
Reliability of Automated Intracranial Volume Measurements by Synthetic Brain MRI in Children

 , , , and
, , , and
Abstract
1. Introduction
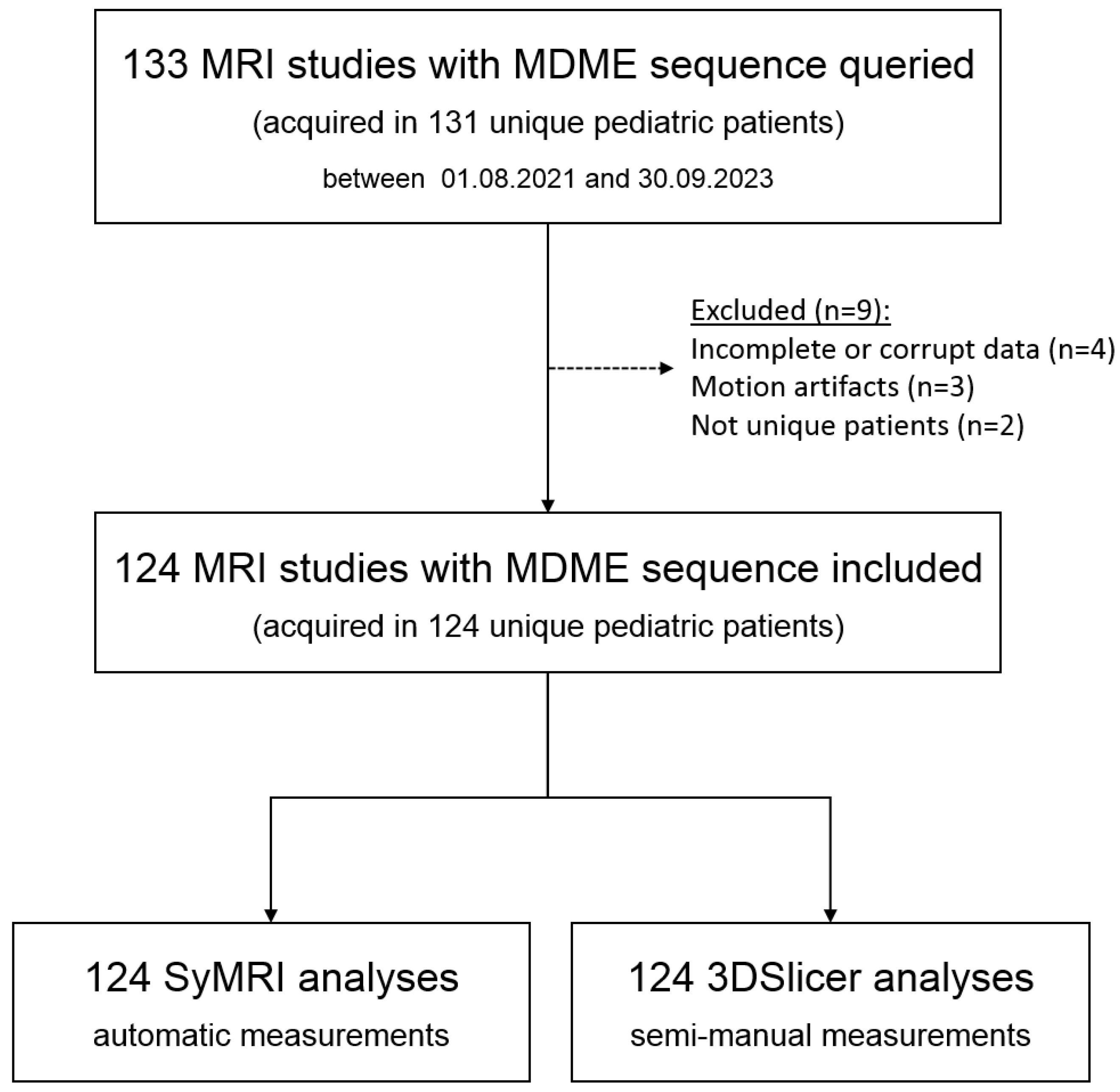
2. Materials and Methods
2.1. MRI Acquisition
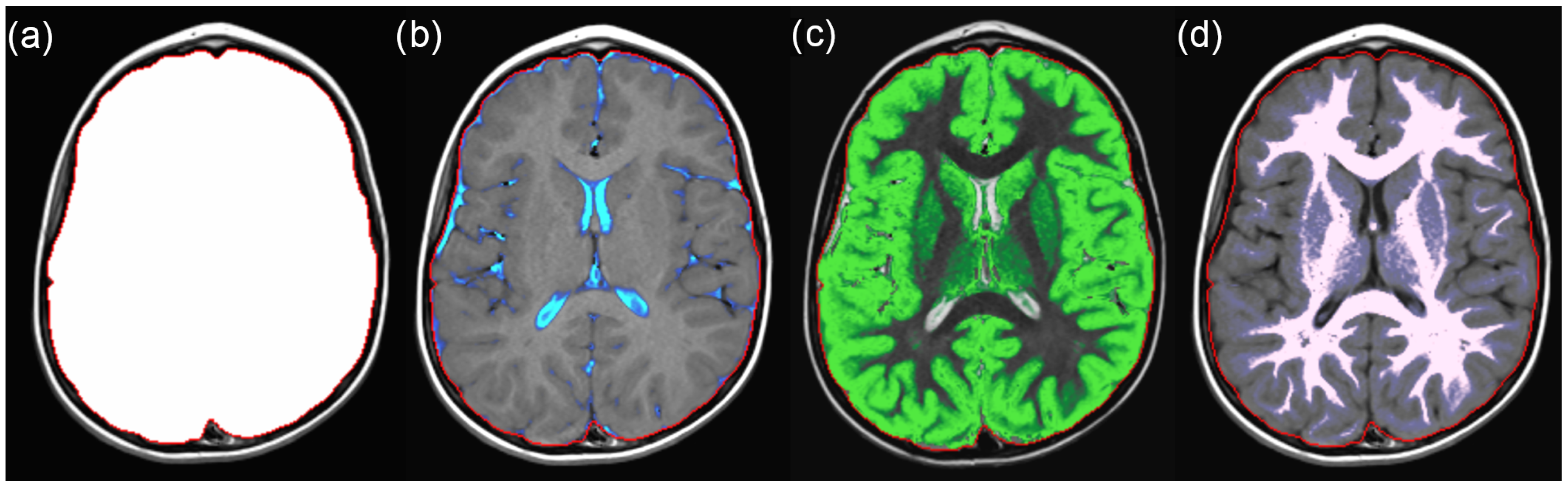
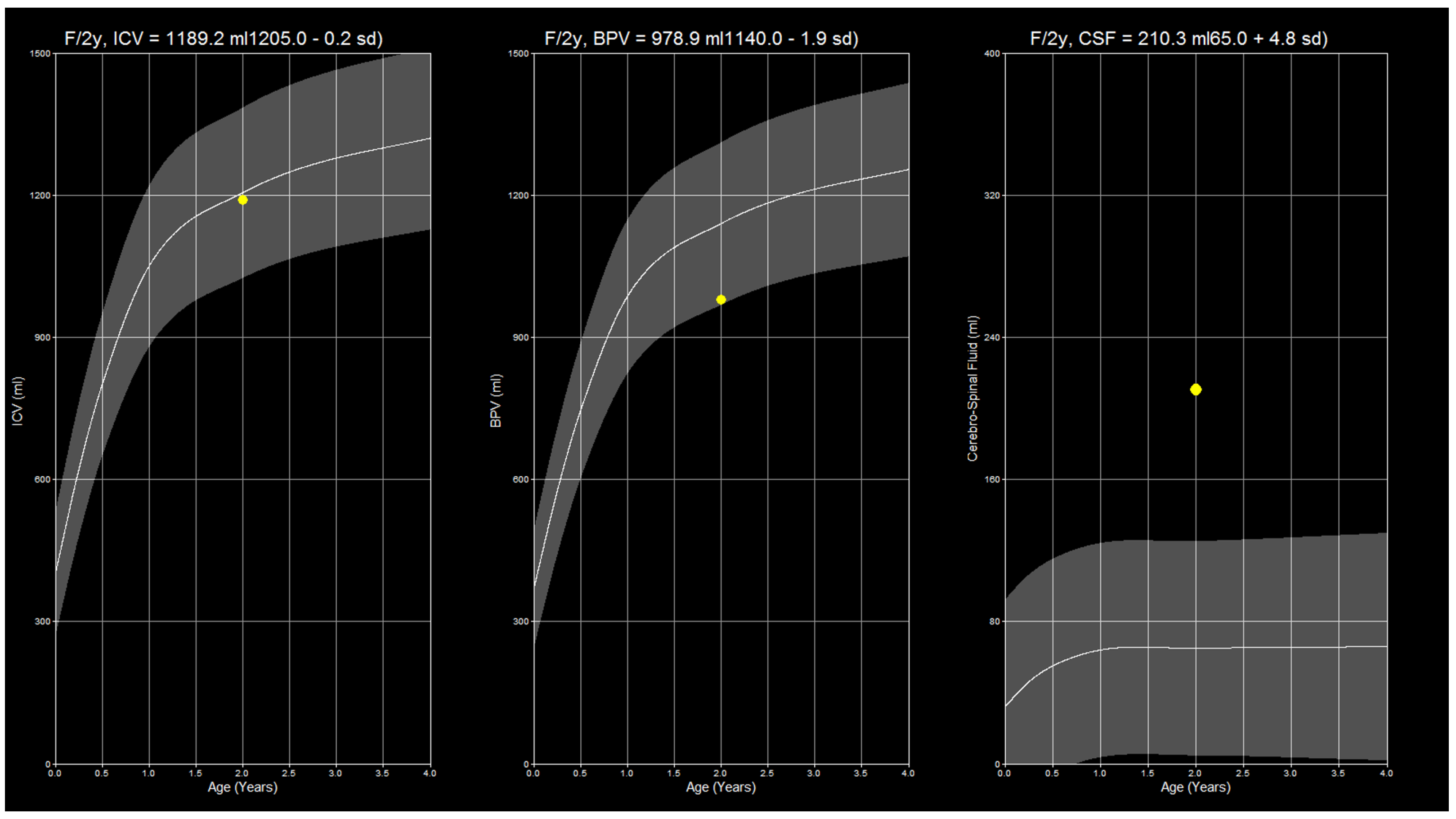
2.2. SyMRI Volume Measurements
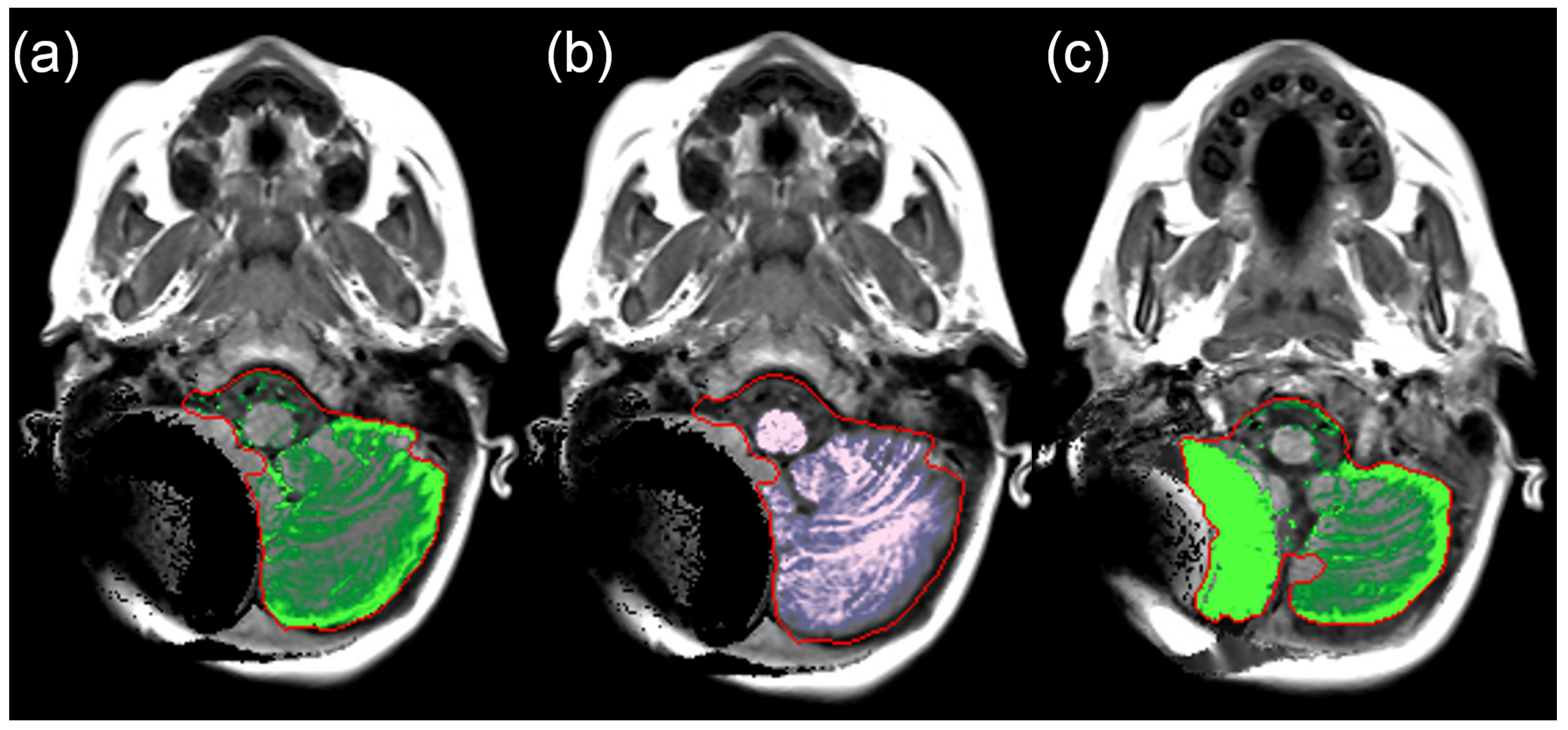
2.3. Manual Volume Measurements
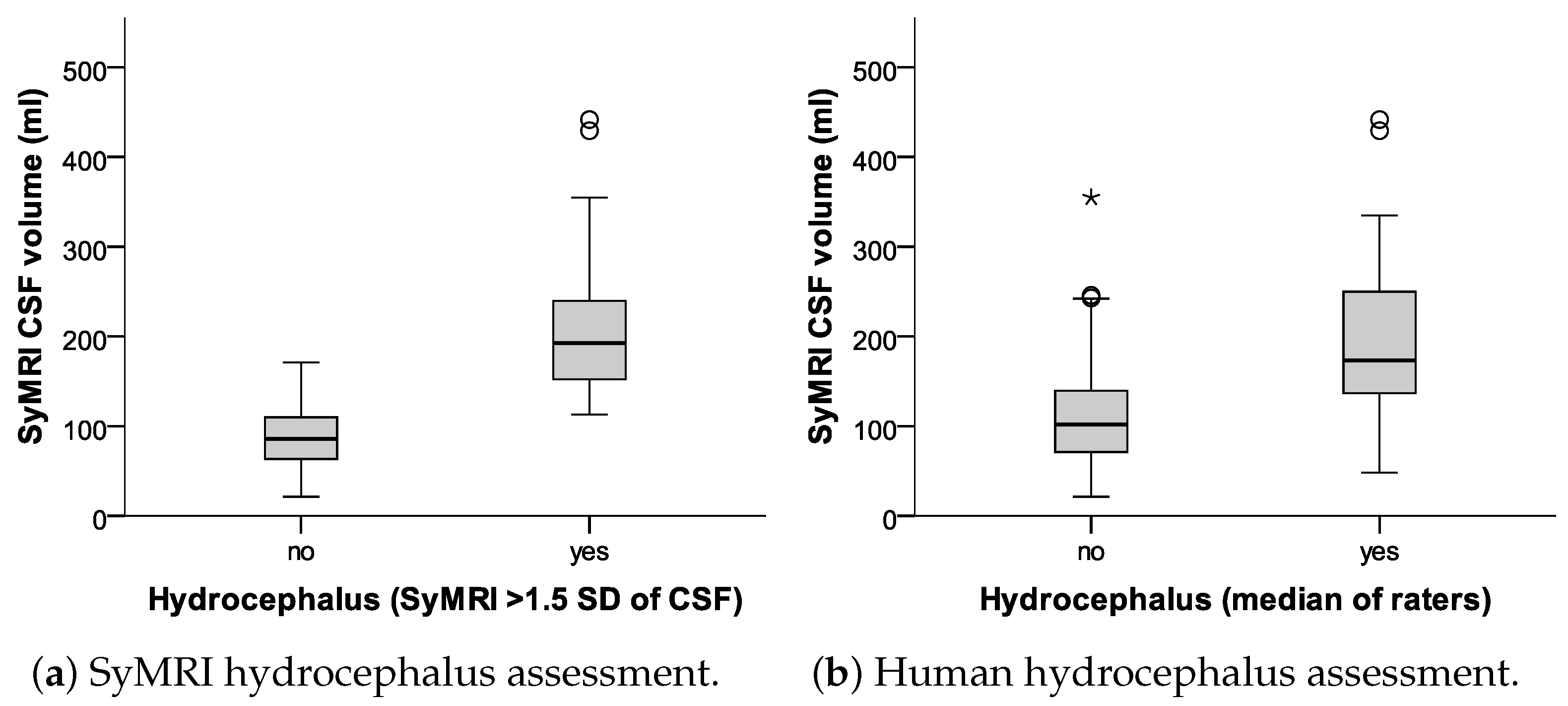
2.4. Subjective Hydrocephalus Rating
2.5. Ethical Approval
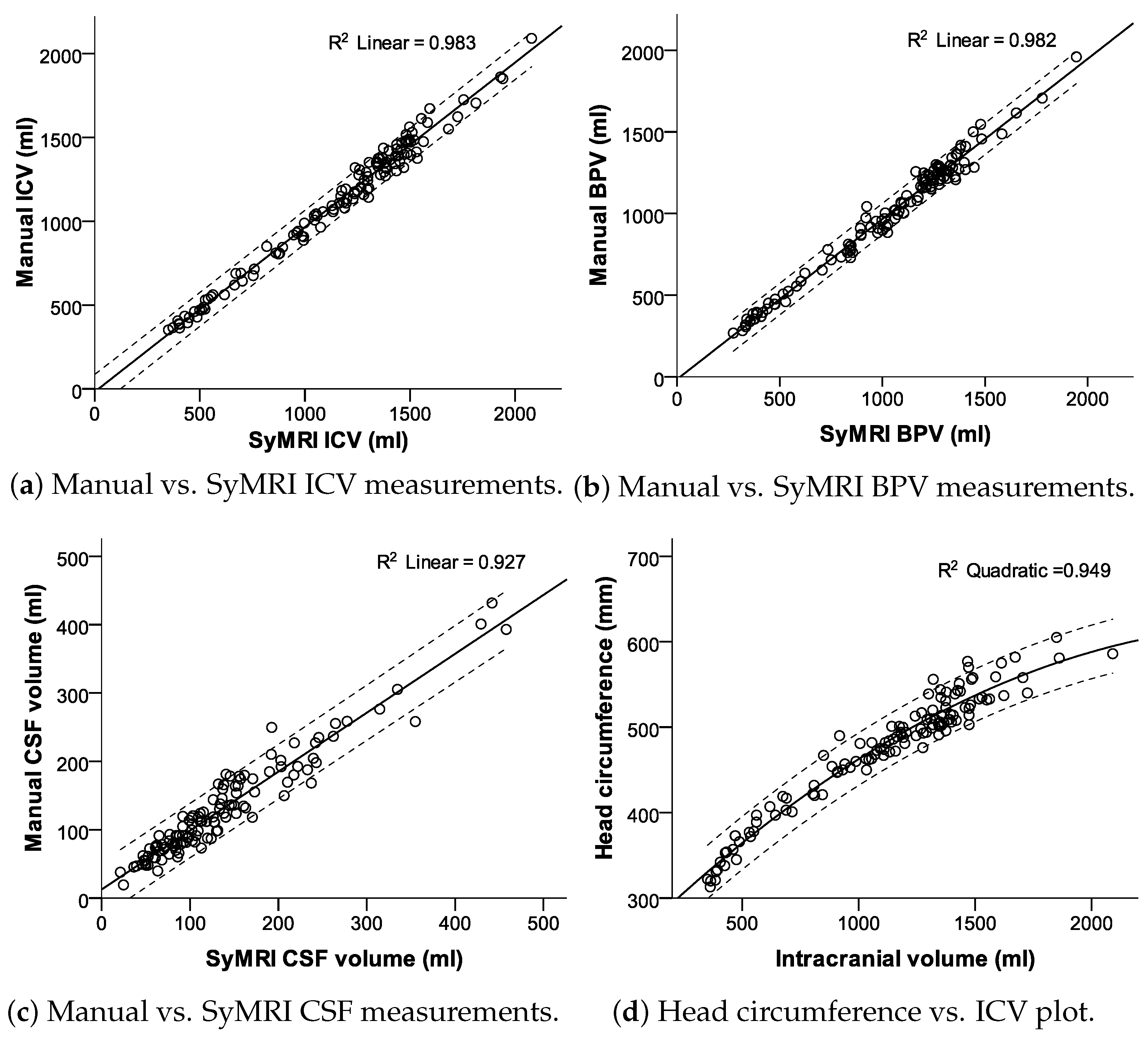
2.6. Statistical Analysis
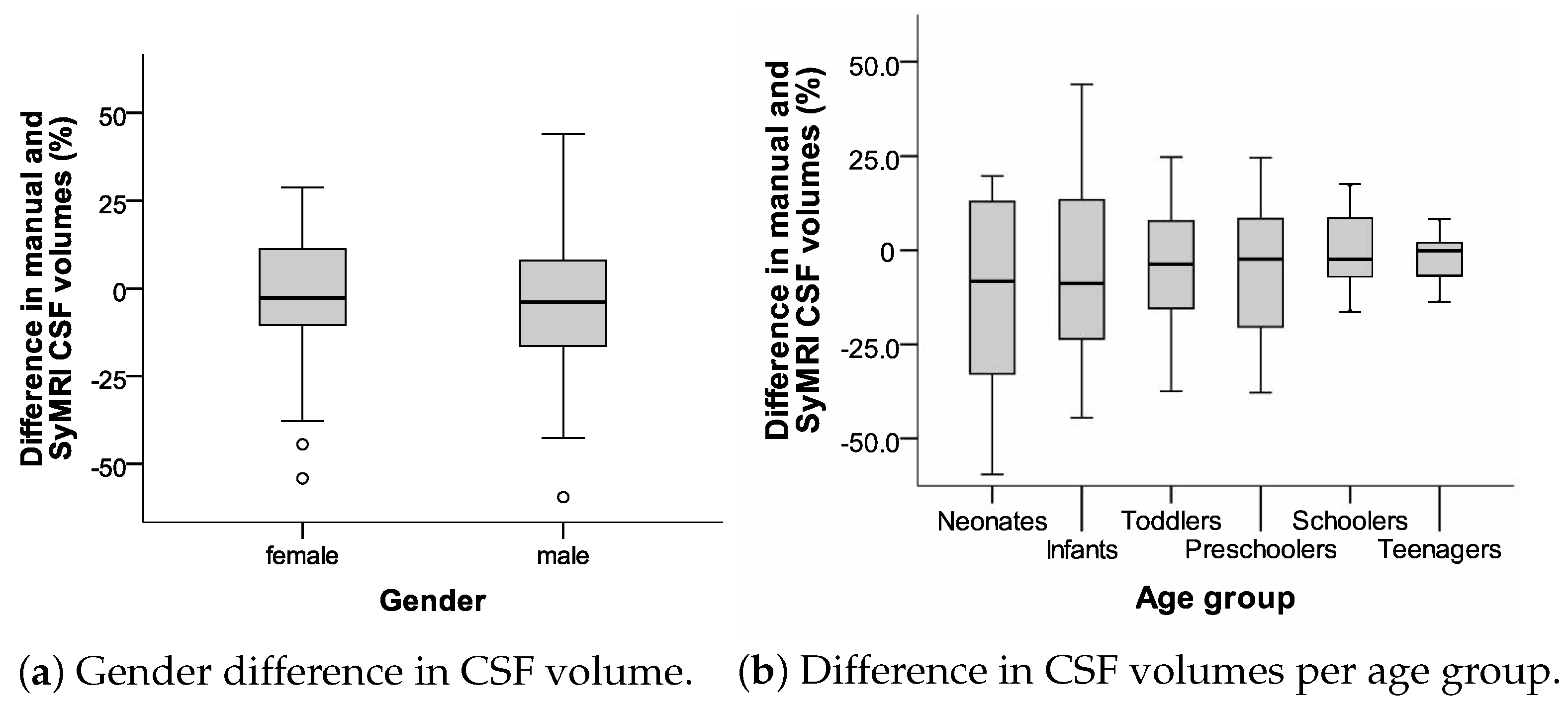
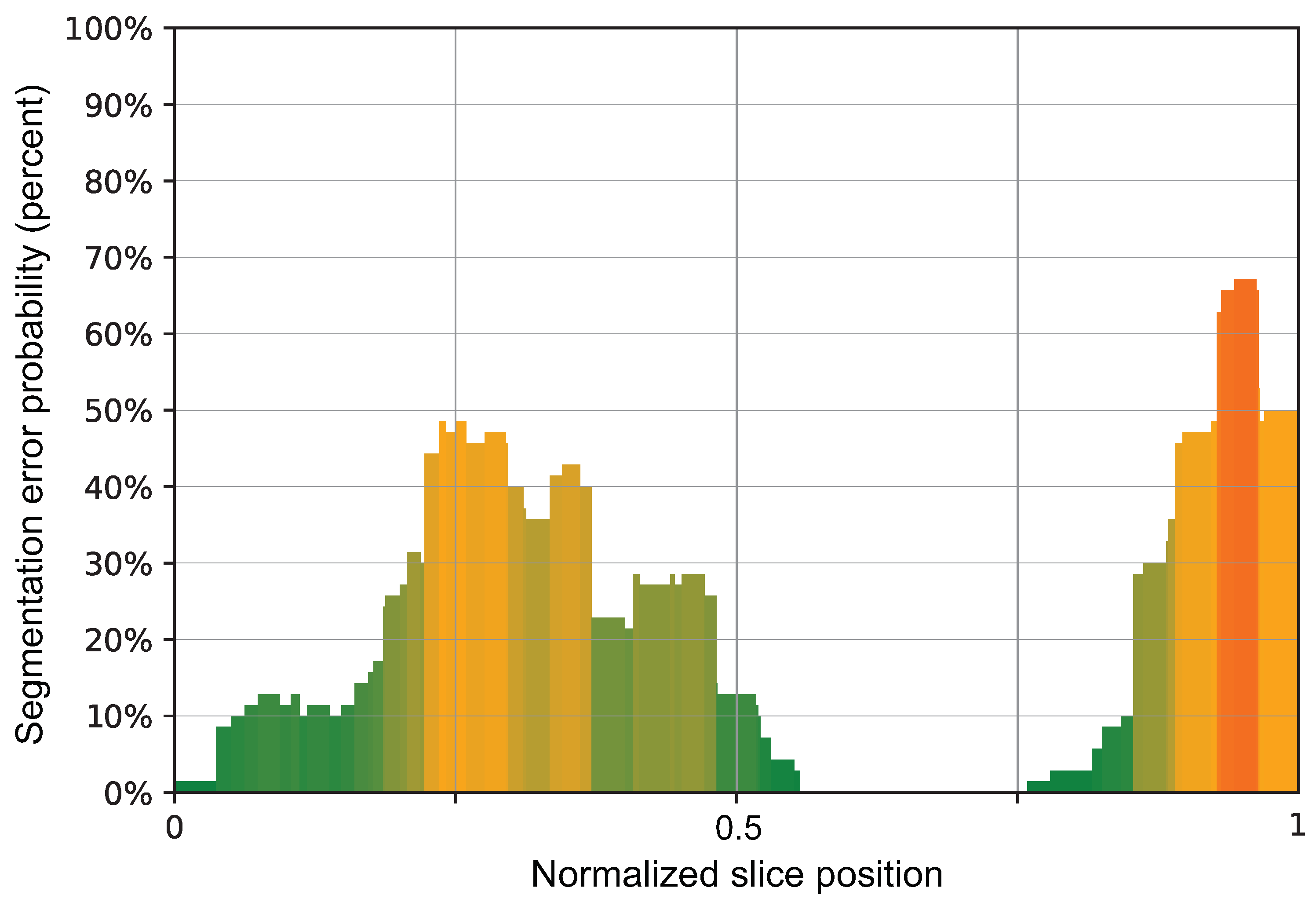
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BPV | Brain parenchyma volume |
| CI | Confidence interval |
| CSF | Cerebrospinal fluid |
| DICOM | Digital Imaging and Communications in Medicine |
| ICV | Intracranial volume |
| MDME | Multi-Dynamic Multi-Echo |
| MRI | Magentic Resonance Imaging |
| NIFTI | Neuroimaging Informatics Technology Initiative |
| PACS | Picture Archiving and Communications System |
References
- Wright, Z.; Larrew, T.W.; Eskandari, R. Pediatric Hydrocephalus: Current State of Diagnosis and Treatment. Pediatr. Rev. 2016, 37, 478–490. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, P.; Raybaud, C.; Palasamudram, S.; Shroff, M. Neuroimaging in pediatric hydrocephalus. Indian J. Pediatr. 2019, 86, 952–960. [Google Scholar] [CrossRef]
