrossRef]
- Mundy, P.; Newell, L. Attention, joint attention, and social cognition. Curr. Dir. Psychol. Sci. 2007, 16, 269–274. [Google Scholar] [CrossRef]
- Kaale, A.; Smith, L.; Sponheim, E. A randomized controlled trial of preschool-based joint attention intervention for children with autism. J. Child Psychol. Psychiatry 2012, 53, 97–105. [Google Scholar] [CrossRef]
- Rogers, S.J.; Estes, A.; Lord, C.; Vismara, L.; Winter, J.; Fitzpatrick, A.; Guo, M.; Dawson, G. Effects of a brief Early Start Denver Model (ESDM)–based parent intervention on toddlers at risk for autism spectrum disorders: A randomized controlled trial. J. Am. Acad. Child Adolesc. Psychiatry 2012, 51, 1052–1065. [Google Scholar] [CrossRef] [PubMed]
- Shih, W.; Shire, S.; Chang, Y.C.; Kasari, C. Joint engagement is a potential mechanism leading to increased initiations of joint attention and downstream effects on language: JASPER early intervention for children with ASD. J. Child Psychol. Psychiatry 2021, 62, 1228–1235. [Google Scholar] [CrossRef] [PubMed]
- So, W.C.; Law, W.W.; Cheng, C.H.; Lee, C.; Ng, K.C.; Kwok, F.Y.; Lam, H.W.; Lam, K.Y. Comparing the effectiveness of robot-based to human-based intervention in improving joint attention in autistic children. Front. Psychiatry 2023, 14, 1114907. [Google Scholar] [CrossRef]
- Waddington, H.; Reynolds, J.E.; Macaskill, E.; Curtis, S.; Taylor, L.J.; Whitehouse, A.J. The effects of JASPER intervention for children with autism spectrum disorder: A systematic review. Autism 2021, 25, 2370–2385. [Google Scholar] [CrossRef] [PubMed]
- Dawson, G.; Webb, S.J.; Wijsman, E.; Schellenberg, G.; Estes, A.; Munson, J.; Faja, S. Neurocognitive and electrophysiological evidence of altered face processing in parents of children with autism: Implications for a model of abnormal development of social brain circuitry in autism. Dev. Psychopathol. 2005, 17, 679–697. [Google Scholar] [CrossRef]
- Falck-Ytter, T.; Kleberg, J.L.; Portugal, A.M.; Thorup, E. Social Attention: Developmental Foundations and Relevance for Autism Spectrum Disorder. Biol. Psychiatry 2023, 94, 8–17. [Google Scholar] [CrossRef]
- Palomo, R.; Ozonoff, S.; Young, G.S.; Belinchon Carmona, M. Social orienting and initiated joint attention behaviors in 9 to 12 month old children with autism spectrum disorder: A family home movies study. Autism Res. 2022, 15, 1109–1119. [Google Scholar] [CrossRef]
- Elsabbagh, M.; Johnson, M.H. Autism and the social brain: The first-year puzzle. Biol. Psychiatry 2016, 80, 94–99. [Google Scholar] [CrossRef]
- Clohessy, A.B.; Posner, M.I.; Rothbart, M.K. Development of the functional visual field. Acta Psychol. 2001, 106, 51–68. [Google Scholar] [CrossRef]
- Mundy, P.; Card, J.; Fox, N. EEG correlates of the development of infant joint attention skills. Dev. Psychobiol. 2000, 36, 325–338. [Google Scholar] [CrossRef]
- Kulke, L.; Atkinson, J.; Braddick, O. Automatic detection of attention shifts in infancy: Eye tracking in the fixation shift paradigm. PLoS ONE 2015, 10, e0142505. [Google Scholar] [CrossRef]
- Sacrey, L.A.R.; Armstrong, V.L.; Bryson, S.E.; Zwaigenbaum, L. Impairments to visual disengagement in autism spectrum disorder: A review of experimental studies from infancy to adulthood. Neurosci. Biobehav. Rev. 2014, 47, 559–577. [Google Scholar] [CrossRef] [PubMed]
- Keehn, B.; Kadlaskar, G.; Bergmann, S.; McNally Keehn, R.; Francis, A. Attentional disengagement and the locus coeruleus–norepinephrine system in children with autism spectrum disorder. Front. Integr. Neurosci. 2021, 15, 716447. [Google Scholar] [CrossRef]
