
Applications of Deep Learning to Neurodevelopment in Pediatric Imaging: Achievements and Challenges


Abstract
:1. Introduction
2. Methods
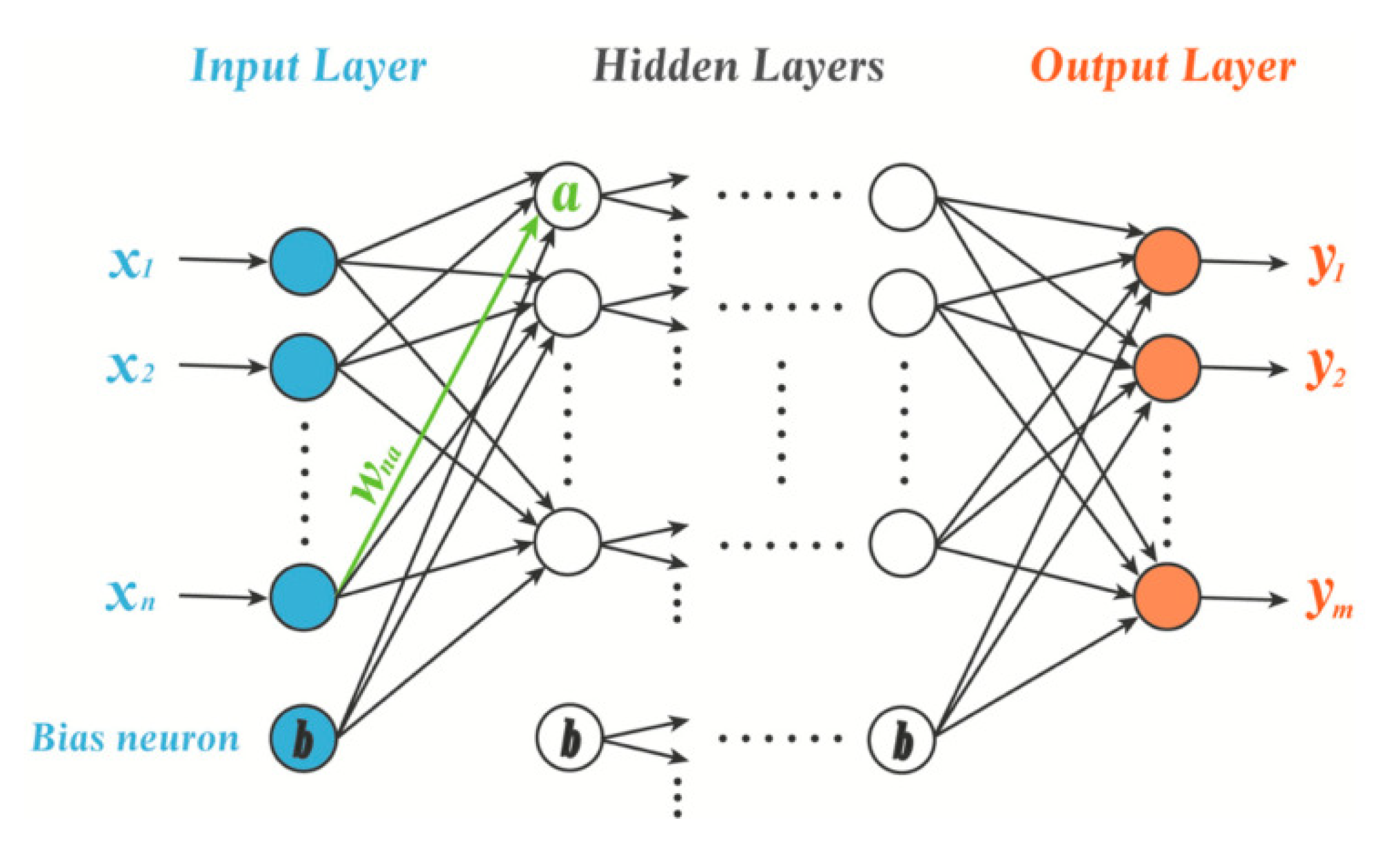
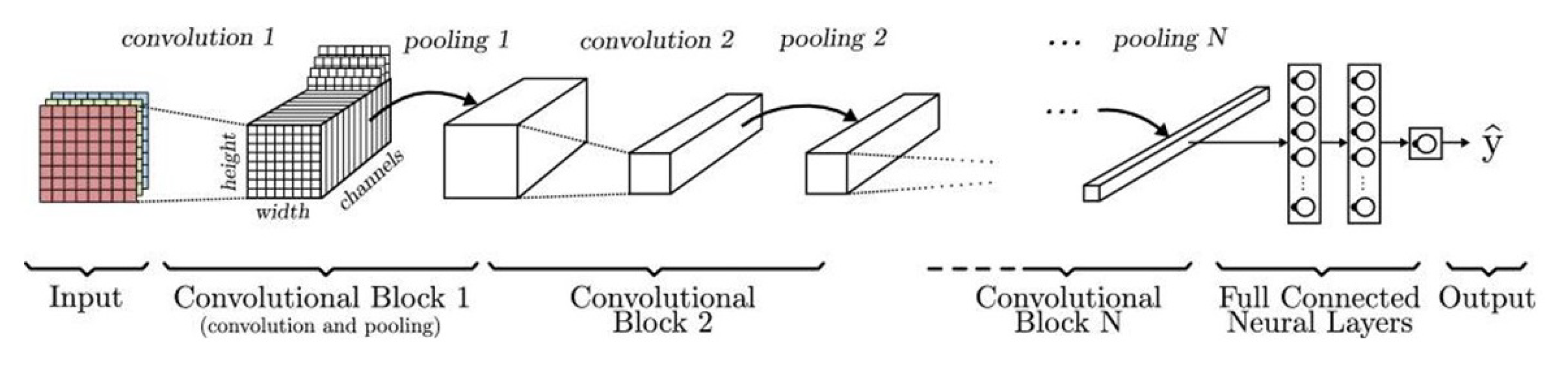
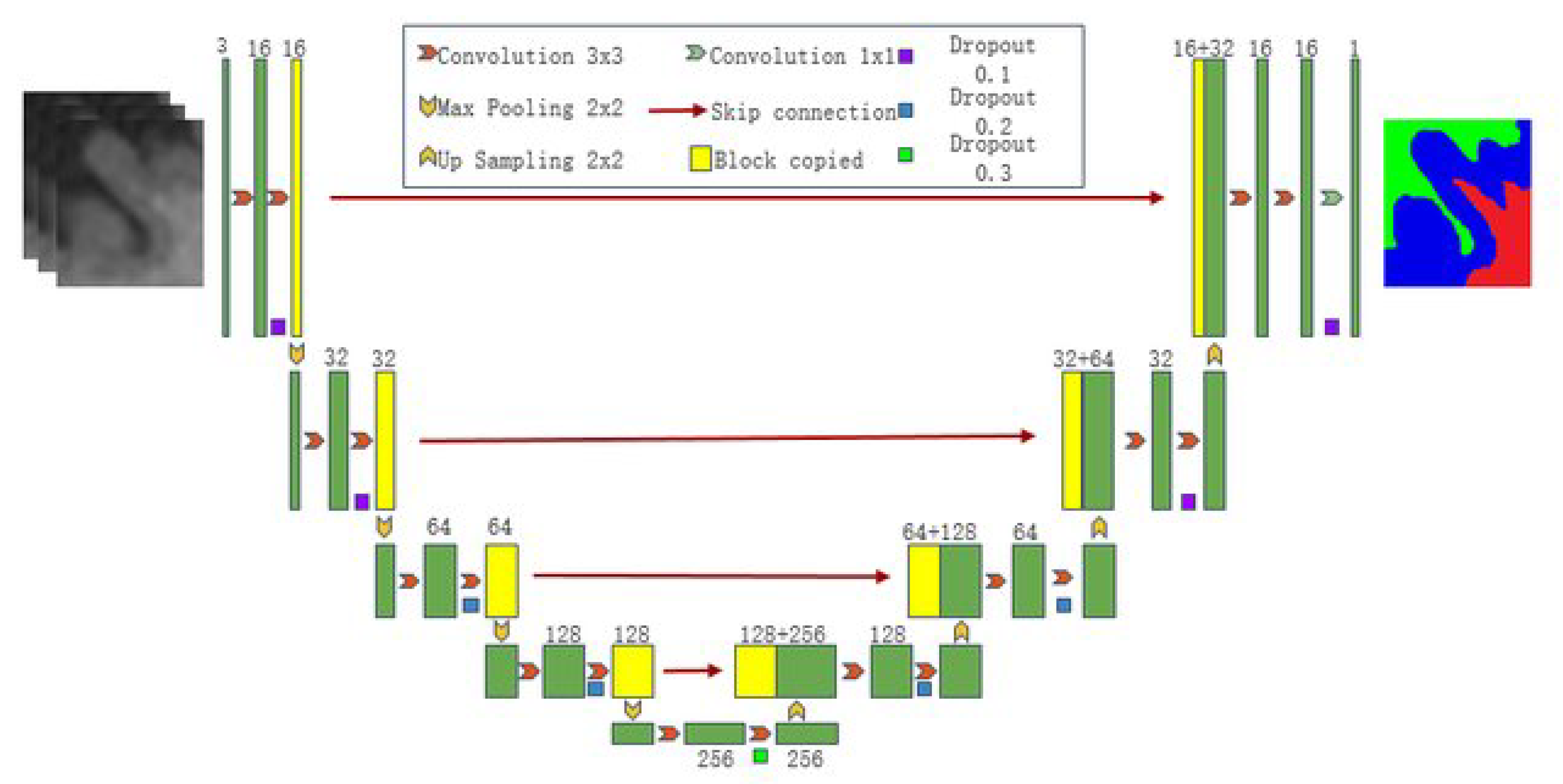
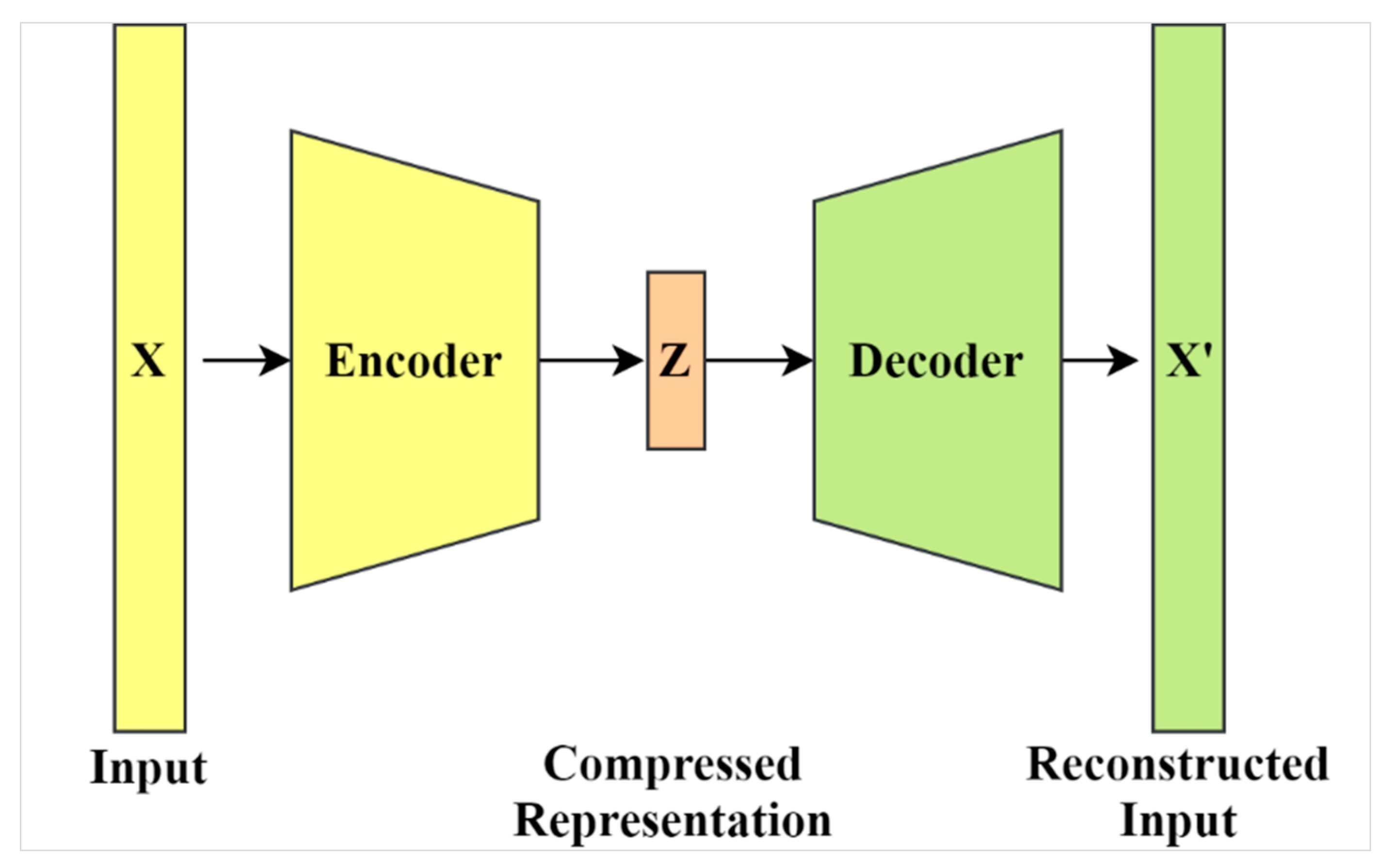
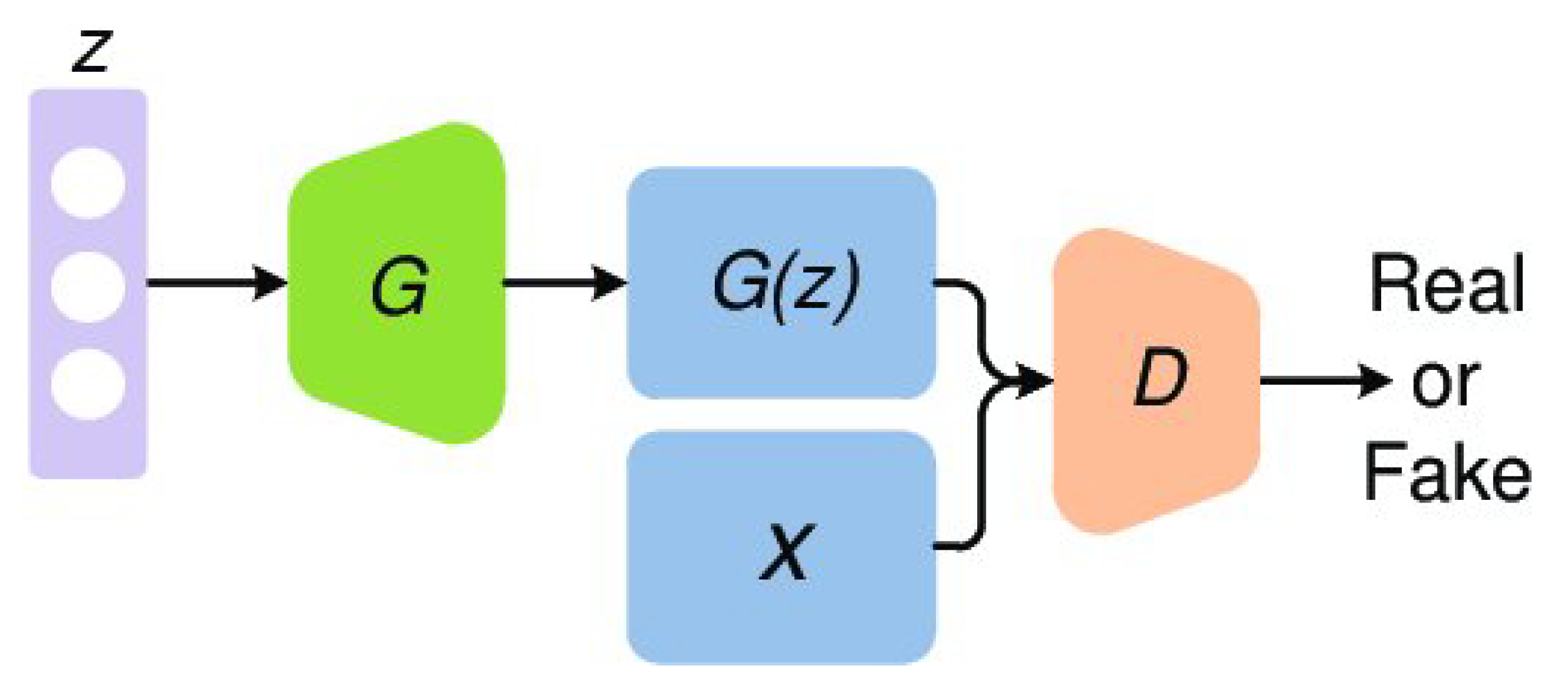
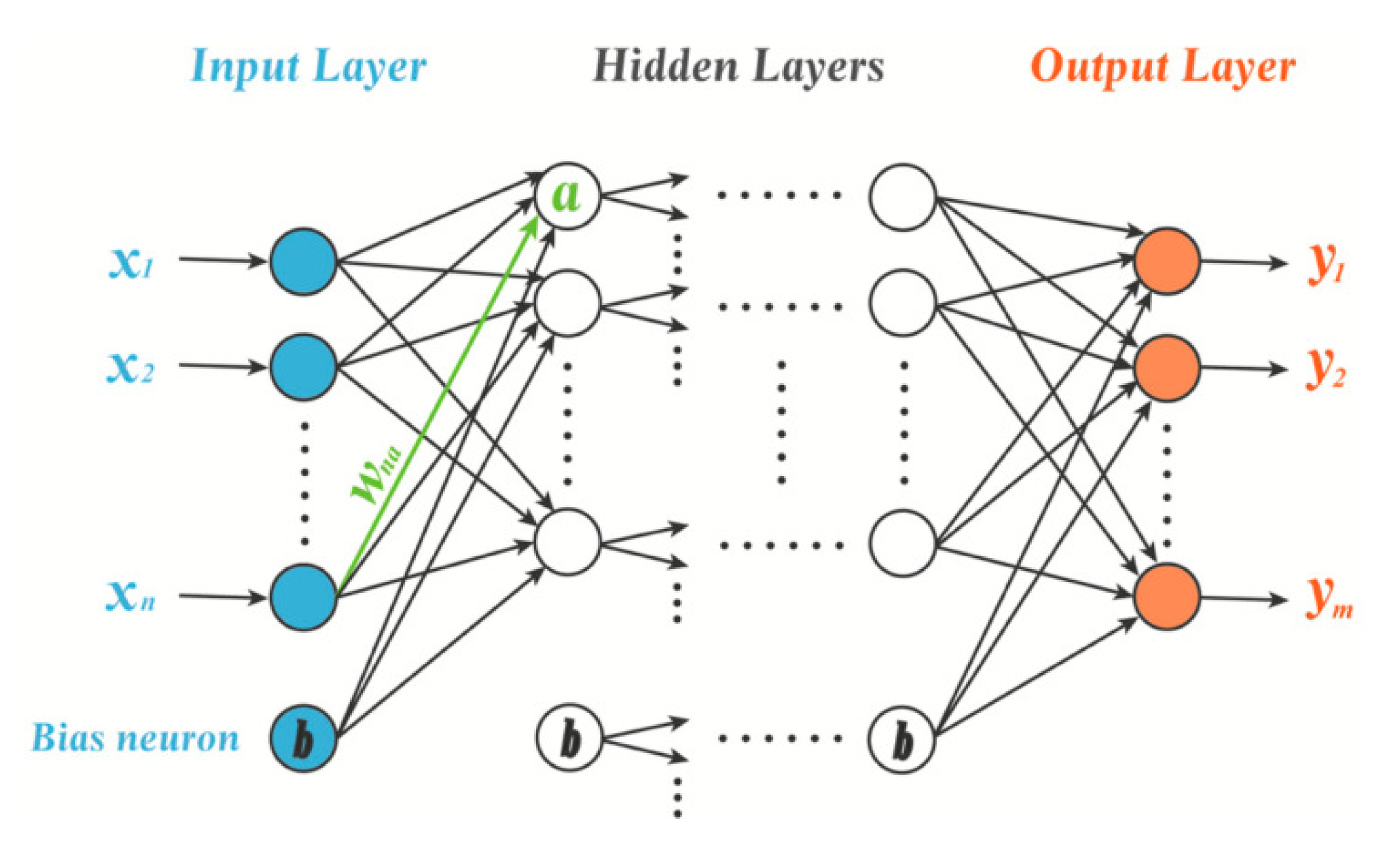
2.1. Deep Learning Model Architectures
2.2. Public Datasets and Repositories
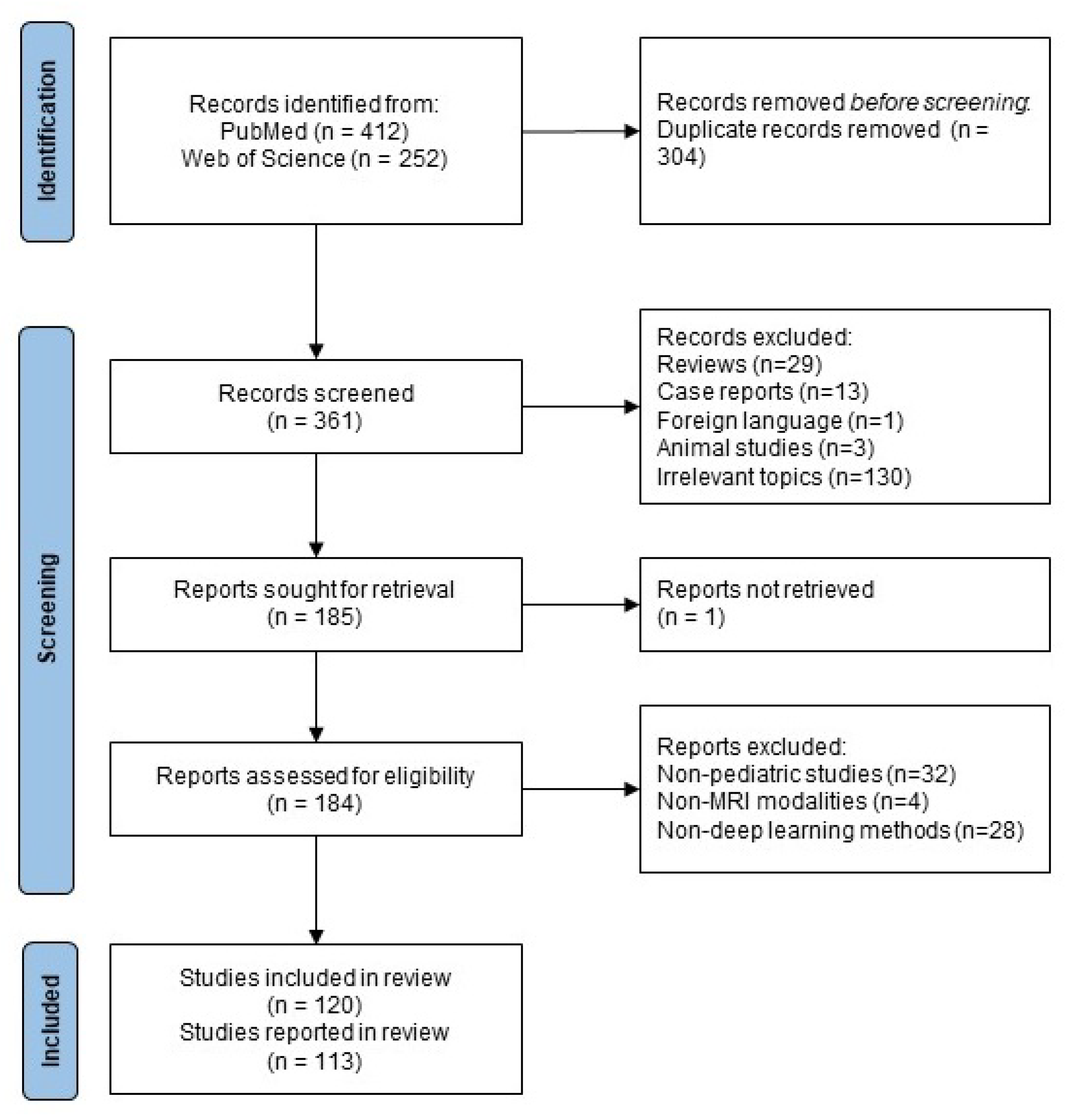
2.3. Review Parameters
3. Results
3.1. Recognizing Neurodevelopmental Disorders

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Disorder | Population | Technique | Preprocessing | Method | Results |
|---|---|---|---|---|---|---|---|
| [79] | 2017 | Autism | ABIDE I dataset 55 ASD (age 14.2 ± 3.2 years) 55 HC (age 12.7 ± 2.4 years) | rs-fMRI | Preprocessed Connectomes Project | MLP | Accuracy 86.36% |
| [80] | 2018 | Autism | 62 ASD 48 HC | task fMRI | FSL | MLP | Accuracy 87.1% |
| [51] | 2018 | Autism | ABIDE I dataset 529 ASD 571 HC | rs-fMRI | In-house pipeline | RNN | Accuracy 70.1% |
| [81] | 2018 | Autism | ABIDE I & II dataset 116 ASD 69 HC (age 5–10 years) | sMRI, rs-fMRI | SPM8 | Deep Belief Network | Accuracy 65.56% |
| [53] | 2019 | Autism | ABIDE I & II dataset 210 ASD 249 HC (age 5–10 years) | rs-fMRI | SPM8 | CNN | Accuracy 72.73% |
| [52] | 2019 | Autism | ABIDE II dataset 117 ASD 81 HC (age 5–12 years) | rs-fMRI | FSL | Auto-encoder | Accuracy 96.26% |
| [55] | 2020 | Autism | multi datasets: ABCD, ABIDE I, II, BioBank, NDAR, ICBM, Open fMRI, 1000 Functional Connectomes 43,838 total connectomes 1711 ASD (age 0.42–78 years) | rs-fMRI, task-fMRI | SPT, AFNI, SpeddyPP | CNN | AUROC 0.6774 |
| [82] | 2020 | Autism | YUM dataset 40 ASD (age 29.4 ± 11.6 years) 33 HC (age 30.1 ± 5.3 years) ABIDE I dataset 521 ASD (age 29.4 ± 11.6 years) 593 HC (age 30.1 ± 5.3 years) | sMRI | SPM8 | 3D CNN | Accuracy 88% (YUM) 64% (ABIDE) |
| [69] | 2021 | Autism | ABIDE I dataset 55 ASD (age 14.52 ± 6.97 years) 55 HC (age 15.81 ± 6.25 years) | rs-fMRI | Configurable Pipeline for the Analysis of Connectomes | 3D CNN | Accuracy 77.74% |
| [74] | 2021 | Autism | 50 ASD 50 HC (age 12–40 months) | task-fMRI | FSL, FEAT | 3D CNN | Accuracy 80% |
| [83] | 2021 | Autism | ABIDE I & II dataset 1060 ASD 1146 HC (age 5–64 years) | rs-fMRI | In-house pipeline | CNN | Accuracy 89.5% |
| [84] | 2021 | Autism | ABIDE I dataset 506 ASD 532 HC (age 10–28 years) | rs-fMRI | DPABI | MLP | Accuracy 78.07 ± 4.38% |
| [85] | 2021 | Autism | 52 ASD 195 HC infants (age 24 months) | MRI | iBEAT | CNN | Accuracy 92% |
| [76] | 2021 | Autism | multi datasets: ABCD, ABIDE I, II, BioBank, NDAR, Open fMRI 29,288 total connectomes 1555 ASD (age 0.42–78 years) | sMRI, rs-fMRI, task-fMRI | AFNI, SpeddyPP | CNN | AUROC 0.7354 |
| [54] | 2022 | Autism | ABIDE & UM dataset 411 HC for offline learning 48 ASD 65 HC for testing (age 13.8 ± 2 years) | rs-fMRI | Connectome Computation System | Auto-encoder | Accuracy 67.2% |
| [73] | 2022 | Autism | Preschool dataset 110 subjects ABIDE I dataset 1099 subjects | sMRI | SPM8 | CNN | AUROC 0.787 (preschool) 0.856 (ABIDE) |
| [86] | 2022 | Autism | 151 ASD 151 HC (age 1–6 years) | sMRI | In-house pipeline | 3D CNN | Accuracy 84.4% |
| [75] | 2022 | Autism | IMPAC dataset 418 ASD 497 hc (age 17 ± 9.6 years) | sMRI, rs-fMRI | In-house pipeline | MLP | AUROC 0.79 ± 0.01 |
| [87] | 2019 | ADHD | ADHD-200 consortium 776 subjects | rs-fMRI | In-house pipeline | 3D CNN | Accuracy 69.01% |
| [88] | 2020 | ADHD | ADHD-200 consortium 262 subjects | rs-fMRI | AFNI, FSL | CNN | Accuracy 73.1% |
| [78] | 2021 | ADHD | ENIGMA-ADHD Working Group 2192 ADHD 1850 HC (age 4–63 years) | sMRI | FreeSurfer | MLP | Testing AUROC 0.60 |
| [89] | 2022 | ADHD | ADHD-200 consortium NI site25 ADHD 23 HC (age 11–22 years) NYU site: 118 ADHD 98 HC (age 7–18 years) KKI site: 22 ADHD 61 HC (age 8–13 years) PU site: 78 ADHD 116 HC (age 8–17 years) PU-1 site: 24 ADHD 62 HC (age 8–17 years) | rs-fMRI | Preprocessed Connectomes Project | Auto-encoder | Accuracy >99% |
| [90] | 2022 | ADHD | ADHD-200 consortium NI site: 28 ADHD-I 37 HC NYU site: 72 ADHD-I, 42 ADHD-C, 96 HC OHSU site: 27 ADHD-I, 13 ADHD-C, 70 HC KKI site: 16 ADHD-I, 5 ADHD-C 60 HC PU-1 site: 16 ADHD-I, 26 ADHD-C, 88 HC PU-2 site: 15 ADHD-I, 20 ADHD-C, 31 HC PU-3 site: 7 ADHD-I, 12 ADHD-C, 23 HC | rs-fMRI | DPABI | CNN | Accuracy >99% |
| [91] | 2022 | ADHD | ADHD-200 consortium Training: 69 ADHD 99HC Testing: 24 ADHD 27 HC (age 7–21 years | rs-fMRI | Athena pipeline | CNN | Testing accuracy 67% |
| [77] | 2022 | ADHD | ADHD-200 consortium 325 ADHD 547 HC (age 12 ± 3.0 years) | rs-fMRI | Athena pipeline | CNN | Accuracy 78.7 ± 4.3% |
| [92] | 2022 | ADHD | 19 ADHD (age 10.25 ± 1.94 years) 20 HC (age 10.15 ± 2.13 years) | sMRI | SPM | CNN | Accuracy 93.45 ± 1.18% |
| [93] | 2022 | ADHD | ABCD Dataset 127 ADHD 127 HC (age 9–10 years) | sMRI | ANTs | CNN | Accuracy 71.1% |
| [57] | 2018 | Cerebellar Dysplasia | 90 patients, 40 HC | sMRI | FSL, ANTs | 3D CNN | Accuracy 98.5 ± 2.41% |
| [61] | 2020 | Conduct Disorder | 60 patients (age 15.3 ± 1.0 years) 60 HC (age 15.5 ± 0.7 years) | sMRI | - | 3D CNN | Accuracy 85% |
| [62] | 2021 | Disruptive Behavior Disorder | ABCD Study: 550 patients, 550 HC (age 9–11 years) | sMRI, rs-fMRI, DTI | FSL | 3D CNN | Accuracy 72% |
| [58] | 2020 | Dyslexic | 36 patients, 19 HC (age 9–12 years) | task fMRI | SPM | 3D CNN | Accuracy 72.73% |
| [94] | 2020 | Embryonic Neurodevelopmental Disorders | 114 patients, 113 HC (age 16–39 weeks) | sMRI | — | CNN | Accuracy 87.7% |
| [59] | 2020 | Epilepsy | 30 patients, 13 HC | sMRI | BET | CNN | Accuracy 66–73% |
| [60] | 2020 | Epilepsy | 59 patients, 70 HC (age 7–18 years) | DTI | SPM | CNN | Accuracy 90.75% |
| [70] | 2021 | Neonatal Hyperbilirubinemia | 47patients, 32 HC (age 1–18 days) | sMRI | CNN | Accuracy 72.15% | |
| [63] | 2021 | PTSD | 33 patients (age 14.3 ± 3.3 years) 53 HC (age 15.0 ± 2.3 years) | rs-fMRI | SPM12 | MLP | Accuracy 72% |
| [64] | 2020 | Tuber | 260 patients, 260 HC | sMRI | FSL | 3D CNN | Accuracy 97.1% |
| [65] | 2022 | Tuber | 296 patients, 245 HC (age 0–8 years) | sMRI | - | 3D CNN | Accuracy 86% |
| [71] | 2020 | Tuber | 114 patients (age 5–15.3 years), 114 HC (age 6.9–15.7 years) | sMRI | In-house pipeline | CNN | Accuracy 95% |
| [95] | 2021 | Tumor | 136 patients, 22 HC (age 0–11 years) | sMRI | SPM | CNN | Accuracy 87 ± 2% |
| [72] | 2020 | Tumor | 617 patients with tumor (age 0.2–34 years) | sMRI | Pydicom | CNN | Accuracy 72% |
| [66] | 2018 | Tumor | 233 subjects | sMRI | - | Capsule Network | Accuracy 86.56% |
| [96] | 2020 | Tumor | 39 pediatric patients | sMRI | - | CNN | Accuracy 87.8% |
| [67] | 2020 | White Matter Pathways | 89 patients with focal epilepsy (age 9.95 ± 5.41 years) | DTI | FreeSurfer | CNN | Accuracy 98% |
| [68] | 2019 | White Matter Pathways | 70 HC (age 12.01 ± 4.80 years), 70 patients with focal epilepsy (age 11.60 ± 4.80 years) | DTI | FreeSurfer, FSL, NIH TORTOISE | CNN | F1 score 0.9525 ± 0.0053 |
3.2. Identifying Brain and Tissue Structures
| Study | Year | Structure | Population | Technique | Preprocessing | Method | Results |
|---|---|---|---|---|---|---|---|
| [104] | 2020 | Amygdala | 171 infants (age 6 months) 204 infants (age 12 months) 201 infants (age 24 months) | sMRI | - | U-net | Dice score 0.882 (6-month) 0.882 (12-month) 0.903 (24-month) |
| [105] | 2020 | Anterior Visual Pathway | 18 subjects | sMRI | - | GAN | Dice score 0.602 ± 0.201 |
| [106] | 2018 | Brain Mask | 10 adolescent subjects (age 10–15 years), 25 newborn subjects from dHCP dataset | sMRI | - | CNN | F1 score 95.21 ± 0.94 (adolescent) 90.24 ± 1.84 (newborns) |
| [99] | 2019 | Brain Mask | 10 adolescent subjects, 26 newborn subjects from dHCP dataset, 25 other subjects (age 0.2–2.5 years) | sMRI | - | CNN | Improve dice score after labeling a very small portion of target dataset (<0.25%) |
| [107] | 2020 | Brain Mask | 197 fetuses (gestation age 24–39 weeks) | rs-fMRI | FSL | U-net | Dice score 0.94 |
| [98] | 2020 | Brain Mask | 71 scans of fetuses | rs-fMRI | AFNI | GAN | Dice score 0.973 ± 0.013 |
| [108] | 2020 | Brain Mask | 37 healthy fetuses (gestation age 27.3 ± 4.11 weeks) 32 fetuses with spina bifida pre-surgery (gestation age 23.06 ± 1.64 weeks) 16 fetuses post-surgery (gestation age 25.69 ± 1.21 weeks) | sMRI | -N4ITK | U-net | Dice score 0.9321 (healthy), 0.9387 (pre-surgery), 0.9294 (post-surgery) |
