
The Influence of Late Gadolinium Enhancement Cardiac Magnetic Resonance Image Analysis Imprecision on Myocardial Damage Quantification in Patients with Myocarditis: A Pilot Study


Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Imaging Protocol
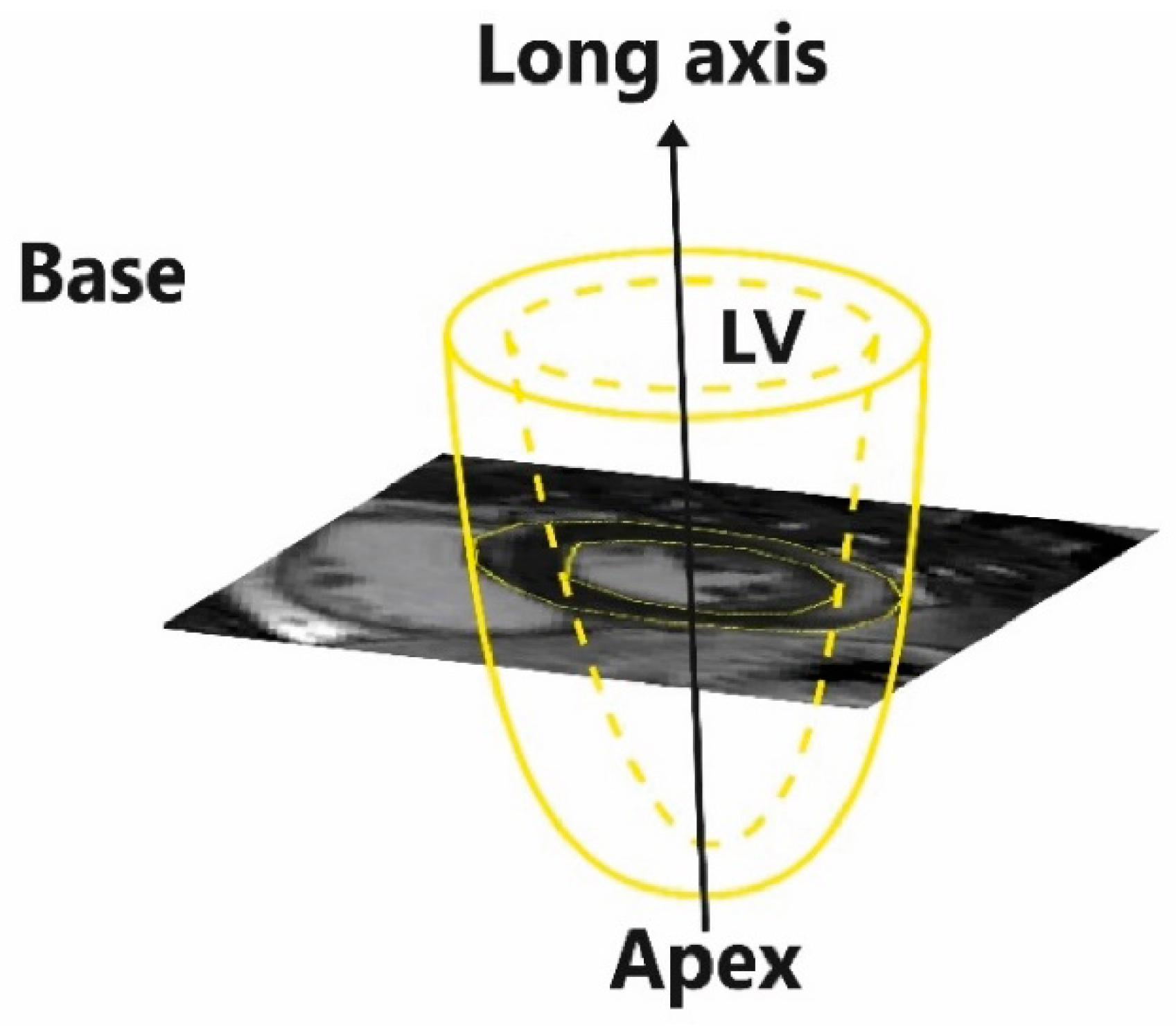
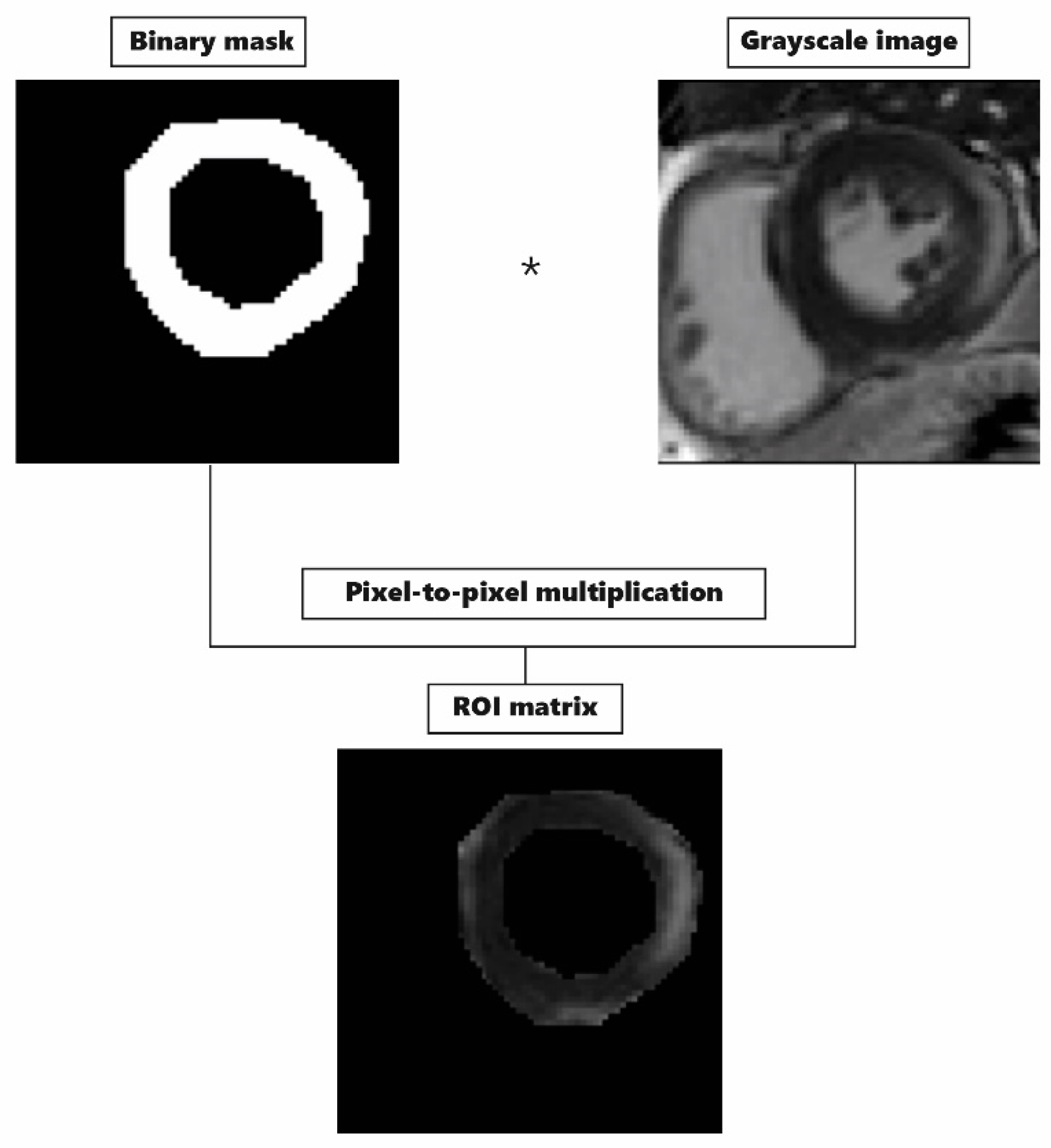
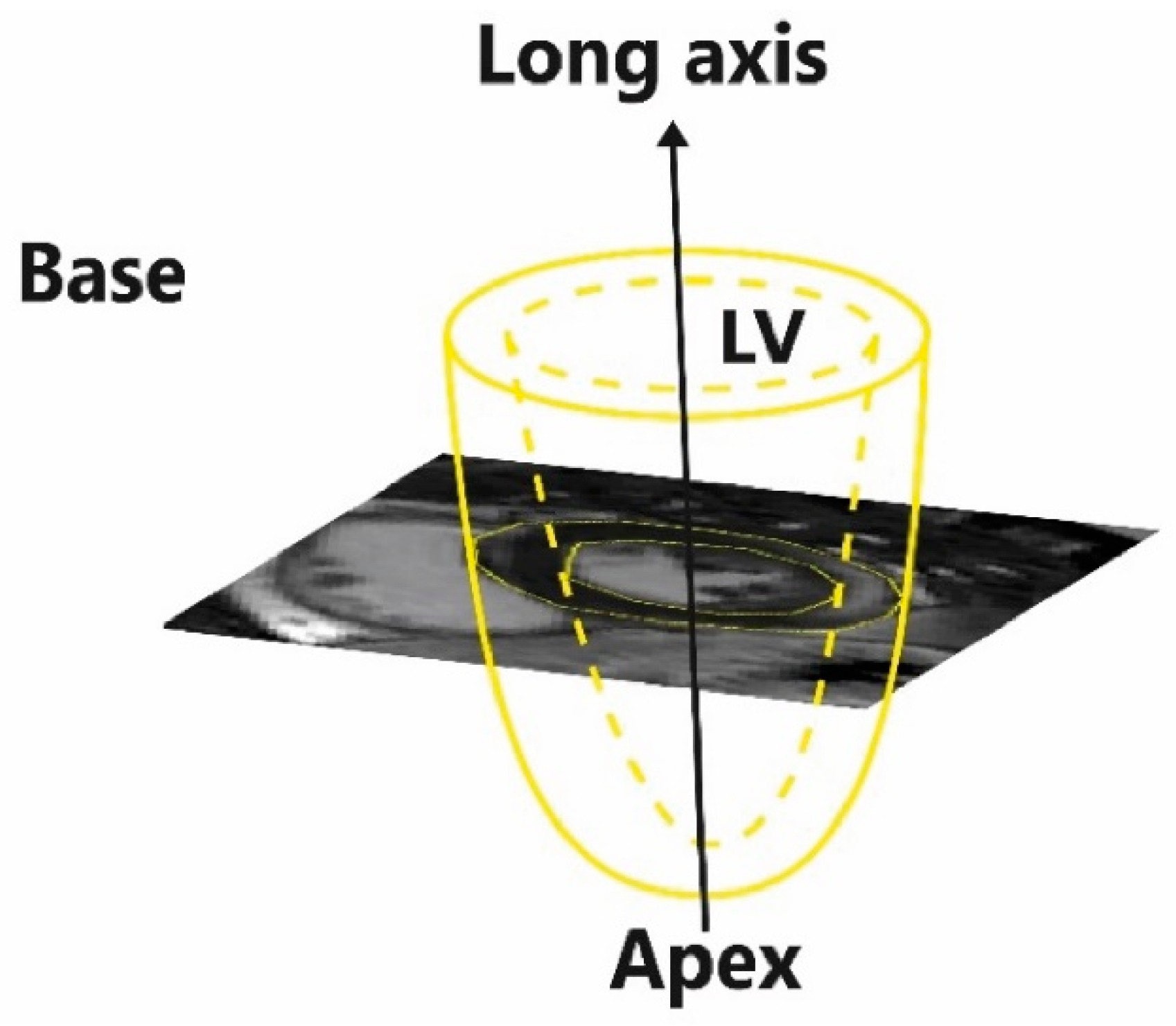
2.2. Image Segmentation Steps
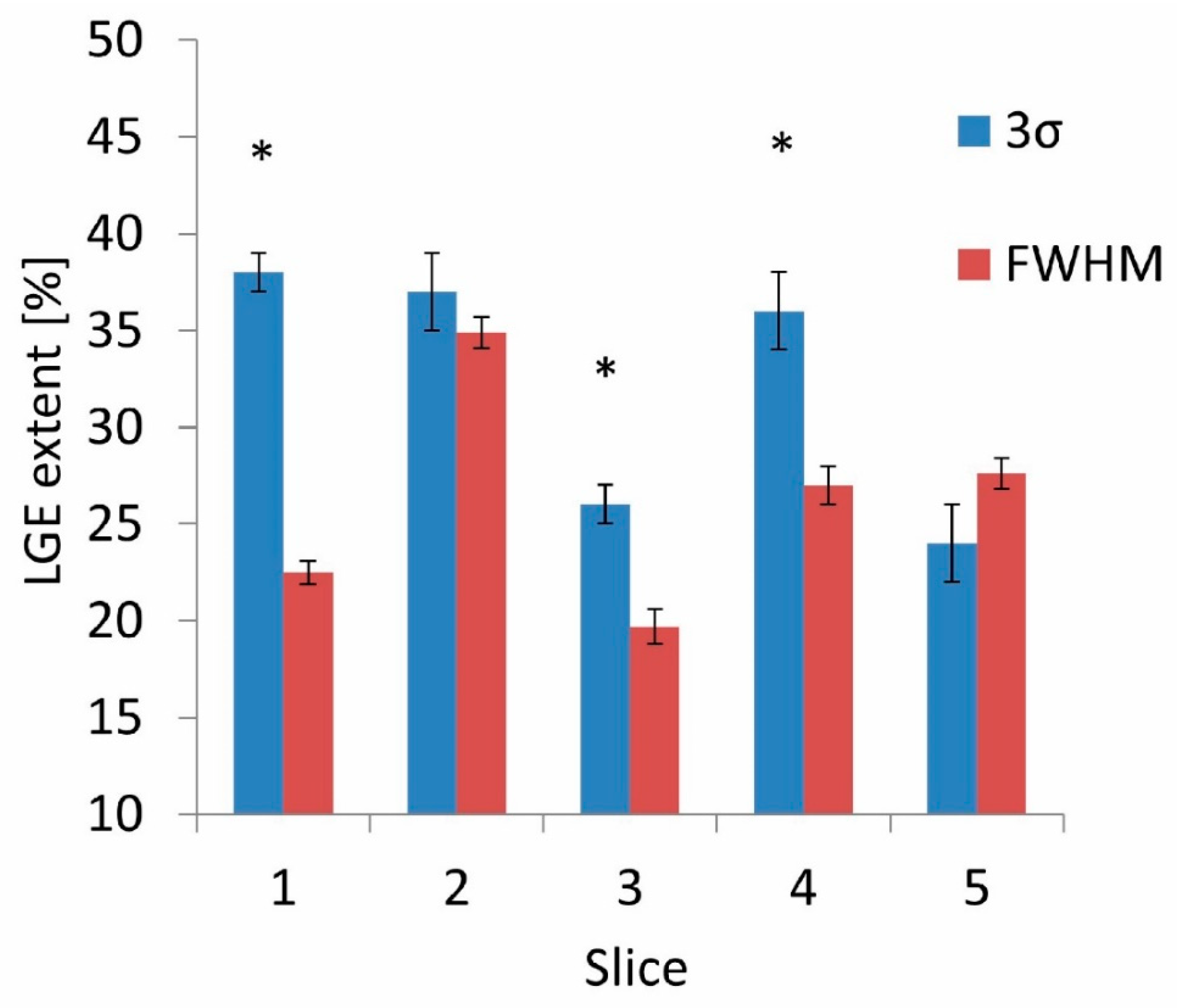
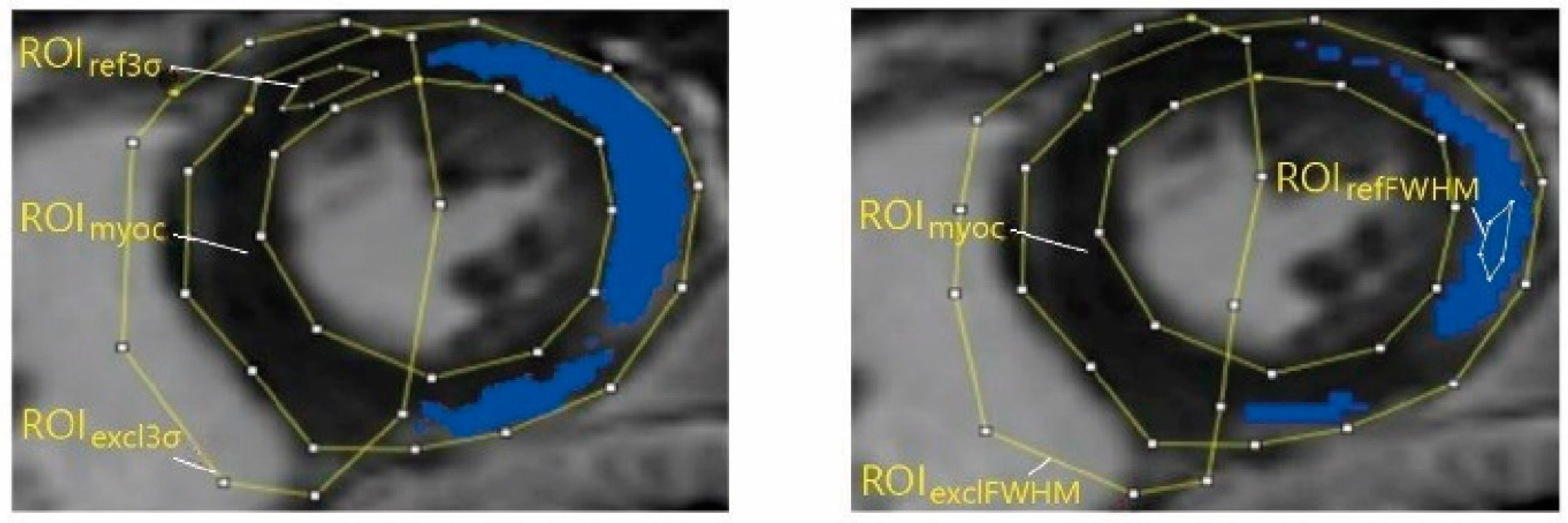
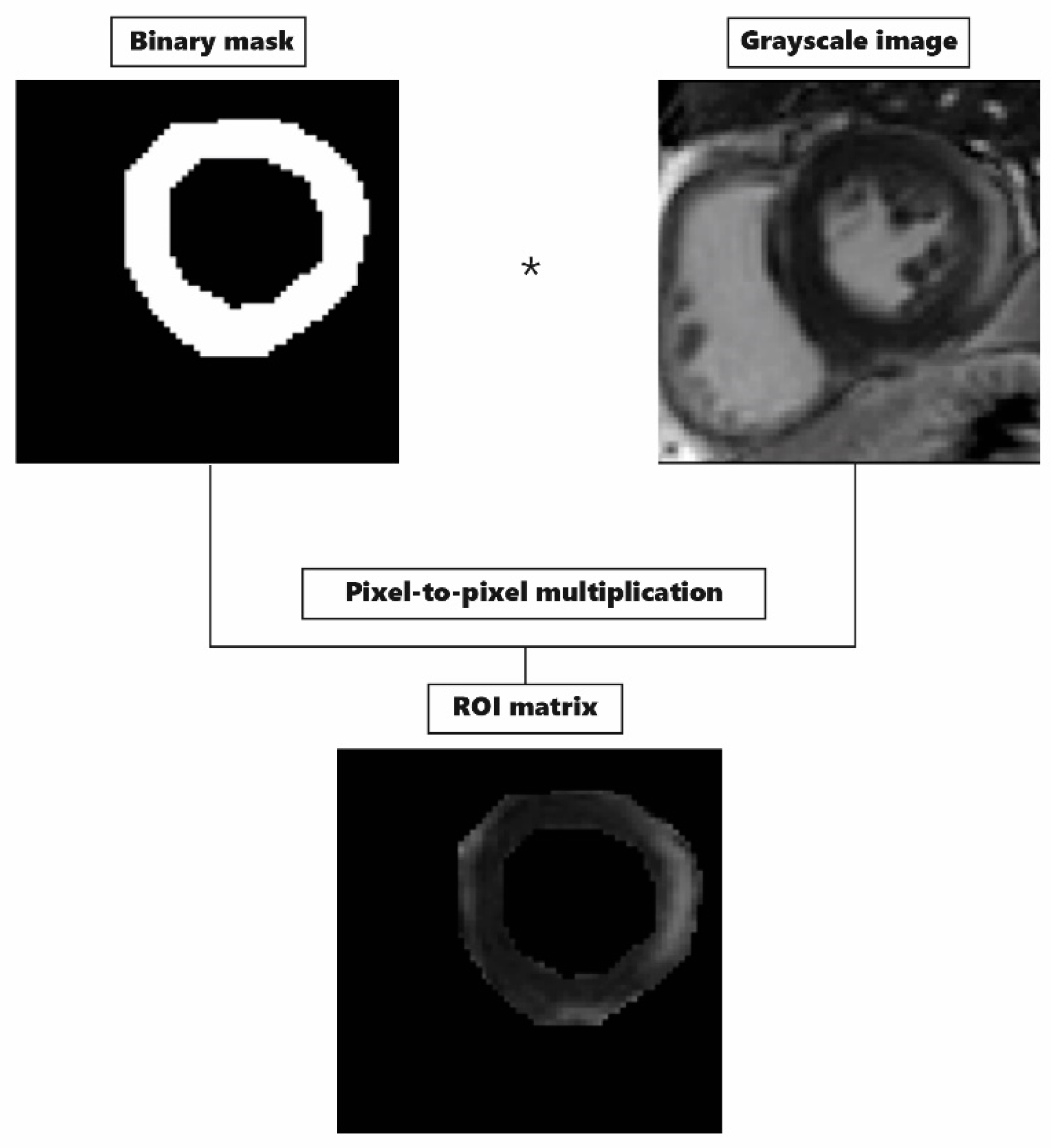
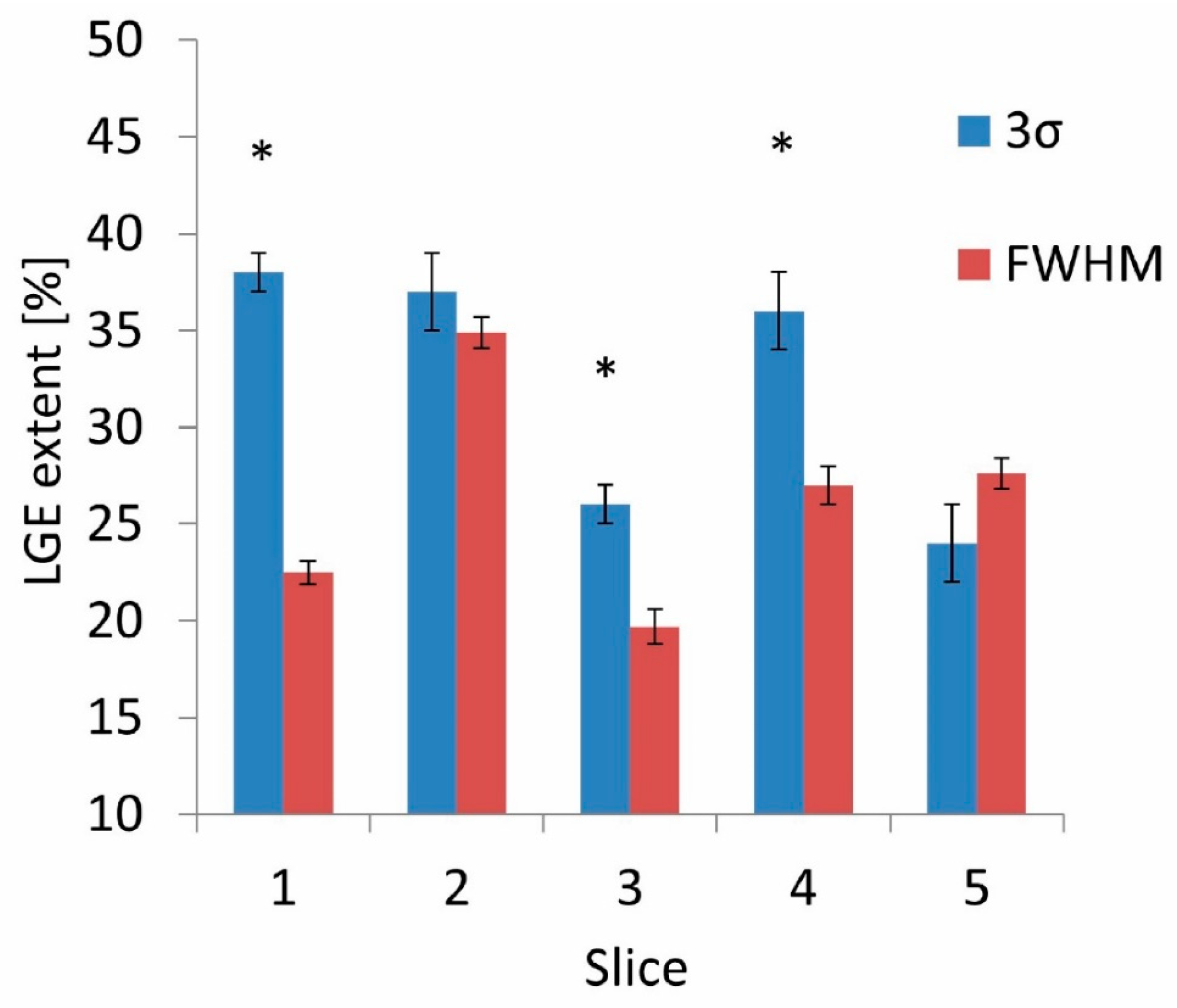
2.3. LGE Quantification
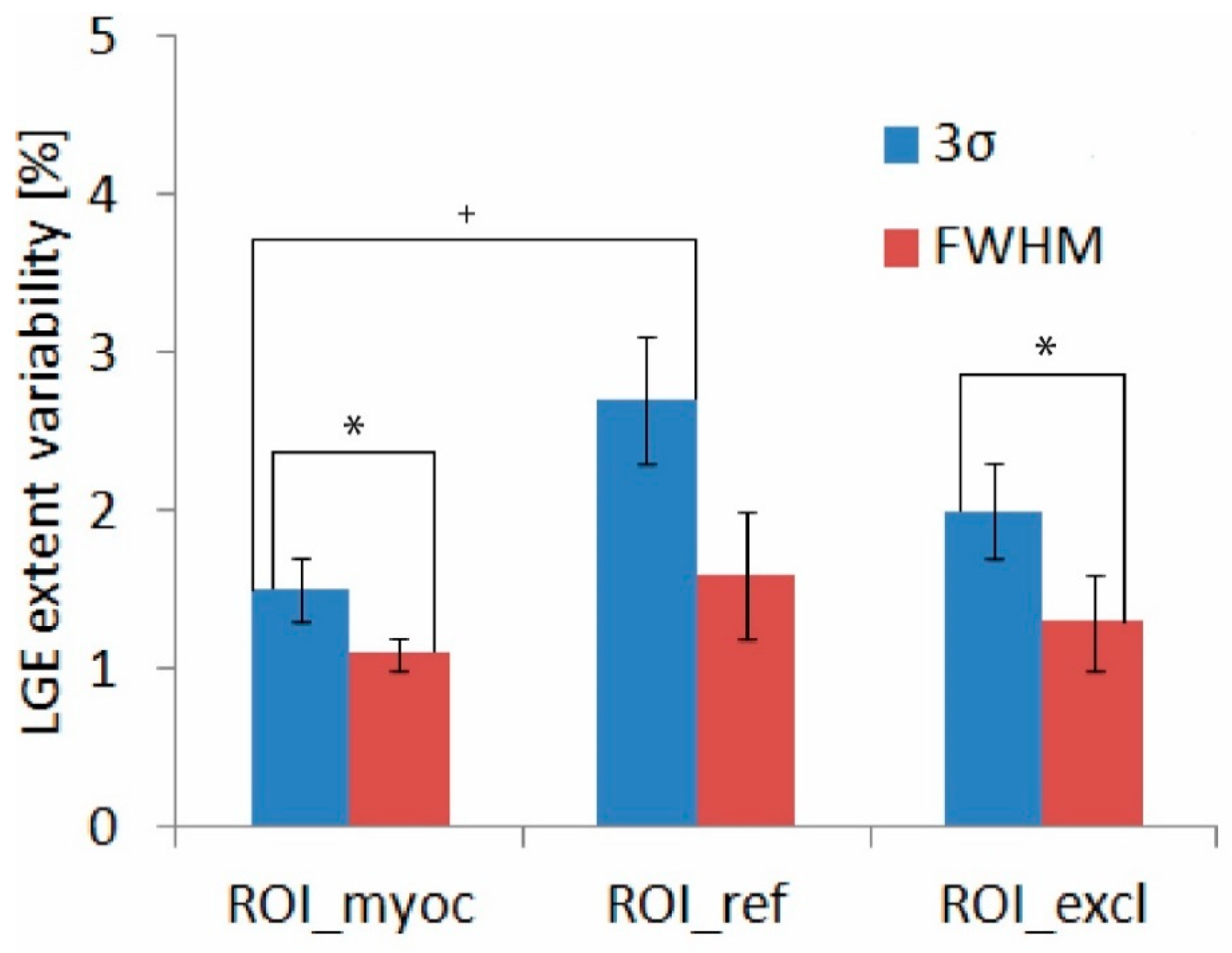
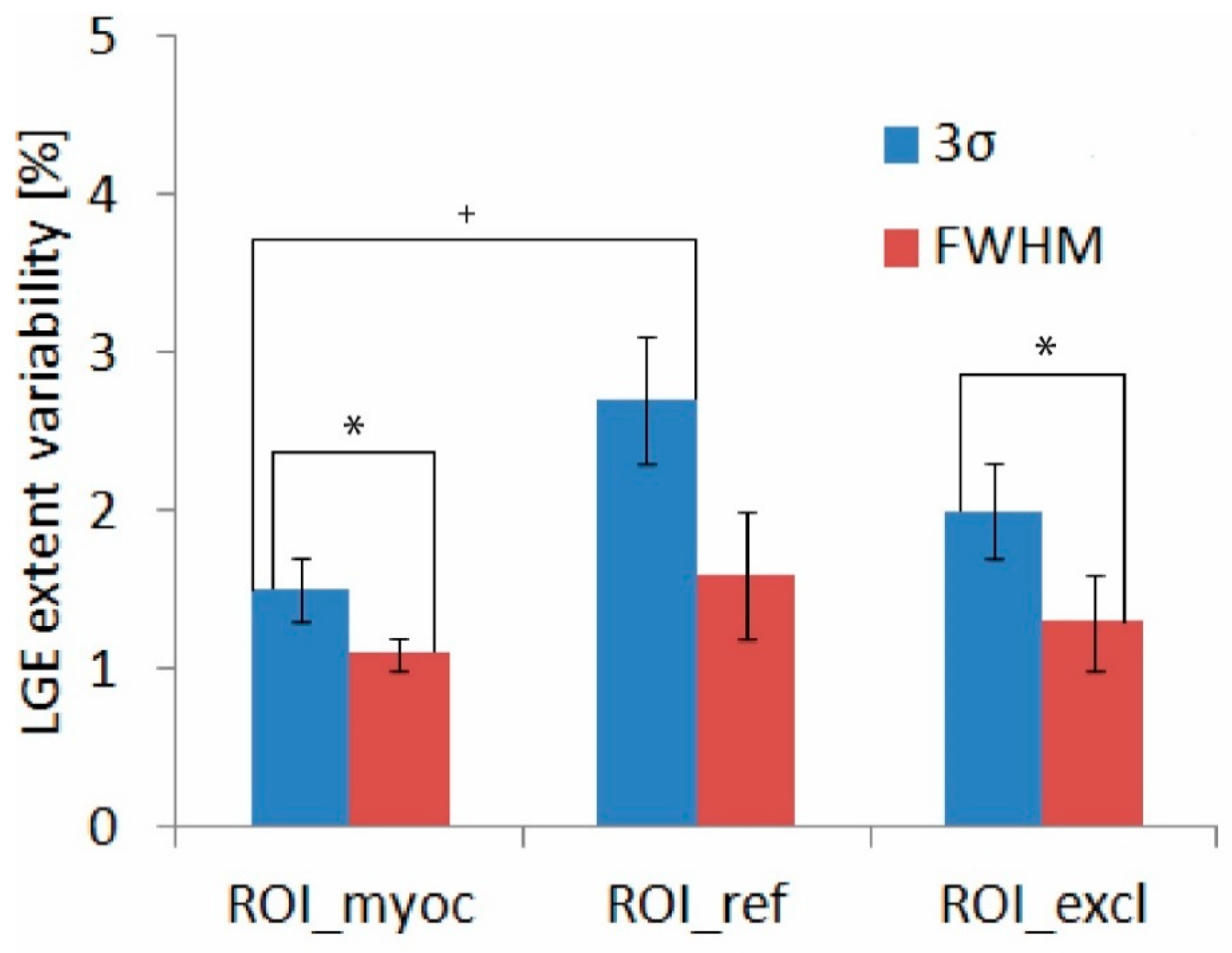
2.4. LGE Extent Reference and Variability
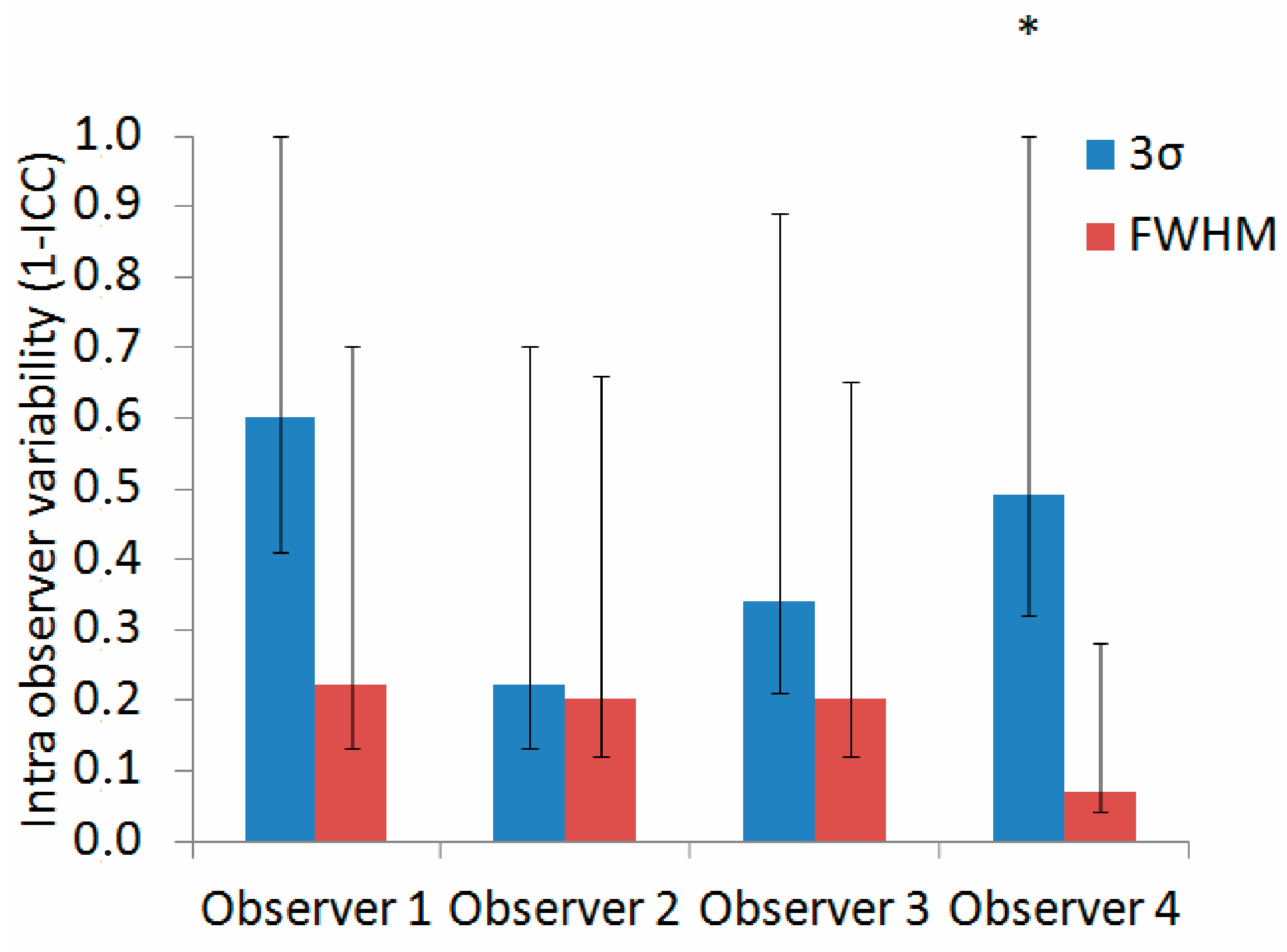
2.5. Inter- and Intraobserver Variability
2.6. Statistical Analysis
3. Results
4. Discussion
5. Limitations and Future Perspectives
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Caforio, A.L.P.