- Hagiwara, A.; Warntjes, M.; Hori, M.; Andica, C.; Nakazawa, M.; Kumamaru, K.K.; Abe, O.; Aoki, S. SyMRI of the Brain: Rapid Quantification of Relaxation Rates and Proton Density, with Synthetic MRI, Automatic Brain Segmentation, and Myelin Measurement. Investig. Radiol. 2017, 52, 647–657. [Google Scholar] [CrossRef]
- Serai, S.D.; Dudley, J.; Leach, J.L. Comparison of whole brain segmentation and volume estimation in children and young adults using SPM and SyMRI. Clin. Imaging 2019, 57, 77–82. [Google Scholar] [CrossRef]
- Vanderhasselt, T.; Zolfaghari, R.; Naeyaert, M.; Dudink, J.; Buls, N.; Allemeersch, G.J.; Raeymaekers, H.; Cools, F.; de Mey, J. Synthetic MRI demonstrates prolonged regional relaxation times in the brain of preterm born neonates with severe postnatal morbidity. Neuroimage Clin. 2021, 29, 102544. [Google Scholar] [CrossRef]
- Ryu, K.H.; Baek, H.J.; Moon, J.I.; Choi, B.H.; Park, S.E.; Ha, J.Y.; Jeon, K.N.; Bae, K.; Choi, D.S.; Cho, S.B.; et al. Initial clinical experience of synthetic MRI as a routine neuroimaging protocol in daily practice: A single-center study. J. Neuroradiol. 2020, 47, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Ryu, K.H.; Choi, D.S.; Baek, H.J.; Cho, S.B.; Ha, J.Y.; Kim, T.B.; Hwang, M.J. Clinical feasibility of 1-min ultrafast brain MRI compared with routine brain MRI using synthetic MRI: A single center pilot study. J. Neurol. 2019, 266, 431–439. [Google Scholar] [CrossRef]