| [101] | 2021 | Brain Mask | 214 fetuses (gestation age 22–38 weeks) | sMRI | - | 3D U-net | Testing dice score 0.944 |
| [109] | 2021 | Brain Mask | 30 subjects (ages 2.34–4.31 years) | sMRI | - | CNN | Dice score 0.90 ± 0.14 |
| [110] | 2019 | Brain Tissue | 29 subjects (age 9.96 ± 7.16 years) | sMRI | - | 3D CNN | Dice score 0.888 (gray matter), 0.863 (white matter), 0.937 (CSF) |
| [111] | 2019 | Brain Tissue | 12 fetuses (gestation age 22.9–34.6 weeks) | sMRI | - | CNN | Dice score 0.88 |
| [112] | 2019 | Brain Tissue | 95 very pre-term infants (gestation age 28.5 ± 2.5 weeks, scan at term age), 28 very pre-term infants (gestation age 26.8 ± 2.1 weeks, scan at term age) | sMRI | - | CNN | Dice score 0.895 ± 0.098 testing dice score 0.845 ± 0.079 |
| [113] | 2020 | Brain Tissue | 47 patients with pediatric hydrocephalus (age 5.8 ± 5.4 years) | sMRI | - | CNN | Dice score 0.86 |
| [114] | 2021 | Brain Tissue | 35 subjects (age 4.2 ± 0.7 years) | sMRI | - | 3D CNN | JS = 0.83 for gray matter JS = 0.92 for white matter |
| [25] | 2021 | Brain Tissue | 98 preterm infants (gestation age ≤ 32 weeks) | DTI | In-house pipeline | 3D U-net | Dice score 0.907 ± 0.041 |
| [102] | 2022 | Brain Tissue | 106 fetuses (gestation age 23–39 weeks) | sMRI | FSL | 3D U-net | Dice score 0.897 |
| [115] | 2022 | Brain Tissue | dHCP datast: 150 term (gestation age 37–44 weeks ) 50 preterm (gestation age ≤ 32 weeks, scan at term-equivalent age) | sMRI | - | CNN | Dice score 0.88 |
| [116] | 2022 | Brain Tissue | 23 infants (age 6 ± 0.5 months) | sMRI | In-house pipeline | U-net | Dice score 0.92 (gray matter), 0.901 (white matter), 0.955 (CSF) |
| [117] | 2020 | Cerebral Arteries | 48 subjects (age 0.8–22 years) | sMRI | In-house pipeline | U-net | Testing dice score 0.75 |
| [118] | 2021 | Cerebral Ventricle | 200 patients with obstructive hydrocephalus (age 0–22 years) 199 HC (age 0–19 years) | sMRI | In-house pipeline | U-net | Dice score 0.901 |
| [103] | 2021 | Cortical Parcellation Network | dHCP datast: 403 infants, ePRIME dataset: 486 infants (gestation age 23–42 weeks, scanned at term-equivalent age) | sMRI | -MRITK | GAN | Dice score 0.96–0.99 |
| [119] | 2020 | Cortical Plate | 52 fetuses (gestation age 22.9–31.4 weeks) | sMRI | In-house pipeline | CNN | Testing dice score 0.907 ± 0.027 |
| [120] | 2021 | Cortical Plate | 12 fetuses (gestation age 16–39 weeks) | sMRI | -AutoNet, ITK-SNAP | CNN | Dice score 0.87 |
| [121] | 2019 | Intracranial Volume | 80 scans of fetuses (gestation age 22.9–34.6 weeks) 101 scans of infants (age 30–44 weeks) | sMRI | - | U-net | Dice score 0.976 |
| [122] | 2022 | Limbic Structure | dHCPdataset: 473 subjects (40.65 ± 2.19) | sMRI | - | CNN | Dice score 0.87 |
| [123] | 2022 | Posterior Limb of Internal Capsule | 450 preterm infants ( gestation age ≤ 32 weeks, scan at term-equivalent age) | sMRI | In-house pipeline | U-net | Dice score 0.690 |
| [124] | 2022 | Tuber | 29 subjects (age 9.96 ± 7.16 years) | sMRI | - | U-net | Testing dice score 0.59 ± 0.23 |
| [125] | 2022 | Tumor | 311 pediatric subjects | sMRI | - | U-net | Dice score 0.773 |
| [126] | 2022 | Tumor | 177 patients (age 0.27–17.87 years) | sMRI | CaPTk software | CNN | Dice score 0.910 |
| [100] | 2022 | Tumor | 122 patients (age 0.2–17.9 years) | sMRI | ANTs | 3D U-net | Dice score 0.724 |
| [97] | 2022 | Tumor | BraTS 2020 Dataset: 369 patients local dataset: 22 patients (average age 7.5–9 years) | sMRI | In-house pipeline | U-net | Dice score 0.896 |
3.3. Predicting Brain Age
3.4. Predicting Neurodevelopment Outcomes
| Study | Year | Score | Population | Technique | Preprocessing | Method | Results |
|---|---|---|---|---|---|---|---|
| [143] | 2021 | Cognitive Deficits | 261 very preterm infants (gestation age ≤32 weeks, scan at 39–44 weeks postmenstrual age) | DTI, rs-fMRI | FSL | CNN | Accuracy 88.4% |
| [145] | 2020 | Fluid Intelligence | ABCD Study 8333 subjects (age 9–10 years) | sMRI | - | 3D CNN | MSE 0.75626 |
| [141] | 2021 | Fluid Intelligence | ABCD Dataset 7709 subjects (age 9–10 years) | sMRI | FSL, ANFI, FreeSuerfer | CNN | Pearson’s correlation coefficient r = 0.18 |
| [138] | 2022 | Fluid Intelligence | ABCD Dataset 8070 subjects (age 9–11 years) HCP Dataset 1079 subjects (age 22–35 years) | sMRI | FreeSurfer | CNN | MSE 0.919 (ABCD Dataset) 0.834 (HCP dataset) |
| [140] | 2022 | Fluid Intelligence | ABCD Dataset 7693 subjects (age 9–11 years) | rs-fMRI | FreeSurfer | CNN | MAE 5.582 ± 0.012 |
| [142] | 2022 | Fluid Intelligence | ABCD Dataset Training: 3739 subjects, Validation 415 subjects, Testing 4515 subjects (age 9–11 years) | sMRI | FSL, ANFI, FreeSuerfer | CNN | MSE 82.56 for testing |
| [146] | 2021 | Language Scores | 31 subjects with persistent language concerns (age 4.25 ± 2.38years) | DTI | In-house pipeline | CNN | MAE 0.28 |
| [147] | 2021 | Language Scores | 37 subjects with epilepsy (age 11.8 ± 3.1years) | DTI | FSL | CNN | MAE 7.77 |
| [144] | 2020 | Motor | 77 very pre-term infants (gestation age <31 weeks ) | DTI | ANTS | CNN | Accuracy 73% |
| [139] | 2021 | Oral Reading | ABCD Study 5252 subjects (age 9–10 years) | sMRI, DTI | - | Auto-encoder | MSE 206.5 |
3.5. Optimizing MRI Brain Imaging and Analysis
| Study | Year | Task | Population | Technique | Preprocessing | Method | Results |
|---|---|---|---|---|---|---|---|
| [158] | 2020 | Image Enhancement | 131 neuro-oncology patients (age 0.4–17.1 years) | ASL | - | Auto-encoder | SNR Gain 62% |
| [159] | 2018 | Image Generation | 28 infants (scan at birth, 3 months, and 6 months) | DTI | FSL | CNN | MAE 44.4 ± 17.5 (3-month-old from neonates) 40.1 ± 10.6 (6-month-old from 3-month-old) |
| [154] | 2019 | Image Generation | 16 subjects (age 1.1–21.3 years) | sMRI | - | GAN | MAE 52.4 ± 17.6 |
| [155] | 2020 | Image Generation | 60 subjects (age 2.6–19 years) | sMRI | In-house pipeline | GAN | MAE 61.0 ± 14.1 |
| [156] | 2022 | Image Generation | ABCD Dataset: 1517 subjects (age 9–10 years) | sMRI | - | GAN | PSNR 31.371 ± 1.813 |
| [149] | 2022 | Image Generation | 127 neonates (postmenstrual age = 41.1 ± 1.5 weeks) | sMRI | ANTs | 3D GAN | RMAE 5.6 ± 1.1% |
| [157] | 2022 | Image Generation | 125 subjects (age 1–20 years) | sMRI | FSL | GAN | PSNR 28.5 ± 2.2 |
| [150] | 2019 | Image Quality Evaluation | ABIDE Dataset: 1112 subjects (age 7–64 years) | sMRI | SPM12 | CNN | Accuracy 84% |
| [153] | 2020 | Image Quality Evaluation | BCP dataset: 534 images (age 0–6 years) | sMRI | - | CNN | capable of real-time large-scale assessment with near-perfect accuracy. |
| [151] | 2021 | Image Quality Evaluation | 211 fetuses (gestation age 30.9 ± 5.5 weeks) | sMRI | In-house pipeline | CNN | Accuracy 85 ± 1% |
| [152] | 2022 | Image Quality Evaluation | ABCD Dataset: 2494 subjects (age 9–10 years) HBN Dataset: 4226 subjects (age 5–21 years) | DTI | MATRIX, FSL | CNN | Accuracy 96.61% (ABCD Dataset) 97.52% (HBN Dataset) |
| [160] | 2021 | Image Reconstruction | 20 fetuses (gestation age 23.4–38 weeks) | DTI | SVR pipeline | CNN | RMSE 0.0379 ± 0.0030 |
| [24] | 2021 | Image Reconstruction | 305 subjects (age 0–15 years) | sMRI | In-house pipeline | CNN+RNN | PSNR 27.85+/−2.12 |
| [161] | 2022 | Image Reconstruction | 107 subjects (age 0.2–18 years) | sMRI | - | CNN | image quality improved significantly by qualitative assessment |
| [148] | 2022 | Image Reconstruction | 47 subjects (age 2.3–14.7 years) | sMRI | - | CNN | Reduce scan time by 42% |
4. Discussion
4.1. Advancements in Deep Learning Applied to Pediatric MRI
4.2. Challenges and Future Directions
4.2.1. Overfitting Caused by Small Sample Size
4.2.2. Inconsistent Preprocessing Pipelines
4.2.3. Difficulty in Interpreting Deep Learning Results
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ABCD | The Adolescent Brain Cognitive Development |
| ABIDE | Autism Brain Imaging Data Exchange |
| ADHD | Attention deficit hyperactivity disorder |
| ASD | Autism spectrum disorder |
| ASL | Arterial spin labeling |
| CNN | Convolutional neural network |
| dHCP | Human Connectomme Project Development |
| DTI | Diffusion tensor imaging |
| fMRI | functional MRI |
| GAN | Generative adversarial network |
| HBN | Human Brain Network |
| HC | Healthy control |
| ICBM | International Consortium for Brain Mapping |
| IMPAC | Imaging Psychiatry Challenge |
| MAE | mean absolute error |
| MLP | Multi-layer perceptron |
| MRI | Magnetic resonance imaging |
| MSE | mean squared error |
| NDAR | National Dtabase for Autism Research |
