
The Integration of Cone Beam Computed Tomography, Artificial Intelligence, Augmented Reality, and Virtual Reality in Dental Diagnostics, Surgical Planning, and Education: A Narrative Review



Abstract
1. Introduction
2. Materials and Methods
- Focused on the application of CBCT, AI, AR/VR, or related digital imaging technologies in dentistry;
- Provided empirical data (clinical trials, observational studies, or systematic reviews) or were technical papers with clear relevance to diagnostics, surgery, or education;
- They were published in peer-reviewed journals.
- Relevance to dental clinical practice,
- Level of evidence (e.g., randomized controlled trials, cohort studies, technical validation),
- Technological innovation and clinical impact.
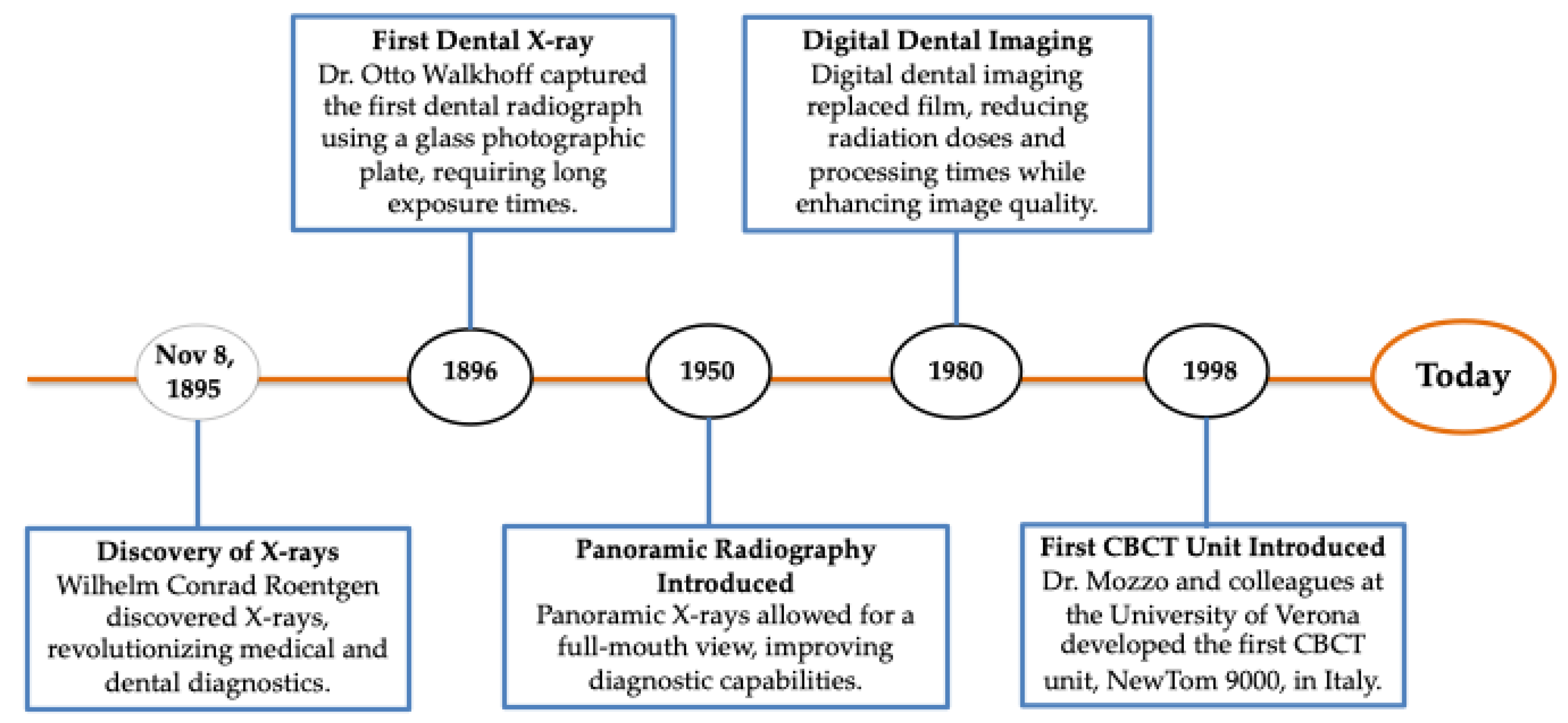
3. Evolution of Radiographic Practice: From Traditional to Digital Imaging
4. Modern Imaging Technologies
4.1. Portable Imaging Devices
4.2. CBCT: A Foundation for 3D Visualization
4.3. Photon-Counting Computed Tomography
4.4. Recent Advances in Radiation Protection in Dental Imaging
5. Enhancement of Dental Imaging Protocols and Applications
5.1. AI Integration and Machine Learning (ML) in Dental Imaging
5.2. Imaging-Guided Diagnosis and Treatment Planning
5.2.1. Endodontics
5.2.2. Implantology
5.2.3. Orthodontics
5.2.4. Forensic Dentistry
5.3. Protocol Optimization in Surgical Imaging
6. The Digital Frontier: AR/VR Applications in Dental Surgery and Education
7. Limitations and Challenges in AI Integration
8. Future Perspectives
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Shah, P.; Zalavadia, K. Recent Advances in Dental Imaging. Sch. J. Dent. Sci. 2021, 8, 184–188. [Google Scholar] [CrossRef]
- Katsumata, A. Deep learning and artificial intelligence in dental diagnostic imaging. Jpn. Dent. Sci. Rev. 2023, 59, 329–333. [Google Scholar] [CrossRef]
- Pauwels, R. History of Dental Radiography: Evolution of 2D and 3D Imaging Modalities. Med. Phys. Int. J. 2020, 3, 235–277. [Google Scholar]
- de Magalhães, A.A.; Santos, A.T. Advancements in Diagnostic Methods and Imaging Technologies in Dentistry: A Literature Review of Emerging Approaches. J. Clin. Med. 2025, 14, 1277. [Google Scholar] [CrossRef]
- Jayachandran, S. Digital Imaging in Dentistry: A review. Contemp. Clin. Dent. 2017, 8, 193–194. [Google Scholar] [CrossRef]
- Elkhateeb, S.M.; Aloyouny, A.Y.; Omer, M.M.S.; Mansour, S.M. Analysis of photostimulable phosphor image plate artifacts and their prevalence. World J. Clin. Cases 2022, 10, 437–447. [Google Scholar] [CrossRef]