- Odriozola, P.; Uddin, L.Q.; Lynch, C.J.; Kochalka, J.; Chen, T.; Menon, V. Insula response and connectivity during social and non-social attention in children with autism. Soc. Cogn. Affect. Neurosci. 2016, 11, 433–444. [Google Scholar] [CrossRef]
- Billeci, L.; Narzisi, A.; Campatelli, G.; Crifaci, G.; Calderoni, S.; Gagliano, A.; Calzone, C.; Colombi, C.; Pioggia, G.; Muratori, F.; et al. Disentangling the initiation from the response in joint attention: An eye-tracking study in toddlers with autism spectrum disorders. Transl. Psychiatry 2016, 6, e808. [Google Scholar] [CrossRef] [PubMed]
- Muratori, F.; Billeci, L.; Calderoni, S.; Boncoddo, M.; Lattarulo, C.; Costanzo, V.; Turi, M.; Colombi, C.; Narzisi, A. How Attention to Faces and Objects Changes Over Time in Toddlers with Autism Spectrum Disorders: Preliminary Evidence from An Eye Tracking Study. Brain Sci. 2019, 9, 344. [Google Scholar] [CrossRef] [PubMed]
- Jones, W.; Klaiman, C.; Richardson, S.; Aoki, C.; Smith, C.; Minjarez, M.; Bernier, R.; Pedapati, E.; Bishop, S.; Ence, W.; et al. Eye-Tracking-Based measurement of Social Visual Engagement compared with Expert Clinical Diagnosis of Autism. J. Am. Med. Assoc. 2023, 330, 854–865. [Google Scholar] [CrossRef]
- Ozdemir, S.; Akin-Bulbul, I.; Yildiz, E. Visual Attention in Joint Attention Bids: A Comparison Between Toddlers with Autism Spectrum Disorder and Typically Developing Toddlers. J. Autism Develompental Disord. 2024, 55, 408–427. [Google Scholar] [CrossRef]
- Vernetti, A.; Butler, M.; Banarjee, C.; Boxberger, A.; All, K.; Macari, S.; Chawarska, K. Face-to-face live eye-tracking in toddlers with autism: Feasibility and impact of familiarity and face covering. Autism Res. 2023, 17, 1381–1390. [Google Scholar] [CrossRef]
- Shic, F.; Naples, A.J.; Barney, E.C.; Chang, S.A.; Li, B.; McAllister, T.; Kim, M.; Dommer, K.J.; Hasselmo, S.; Atyabi, A.; et al. The autism biomarkers consortium for clinical trials: Evaluation of a battery of candidate eye-tracking biomarkers for use in autism clinical trials. Mol. Autism 2022, 13, 15. [Google Scholar] [CrossRef]
- Frazier, T.W.; Strauss, M.; Klingemier, E.W.; Zetzer, E.E.; Hardan, A.Y.; Eng, C.; Youngstrom, E.A. A meta-analysis of gaze differences to social and nonsocial information between individuals with and without autism. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 546–555. [Google Scholar] [CrossRef] [PubMed]
- Wen, T.H.; Cheng, A.; Andreason, C.; Zahiri, J.; Xiao, Y.; Xu, R.; Bao, B.; Courchesne, E.; Barnes, C.C.; Arias, S.J.; et al. Large scale validation of an early-age eye-tracking biomarker of an autism spectrum disorder subtype. Sci. Rep. 2022, 12, 4253. [Google Scholar] [CrossRef]
- Hamner, T.; Vivanti, G. Eye-Tracking Research in Autism Spectrum Disorder: What Are We Measuring and for What Purposes? J. Autism Dev. Disord. 2022, 52, 1360–1374. [Google Scholar] [CrossRef]
- Murias, M.; Major, S.; Davlantis, K.; Franz, L.; Harris, A.; Rardin, B.; Sabatos-DeVito, M.; Dawson, G. Validation of eye-tracking measures of social attention as a potential biomarker for autism clinical trials. Autism Res. 2021, 14, 2620–2633. [Google Scholar] [CrossRef] [PubMed]
- Elison, J.T.; Paterson, S.J.; Wolff, J.J.; Reznick, J.S.; Sasson, N.J.; Gu, H.; Botteron, K.N.; Dager, S.R.; Estes, A.M.; Evans, A.C.; et al. White matter microstructure and atypical visual orienting in 7-month-olds at risk for autism. Am. J. Psychiatry 2013, 170, 899–908. [Google Scholar] [CrossRef]