| PNC | Philadelphia Neurodevelopmental Cohort |
| PRISMA | preferred reporting items for systematic reviews and meta-analysis |
| PSNR | Peak signal-to-noise ratio |
| rs-fMRI | resting-state fMRI |
| sMRI | structural MRI |
Appendix A. Risk of Bias Analysis
| Study | Confounding | Selection of Participants | Classification of Interventions | Deviations from Intended Interventions | Missing Data | Measurement of Outcomes | Selection of Reported Results | Summary |
|---|---|---|---|---|---|---|---|---|
| [79] | PN | PY | N | N | N | PY | N | Moderate |
| [80] | N | PY | N | N | N | PY | N | Moderate |
| [51] | PN | N | N | N | N | PY | N | Low |
| [81] | PN | PY | N | N | N | PY | N | Moderate |
| [53] | PN | PN | N | N | N | PY | N | Low |
| [52] | PN | PY | N | N | N | PY | N | Moderate |
| [55] | PN | N | N | N | N | PY | N | Low |
| [82] | PN | N | N | N | N | PY | N | Low |
| [69] | PN | PY | N | N | N | PY | N | Moderate |
| [74] | N | PY | N | N | N | PY | N | Moderate |
| [83] | PN | N | N | N | N | PY | N | Low |
| [84] | PN | N | N | N | N | PY | N | Low |
| [85] | N | PY | N | N | N | PY | N | Moderate |
| [76] | PN | N | N | N | N | PY | N | Low |
| [54] | PN | N | N | N | N | N | N | Low |
| [73] | PN | N | N | N | N | PY | N | Low |
| [86] | N | PN | N | N | N | PY | N | Low |
| [75] | PN | PN | N | N | N | PY | N | Low |
| [87] | PN | N | N | PY | N | PY | N | Moderate |
| [88] | PN | PN | N | N | N | PY | N | Low |
| [78] | PN | N | N | N | N | N | N | Low |
| [89] | PN | N | N | N | N | PY | N | Low |
| [90] | PN | N | N | N | N | PY | N | Low |
| [91] | PN | PY | N | N | N | N | N | Low |
| [77] | PN | N | N | N | N | PY | N | Low |
| [92] | N | PY | N | N | N | PY | N | Moderate |
| [93] | N | PN | N | N | N | PY | N | Low |
| [57] | N | PY | N | N | N | PY | N | Moderate |
| [61] | N | PY | N | N | N | PY | N | Moderate |
| [62] | PN | N | N | N | N | PY | N | Low |
| [58] | N | PY | N | N | N | PY | N | Moderate |
| [70] | N | PN | N | N | N | PY | N | Low |
| [59] | N | PY | N | N | N | PY | N | Moderate |
| [60] | N | PY | N | N | N | PY | N | Moderate |
| [94] | N | PY | N | N | N | PY | N | Moderate |
| [63] | N | PY | N | N | N | PY | N | Moderate |
| [64] | N | PN | N | N | N | PY | N | Low |
| [65] | N | PN | N | N | N | PY | N | Low |
| [71] | N | PN | N | N | N | PY | N | Low |
| [95] | PY | PY | N | N | N | PY | N | Moderate |
| [72] | N | N | N | N | N | PY | N | Low |
| [66] | N | PN | N | N | N | PY | N | Low |
| [96] | N | PY | N | N | N | PY | N | Moderate |
| [67] | N | PY | N | N | N | PY | N | Moderate |
| [68] | N | PY | N | N | N | PY | N | Moderate |
| [104] | N | PN | N | N | N | PY | N | Low |
| [105] | N | PY | N | N | N | PY | N | Moderate |
| [106] | N | PY | N | N | N | PY | N | Moderate |
| [99] | N | PY | N | N | N | PY | N | Moderate |
| [107] | N | PN | N | N | N | PY | N | Low |
| [98] | N | PY | N | N | N | PY | N | Moderate |
| [108] | N | PY | N | N | N | PY | N | Moderate |
| [101] | N | PN | N | N | N | PY | N | Low |
| [109] | N | PY | N | N | N | PY | N | Moderate |
| [110] | N | PY | N | N | N | PY | N | Moderate |
| [111] | N | PY | N | N | N | PY | N | Moderate |
| [112] | N | PY | N | N | N | PN | N | Low |
| [113] | N | PY | N | N | N | PY | N | Moderate |
| [114] | N | PY | N | N | N | PY | N | Moderate |
| [25] | N | PY | N | N | N | PY | N | Moderate |
| [102] | N | PN | N | N | N | PY | N | Low |
| [115] | PN | PN | N | N | N | PY | N | Low |
| [116] | N | PY | N | N | N | PY | N | Moderate |
| [117] | N | PY | N | N | N | PN | N | Low |
| [118] | N | PN | N | N | N | PY | N | Low |
| [103] | PN | PN | N | N | N | PY | N | Low |
| [119] | N | PY | N | N | N | PN | N | Low |
| [120] | N | PY | N | N | N | PY | N | Moderate |
| [121] | N | PY | N | N | N | PY | N | Moderate |
| [122] | PN | PN | N | N | N | PY | N | Low |
| [123] | N | PN | N | N | N | PY | N | Low |
| [124] | N | PY | N | N | N | PN | N | Low |
| [125] | N | PN | N | N | N | PY | N | Low |
| [126] | N | PN | N | N | N | PY | N | Low |
| [100] | N | PN | N | N | N | PY | N | Low |
| [97] | N | PN | N | N | N | PY | N | Low |
| [84] | N | PN | N | N | N | PY | N | Low |
| [130] | N | N | N | N | N | PY | N | Low |
| [131] | N | N | N | N | N | PY | N | Low |
| [132] | PN | N | N | N | N | N | N | Low |
| [127] | N | PN | N | N | N | PY | N | Low |
| [129] | N | N | N | N | N | PY | N | Low |
| [128] | N | PY | N | N | N | PY | N | Moderate |
| [133] | N | PY | N | N | N | PY | N | Moderate |
| [134] | N | PN | N | N | N | PY | N | Low |
| [135] | N | PN | N | N | N | PY | N | Low |
| [136] | N | PN | N | N | N | PY | N | Low |
| [137] | N | N | N | N | N | PY | N | Low |
| [143] | N | PN | N | N | N | PY | N | Low |
| [145] | PN | N | N | N | N | PY | N | Low |
| [141] | PN | N | N | N | N | PY | N | Low |
| [138] | PN | N | N | N | N | PY | N | Low |
| [140] | PN | N | N | N | N | PY | N | Low |
| [142] | PN | N | N | N | N | N | N | Low |
| [146] | N | PY | N | N | N | PY | N | Moderate |
| [147] | N | PY | N | N | N | PY | N | Moderate |
| [144] | N | PY | N | N | N | PY | N | Moderate |
| [139] | PN | N | N | N | N | PY | N | Low |
| [158] | N | PN | N | N | N | PY | N | Low |
| [159] | N | PY | N | N | N | PY | N | Moderate |
| [154] | N | PY | N | N | N | PY | N | Moderate |
| [155] | N | PY | N | N | N | PY | N | Moderate |
| [156] | N | N | N | N | N | PY | N | Low |
| [149] | N | PN | N | N | N | PY | N | Low |
| [157] | N | PN | N | N | N | PY | N | Low |
| [150] | PN | N | N | N | N | PY | N | Low |
| [153] | PN | N | N | N | N | PY | N | Low |
| [151] | N | PN | N | N | N | PY | N | Low |
| [152] | PN | N | N | N | N | PY | N | Low |
| [160] | N | PY | N | N | N | PY | N | Moderate |
| [24] | N | PN | N | N | N | PY | N | Low |
| [161] | N | PN | N | N | N | PN | N | Low |
| [148] | N | PN | N | N | N | PY | N | Low |
References
- Jordan, M.I.; Mitchell, T.M. Machine learning: Trends, perspectives, and prospects. Science 2015, 349, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Celard, P.; Iglesias, E.; Sorribes-Fdez, J.; Romero, R.; Vieira, A.S.; Borrajo, L. A survey on deep learning applied to medical images: From simple artificial neural networks to generative models. Neural Comput. Appl. 2022, 35, 2291–2323. [Google Scholar] [CrossRef] [PubMed]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Gu, J.; Wang, Z.; Kuen, J.; Ma, L.; Shahroudy, A.; Shuai, B.; Liu, T.; Wang, X.; Wang, G.; Cai, J.; et al. Recent advances in convolutional neural networks. Pattern Recognit. 2018, 77, 354–377. [Google Scholar] [CrossRef]
- Hosny, A.; Parmar, C.; Quackenbush, J.; Schwartz, L.H.; Aerts, H.J.W.L. Artificial intelligence in radiology. Nat. Reviews. Cancer 2018, 18, 500–510. [Google Scholar] [CrossRef]
- Reig, B.; Heacock, L.; Geras, K.J.; Moy, L. Machine learning in breast MRI. J. Magn. Reson. Imaging JMRI 2020, 52, 998–1018. [Google Scholar] [CrossRef]
- Eslami, T.; Almuqhim, F.; Raiker, J.S.; Saeed, F. Machine learning methods for diagnosing autism spectrum disorder and attention-deficit/hyperactivity disorder using functional and structural MRI: A survey. Front. Neuroinformatics 2021, 14, 575999. [Google Scholar] [CrossRef]
- Zhang, Z.; Li, G.; Xu, Y.; Tang, X. Application of artificial intelligence in the MRI classification task of human brain neurological and psychiatric diseases: A scoping review. Diagnostics 2021, 11, 1402. [Google Scholar] [CrossRef]
- Yousaf, T.; Dervenoulas, G.; Politis, M. Advances in MRI methodology. Int. Rev. Neurobiol. 2018, 141, 31–76. [Google Scholar] [CrossRef]
- Pykett, I.L.; Newhouse, J.H.; Buonanno, F.S.; Brady, T.J.; Goldman, M.R.; Kistler, J.P.; Pohost, G.M. Principles of nuclear magnetic resonance imaging. Radiology 1982, 143, 157–168. [Google Scholar] [CrossRef]
- Van Geuns, R.J.M.; Wielopolski, P.A.; de Bruin, H.G.; Rensing, B.J.; van Ooijen, P.M.; Hulshoff, M.; Oudkerk, M.; de Feyter, P.J. Basic principles of magnetic resonance imaging. Prog. Cardiovasc. Dis. 1999, 42, 149–156. [Google Scholar] [CrossRef]
- Huettel, S.A.; Song, A.W.; McCarthy, G. Functional Magnetic Resonance Imaging; Sinauer Associates Sunderland: Sunderland, MA, USA, 2004; Volume 1. [Google Scholar]
- Mori, S.; Zhang, J. Principles of diffusion tensor imaging and its applications to basic neuroscience research. Neuron 2006, 51, 527–539. [Google Scholar] [CrossRef] [PubMed]