- Martins, G.C.; Rocha, T.G.; de Lima Azeredo, T.; de Castro Domingos, A.; Visconti, M.A.; Villoria, E.M. Hand-held dental X-ray device: Attention to correct use. Imaging Sci. Dent. 2023, 53, 265–266. [Google Scholar] [CrossRef]
- Nitschke, J.; Schorn, L.; Holtmann, H.; Zeller, U.; Handschel, J.; Sonntag, D.; Lommen, J. Image quality of a portable X-ray device (Nomad Pro 2) compared to a wall-mounted device in intraoral radiography. Oral Radiol. 2021, 37, 224–230. [Google Scholar] [CrossRef]
- Kazimierczak, W.; Wajer, R.; Komisarek, O.; Dyszkiewicz-Konwińska, M.; Wajer, A.; Kazimierczak, N.; Janiszewska-Olszowska, J.; Serafin, Z. Evaluation of a Vendor-Agnostic Deep Learning Model for Noise Reduction and Image Quality Improvement in Dental CBCT. Diagnostics 2024, 14, 2410. [Google Scholar] [CrossRef]
- Baccher, S.; Gowdar, I.; Guruprasad, Y.; Solanki, R.; Medhi, R.; Shah, M.; Mehta, D. CBCT: A Comprehensive Overview of its Applications and Clinical Significance in Dentistry. J. Pharm. Bioallied Sci. 2024, 16, S1923–S1925. [Google Scholar] [CrossRef]
- Hora, B.; Varghese, A.; Patil, P.; Anbalagan, S.; Sagolsem, C.; Shaik, N. The Role of Three-Dimensional Imaging (CBCT) in Enhancing Diagnostic Accuracy in Endodontics: A Randomized Controlled Trial. J. Pharm. Bioallied Sci. 2024, 16, S874–S876. [Google Scholar] [CrossRef]
- Vasegh, Z.; Safi, Y.; Azar, M.S.; Ahsaie, M.G.; Arianezhad, S.M. Assessment of bony changes in temporomandibular joint in patients using cone beam computed tomography—A cross sectional study. Head Face Med. 2023, 19, 47. [Google Scholar] [CrossRef]
- Weiss, R., 2nd; Read-Fuller, A. Cone Beam Computed Tomography in Oral and Maxillofacial Surgery: An Evidence-Based Review. Dent. J. 2019, 7, 52. [Google Scholar] [CrossRef]
- Joachim, M.V.; Miloro, M. The Evolution of Virtual Surgical Planning in Craniomaxillofacial Surgery: A Comprehensive Review. J. Oral Maxillofac. Surg. 2025, 83, 294–306. [Google Scholar] [CrossRef]
- Srinivas-Rao, S.; Cao, J.; Marin, D.; Kambadakone, A. Dual-Energy Computed Tomography to Photon Counting Computed Tomography: Emerging Technological Innovations. Radiol. Clin. N. Am. 2023, 61, 933–944. [Google Scholar] [CrossRef]
- Zanon, C.; Pepe, A.; Cademartiri, F.; Bini, C.; Maffei, E.; Quaia, E.; Stellini, E.; Di Fiore, A. Potential Benefits of Photon-Counting CT in Dental Imaging: A Narrative Review. J. Clin. Med. 2024, 13, 2436. [Google Scholar] [CrossRef]
- Dogra, S.; Shekhrajka, N.; Moonis, G. A Review of Applications of Photon-Counting Computed Tomography in Head and Neck Imaging. Br. J. Radiol. 2024, tqae226. [Google Scholar] [CrossRef]