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Heliö, T.; Heymans, S.; Jahns, R.; et al. Current State of Knowledge on Aetiology, Diagnosis, Management, and Therapy of Myocarditis: A Position Statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2013, 34, 2636–2648. [Google Scholar] [CrossRef] [PubMed]
- Mahrholdt, H.; Greulich, S. Prognosis in Myocarditis: Better Late Than (N)Ever! J. Am. Coll. Cardiol. 2017, 70, 1988–1990. [Google Scholar] [CrossRef] [PubMed]
- Imbriaco, M.; Nappi, C.; Puglia, M.; de Giorgi, M.; Dell’Aversana, S.; Cuocolo, R.; Ponsiglione, A.; de Giorgi, I.; Polito, M.V.; Klain, M.; et al. Assessment of Acute Myocarditis by Cardiac Magnetic Resonance Imaging: Comparison of Qualitative and Quantitative Analysis Methods. J. Nucl. Cardiol. 2019, 26, 857–865. [Google Scholar] [CrossRef] [PubMed]
- Ammirati, E.; Buono, A.; Moroni, F.; Gigli, L.; Power, J.R.; Ciabatti, M.; Garascia, A.; Adler, E.D.; Pieroni, M. State-of-the-Art of Endomyocardial Biopsy on Acute Myocarditis and Chronic Inflammatory Cardiomyopathy. Curr. Cardiol. Rep. 2022, 24, 597–609. [Google Scholar] [CrossRef]