- Colombo, E.; Fick, T.; Esposito, G.; Germans, M.; Regli, L.; van Doormaal, T. Segmentation techniques of brain arteriovenous malformations for 3D visualization: A systematic review. Radiol. Medica 2022, 127, 1333–1341. [Google Scholar] [CrossRef] [PubMed]
- Castiglioni, I.; Rundo, L.; Codari, M.; Di Leo, G.; Salvatore, C.; Interlenghi, M.; Gallivanone, F.; Cozzi, A.; D’Amico, N.C.; Sardanelli, F. AI applications to medical images: From machine learning to deep learning. Phys. Medica 2021, 83, 9–24. [Google Scholar] [CrossRef] [PubMed]
- Khodatars, M.; Shoeibi, A.; Sadeghi, D.; Ghaasemi, N.; Jafari, M.; Moridian, P.; Khadem, A.; Alizadehsani, R.; Zare, A.; Kong, Y.; et al. Deep learning for neuroimaging-based diagnosis and rehabilitation of autism spectrum disorder: A review. Comput. Biol. Med. 2021, 139, 104949. [Google Scholar] [CrossRef] [PubMed]
- Bahathiq, R.A.; Banjar, H.; Bamaga, A.K.; Jarraya, S.K. Machine learning for autism spectrum disorder diagnosis using structural magnetic resonance imaging: Promising but challenging. Front. Neuroinform. 2022, 16, 949926. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Di, J.; Wang, D.; Dai, X.; Hua, Y.; Gao, X.; Zheng, A.; Gao, J. State-of-the-Art Review of Artificial Neural Networks to Predict, Characterize and Optimize Pharmaceutical Formulation. Pharmaceutics 2022, 14, 183. [Google Scholar] [CrossRef] [PubMed]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. Commun. ACM 2017, 60, 84–90. [Google Scholar] [CrossRef]
- Szegedy, C.; Liu, W.; Jia, Y.; Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going deeper with convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; pp. 1–9. [Google Scholar] [CrossRef]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar] [CrossRef]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In Proceedings of the International Conference on Medical image Computing and Computer-Assisted Intervention, Munich, Germany, 5–9 October 2015; Springer: Berlin/Heidelberg, Germany, 2015; pp. 234–241. [Google Scholar] [CrossRef]
- Li, Z.; Yu, J.; Wang, Y.; Zhou, H.; Yang, H.; Qiao, Z. Deepvolume: Brain structure and spatial connection-aware network for brain mri super-resolution. IEEE Trans. Cybern. 2019, 51, 3441–3454. [Google Scholar] [CrossRef]
- Li, H.; Chen, M.; Wang, J.; Illapani, V.S.P.; Parikh, N.A.; He, L. Automatic Segmentation of Diffuse White Matter Abnormality on T2-weighted Brain MR Images Using Deep Learning in Very Preterm Infants. Radiol. Artif. Intell. 2021, 3, e200166. [Google Scholar] [CrossRef]
- Yuan, J.; Ran, X.; Liu, K.; Yao, C.; Yao, Y.; Wu, H.; Liu, Q. Machine learning applications on neuroimaging for diagnosis and prognosis of epilepsy: A review. J. Neurosci. Methods 2021, 368, 109441. [Google Scholar] [CrossRef] [PubMed]
- Elbattah, M.; Loughnane, C.; Guérin, J.L.; Carette, R.; Cilia, F.; Dequen, G. Variational Autoencoder for Image-Based Augmentation of Eye-Tracking Data. J. Imaging 2021, 7, 83. [Google Scholar] [CrossRef] [PubMed]
- Goodfellow, I.; Pouget-Abadie, J.; Mirza, M.; Xu, B.; Warde-Farley, D.; Ozair, S.; Courville, A.; Bengio, Y. Generative Adversarial Nets. In Proceedings of the Advances in Neural Information Processing Systems; Ghahramani, Z., Welling, M., Cortes, C., Lawrence, N., Weinberger, K.Q., Eds.; Curran Associates, Inc.: New York, NY, USA, 2014; Volume 27. [Google Scholar]
- Pan, Z.; Yu, W.; Yi, X.; Khan, A.; Yuan, F.; Zheng, Y. Recent progress on generative adversarial networks (GANs): A survey. IEEE Access 2019, 7, 36322–36333. [Google Scholar] [CrossRef]
- Yi, X.; Walia, E.; Babyn, P. Generative adversarial network in medical imaging: A review. Med. Image Anal. 2019, 58, 101552. [Google Scholar] [CrossRef]
- Di Martino, A.; Yan, C.G.; Li, Q.; Denio, E.; Castellanos, F.X.; Alaerts, K.; Anderson, J.S.; Assaf, M.; Bookheimer, S.Y.; Dapretto, M.; et al. The autism brain imaging data exchange: Towards a large-scale evaluation of the intrinsic brain architecture in autism. Mol. Psychiatry 2014, 19, 659–667. [Google Scholar] [CrossRef]
- Di Martino, A.; O’Connor, D.; Chen, B.; Alaerts, K.; Anderson, J.S.; Assaf, M.; Balsters, J.H.; Baxter, L.; Beggiato, A.; Bernaerts, S.; et al. Enhancing studies of the connectome in autism using the autism brain imaging data exchange II. Sci. Data 2017, 4, 170010. [Google Scholar] [CrossRef]
- IMPAC—Imaging-Psychiatry Challenge: Predicting Autism. Available online: https://paris-saclay-cds.github.io/autism_challenge/ (accessed on 15 December 2022).
- Consortium, T.A. The ADHD-200 consortium: A model to advance the translational potential of neuroimaging in clinical neuroscience. Front. Syst. Neurosci. 2012, 6, 62. [Google Scholar] [CrossRef]
- Sudlow, C.; Gallacher, J.; Allen, N.; Beral, V.; Burton, P.; Danesh, J.; Downey, P.; Elliott, P.; Green, J.; Landray, M.; et al. UK biobank: An open access resource for identifying the causes of a wide range of complex diseases of middle and old age. PLoS Med. 2015, 12, e1001779. [Google Scholar] [CrossRef]
- Payakachat, N.; Tilford, J.M.; Ungar, W.J. National Database for Autism Research (NDAR): Big Data Opportunities for Health Services Research and Health Technology Assessment. PharmacoEconomics 2016, 34, 127–138. [Google Scholar] [CrossRef]
- Poldrack, R.A.; Barch, D.M.; Mitchell, J.P.; Wager, T.D.; Wagner, A.D.; Devlin, J.T.; Cumba, C.; Koyejo, O.; Milham, M.P. Toward open sharing of task-based fMRI data: The OpenfMRI project. Front. Neuroinform. 2013, 7, 12. [Google Scholar] [CrossRef]
- Mazziotta, J.; Toga, A.; Evans, A.; Fox, P.; Lancaster, J.; Zilles, K.; Woods, R.; Paus, T.; Simpson, G.; Pike, B.; et al. A probabilistic atlas and reference system for the human brain: International Consortium for Brain Mapping (ICBM). Philos. Trans. R. Soc. London. Ser. B Biol. Sci. 2001, 356, 1293–1322. [Google Scholar] [CrossRef] [PubMed]
- Yan, C.G.; Craddock, R.C.; Zuo, X.N.; Zang, Y.F.; Milham, M.P. Standardizing the intrinsic brain: Towards robust measurement of inter-individual variation in 1000 functional connectomes. Neuroimage 2013, 80, 246–262. [Google Scholar] [CrossRef] [PubMed]
- Casey, B.J.; Cannonier, T.; Conley, M.I.; Cohen, A.O.; Barch, D.M.; Heitzeg, M.M.; Soules, M.E.; Teslovich, T.; Dellarco, D.V.; Garavan, H. The adolescent brain cognitive development (ABCD) study: Imaging acquisition across 21 sites. Dev. Cogn. Neurosci. 2018, 32, 43–54. [Google Scholar] [CrossRef]
- Thompson, P.M.; Stein, J.L.; Medland, S.E.; Hibar, D.P.; Vasquez, A.A.; Renteria, M.E.; Toro, R.; Jahanshad, N.; Schumann, G.; Franke, B. The ENIGMA Consortium: Large-scale collaborative analyses of neuroimaging and genetic data. Brain Imaging Behav. 2014, 8, 153–182. [Google Scholar] [CrossRef]
- Satterthwaite, T.D.; Elliott, M.A.; Ruparel, K.; Loughead, J.; Prabhakaran, K.; Calkins, M.E.; Hopson, R.; Jackson, C.; Keefe, J.; Riley, M. Neuroimaging of the Philadelphia neurodevelopmental cohort. Neuroimage 2014, 86, 544–553. [Google Scholar] [CrossRef]
- Alexander, L.M.; Escalera, J.; Ai, L.; Andreotti, C.; Febre, K.; Mangone, A.; Vega-Potler, N.; Langer, N.; Alexander, A.; Kovacs, M. An open resource for transdiagnostic research in pediatric mental health and learning disorders. Sci. Data 2017, 4, 1–26. [Google Scholar] [CrossRef]
- Van Essen, D.C.; Ugurbil, K.; Auerbach, E.; Barch, D.; Behrens, T.E.J.; Bucholz, R.; Chang, A.; Chen, L.; Corbetta, M.; Curtiss, S.W. The Human Connectome Project: A data acquisition perspective. Neuroimage 2012, 62, 2222–2231. [Google Scholar] [CrossRef]
- Howell, B.R.; Styner, M.A.; Gao, W.; Yap, P.T.; Wang, L.; Baluyot, K.; Yacoub, E.; Chen, G.; Potts, T.; Salzwedel, A.; et al. The UNC/UMN Baby Connectome Project (BCP): An overview of the study design and protocol development. NeuroImage 2019, 185, 891–905. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355. [Google Scholar] [CrossRef]
- Edition, F. Diagnostic and statistical manual of mental disorders. Am. Psychiatr. Assoc. 2013, 21, 591–643. [Google Scholar]
- Morris-Rosendahl, D.J.; Crocq, M.A. Neurodevelopmental disorders-the history and future of a diagnostic concept. Dialogues Clin. Neurosci. 2020, 22, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Dvornek, N.C.; Ventola, P.; Duncan, J.S. Combining phenotypic and resting-state fMRI data for autism classification with recurrent neural networks. In Proceedings of the 2018 IEEE 15th International Symposium on Biomedical Imaging (ISBI 2018), Washington, DC, USA, 4–7 April 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 725–728. [Google Scholar]