- Elsabbagh, M.; Fernandes, J.; Webb, S.J.; Dawson, G.; Charman, T.; Johnson, M.H.; British Autism Study of Infant Siblings Team. Disengagement of visual attention in infancy is associated with emerging autism in toddlerhood. Biol. Psychiatry 2013, 74, 189–194. [Google Scholar] [CrossRef]
- Chawarska, K.; Volkmar, F.; Klin, A. Limited attentional bias for faces in toddlers with autism spectrum disorders. Arch. Gen. Psychiatry 2010, 67, 178–185. [Google Scholar]
- Hansen, S.N.; Schendel, D.E.; Francis, R.W.; Windham, G.C.; Bresnahan, M.; Levine, S.Z.; Reichenberg, A.; Gissler, M.; Kodesh, A.; Bai, D.; et al. Recurrence Risk of Autism in Siblings and Cousins: A Multinational, Population-Based Study. J. Am. Acad. Child Adolesc. Psychiatry 2019, 58, 866–875. [Google Scholar] [CrossRef]
- Ozonoff, S.; Young, G.S.; Carter, A.; Messinger, D.; Yirmiya, N.; Zwaigenbaum, L.; Bryson, S.; Carver, L.J.; Constantino, J.N.; Dobkins, K.; et al. Recurrence risk for autism spectrum disorders: A Baby Siblings Research Consortium study. Pediatrics 2011, 128, e488–e495. [Google Scholar] [CrossRef]
- Luyster, R.; Gotham, K.; Guthrie, W.; Coffing, M.; Petrak, R.; Pierce, K.; Bishop, S.; Esler, A.; Hus, V.; Oti, R.; et al. The Autism Diagnostic Observation Schedule—Toddler Module: A new module of a standardized diagnostic measure for autism spectrum disorders. J. Autism Dev. Disord. 2009, 39, 1305–1320. [Google Scholar] [CrossRef]
- Griffiths, R. Griffiths Mental Developmental Scales-Extended Revised; Hogrefe Limited: Oxford, UK, 2006. [Google Scholar]
- Sparrow, S.S.; Cicchetti, D.V.; Balla, D.A. Vineland Adaptive Behavior Scales, 2nd ed.; American Guidance Service: Circle Pines, MN, USA, 2005. [Google Scholar]
- Chita-Tegmark, M. Social attention in ASD: A review and meta-analysis of eye-tracking studies. Res. Dev. Disabil. 2016, 48, 79–93. [Google Scholar] [CrossRef] [PubMed]
- Bradshaw, J.; Shic, F.; Holden, A.N.; Horowitz, E.J.; Barrett, A.C.; German, T.C.; Vernon, T.W. The Use of Eye Tracking as a Biomarker of Treatment Outcome in a Pilot Randomized Clinical Trial for Young Children with Autism. Autism Res. Off. J. Int. Soc. Autism Res. 2019, 12, 779–793. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Cohen, J. The effect size. In Statistical Power Analysis for the Behavioral Sciences; Routledge: Abingdon, UK, 1988; pp. 77–83. [Google Scholar]
- Costanzo, V.; Narzisi, A.; Cerullo, S.; Crifaci, G.; Boncoddo, M.; Turi, M.; Apicella, F.; Tancredi, R.; Muratori, F.; Calderoni, S.; et al. High-Risk Siblings without Autism: Insights from a Clinical and Eye-Tracking Study. J. Pers. Med. 2022, 12, 1789. [Google Scholar] [CrossRef]
- Souter, N.E.; Arunachalam, S.; Luyster, R.J. The robustness of eye–mouth index as an eye-tracking metric of social attention in toddlers. Int. J. Behav. Dev. 2020, 44, 469–478. [Google Scholar] [CrossRef]
- Frick, J.E.; Colombo, J.; Saxon, T.F. Individual and developmental differences in disengagement of fixation in early infancy. Child Dev. 1999, 70, 537–548. [Google Scholar] [CrossRef] [PubMed]
- Mundy, P.; Delgado, C.; Block, J.; Venezia, M.; Hogan, A.; Seibert, J. Early Social Communication Scales (ESCS); University of Miami: Coral Gables, FL, USA, 2003. [Google Scholar]
- Noldus. The Observer Reference Manual, Version 10.0; Noldus Information Technology bv Sede Internazionale: Wageningen, The Netherlands, 2010.