- Coban, G.; Gumeler, E.; Parlak, S.; Konuskan, B.; Karakaya, J.; Yalnizoglu, D.; Anlar, B.; Oguz, K.K. Synthetic MRI in children with tuberous sclerosis complex. Insights Imaging 2022, 13, 115. [Google Scholar] [CrossRef] [PubMed]
- Hagiwara, A.; Andica, C.; Hori, M.; Aoki, S. Synthetic MRI showed increased myelin partial volume in the white matter of a patient with Sturge-Weber syndrome. Neuroradiology 2017, 59, 1065–1066. [Google Scholar] [CrossRef]
- Betts, A.M.; Leach, J.L.; Jones, B.V.; Zhang, B.; Serai, S. Brain imaging with synthetic MR in children: Clinical quality assessment. Neuroradiology 2016, 58, 1017–1026. [Google Scholar] [CrossRef]
- West, H.; Leach, J.L.; Jones, B.V.; Care, M.; Radhakrishnan, R.; Merrow, A.C.; Alvarado, E.; Serai, S.D. Clinical validation of synthetic brain MRI in children: Initial experience. Neuroradiology 2017, 59, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.M.; Choi, Y.H.; Cheon, J.E.; Kim, I.O.; Cho, S.H.; Kim, W.H.; Kim, H.J.; Cho, H.H.; You, S.K.; Park, S.H.; et al. Image quality at synthetic brain magnetic resonance imaging in children. Pediatr. Radiol. 2017, 47, 1638–1647. [Google Scholar] [CrossRef] [PubMed]