- Xiao, Z.; Wu, J.; Wang, C.; Jia, N.; Yang, X. Computer-aided diagnosis of school-aged children with ASD using full frequency bands and enhanced SAE: A multi-institution study. Exp. Ther. Med. 2019, 17, 4055–4063. [Google Scholar] [CrossRef] [PubMed]
- Aghdam, M.A.; Sharifi, A.; Pedram, M.M. Diagnosis of autism spectrum disorders in young children based on resting-state functional magnetic resonance imaging data using convolutional neural networks. J. Digit. Imaging 2019, 32, 899–918. [Google Scholar] [CrossRef]
- Li, H.; Parikh, N.A.; He, L. A novel transfer learning approach to enhance deep neural network classification of brain functional connectomes. Front. Neurosci. 2018, 12, 491. [Google Scholar] [CrossRef]
- Leming, M.; Górriz, J.M.; Suckling, J. Ensemble deep learning on large, mixed-site fMRI datasets in autism and other tasks. Int. J. Neural Syst. 2020, 30, 2050012. [Google Scholar] [CrossRef] [PubMed]
- Sibley, M.H.; Swanson, J.M.; Arnold, L.E.; Hechtman, L.T.; Owens, E.B.; Stehli, A.; Abikoff, H.; Hinshaw, S.P.; Molina, B.S.; Mitchell, J.T.; et al. Defining ADHD symptom persistence in adulthood: Optimizing sensitivity and specificity. J. Child Psychol. Psychiatry 2017, 58, 655–662. [Google Scholar] [CrossRef]
- Ceschin, R.; Zahner, A.; Reynolds, W.; Gaesser, J.; Zuccoli, G.; Lo, C.W.; Gopalakrishnan, V.; Panigrahy, A. A computational framework for the detection of subcortical brain dysmaturation in neonatal MRI using 3D Convolutional Neural Networks. NeuroImage 2018, 178, 183–197. [Google Scholar] [CrossRef]
- Zahia, S.; Garcia-Zapirain, B.; Saralegui, I.; Fernandez-Ruanova, B. Dyslexia detection using 3D convolutional neural networks and functional magnetic resonance imaging. Comput. Methods Programs Biomed. 2020, 197, 105726. [Google Scholar] [CrossRef]
- Aminpour, A.; Ebrahimi, M.; Widjaja, E. Deep learning-based lesion segmentation in paediatric epilepsy. In Proceedings of the Medical Imaging 2021: Computer-Aided Diagnosis, Online, 15–19 February 2021; SPIE: Washington, DC, USA, 2021; Volume 11597, pp. 635–641. [Google Scholar] [CrossRef]
- Huang, J.; Xu, J.; Kang, L.; Zhang, T. Identifying epilepsy based on deep learning using DKI images. Front. Hum. Neurosci. 2020, 14, 590815. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Li, X.; Li, Y.; Wang, M.; Huang, B.; Yao, S.; Shen, L. Three dimensional convolutional neural network-based classification of conduct disorder with structural MRI. Brain Imaging Behav. 2020, 14, 2333–2340. [Google Scholar] [CrossRef] [PubMed]
- Menon, S.S.; Krishnamurthy, K. Multimodal Ensemble Deep Learning to Predict Disruptive Behavior Disorders in Children. Front. Neuroinform. 2021, 15, 742807. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Lei, D.; Qin, K.; Pinaya, W.H.; Suo, X.; Li, W.; Li, L.; Kemp, G.J.; Gong, Q. Using deep learning to classify pediatric posttraumatic stress disorder at the individual level. BMC Psychiatry 2021, 21, 535. [Google Scholar] [CrossRef] [PubMed]
- Jiang, D.; Hu, Z.; Zhao, C.; Zhao, X.; Yang, J.; Zhu, Y.; Liao, J.; Liang, D.; Wang, H. Identification of Children’s Tuberous Sclerosis Complex with Multiple-contrast MRI and 3D Convolutional Network. In Proceedings of the 2022 44th Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Scotland, UK, 11–15 July 2022; IEEE: Piscataway, NJ, USA, 2022; pp. 2924–2927. [Google Scholar]
- Shabanian, M.; Imran, A.A.Z.; Siddiqui, A.; Davis, R.L.; Bissler, J.J. 3D deep neural network to automatically identify TSC structural brain pathology based on MRI. In Proceedings of the Medical Imaging 2022: Image Processing, San Diego, CA, USA, 20–24 February 2022; SPIE: Washington, DC, USA, 2022; Volume 12032, pp. 613–619. [Google Scholar]
- Afshar, P.; Mohammadi, A.; Plataniotis, K.N. Brain tumor type classification via capsule networks. In Proceedings of the 2018 25th IEEE international conference on image processing (ICIP), Athens, Greece, 7–10 October 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 3129–3133. [Google Scholar] [CrossRef]
- Lee, M.H.; O’Hara, N.; Sonoda, M.; Kuroda, N.; Juhasz, C.; Asano, E.; Dong, M.; Jeong, J.W. Novel deep learning network analysis of electrical stimulation mapping-driven diffusion MRI tractography to improve preoperative evaluation of pediatric epilepsy. IEEE Trans. Biomed. Eng. 2020, 67, 3151–3162. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Dong, M.; Lee, M.H.; O’Hara, N.; Asano, E.; Jeong, J.W. Objective detection of eloquent axonal pathways to minimize postoperative deficits in pediatric epilepsy surgery using diffusion tractography and convolutional neural networks. IEEE Trans. Med. Imaging 2019, 38, 1910–1922. [Google Scholar] [CrossRef]
- Yang, M.; Cao, M.; Chen, Y.; Chen, Y.; Fan, G.; Li, C.; Wang, J.; Liu, T. Large-scale brain functional network integration for discrimination of autism using a 3-D deep learning model. Front. Hum. Neurosci. 2021, 15, 277. [Google Scholar] [CrossRef]
- Wu, M.; Shen, X.; Lai, C.; Zheng, W.; Li, Y.; Shangguan, Z.; Yan, C.; Liu, T.; Wu, D. Detecting neonatal acute bilirubin encephalopathy based on T1-weighted MRI images and learning-based approaches. BMC Med. Imaging 2021, 21, 103. [Google Scholar] [CrossRef]
- Sánchez Fernández, I.; Yang, E.; Calvachi, P.; Amengual-Gual, M.; Wu, J.Y.; Krueger, D.; Northrup, H.; Bebin, M.E.; Sahin, M.; Yu, K.H.; et al. Deep learning in rare disease. Detection of tubers in tuberous sclerosis complex. PLoS ONE 2020, 15, e0232376. [Google Scholar] [CrossRef]
- Quon, J.; Bala, W.; Chen, L.; Wright, J.; Kim, L.; Han, M.; Shpanskaya, K.; Lee, E.; Tong, E.; Iv, M.; et al. Deep learning for pediatric posterior fossa tumor detection and classification: A multi-institutional study. Am. J. Neuroradiol. 2020, 41, 1718–1725. [Google Scholar] [CrossRef]
- Li, S.; Tang, Z.; Jin, N.; Yang, Q.; Liu, G.; Liu, T.; Hu, J.; Liu, S.; Wang, P.; Hao, J.; et al. Uncovering Brain Differences in Preschoolers and Young Adolescents with Autism Spectrum Disorder Using Deep Learning. Int. J. Neural Syst. 2022, 32, 2250044. [Google Scholar] [CrossRef] [PubMed]
- Haweel, R.; Shalaby, A.; Mahmoud, A.; Seada, N.; Ghoniemy, S.; Ghazal, M.; Casanova, M.F.; Barnes, G.N.; El-Baz, A. A robust DWT–CNN-based CAD system for early diagnosis of autism using task-based fMRI. Med. Phys. 2021, 48, 2315–2326. [Google Scholar] [CrossRef] [PubMed]
- Mellema, C.J.; Nguyen, K.P.; Treacher, A.; Montillo, A. Reproducible neuroimaging features for diagnosis of autism spectrum disorder with machine learning. Sci. Rep. 2022, 12, 3057. [Google Scholar] [CrossRef] [PubMed]
- Leming, M.J.; Baron-Cohen, S.; Suckling, J. Single-participant structural similarity matrices lead to greater accuracy in classification of participants than function in autism in MRI. Mol. Autism 2021, 12, 34. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Li, H.; Fan, H.; Dillman, J.R.; Wang, H.; Altaye, M.; Zhang, B.; Parikh, N.A.; He, L. ConCeptCNN: A novel multi-filter convolutional neural network for the prediction of neurodevelopmental disorders using brain connectome. Med. Phys. 2022, 49, 3171–3184. [Google Scholar] [CrossRef]
- Zhang-James, Y.; Helminen, E.C.; Liu, J.; Franke, B.; Hoogman, M.; Faraone, S.V. Evidence for similar structural brain anomalies in youth and adult attention-deficit/hyperactivity disorder: A machine learning analysis. Transl. Psychiatry 2021, 11, 82. [Google Scholar] [CrossRef]
- Guo, X.; Dominick, K.C.; Minai, A.A.; Li, H.; Erickson, C.A.; Lu, L.J. Diagnosing autism spectrum disorder from brain resting-state functional connectivity patterns using a deep neural network with a novel feature selection method. Front. Neurosci. 2017, 11, 460. [Google Scholar] [CrossRef]
- Li, X.; Dvornek, N.C.; Zhuang, J.; Ventola, P.; Duncan, J.S. Brain biomarker interpretation in ASD using deep learning and fMRI. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Granada, Spain, 16–20 September 2018; Springer: Berlin/Heidelberg, Germany, 2018; pp. 206–214. [Google Scholar]
- Akhavan Aghdam, M.; Sharifi, A.; Pedram, M.M. Combination of rs-fMRI and sMRI data to discriminate autism spectrum disorders in young children using deep belief network. J. Digit. Imaging 2018, 31, 895–903. [Google Scholar] [CrossRef]
- Ke, F.; Choi, S.; Kang, Y.H.; Cheon, K.A.; Lee, S.W. Exploring the structural and strategic bases of autism spectrum disorders with deep learning. IEEE Access 2020, 8, 153341–153352. [Google Scholar] [CrossRef]
- Husna, R.N.S.; Syafeeza, A.; Hamid, N.A.; Wong, Y.; Raihan, R.A. Functional magnetic resonance imaging for autism spectrum disorder detection using deep learning. J. Teknol. 2021, 83, 45–52. [Google Scholar] [CrossRef]