- Shah, N.; Bansal, N.; Logani, A. Recent advances in imaging technologies in dentistry. World J. Radiol. 2014, 6, 794–807. [Google Scholar] [CrossRef]
- Kaasalainen, T.; Uusitalo, A.; Mäki, M. Dental cone beam CT: An updated review. Phys. Med. 2022, 88, 193–217. [Google Scholar] [CrossRef]
- Miragall, M.F.; Knoedler, S.; Kauke-Navarro, M.; Saadoun, R.; Grabenhorst, A.; Grill, F.D.; Ritschl, L.M.; Fichter, A.M.; Safi, A.-F.; Knoedler, L. Face the Future—Artificial Intelligence in Oral and Maxillofacial Surgery. J. Clin. Med. 2023, 12, 6843. [Google Scholar] [CrossRef]
- Tsapaki, V. Radiation Protection in Dental Radiology—Recent Advances and Future Directions. Phys. Med. 2017, 44, 222–226. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Zhang, Y.; Kalra, M.K.; Lin, F.; Chen, Y.; Liao, P.; Zhou, J.; Wang, G. Low-Dose CT With a Residual Encoder-Decoder Convolutional Neural Network. IEEE Trans. Med. Imaging 2017, 36, 2524–2535. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Hao, J.; Lin, H.; Pan, W.; Yang, J.; Feng, Y.; Wang, G.; Li, J.; Jin, Z.; Zhao, Z.; et al. Deep Learning-Enabled 3D Multimodal Fusion of Cone-Beam CT and Intraoral Mesh Scans for Clinically Applicable Tooth-Bone Reconstruction. Patterns 2023, 4, 100825. [Google Scholar] [CrossRef]
- Shujaat, S.; Riaz, M.; Jacobs, R. Synergy between artificial intelligence and precision medicine for computer-assisted oral and maxillofacial surgical planning. Clin. Oral Investig. 2023, 27, 897–906. [Google Scholar] [CrossRef] [PubMed]
- Kot, W.Y.; Au Yeung, S.Y.; Leung, Y.Y.; Leung, P.H.; Yang, W.F. Evolution of deep learning tooth segmentation from CT/CBCT images: A systematic review and meta-analysis. BMC Oral Health 2025, 25, 800. [Google Scholar] [CrossRef]
- Vial, A.; Stirling, D.; Field, M.; Ros, M.; Ritz, C.; Carolan, M.; Holloway, L.; Miller, A.A. The Role of Deep Learning and Radiomic Feature Extraction in Cancer-Specific Predictive Modelling: A Review. Transl. Cancer Res. 2018, 7, 803–816. [Google Scholar] [CrossRef]
- Hung, K.F.; Ai, Q.Y.H.; Wong, L.M.; Yeung, A.W.K.; Li, D.T.S.; Leung, Y.Y. Current Applications of Deep Learning and Radiomics on CT and CBCT for Maxillofacial Diseases. Diagnostics 2022, 13, 110. [Google Scholar] [CrossRef]
- Mayerhoefer, M.E.; Materka, A.; Langs, G.; Häggström, I.; Szczypiński, P.; Gibbs, P.; Cook, G. Introduction to Radiomics. J. Nucl. Med. 2020, 61, 488–495. [Google Scholar] [CrossRef]
- Tandon, D.; Rajawat, J. Present and Future of Artificial Intelligence in Dentistry. J. Oral Biol. Craniofacial Res. 2020, 10, 391–396. [Google Scholar] [CrossRef]