- Urzua Fresno, C.; Sanchez Tijmes, F.; Shaw, K.E.; Huang, F.; Thavendiranathan, P.; Khullar, S.; Seidman, M.A.; Hanneman, K. Cardiac Imaging in Myocarditis: Current Evidence and Future Directions. Can. Assoc. Radiol. J. 2023, 74, 147–159. [Google Scholar] [CrossRef]
- Gräni, C.; Eichhorn, C.; Bière, L.; Kaneko, K.; Murthy, V.L.; Agarwal, V.; Aghayev, A.; Steigner, M.; Blankstein, R.; Jerosch-Herold, M.; et al. Comparison of Myocardial Fibrosis Quantification Methods by Cardiovascular Magnetic Resonance Imaging for Risk Stratification of Patients with Suspected Myocarditis. J. Cardiovasc. Magn. Reson. 2019, 21, 14. [Google Scholar] [CrossRef]
- Haaf, P.; Garg, P.; Messroghli, D.R.; Broadbent, D.A.; Greenwood, J.P.; Plein, S. Cardiac T1 Mapping and Extracellular Volume (ECV) in Clinical Practice: A Comprehensive Review. J. Cardiovasc. Magn. Reson. 2016, 18, 89. [Google Scholar] [CrossRef]
- Van Der Geest, R.J.; Reiber, J.H.C. Quantification in Cardiac MRI. J. Magn. Reson. Imaging 1999, 10, 602–608. [Google Scholar] [CrossRef]