- Ronconi, L.; Cantiani, C.; Riva, V.; Franchin, L.; Bettoni, R.; Gori, S.; Bulf, H.; Valenza, E.; Facoetti, A. Infants’ reorienting efficiency depends on parental autistic traits and predicts future socio-communicative behaviors. Cereb. Cortex 2024, 34, 40–49. [Google Scholar] [CrossRef]
- Schietecatte, I.; Roeyers, H.; Warreyn, P. Exploring the nature of joint attention impairments in young children with autism spectrum disorder: Associated social and cognitive skills. J. Autism Dev. Disord. 2012, 42, 1–12. [Google Scholar] [CrossRef]
- Karmiloff-Smith, A. An Alternative to Domain-general or Domain-specific Frameworks for Theorizing about Human Evolution and Ontogenesis. AIMS Neurosci. 2015, 2, 91–104. [Google Scholar] [CrossRef]
- Landry, R.; Bryson, S.E. Impaired disengagement of attention in young children with autism. J. Child Psychol. Psychiatry 2004, 45, 1115–1122. [Google Scholar] [CrossRef]
- Bryson, S.E.; Zwaigenbaum, L.; Brian, J.; Roberts, W.; Szatmari, P.; Rombough, V.; McDermott, C. A prospective case series of high-risk infants who developed autism. J. Autism Dev. Disord. 2007, 37, 12–24. [Google Scholar] [CrossRef]
- Canu, D.; Van der Paelt, S.; Canal-Bedia, R.; Posada, M.; Vanvuchelen, M.; Roeyers, H. Early non social behavioural indicators of autism spectrum disorder (ASD) in siblings at elevated likelihood for ASD: A systematic review. Eur. Child Adolesc. Psychiatry 2021, 30, 497–538. [Google Scholar] [CrossRef] [PubMed]
- Inui, T.; Kumagaya, S.; Myowa-Yamakoshi, M. Neurodevelopmental hypothesis about the etiology of autism spectrum disorders. Front. Hum. Neurosci. 2017, 11, 354. [Google Scholar] [CrossRef] [PubMed]
- Mundy, P.; Bullen, J. The bidirectional social-cognitive mechanisms of the social-attention symptoms of autism. Front. Psychiatry 2022, 12, 2570. [Google Scholar] [CrossRef] [PubMed]
- Franchini, M.; Duku, E.; Armstrong, V.; Brian, J.; Bryson, S.E.; Garon, N.; Roberts, W.; Roncadin, C.; Zwaigenbaum, L.; Smith, I.M. Variability in verbal and nonverbal communication in infants at risk for autism spectrum disorder: Predictors and outcomes. J. Autism Dev. Disord. 2018, 48, 3417–3431. [Google Scholar] [CrossRef]
- Wass, S.; Porayska-Pomsta, K.; Johnson, M.H. Training attentional control in infancy. Curr. Biol. 2011, 21, 1543–1547. [Google Scholar] [CrossRef]
- Zwaigenbaum, L.; Bryson, S.; Rogers, T.; Roberts, W.; Brian, J.; Szatmari, P. Behavioral manifestations of autism in the first year of life. Int. J. Dev. Neurosci. 2005, 23, 143–152. [Google Scholar] [CrossRef]
- Gangi, D.N.; Ibañez, L.V.; Messinger, D.S. Joint attention initiation with and without positive affect: Risk group differences and associations with ASD symptoms. J. Autism Dev. Disord. 2014, 44, 1414–1424. [Google Scholar] [CrossRef]
- Ibanez, L.V.; Grantz, C.J.; Messinger, D.S. The development of referential communication and autism symptomatology in high-risk infants. Infancy 2013, 18, 687–707. [Google Scholar] [CrossRef]
- Landa, R.J.; Gross, A.L.; Stuart, E.A.; Faherty, A. Developmental trajectories in children with and without autism spectrum disorders: The first 3 years. Child Dev. 2013, 84, 429–442. [Google Scholar] [CrossRef]