- Iruvuri, A.G.; Miryala, G.; Khan, Y.; Ramalingam, N.T.; Sevugaperumal, B.; Soman, M.; Padmanabhan, A. Revolutionizing Dental Imaging: A Comprehensive Study on the Integration of Artificial Intelligence in Dental and Maxillofacial Radiology. Cureus 2023, 15, e50292. [Google Scholar] [CrossRef]
- Ríos-Osorio, N.; Quijano-Guauque, S.; Briñez-Rodríguez, S.; Velasco-Flechas, G.; Muñoz-Solís, A.; Chávez, C.; Fernandez-Grisales, R. Cone-Beam Computed Tomography in Endodontics: From the Specific Technical Considerations of Acquisition Parameters and Interpretation to Advanced Clinical Applications. Restor. Dent. Endod. 2023, 49, e1. [Google Scholar] [CrossRef] [PubMed]
- Schloss, T.; Sonntag, D.; Kohli, M.R.; Setzer, F.C. A Comparison of 2- and 3-Dimensional Healing Assessment after Endodontic Surgery Using Cone-Beam Computed Tomographic Volumes or Periapical Radiographs. J. Endod. 2017, 43, 1072–1079. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wang, B.; Liu, Y.Y.; Luo, Y.; Wu, Y.; Xiang, L.; Yang, X.; Qu, Y.; Tian, T.; Man, Y. Recent Advances in Digital Technology in Implant Dentistry. J. Dent. Res. 2024, 103, 787–799. [Google Scholar] [CrossRef]
- Bianchi, J.; Mendonca, G.; Gillot, M.; Oh, H.; Park, J.; Turkestani, N.A.; Gurgel, M.; Cevidanes, L. Three-Dimensional Digital Applications for Implant Space Planning in Orthodontics: A Narrative Review. J. World Fed. Orthod. 2022, 11, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Polizzi, A.; Serra, S.; Leonardi, R. Use of CBCT in Orthodontics: A Scoping Review. J. Clin. Med. 2024, 13, 6941. [Google Scholar] [CrossRef]
- Pandey, R.; Kamble, R.; Kanani, H. Revolutionizing Smiles: Advancing Orthodontics Through Digital Innovation. Cureus 2024, 16, e64086. [Google Scholar] [CrossRef]
- Perkins, H.; Chiam, T.L.; Forrest, A.; Higgins, D. 3D Dental Images in Forensic Odontology: A Scoping Review of Superimposition Approaches Utilizing 3D Imaging. Forensic Imaging 2025, 40, 200622. [Google Scholar] [CrossRef]
- Christoloukas, N.; Mitsea, A.; Rontogianni, A.; Papadakis, E.; Angelopoulos, C. Evaluation of Bitemark Analysis’s Potential Application in Forensic Identification: A Systematic Review. Diagnostics 2024, 14, 1180. [Google Scholar] [CrossRef]
- Thurzo, A.; Kosnáčová, H.S.; Kurilová, V.; Kosmeľ, S.; Beňuš, R.; Moravanský, N.; Kováč, P.; Kuracinová, K.M.; Palkovič, M.; Varga, I. Use of Advanced Artificial Intelligence in Forensic Medicine, Forensic Anthropology and Clinical Anatomy. Healthcare 2021, 9, 1545. [Google Scholar] [CrossRef]