- Schmidbauer, V.; Geisl, G.; Cardoso Diogo, M.; Jengojan, S.; Perepelov, V.; Weber, M.; Goeral, K.; Lindenlaub, F.; Klebermass-Schrehof, K.; Berger, A.; et al. Validity of SyMRI for Assessment of the Neonatal Brain. Clin. Neuroradiol. 2020, 31, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.; Cho, H.H.; Cho, S.H.; Park, B.; Hong, J.; Shin, K.M.; Hwang, M.J.; You, S.K.; Lee, S.M. Accelerated Synthetic MRI with Deep Learning-Based Reconstruction for Pediatric Neuroimaging. Am. J. Neuroradiol. 2022, 43, 1653–1659. [Google Scholar] [CrossRef]
- Goto, M.; Hagiwara, A.; Kato, A.; Fujita, S.; Hori, M.; Kamagata, K.; Sugano, H.; Arai, H.; Aoki, S.; Abe, O.; et al. Estimation of intracranial volume: A comparative study between synthetic MRI and FSL-brain extraction tool (BET)2. J. Clin. Neurosci. 2020, 79, 178–182. [Google Scholar] [CrossRef]
- Chen, Y.; Su, S.; Dai, Y.; Wen, Z.; Qian, L.; Zhang, H.; Liu, M.; Fan, M.; Chu, J.; Yang, Z. Brain Volumetric Measurements in Children with Attention Deficit Hyperactivity Disorder: A Comparative Study between Synthetic and Conventional Magnetic Resonance Imaging. Front. Neurosci. 2021, 15, 711528. [Google Scholar] [CrossRef]
- Lee, S.M.; Kim, E.; You, S.K.; Cho, H.H.; Hwang, M.J.; Hahm, M.H.; Cho, S.H.; Kim, W.H.; Kim, H.J.; Shin, K.M.; et al. T: Comparison with modified SPM segmentation methods. Neuroradiology 2022, 64, 381–392. [Google Scholar] [CrossRef]