- Kawahara, J.; Brown, C.J.; Miller, S.P.; Booth, B.G.; Chau, V.; Grunau, R.E.; Zwicker, J.G.; Hamarneh, G. BrainNetCNN: Convolutional neural networks for brain networks; towards predicting neurodevelopment. NeuroImage 2017, 146, 1038–1049. [Google Scholar] [CrossRef] [PubMed]
- Gao, K.; Sun, Y.; Niu, S.; Wang, L. Unified framework for early stage status prediction of autism based on infant structural magnetic resonance imaging. Autism Res. 2021, 14, 2512–2523. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Wang, J.; Wang, X.; Liu, W.; Yu, H.; Xu, L.; Li, H.; Wu, J.; Dong, M.; Tan, W.; et al. Diagnosing autism spectrum disorder in children using conventional MRI and apparent diffusion coefficient based deep learning algorithms. Eur. Radiol. 2022, 32, 761–770. [Google Scholar] [CrossRef]
- Wang, T.; Kamata, S.I. Classification of structural MRI images in Adhd using 3D fractal dimension complexity map. In Proceedings of the 2019 IEEE International Conference on Image Processing (ICIP), Taipei, Taiwan, 22–25 September 2018; IEEE: Piscataway, NJ, USA, 2019; pp. 215–219. [Google Scholar]
- Riaz, A.; Asad, M.; Alonso, E.; Slabaugh, G. DeepFMRI: End-to-end deep learning for functional connectivity and classification of ADHD using fMRI. J. Neurosci. Methods 2020, 335, 108506. [Google Scholar] [CrossRef]
- Tang, Y.; Sun, J.; Wang, C.; Zhong, Y.; Jiang, A.; Liu, G.; Liu, X. ADHD classification using auto-encoding neural network and binary hypothesis testing. Artif. Intell. Med. 2022, 123, 102209. [Google Scholar] [CrossRef]
- Ke, H.; Wang, F.; Ma, H.; He, Z. ADHD identification and its interpretation of functional connectivity using deep self-attention factorization. Knowl.-Based Syst. 2022, 250, 109082. [Google Scholar] [CrossRef]
- Wang, D.; Hong, D.; Wu, Q. Attention Deficit Hyperactivity Disorder Classification Based on Deep Learning. IEEE/Acm Trans. Comput. Biol. Bioinform. 2022, 1. [Google Scholar] [CrossRef]
- Uyulan, C.; Erguzel, T.T.; Turk, O.; Farhad, S.; Metin, B.; Tarhan, N. A Class Activation Map-Based Interpretable Transfer Learning Model for Automated Detection of ADHD from fMRI Data. Clin. EEG Neurosci. 2022, 54, 15500594221122699. [Google Scholar] [CrossRef]
- Stanley, E.A.M.; Rajashekar, D.; Mouches, P.; Wilms, M.; Plettl, K.; Forkert, N.D. A fully convolutional neural network for explainable classification of attention deficit hyperactivity disorder. In Proceedings of the Medical Imaging 2022: Computer-Aided Diagnosis, Leicester, UK, 20–21 November 2022; SPIE: Washington, DC, USA, 2022; Volume 12033, pp. 296–301. [Google Scholar]
- Attallah, O.; Sharkas, M.A.; Gadelkarim, H. Deep learning techniques for automatic detection of embryonic neurodevelopmental disorders. Diagnostics 2020, 10, 27. [Google Scholar] [CrossRef]
- Artzi, M.; Redmard, E.; Tzemach, O.; Zeltser, J.; Gropper, O.; Roth, J.; Shofty, B.; Kozyrev, D.A.; Constantini, S.; Ben-Sira, L. Classification of pediatric posterior fossa tumors using convolutional neural network and tabular data. IEEE Access 2021, 9, 91966–91973. [Google Scholar] [CrossRef]
- Prince, E.W.; Whelan, R.; Mirsky, D.M.; Stence, N.; Staulcup, S.; Klimo, P.; Anderson, R.C.; Niazi, T.N.; Grant, G.; Souweidane, M.; et al. Robust deep learning classification of adamantinomatous craniopharyngioma from limited preoperative radiographic images. Sci. Rep. 2020, 10, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Nalepa, J.; Adamski, S.; Kotowski, K.; Chelstowska, S.; Machnikowska-Sokolowska, M.; Bozek, O.; Wisz, A.; Jurkiewicz, E. Segmenting pediatric optic pathway gliomas from MRI using deep learning. Comput. Biol. Med. 2022, 142, 105237. [Google Scholar] [CrossRef] [PubMed]
- Asis-Cruz, D.; Krishnamurthy, D.; Jose, C.; Cook, K.M.; Limperopoulos, C. FetalGAN: Automated Segmentation of Fetal Functional Brain MRI Using Deep Generative Adversarial Learning and Multi-Scale 3D U-Net. Front. Neurosci. 2022, 16, 852. [Google Scholar] [CrossRef]
- Sourati, J.; Gholipour, A.; Dy, J.G.; Tomas-Fernandez, X.; Kurugol, S.; Warfield, S.K. Intelligent labeling based on fisher information for medical image segmentation using deep learning. IEEE Trans. Med. Imaging 2019, 38, 2642–2653. [Google Scholar] [CrossRef] [PubMed]
- Peng, J.; Kim, D.D.; Patel, J.B.; Zeng, X.; Huang, J.; Chang, K.; Xun, X.; Zhang, C.; Sollee, J.; Wu, J.; et al. Deep learning-based automatic tumor burden assessment of pediatric high-grade gliomas, medulloblastomas, and other leptomeningeal seeding tumors. Neuro-oncology 2022, 24, 289–299. [Google Scholar] [CrossRef] [PubMed]
- Avisdris, N.; Yehuda, B.; Ben-Zvi, O.; Link-Sourani, D.; Ben-Sira, L.; Miller, E.; Zharkov, E.; Ben Bashat, D.; Joskowicz, L. Automatic linear measurements of the fetal brain on MRI with deep neural networks. Int. J. Comput. Assist. Radiol. Surg. 2021, 16, 1481–1492. [Google Scholar] [CrossRef]
- Zhao, L.; Asis-Cruz, J.; Feng, X.; Wu, Y.; Kapse, K.; Largent, A.; Quistorff, J.; Lopez, C.; Wu, D.; Qing, K.; et al. Automated 3D Fetal Brain Segmentation Using an Optimized Deep Learning Approach. Am. J. Neuroradiol. 2022, 43, 448–454. [Google Scholar] [CrossRef]
- Grigorescu, I.; Vanes, L.; Uus, A.; Batalle, D.; Cordero-Grande, L.; Nosarti, C.; Edwards, A.D.; Hajnal, J.V.; Modat, M.; Deprez, M. Harmonized segmentation of neonatal brain MRI. Front. Neurosci. 2021, 15, 662005. [Google Scholar] [CrossRef]
- Li, G.; Chen, M.H.; Li, G.; Wu, D.; Lian, C.; Sun, Q.; Rushmore, R.J.; Wang, L. Volumetric Analysis of Amygdala and Hippocampal Subfields for Infants with Autism. J. Autism Dev. Disord. 2022, 1–15. [Google Scholar] [CrossRef]
- Tor-Diez, C.; Porras, A.R.; Packer, R.J.; Avery, R.A.; Linguraru, M.G. Unsupervised MRI homogenization: Application to pediatric anterior visual pathway segmentation. In Proceedings of the International Workshop on Machine Learning in Medical Imaging 2020, Lima, Peru, 4 October 2020; pp. 180–188. [Google Scholar] [CrossRef]
- Sourati, J.; Gholipour, A.; Dy, J.G.; Kurugol, S.; Warfield, S.K. Active deep learning with fisher information for patch-wise semantic segmentation. In Proceedings of the Deep Learning in Medical Image Analysis and Multimodal Learning for Clinical Decision Support: 4th International Workshop, DLMIA 2018, and 8th International Workshop, ML-CDS 2018, Held in Conjunction with MICCAI 2018, Granada, Spain, 20 September 2018; Springer: Berlin/Heidelberg, Germany, 2018; pp. 83–91. [Google Scholar] [CrossRef]
- Rutherford, S.; Sturmfels, P.; Angstadt, M.; Hect, J.; Wiens, J.; van den Heuvel, M.I.; Scheinost, D.; Sripada, C.; Thomason, M. Automated brain masking of fetal functional MRI with open data. Neuroinformatics 2022, 20, 173–185. [Google Scholar] [CrossRef]
- Ebner, M.; Wang, G.; Li, W.; Aertsen, M.; Patel, P.A.; Aughwane, R.; Melbourne, A.; Doel, T.; Dymarkowski, S.; De Coppi, P.; et al. An automated framework for localization, segmentation and super-resolution reconstruction of fetal brain MRI. NeuroImage 2020, 206, 116324. [Google Scholar] [CrossRef]
- Bermudez, C.; Blaber, J.; Remedios, S.W.; Reynolds, J.E.; Lebel, C.; McHugo, M.; Heckers, S.; Huo, Y.; Landman, B.A. Generalizing deep whole brain segmentation for pediatric and post-contrast MRI with augmented transfer learning. In Proceedings of the Medical Imaging 2020: Image Processing, Houston, TX, USA, 17–20 February 2020; SPIE: Washington, DC, USA, 2020; Volume 11313, pp. 111–118. [Google Scholar]
- Enguehard, J.; O’Halloran, P.; Gholipour, A. Semi-supervised learning with deep embedded clustering for image classification and segmentation. IEEE Access 2019, 7, 11093–11104. [Google Scholar] [CrossRef] [PubMed]
- Khalili, N.; Lessmann, N.; Turk, E.; Claessens, N.; de Heus, R.; Kolk, T.; Viergever, M.A.; Benders, M.J.; Išgum, I. Automatic brain tissue segmentation in fetal MRI using convolutional neural networks. Magn. Reson. Imaging 2019, 64, 77–89. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Parikh, N.A.; Wang, J.; Merhar, S.; Chen, M.; Parikh, M.; Holland, S.; He, L. Objective and automated detection of diffuse white matter abnormality in preterm infants using deep convolutional neural networks. Front. Neurosci. 2019, 13, 610. [Google Scholar] [CrossRef]