- Parlade, M.V.; Iverson, J.M. The development of coordinated communication in infants at heightened risk for autism spectrum disorder. J. Autism Dev. Disord. 2015, 45, 2218–2234. [Google Scholar] [CrossRef]
- Thorup, E.; Nyström, P.; Gredebäck, G.; Bölte, S.; Falck-Ytter, T.; EASE Team. Altered gaze following during live interaction in infants at risk for autism: An eye tracking study. Mol. Autism 2016, 7, 12. [Google Scholar] [CrossRef] [PubMed]
- Bedford, R.; Pickles, A.; Gliga, T.; Elsabbagh, M.; Charman, T.; Johnson, M.H.; BASIS Team. Additive effects of social and non-social attention during infancy relate to later autism spectrum disorder. Dev. Sci. 2014, 17, 612–620. [Google Scholar] [CrossRef]
- Atkinson, J.; Braddick, O. Visual attention in the first years: Typical development and developmental disorders. Dev. Med. Child Neurol. 2012, 54, 589–595. [Google Scholar] [CrossRef]
- Hitzert, M.M.; Van Braeckel, K.N.; Bos, A.F.; Hunnius, S.; Geuze, R.H. Early visual attention in preterm and fullterm infants in relation to cognitive and motor outcomes at school age: An exploratory study. Front. Pediatr. 2014, 2, 106. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, J.; Braddick, O.; Anker, S.; Nardini, M.; Birtles, D.; Rutherford, M.A.; Mercuri, E.; Dyet, L.E.; Edwards, A.D.; Cowan, F.M. Cortical vision, MRI and developmental outcome in preterm infants. Arch. Dis. Child.-Fetal Neonatal Ed. 2008, 93, F292–F297. [Google Scholar] [CrossRef]
- Mercuri, E.; Rutherford, M.; Cowan, F.; Pennock, J.; Counsell, S.; Papadimitriou, M.; Azzopardi, D.; Bydder, G.; Dubowitz, L. Early prognostic indicators of outcome in infants with neonatal cerebral infarction: A clinical, electroencephalogram, and magnetic resonance imaging study. Pediatrics 1999, 103, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Hus, V.; Pickles, A.; Cook, E.H., Jr.; Risi, S.; Lord, C. Using the autism diagnostic interview—Revised to increase phenotypic homogeneity in genetic studies of autism. Biol. Psychiatry 2007, 61, 438–448. [Google Scholar] [CrossRef]
- Ozdemir, S.; Akin-Bulbul, I.; Kok, I.; Ozdemir, S. Development of a visual attention based decision support system for autism spectrum disorder screening. Int. J. Psychophysiol. 2022, 173, 69–81. [Google Scholar] [CrossRef]
- Billeci, L.; Narzisi, A.; Tonacci, A.; Sbriscia-Fioretti, B.; Serasini, L.; Fulceri, F.; Apicella, F.; Sicca, F.; Calderoni, S.; Muratori, F. An integrated EEG and eye-tracking approach for the study of responding and initiating joint attention in Autism Spectrum Disorders. Sci. Rep. 2017, 7, 13560. [Google Scholar] [CrossRef]
- Han, J.; Jiang, G.; Ouyang, G.; Li, X. A multimodal approach for identifying autism spectrum disorders in children. IEEE Trans. Neural Syst. Rehabil. Eng. 2022, 30, 2003–2011. [Google Scholar] [CrossRef] [PubMed]
- Charman, T.; Young, G.S.; Brian, J.; Carter, A.; Carver, L.J.; Chawarska, K.; Hertz-Picciotto, I. Non-ASD outcomes at 36 months in siblings at familial risk for autism spectrum disorder (ASD): A baby siblings research consortium (BSRC) study. Autism Res. 2017, 10, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Shephard, E.; Milosavljevic, B.; Pasco, G.; Jones, E.J.; Gliga, T.; Happé, F.; Johnson, M.H.; Charman, T. the BASIS team Mid-childhood outcomes of infant siblings at familial high-risk of autism spectrum disorder. Autism Res. 2017, 10, 546–557. [Google Scholar] [CrossRef] [PubMed]