- Vanderhasselt, T.; Naeyaert, M.; Watté, N.; Allemeersch, G.J.; Raeymaeckers, S.; Dudink, J.; de Mey, J.; Raeymaekers, H. Synthetic MRI of Preterm Infants at Term-Equivalent Age: Evaluation of Diagnostic Image Quality and Automated Brain Volume Segmentation. Am. J. Neuroradiol. 2020, 41, 882–888. [Google Scholar] [CrossRef]
- Research Imaging Institute; UTHSCSA; Habes, M. Mango; Research Imaging Institute, UTHSCSA: San Antonio, TX, USA, 2019. [Google Scholar]
- Fischl, B. FreeSurfer. Neuroimage 2012, 62, 774–781. [Google Scholar] [CrossRef]
- Hoopes, A.; Mora, J.S.; Dalca, A.V.; Fischl, B.; Hoffmann, M. SynthStrip: Skull-stripping for any brain image. NeuroImage 2022, 260, 119474. [Google Scholar] [CrossRef]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.M.; Sonka, M.; et al. 3D Slicer as an Image Computing Platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [PubMed]
- IBM (Ed.) IBM SPSS Statistics 21 Algorithms; IBM: Armonk, NY, USA, 2012. [Google Scholar]
- DATAtab Team. DATAtab: Online Statistics Calculator; DATAtab e.U.: Graz, Austria, 2023. [Google Scholar]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Hagiwara, A.; Hori, M.; Yokoyama, K.; Takemura, M.; Andica, C.; Tabata, T.; Kamagata, K.; Suzuki, M.; Kumamaru, K.; Nakazawa, M.; et al. Synthetic MRI in the Detection of Multiple Sclerosis Plaques. Am. J. Neuroradiol. 