- Grimm, F.; Edl, F.; Kerscher, S.R.; Nieselt, K.; Gugel, I.; Schuhmann, M.U. Semantic segmentation of cerebrospinal fluid and brain volume with a convolutional neural network in pediatric hydrocephalus—transfer learning from existing algorithms. Acta Neurochir. 2020, 162, 2463–2474. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.; Zuo, H.; Han, S.; Zhang, X.; Zhang, Q. Computer-Aided Diagnosis of Children with Cerebral Palsy under Deep Learning Convolutional Neural Network Image Segmentation Model Combined with Three-Dimensional Cranial Magnetic Resonance Imaging. J. Healthc. Eng. 2021, 2021, 1822776. [Google Scholar] [CrossRef]
- Uus, A.U.; Ayub, M.U.; Gartner, A.; Kyriakopoulou, V.; Pietsch, M.; Grigorescu, I.; Christiaens, D.; Hutter, J.; Grande, L.C.; Price, A. Segmentation of Periventricular White Matter in Neonatal Brain MRI: Analysis of Brain Maturation in Term and Preterm Cohorts. In Proceedings of the International Workshop on Preterm, Perinatal and Paediatric Image Analysis, Messina, Italy, 13–15 July 2022; Springer: Berlin/Heidelberg, Germany, 2022; pp. 94–104. [Google Scholar]
- Luan, X.; Li, W.; Liu, L.; Shu, Y.; Guo, Y. Rubik-Net: Learning Spatial Information via Rotation-Driven Convolutions for Brain Segmentation. IEEE J. Biomed. Health Inform. 2021, 26, 289–300. [Google Scholar] [CrossRef]
- Quon, J.L.; Chen, L.C.; Kim, L.; Grant, G.A.; Edwards, M.S.; Cheshier, S.H.; Yeom, K.W. Deep learning for automated delineation of pediatric cerebral arteries on pre-operative brain magnetic resonance imaging. Front. Surg. 2020, 7, 89. [Google Scholar] [CrossRef]
- Quon, J.L.; Han, M.; Kim, L.H.; Koran, M.E.; Chen, L.C.; Lee, E.H.; Wright, J.; Ramaswamy, V.; Lober, R.M.; Taylor, M.D.; et al. Artificial intelligence for automatic cerebral ventricle segmentation and volume calculation: A clinical tool for the evaluation of pediatric hydrocephalus. J. Neurosurg. Pediatr. 2020, 27, 131–138. [Google Scholar] [CrossRef]
- Hong, J.; Yun, H.J.; Park, G.; Kim, S.; Laurentys, C.T.; Siqueira, L.C.; Tarui, T.; Rollins, C.K.; Ortinau, C.M.; Grant, P.E.; et al. Fetal cortical plate segmentation using fully convolutional networks with multiple plane aggregation. Front. Neurosci. 2020, 14, 591683. [Google Scholar] [CrossRef]
- Dou, H.; Karimi, D.; Rollins, C.K.; Ortinau, C.M.; Vasung, L.; Velasco-Annis, C.; Ouaalam, A.; Yang, X.; Ni, D.; Gholipour, A. A deep attentive convolutional neural network for automatic cortical plate segmentation in fetal MRI. IEEE Trans. Med. Imaging 2020, 40, 1123–1133. [Google Scholar] [CrossRef] [PubMed]
- Khalili, N.; Turk, E.; Benders, M.; Moeskops, P.; Claessens, N.; de Heus, R.; Franx, A.; Wagenaar, N.; Breur, J.; Viergever, M.; et al. Automatic extraction of the intracranial volume in fetal and neonatal MR scans using convolutional neural networks. Neuroimage Clin. 2019, 24, 102061. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Haghpanah, F.S.; Zhang, X.; Santamaria, K.; da Costa Aguiar Alves, G.K.; Bruno, E.; Aw, N.; Maddocks, A.; Duarte, C.S.; Monk, C.; et al. ID-Seg: An infant deep learning-based segmentation framework to improve limbic structure estimates. Brain Inform. 2022, 9, 12. [Google Scholar] [CrossRef]
- Gruber, N.; Galijasevic, M.; Regodic, M.; Grams, A.E.; Siedentopf, C.; Steiger, R.; Hammerl, M.; Haltmeier, M.; Gizewski, E.R.; Janjic, T. A deep learning pipeline for the automated segmentation of posterior limb of internal capsule in preterm neonates. Artif. Intell. Med. 2022, 132, 102384. [Google Scholar] [CrossRef] [PubMed]
- Park, D.K.; Kim, W.; Thornburg, O.S.; McBrian, D.K.; McKhann, G.M.; Feldstein, N.A.; Maddocks, A.B.; Gonzalez, E.; Shen, M.Y.; Akman, C.; et al. Convolutional neural network-aided tuber segmentation in tuberous sclerosis complex patients correlates with electroencephalogram. Epilepsia 2022, 63, 1530–1541. [Google Scholar] [CrossRef] [PubMed]
- Vafaeikia, P.; Wagner, M.W.; Hawkins, C.; Tabori, U.; Ertl-Wagner, B.B.; Khalvati, F. Improving the segmentation of pediatric low-grade gliomas through multitask learning. In Proceedings of the 2022 44th Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Scotland, UK, 11–15 July 2022; IEEE: Piscataway, NJ, USA, 2022; pp. 2119–2122. [Google Scholar]
- Madhogarhia, R.; Kazerooni, A.F.; Arif, S.; Ware, J.B.; Familiar, A.M.; Vidal, L.; Bagheri, S.; Anderson, H.; Haldar, D.; Yagoda, S. Automated segmentation of pediatric brain tumors based on multi-parametric MRI and deep learning. In Proceedings of the Medical Imaging 2022: Computer-Aided Diagnosis, Leicester, UK, 10 August 2022; SPIE: Washington, DC, USA, 2022; Volume 12033, pp. 723–731. [Google Scholar]
- Hong, J.; Feng, Z.; Wang, S.H.; Peet, A.; Zhang, Y.D.; Sun, Y.; Yang, M. Brain age prediction of children using routine brain MR images via deep learning. Front. Neurol. 2020, 11, 584682. [Google Scholar] [CrossRef]
- Kawaguchi, M.; Kidokoro, H.; Ito, R.; Shiraki, A.; Suzuki, T.; Maki, Y.; Tanaka, M.; Sakaguchi, Y.; Yamamoto, H.; Takahashi, Y.; et al. Age estimates from brain magnetic resonance images of children younger than two years of age using deep learning. Magn. Reson. Imaging 2021, 79, 38–44. [Google Scholar] [CrossRef]
- Niu, X.; Zhang, F.; Kounios, J.; Liang, H. Improved prediction of brain age using multimodal neuroimaging data. Hum. Brain Mapp. 2020, 41, 1626–1643. [Google Scholar] [CrossRef]
- Shabanian, M.; Eckstein, E.C.; Chen, H.; DeVincenzo, J.P. Classification of neurodevelopmental age in normal infants using 3D-CNN based on brain MRI. In Proceedings of the 2019 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), San Diego, CA, USA, 18–21 November 2019; IEEE: Piscataway, NJ, USA, 2019; pp. 2373–2378. [Google Scholar]
- Hu, W.; Cai, B.; Zhang, A.; Calhoun, V.D.; Wang, Y.P. Deep collaborative learning with application to the study of multimodal brain development. IEEE Trans. Biomed. Eng. 2019, 66, 3346–3359. [Google Scholar] [CrossRef]
- Qu, T.; Yue, Y.; Zhang, Q.; Wang, C.; Zhang, Z.; Lu, G.; Du, W.; Li, X. Baenet: A brain age estimation network with 3d skipping and outlier constraint loss. In Proceedings of the 2020 IEEE 17th International Symposium on Biomedical Imaging (ISBI), Iowa City, IA, USA, 3–7 April 2020; IEEE: Piscataway, NJ, USA, 2020; pp. 399–403. [Google Scholar]
- Shabanian, M.; Wenzel, M.; DeVincenzo, J.P. Infant brain age classification: 2D CNN outperforms 3D CNN in small dataset. In Proceedings of the Medical Imaging 2022: Image Processing, San Diego, CA, USA, 20–24 February 2022; SPIE: Washington, DC, USA, 2022; Volume 12032, pp. 626–633. [Google Scholar]
- Wada, A.; Saito, Y.; Fujita, S.; Irie, R.; Akashi, T.; Sano, K.; Kato, S.; Ikenouchi, Y.; Hagiwara, A.; Sato, K.; et al. Automation of a Rule-based Workflow to Estimate Age from Brain MR Imaging of Infants and Children Up to 2 Years Old Using Stacked Deep Learning. Magn. Reson. Med. Sci. 2023, 22, 57–66. [Google Scholar] [CrossRef]
- Hong, J.; Yun, H.J.; Park, G.; Kim, S.; Ou, Y.; Vasung, L.; Rollins, C.K.; Ortinau, C.M.; Takeoka, E.; Akiyama, S.; et al. Optimal method for fetal brain age prediction using multiplanar slices from structural magnetic resonance imaging. Front. Neurosci. 2021, 15, 1284. [Google Scholar] [CrossRef]
- Zhang, Q.; He, Y.; Qu, T.; Yang, F.; Lin, Y.; Hu, Z.; Li, X.; Xu, Q.; Xing, W.; Gumenyuk, V.; et al. Delayed brain development of Rolandic epilepsy profiled by deep learning–based neuroanatomic imaging. Eur. Radiol. 2021, 31, 9628–9637. [Google Scholar] [CrossRef]
- Taoudi-Benchekroun, Y.; Christiaens, D.; Grigorescu, I.; Gale-Grant, O.; Schuh, A.; Pietsch, M.; Chew, A.; Harper, N.; Falconer, S.; Poppe, T.; et al. Predicting age and clinical risk from the neonatal connectome. NeuroImage 2022, 257, 119319. [Google Scholar] [CrossRef]
- Wu, Y.; Besson, P.; Azcona, E.A.; Bandt, S.K.; Parrish, T.B.; Breiter, H.C.; Katsaggelos, A.K. A multicohort geometric deep learning study of age dependent cortical and subcortical morphologic interactions for fluid intelligence prediction. Sci. Rep. 2022, 12, 17760. [Google Scholar] [CrossRef]
- Liu, M.; Zhang, Z.; Dunson, D.B. Graph auto-encoding brain networks with applications to analyzing large-scale brain imaging datasets. Neuroimage 2021, 245, 118750. [Google Scholar] [CrossRef]
- Huang, S.G.; Xia, J.; Xu, L.; Qiu, A. Spatio-temporal directed acyclic graph learning with attention mechanisms on brain functional time series and connectivity. Med. Image Anal. 2022, 77, 102370. [Google Scholar] [CrossRef]
- Saha, S.; Pagnozzi, A.; Bradford, D.; Fripp, J. Predicting fluid intelligence in adolescence from structural MRI with deep learning methods. Intelligence 2021, 88, 101568. [Google Scholar] [CrossRef]