- Saini, R.S.; Bavabeedu, S.S.; Quadri, S.A.; Gurumurthy, V.; Kanji, M.A.; Kuruniyan, M.S.; Binduhayyim, R.I.H.; Avetisyan, A.; Heboyan, A. Impact of 3D Imaging Techniques and Virtual Patients on the Accuracy of Planning and Surgical Placement of Dental Implants: A Systematic Review. Digit. Health 2024, 10, 20552076241253550. [Google Scholar] [CrossRef]
- Yepes, J.F.; Al-Sabbagh, M. Use of cone-beam computed tomography in early detection of implant failure. Dent. Clin. N. Am. 2015, 59, 41–56. [Google Scholar] [CrossRef] [PubMed]
- Jiang, W.; Ma, L.; Zhang, B.; Fan, Y.; Qu, X.; Zhang, X.; Liao, H. Evaluation of the 3D Augmented Reality-Guided Intraoperative Positioning of Dental Implants in Edentulous Mandibular Models. Int. J. Oral Maxillofac. Implant. 2018, 33, 1219–1228. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.Y.; Chen, T.C.; Lin, C.J.; Huang, C.C.; Tsai, Y.H.; Tsai, Y.L.; Wang, C.Y. The Use of Augmented Reality (AR) and Virtual Reality (VR) in Dental Surgery Education and Practice: A Narrative Review. J. Dent. Sci. 2024, 19, S91–S101. [Google Scholar] [CrossRef] [PubMed]
- Fahim, S.; Maqsood, A.; Das, G.; Ahmed, N.; Saquib, S.; Lal, A.; Khan, A.A.G.; Alam, M.K. Augmented Reality and Virtual Reality in Dentistry: Highlights from the Current Research. Appl. Sci. 2022, 12, 3719. [Google Scholar] [CrossRef]
- Al-Saud, L.M.; Mushtaq, F.; Allsop, M.J.; Culmer, P.C.; Mirghani, I.; Yates, E.; Keeling, A.; Mon-Williams, M.A.; Manogue, M. Feedback and motor skill acquisition using a haptic dental simulator. Eur. J. Dent. Educ. 2017, 21, 240–247. [Google Scholar] [CrossRef]
- Mosch, R.; Alevizakos, V.; Ströbele, D.A.; Schiller, M.; von See, C. Exploring augmented reality for dental implant surgery: Feasibility of using smartphones as navigation tools. Clin. Exp. Dent. Res. 2025, 11, e70110. [Google Scholar] [CrossRef]
- Ayoub, A.; Pulijala, Y. The Application of Virtual Reality and Augmented Reality in Oral & Maxillofacial Surgery. BMC Oral Health 2019, 19, 238. [Google Scholar] [CrossRef]
- García-Robles, P.; Cortés-Pérez, I.; Nieto-Escámez, F.A.; García-López, H.; Obrero-Gaitán, E.; Osuna-Pérez, M.C. Immersive virtual reality and augmented reality in anatomy education: A systematic review and meta-analysis. Anat. Sci. Educ. 2024, 17, 514–528. [Google Scholar] [CrossRef]
- Reiners, D.; Davahli, M.R.; Karwowski, W.; Cruz-Neira, C. The Combination of Artificial Intelligence and Extended Reality: A Systematic Review. Front. Virtual Real. 2021, 2, 721933. [Google Scholar] [CrossRef]
- Dinh, A.; Yin, A.L.; Estrin, D.; Greenwald, P.; Fortenko, A. Augmented Reality in Real-time Telemedicine and Telementoring: Scoping Review. JMIR mHealth uHealth 2023, 11, e45464. [Google Scholar] [CrossRef]