2017, 38, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Granberg, T.; Uppman, M.; Hashim, F.; Cananau, C.; Nordin, L.E.; Shams, S.; Berglund, J.; Forslin, Y.; Aspelin, P.; Fredrikson, S.; et al. Clinical Feasibility of Synthetic MRI in Multiple Sclerosis: A Diagnostic and Volumetric Validation Study. Am. J. Neuroradiol. 2016, 37, 1023–1029. [Google Scholar] [CrossRef] [PubMed]
- Warntjes, J.; Leinhard, O.D.; West, J.; Lundberg, P. Rapid magnetic resonance quantification on the brain: Optimization for clinical usage. Magn. Reson. Med. 2008, 60, 320–329. [Google Scholar] [CrossRef] [PubMed]
- Hagiwara, A.; Hori, M.; Suzuki, M.; Andica, C.; Nakazawa, M.; Tsuruta, K.; Takano, N.; Sato, S.; Hamasaki, N.; Yoshida, M.; et al. Contrast-enhanced synthetic MRI for the detection of brain metastases. Acta Radiol. Open 2016, 5, 2058460115626757. [Google Scholar] [CrossRef] [PubMed]
- Blystad, I.; Warntjes, J.; Smedby, O.; Landtblom, A.M.; Lundberg, P.; Larsson, E.M. Synthetic Mri of the Brain in a Clinical Setting. Acta Radiol. 2012, 53, 1158–1163. [Google Scholar] [CrossRef]
- Kidokoro, H.; Anderson, P.J.; Doyle, L.W.; Woodward, L.J.; Neil, J.J.; Inder, T.E. Brain Injury and Altered Brain Growth in Preterm Infants: Predictors and Prognosis. Pediatrics 2014, 134, e444–e453. [Google Scholar] [CrossRef] [PubMed]