- Landa, R.J.; Reetzke, R.; Holingue, C.B.; Herman, D.; Hess, C.R. Diagnostic stability and phenotypic differences among school-age children diagnosed with ASD before age 2. Front. Psychiatry 2022, 13, 805686. [Google Scholar] [CrossRef]
- Pierce, K.; Gazestani, V.H.; Bacon, E.; Barnes, C.C.; Cha, D.; Nalabolu, S.; Lopez, L.; Moore, A.; Pence-Stophaeros, S.; Courchesne, E. Evaluation of the diagnostic stability of the early autism spectrum disorder phenotype in the general population starting at 12 months. JAMA Pediatr. 2019, 173, 578–587. [Google Scholar] [CrossRef]
- Zwaigenbaum, L.; Bryson, S.E.; Brian, J.; Smith, I.M.; Roberts, W.; Szatmari, P.; Roncadin, C.; Garon, N.; Vaillancourt, T. Stability of diagnostic assessment for autism spectrum disorder between 18 and 36 months in a high-risk cohort. Autism Res. 2016, 9, 790–800. [Google Scholar] [CrossRef]
- Ozonoff, S.; Young, G.S.; Landa, R.J.; Brian, J.; Bryson, S.; Charman, T.; Chawarska, K.; Macari, S.L.; Messinger, D.; Stone, W.L.; et al. Diagnostic stability in young children at risk for autism spectrum disorder: A baby siblings research consortium study. J. Child Psychol. Psychiatry 2015, 56, 988–998. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costanzo, V.; Apicella, F.; Billeci, L.; Mancini, A.; Tancredi, R.; Beretta, C.; Muratori, F.; Vivanti, G.; Calderoni, S. Altered Visual Attention at 12 Months Predicts Joint Attention Ability and Socio-Communicative Development at 24 Months: A Single-Center Eye-Tracking Study on Infants at Elevated Likelihood to Develop Autism. Appl. Sci. 2025, 15, 3288. https://doi.org/10.3390/app15063288
Costanzo V, Apicella F, Billeci L, Mancini A, Tancredi R, Beretta C, Muratori F, Vivanti G, Calderoni S. Altered Visual Attention at 12 Months Predicts Joint Attention Ability and Socio-Communicative Development at 24 Months: A Single-Center Eye-Tracking Study on Infants at Elevated Likelihood to Develop Autism. Applied Sciences. 2025; 15(6):3288. https://doi.org/10.3390/app15063288
Chicago/Turabian StyleCostanzo, Valeria, Fabio Apicella, Lucia Billeci, Alice Mancini, Raffaella Tancredi, Carolina Beretta, Filippo Muratori, Giacomo Vivanti, and Sara Calderoni. 2025. "Altered Visual Attention at 12 Months Predicts Joint Attention Ability and Socio-Communicative Development at 24 Months: A Single-Center Eye-Tracking Study on Infants at Elevated Likelihood to Develop Autism" Applied Sciences 15, no. 6: 3288. https://doi.org/10.3390/app15063288
APA StyleCostanzo, V., Apicella, F., Billeci, L., Mancini, A., Tancredi, R., Beretta, C., Muratori, F., Vivanti, G., & Calderoni, S. (2025). Altered Visual Attention at 12 Months Predicts Joint Attention Ability and Socio-Communicative Development at 24 Months: A Single-Center Eye-Tracking Study on Infants at Elevated Likelihood to Develop Autism. Applied Sciences, 15(6), 3288. https://doi.org/10.3390/app15063288