- Kellman, P.; Arai, A.E. Cardiac Imaging Techniques for Physicians: Late Enhancement. J. Magn. Reson. Imaging 2012, 36, 529–542. [Google Scholar] [CrossRef]
- Flett, A.S.; Hasleton, J.; Cook, C.; Hausenloy, D.; Quarta, G.; Ariti, C.; Muthurangu, V.; Moon, J.C. Evaluation of Techniques for the Quantification of Myocardial Scar of Differing Etiology Using Cardiac Magnetic Resonance. JACC Cardiovasc. Imaging 2011, 4, 150–156. [Google Scholar] [CrossRef]
- McAlindon, E.; Pufulete, M.; Lawton, C.; Angelini, G.D.; Bucciarelli-Ducci, C. Quantification of Infarct Size and Myocardium at Risk: Evaluation of Different Techniques and Its Implications. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 738–746. [Google Scholar] [CrossRef] [PubMed]
- Flett, A.S.; Hasleton, J.M.; Quarta, G.; Hausenloy, D.; Muthurangu, V.; Moon, J.C. The Full Width Half Maximum Technique Is Superior for LGE Quantification Regardless of Its Aetiology. J. Cardiovasc. Magn. Reson. 2010, 12, O41. [Google Scholar] [CrossRef]
- Kellman, P.; Arai, A.E.; McVeigh, E.R.; Aletras, A.H. Phase-Sensitive Inversion Recovery for Detecting Myocardial Infarction Using Gadolinium-Delayed Hyperenhancement. Magn. Reson. Med. 2002, 47, 372–383. [Google Scholar] [CrossRef] [PubMed]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an Image Computing Platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [PubMed]
- Ku, H.H. Notes on the Use of Propagation of Error Formulas. J. Res. Natl. Bur. Stand. Sect. C Eng. Instrum. 1966, 70, 263. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Liljequist, D.; Elfving, B.; Roaldsen, K.S. Intraclass Correlation—A Discussion and Demonstration of Basic Features. PLoS ONE 2019, 14, e0219854. [Google Scholar] [CrossRef]
- Giuseppe Via San Lorenzo, P. StaTips Part IV: Selection, Interpretation and Reporting of the Intraclass Correlation Coefficient. South Eur. J. Orthod. Dentofac. Res. 2018, 5, 3–5. [Google Scholar] [CrossRef]
- Bonett, D.G. Sample Size Requirements for Estimating Intraclass Correlations with Desired Precision. Stat. Med. 2002, 21, 1331–1335. [Google Scholar] [CrossRef]
- Ghasemi, A.; Zahediasl, S. Normality Tests for Statistical Analysis: A Guide for Non-Statisticians. Int. J. Endocrinol. Metab. 2012, 10, 486–489. [Google Scholar] [CrossRef]