- Keunen, K.; Išgum, I.; van Kooij, B.J.; Anbeek, P.; van Haastert, I.C.; Koopman-Esseboom, C.; Fieret-van Stam, P.C.; Nievelstein, R.A.; Viergever, M.A.; de Vries, L.S.; et al. Brain Volumes at Term-Equivalent Age in Preterm Infants: Imaging Biomarkers for Neurodevelopmental Outcome through Early School Age. J. Pediatr. 2016, 172, 88–95. [Google Scholar] [CrossRef]
- Gui, L.; Loukas, S.; Lazeyras, F.; Hüppi, P.; Meskaldji, D.; Borradori Tolsa, C. Longitudinal study of neonatal brain tissue volumes in preterm infants and their ability to predict neurodevelopmental outcome. NeuroImage 2019, 185, 728–741. [Google Scholar] [CrossRef]
- Abreu, N.J.; Selvaraj, B.; Truxal, K.V.; Moore-Clingenpeel, M.; Zumberge, N.A.; McNally, K.A.; McBride, K.L.; Ho, M.L.; Flanigan, K.M. Longitudinal MRI brain volume changes over one year in children with mucopolysaccharidosis types IIIA and IIIB. Mol. Genet. Metab. 2021, 133, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Al Kaissi, A.; Ryabykh, S.; Chehida, F.B.; Al Kaissi, H.; Kircher, S.G.; Grill, F.; Guben, A. Meticulous and Early Understanding of Congenital Cranial Defects Can Save Lives. Children 2023, 10, 1240. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Age (Years) | Weight (kg) | Body Size (m) | BMI |
|---|---|---|---|---|
| Cases (n) | 124 | 124 | 124 | 124 |
| Minimum | 0.0 | 1.8 | 0.4 | 8.6 |
| Maximum | 18.1 | 79.0 | 1.7 | 29.7 |