- Moreno Arjonilla, J.; López Ruiz, A.; Jiménez, J.R.; Aguilera, J.; Jurado, J.M. Eye-tracking on Virtual Reality: A Survey. Virtual Real. 2024, 28, 38. [Google Scholar] [CrossRef]
- Aliwi, I.; Schot, V.; Carrabba, M.; Duong, P.; Shievano, S.; Caputo, M.; Wray, J.; de Vecchi, A.; Biglino, G. The Role of Immersive Virtual Reality and Augmented Reality in Medical Communication: A Scoping Review. J. Patient Exp. 2023, 10, 23743735231171562. [Google Scholar] [CrossRef] [PubMed]
- Lacoche, J.; Villain, E.; Foulonneau, A. Evaluating Usability and User Experience of AR Applications in VR Simulation. Front. Virtual Real. 2022, 3, 881318. [Google Scholar] [CrossRef]
- Tai, C.-J.; Tatakis, D.N.; Chien, H.H. The Applications and Limitations of Advanced (3-Dimensional) Radiographic Imaging Techniques. In Clinical Maxillary Sinus Elevation Surgery, 1st ed.; Kao, D.W.K., Ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2014; pp. 31–56. [Google Scholar] [CrossRef]
- Ghaffari, M.; Zhu, Y.; Shrestha, A. A Review of Advancements of Artificial Intelligence in Dentistry. Dent. Rev. 2024, 4, 100081. [Google Scholar] [CrossRef]
- Schwendicke, F.; Samek, W.; Krois, J. Artificial Intelligence in Dentistry: Chances and Challenges. J. Dent. Res. 2020, 99, 769–774. [Google Scholar] [CrossRef]
- Schwendicke, F.; Singh, T.; Lee, J.-H.; Gaudin, R.; Chaurasia, A.; Wiegand, T.; Uribe, S.; Krois, J. Artificial intelligence in dental research: Checklist for authors, reviewers, readers. J. Dent. 2021, 107, 103610. [Google Scholar] [CrossRef]
- Ducret, M.; Mörch, C.M. Focus on Artificial Intelligence Ethics in Dentistry. J. Dent. Sci. 2023, 18, 1409–1410. [Google Scholar] [CrossRef]
- European Commission. Proposal for a Regulation of the European Parliament and of the Council Laying Down Harmonised Rules on Artificial Intelligence (Artificial Intelligence Act). 2021. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX%3A52021PC0206 (accessed on 21 April 2021).
- Khandare, L.; Sreekantha, D.K.; Sairam, K. A Study on Encryption Techniques to Protect the Patient Privacy in Health Care Systems. In Proceedings of the 2019 Innovations in Power and Advanced Computing Technologies (i-PACT), Vellore, India, 22–23 March 2019; IEEE: Piscataway, NJ, USA, 2019; pp. 1–5. [Google Scholar]
- FDA. Artificial Intelligence and Machine Learning (AI/ML)-Based Software as a Medical Device (SaMD) Action Plan; U.S. Food and Drug Administration: Silver Spring, MD, USA, 2022. Available online: https://www.fda.gov/media/145022/download (accessed on 25 March 2025).