- Xu, M.; Fralick, D.; Zheng, J.Z.; Wang, B.; Tu, X.M.; Feng, C. The Differences and Similarities between Two-Sample t-Test and Paired t-Test. Shanghai Arch. Psychiatry 2017, 29, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Ngo, T.A.; Lu, Z.; Carneiro, G. Combining Deep Learning and Level Set for the Automated Segmentation of the Left Ventricle of the Heart from Cardiac Cine Magnetic Resonance. Med. Image Anal. 2017, 35, 159–171. [Google Scholar] [CrossRef] [PubMed]
- Alabed, S.; Alandejani, F.; Dwivedi, K.; Karunasaagarar, K.; Sharkey, M.; Garg, P.; de Koning, P.J.H.; Tóth, A.; Shahin, Y.; Johns, C.; et al. Validation of Artificial Intelligence Cardiac MRI Measurements: Relationship to Heart Catheterization and Mortality Prediction. Radiology 2022, 305, 68–79. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Qin, C.; Qiu, H.; Tarroni, G.; Duan, J.; Bai, W.; Rueckert, D. Deep Learning for Cardiac Image Segmentation: A Review. Front. Cardiovasc. Med. 2020, 7, 25. [Google Scholar] [CrossRef]
- Gossuin, Y.; Aline, H.; Gillis, P.; Vuong Quoc, L.; Yves, G.; Pierre, G.; Quoc Lam, V. Physics of Magnetic Resonance Imaging: From Spin to Pixel Physics of Magnetic Resonance Imaging: From Spin to Pixel Physics of Magnetic Resonance Imaging: From Spin to Pixel. J. Phys. D Appl. Phys. 2010, 43, 213001. [Google Scholar] [CrossRef]
- Ridgway, J.P. Cardiovascular Magnetic Resonance Physics for Clinicians: Part I. J. Cardiovasc. Magn. Reson. 2010, 12, 71. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample (n = 5) | |
|---|---|
| Male/female | 5/0 |
| Age (mean ± standard error) (y) | 30 ± 5 |
| BMI (mean ± standard error) (kg/m2) | 29 ± 2 |
| Mean LGE extent (mean ± standard error) (%) | 24 ± 5 |
| Maximum troponin (mean ± standard error) (ng/L) | 18,564 ± 5000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kralj, L.; Cerne Cercek, A.; Gomišček Novak, A.; Kirn, B. The Influence of Late Gadolinium Enhancement Cardiac Magnetic Resonance Image Analysis Imprecision on Myocardial Damage Quantification in Patients with Myocarditis: A Pilot Study. Appl. Sci. 2024, 14, 117. https://doi.org/10.3390/app14010117
Kralj L, Cerne Cercek A, Gomišček Novak A, Kirn B. The Influence of Late Gadolinium Enhancement Cardiac Magnetic Resonance Image Analysis Imprecision on Myocardial Damage Quantification in Patients with Myocarditis: A Pilot Study. Applied Sciences. 2024; 14(1):117. https://doi.org/10.3390/app14010117
Chicago/Turabian StyleKralj, Lana, Andreja Cerne Cercek, Alja Gomišček Novak, and Borut Kirn. 2024. "The Influence of Late Gadolinium Enhancement Cardiac Magnetic Resonance Image Analysis Imprecision on Myocardial Damage Quantification in Patients with Myocarditis: A Pilot Study" Applied Sciences 14, no. 1: 117. https://doi.org/10.3390/app14010117
APA StyleKralj, L., Cerne Cercek, A., Gomišček Novak, A., & Kirn, B. (2024). The Influence of Late Gadolinium Enhancement Cardiac Magnetic Resonance Image Analysis Imprecision on Myocardial Damage Quantification in Patients with Myocarditis: A Pilot Study. Applied Sciences, 14(1), 117. https://doi.org/10.3390/app14010117