| 25th percentile | 0.89 | 7.45 | 0.69 | 14.26 |
| Median | 2.75 | 14.00 | 0.93 | 16.00 |
| 75th percentile | 5.36 | 22.38 | 1.19 | 18.52 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weiss, V.; Vishwanathan, N.; Dutschke, A.; Stranger, N.; Scherkl, M.; Nagy, E.; Ciornei-Hoffman, A.; Tschauner, S. Reliability of Automated Intracranial Volume Measurements by Synthetic Brain MRI in Children. Appl. Sci. 2024, 14, 4751. https://doi.org/10.3390/app14114751
Weiss V, Vishwanathan N, Dutschke A, Stranger N, Scherkl M, Nagy E, Ciornei-Hoffman A, Tschauner S. Reliability of Automated Intracranial Volume Measurements by Synthetic Brain MRI in Children. Applied Sciences. 2024; 14(11):4751. https://doi.org/10.3390/app14114751
Chicago/Turabian StyleWeiss, Veronika, Nathan Vishwanathan, Anja Dutschke, Nikolaus Stranger, Mario Scherkl, Eszter Nagy, Andreea Ciornei-Hoffman, and Sebastian Tschauner. 2024. "Reliability of Automated Intracranial Volume Measurements by Synthetic Brain MRI in Children" Applied Sciences 14, no. 11: 4751. https://doi.org/10.3390/app14114751
APA StyleWeiss, V., Vishwanathan, N., Dutschke, A., Stranger, N., Scherkl, M., Nagy, E., Ciornei-Hoffman, A., & Tschauner, S. (2024). Reliability of Automated Intracranial Volume Measurements by Synthetic Brain MRI in Children. Applied Sciences, 14(11), 4751. https://doi.org/10.3390/app14114751