- Yu, K.H.; Beam, A.L.; Kohane, I.S. Artificial intelligence in healthcare. Nat. Biomed. Eng. 2018, 2, 719–731. [Google Scholar] [CrossRef]
- Albano, D.; Galiano, V.; Basile, M.; Di Luca, F.; Gitto, S.; Messina, C.; Cagetti, M.G.; Del Fabbro, M.; Tartaglia, G.M.; Sconfienza, L.M. Artificial intelligence for radiographic imaging detection of caries lesions: A systematic review. BMC Oral Health 2024, 24, 274. [Google Scholar] [CrossRef]
- Jiang, F.; Jiang, Y.; Zhi, H.; Dong, Y.; Li, H.; Ma, S.; Wang, Y.; Dong, Q.; Shen, H.; Wang, Y. Artificial intelligence in healthcare: Past, present and future. Stroke Vasc. Neurol. 2017, 2, 230–243. [Google Scholar] [CrossRef]
- Farhadi Nia, M.; Ahmadi, M.; Irankhah, E. Transforming Dental Diagnostics with Artificial Intelligence: Advanced Integration of ChatGPT and Large Language Models for Patient Care. Front. Dent. Med. 2025, 5, 1456208. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S.Y.; Kim, S.K.; Heo, S.J.; Koak, J.Y.; Kim, J.G. Dimensional Accuracy of Dental Models for Three-Unit Prostheses Fabricated by Various 3D Printing Technologies. Materials 2021, 14, 1550. [Google Scholar] [CrossRef] [PubMed]
- Fidvi, S.; Holder, J.; Li, H.; Parnes, G.J.; Shamir, S.B.; Wake, N. Advanced 3D Visualization and 3D Printing in Radiology. Adv. Exp. Med. Biol. 2023, 1406, 103–138. [Google Scholar] [CrossRef] [PubMed]
- Elani, H.W.; Giannobile, W.V. Harnessing Artificial Intelligence to Address Oral Health Disparities. JAMA Health Forum 2024, 5, e240642. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Limitation/Challenge | Description | References |
|---|---|---|
| High Costs and Accessibility | Advanced systems like CBCT and AI platforms are expensive to acquire and maintain, limiting access in under-resourced settings. | [54,55] |
| Training and Maintenance | Clinicians require specialized training, and systems need regular updates and calibration to function effectively. | [54,55] |
| Radiation Exposure and Image Quality | Though improved, CBCT still poses radiation risks, requiring strict adherence to dose optimization protocols. | [56] |
| Inconsistent Image Quality | Operator variability and poor equipment calibration can lead to inconsistent diagnostic image quality. | [56] |
| Lack of Generalizability of AI Models (Algorithm Validation) | AI models trained on limited or non-diverse datasets perform poorly across varied demographics or imaging protocols. | [56,57] |
| Data Privacy and Security Risks | AI relies on large data volumes, raising concerns about patient consent, data breaches, and compliance with regulations. | [58,59,60] |
| Automation Bias and Black-Box Models | Clinicians may over-rely on AI outputs, especially when decisions are not explainable, leading to diagnostic errors. | [61,62] |
| Lack of Explainability | Deep learning systems often lack transparency, making it hard to understand or justify AI decisions | [61] |
| Insufficient External Validation | AI tools often lack real-world testing on varied datasets, limiting their applicability and performance consistency | [63] |
| Lack of Standardized Guidelines | There are no unified standards for evaluating, certifying, or regulating AI tools in dental radiology | [63] |
| Technical Barriers in Integration | Smaller clinics may lack IT infrastructure and staff to adopt and maintain AI tools effectively | [64] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meto, A.; Halilaj, G. The Integration of Cone Beam Computed Tomography, Artificial Intelligence, Augmented Reality, and Virtual Reality in Dental Diagnostics, Surgical Planning, and Education: A Narrative Review. Appl. Sci. 2025, 15, 6308. https://doi.org/10.3390/app15116308
Meto A, Halilaj G. The Integration of Cone Beam Computed Tomography, Artificial Intelligence, Augmented Reality, and Virtual Reality in Dental Diagnostics, Surgical Planning, and Education: A Narrative Review. Applied Sciences. 2025; 15(11):6308. https://doi.org/10.3390/app15116308
Chicago/Turabian StyleMeto, Aida, and Gerta Halilaj. 2025. "The Integration of Cone Beam Computed Tomography, Artificial Intelligence, Augmented Reality, and Virtual Reality in Dental Diagnostics, Surgical Planning, and Education: A Narrative Review" Applied Sciences 15, no. 11: 6308. https://doi.org/10.3390/app15116308
APA StyleMeto, A., & Halilaj, G. (2025). The Integration of Cone Beam Computed Tomography, Artificial Intelligence, Augmented Reality, and Virtual Reality in Dental Diagnostics, Surgical Planning, and Education: A Narrative Review. Applied Sciences, 15(11), 6308. https://doi.org/10.3390/app15116308