- Li, M.; Jiang, M.; Zhang, G.; Liu, Y.; Zhou, X. Prediction of fluid intelligence from T1-w MRI images: A precise two-step deep learning framework. PLoS ONE 2022, 17, e0268707. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Li, H.; Chen, M.; Wang, J.; Altaye, M.; Dillman, J.R.; Parikh, N.A. Deep multimodal learning from MRI and clinical data for early prediction of neurodevelopmental deficits in very preterm infants. Front. Neurosci. 2021, 15, 753033. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.; Pagnozzi, A.; Bourgeat, P.; George, J.M.; Bradford, D.; Colditz, P.B.; Boyd, R.N.; Rose, S.E.; Fripp, J.; Pannek, K. Predicting motor outcome in preterm infants from very early brain diffusion MRI using a deep learning convolutional neural network (CNN) model. Neuroimage 2020, 215, 116807. [Google Scholar] [CrossRef] [PubMed]
- Han, S.; Zhang, Y.; Ren, Y.; Posner, J.; Yoo, S.; Cha, J. 3D distributed deep learning framework for prediction of human intelligence from brain MRI. In Proceedings of the Medical Imaging 2020: Biomedical Applications in Molecular, Structural, and Functional Imaging, Houston, TX, USA, 18–20 February 2020; SPIE: Washington, DC, USA, 2020; Volume 11317, pp. 484–490. [Google Scholar]
- Jeong, J.W.; Banerjee, S.; Lee, M.H.; O’Hara, N.; Behen, M.; Juhasz, C.; Dong, M. Deep reasoning neural network analysis to predict language deficits from psychometry-driven DWI connectome of young children with persistent language concerns. Hum. Brain Mapp. 2021, 42, 3326–3338. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J.W.; Lee, M.H.; O’Hara, N.; Juhász, C.; Asano, E. Prediction of baseline expressive and receptive language function in children with focal epilepsy using diffusion tractography-based deep learning network. Epilepsy Behav. 2021, 117, 107909. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.; Cho, H.H.; Cho, S.; Park, B.; Hong, J.; Shin, K.; Hwang, M.; You, S.; Lee, S. Accelerated Synthetic MRI with Deep Learning–Based Reconstruction for Pediatric Neuroimaging. Am. J. Neuroradiol. 2022, 43, 1653–1659. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, S.; Perrone, A.; Alexopoulos, D.; Kenley, J.K.; Barch, D.M.; Buss, C.; Elison, J.T.; Graham, A.M.; Neil, J.J.; O’Connor, T.G.; et al. Synthesizing pseudo-T2w images to recapture missing data in neonatal neuroimaging with applications in rs-fMRI. NeuroImage 2022, 253, 119091. [Google Scholar] [CrossRef]
- Sujit, S.J.; Coronado, I.; Kamali, A.; Narayana, P.A.; Gabr, R.E. Automated image quality evaluation of structural brain MRI using an ensemble of deep learning networks. J. Magn. Reson. Imaging 2019, 50, 1260–1267. [Google Scholar] [CrossRef]
- Largent, A.; Kapse, K.; Barnett, S.D.; De Asis-Cruz, J.; Whitehead, M.; Murnick, J.; Zhao, L.; Andersen, N.; Quistorff, J.; Lopez, C.; et al. Image quality assessment of fetal brain MRI using multi-instance deep learning methods. J. Magn. Reson. Imaging 2021, 54, 818–829. [Google Scholar] [CrossRef]
- Ettehadi, N.; Kashyap, P.; Zhang, X.; Wang, Y.; Semanek, D.; Desai, K.; Guo, J.; Posner, J.; Laine, A.F. Automated Multiclass Artifact Detection in Diffusion MRI Volumes via 3D Residual Squeeze-and-Excitation Convolutional Neural Networks. Front. Hum. Neurosci. 2022, 16, 877326. [Google Scholar] [CrossRef]
- Liu, S.; Thung, K.H.; Lin, W.; Yap, P.T.; Shen, D. Real-time quality assessment of pediatric MRI via semi-supervised deep nonlocal residual neural networks. IEEE Trans. Image Process. 2020, 29, 7697–7706. [Google Scholar] [CrossRef]
- Wang, C.; Uh, J.; He, X.; Hua, C.h.; Acharya, S. Transfer learning-based synthetic CT generation for MR-only proton therapy planning in children with pelvic sarcomas. In Proceedings of the Medical Imaging 2021: Physics of Medical Imaging, Online, 5–19 February 2021; SPIE: Washington, DC, USA, 2021; Volume 11595, pp. 1112–1118. [Google Scholar]
- Maspero, M.; Bentvelzen, L.G.; Savenije, M.H.; Guerreiro, F.; Seravalli, E.; Janssens, G.O.; van den Berg, C.A.; Philippens, M.E. Deep learning-based synthetic CT generation for paediatric brain MR-only photon and proton radiotherapy. Radiother. Oncol. 2020, 153, 197–204. [Google Scholar] [CrossRef]
- Zhang, H.; Li, H.; Dillman, J.R.; Parikh, N.A.; He, L. Multi-Contrast MRI Image Synthesis Using Switchable Cycle-Consistent Generative Adversarial Networks. Diagnostics 2022, 12, 816. [Google Scholar] [CrossRef]
- Wang, C.; Uh, J.; Merchant, T.E.; Hua, C.h.; Acharya, S. Facilitating MR-Guided Adaptive Proton Therapy in Children Using Deep Learning-Based Synthetic CT. Int. J. Part. Ther. 2022, 8, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Hales, P.W.; Pfeuffer, J.; A Clark, C. Combined denoising and suppression of transient artifacts in arterial spin labeling MRI using deep learning. J. Magn. Reson. Imaging 2020, 52, 1413–1426. [Google Scholar] [CrossRef]
- Kim, J.; Hong, Y.; Chen, G.; Lin, W.; Yap, P.T.; Shen, D. Graph-based deep learning for prediction of longitudinal infant diffusion MRI data. In Proceedings of the Computational Diffusion MRI: International MICCAI Workshop, Granada, Spain, 22 September 2018; Springer: Berlin/Heidelberg, Germany, 2019; pp. 133–141. [Google Scholar] [CrossRef]
- Karimi, D.; Jaimes, C.; Machado-Rivas, F.; Vasung, L.; Khan, S.; Warfield, S.K.; Gholipour, A. Deep learning-based parameter estimation in fetal diffusion-weighted MRI. Neuroimage 2021, 243, 118482. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Choi, Y.H.; Lee, J.S.; Lee, S.B.; Cho, Y.J.; Lee, S.H.; Shin, S.M.; Cheon, J.E. Deep learning reconstruction in pediatric brain MRI: Comparison of image quality with conventional T2-weighted MRI. Neuroradiology 2022, 65, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Winterburn, J.L.; Voineskos, A.N.; Devenyi, G.A.; Plitman, E.; de la Fuente-Sandoval, C.; Bhagwat, N.; Graff-Guerrero, A.; Knight, J.; Chakravarty, M.M. Can we accurately classify schizophrenia patients from healthy controls using magnetic resonance imaging and machine learning? A multi-method and multi-dataset study. Schizophr. Res. 2019, 214, 3–10. [Google Scholar] [CrossRef]
- Bishop, C.M.; Nasrabadi, N.M. Pattern Recognition and Machine Learning; Springer: Berlin/Heidelberg, Germany, 2006; Volume 4. [Google Scholar]
- Tzourio-Mazoyer, N.; Landeau, B.; Papathanassiou, D.; Crivello, F.; Etard, O.; Delcroix, N.; Mazoyer, B.; Joliot, M. Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. Neuroimage 2002, 15, 273–289. [Google Scholar] [CrossRef]
- Cox, R.W. AFNI: Software for analysis and visualization of functional magnetic resonance neuroimages. Comput. Biomed. Res. 1996, 29, 162–173. [Google Scholar] [CrossRef]
- Avants, B.B.; Tustison, N.; Song, G. Advanced normalization tools (ANTS). Insight J. 2009, 2, 1–35. [Google Scholar]
- Smith, S.M.; Jenkinson, M.; Woolrich, M.W.; Beckmann, C.F.; Behrens, T.E.J.; Johansen-Berg, H.; Bannister, P.R.; De Luca, M.; Drobnjak, I.; Flitney, D.E. Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage 2004, 23, S208–S219. [Google Scholar] [CrossRef]
- Yan, C.G.; Wang, X.D.; Zuo, X.N.; Zang, Y.F. DPABI: Data processing & analysis for (resting-state) brain imaging. Neuroinformatics 2016, 14, 339–351. [Google Scholar] [CrossRef]
- Fischl, B. FreeSurfer. Neuroimage 2012, 62, 774–781. [Google Scholar] [CrossRef] [PubMed]
- Gorgolewski, K.J.; Auer, T.; Calhoun, V.D.; Craddock, R.C.; Das, S.; Duff, E.P.; Flandin, G.; Ghosh, S.S.; Glatard, T.; Halchenko, Y.O.; et al. The brain imaging data structure, a format for organizing and describing outputs of neuroimaging experiments. Sci. Data 2016, 3, 160044. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Ye, Q.; Xia, J. Unbox the black-box for the medical explainable AI via multi-modal and multi-centre data fusion: A mini-review, two showcases and beyond. Inf. Fusion 2022, 77, 29–52. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.; Khosla, A.; Lapedriza, A.; Oliva, A.; Torralba, A. Learning deep features for discriminative localization. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 2921–2929. [Google Scholar] [CrossRef]
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-cam: Visual explanations from deep networks via gradient-based localization. In Proceedings of the IEEE International Conference on Computer Vision, Venice, Italy, 22–29 October 2017; pp. 618–626. [Google Scholar] [CrossRef]
- Guidotti, R.; Monreale, A.; Ruggieri, S.; Turini, F.; Giannotti, F.; Pedreschi, D. A survey of methods for explaining black box models. ACM Comput. Surv. (CSUR) 2018, 51, 1–42. [Google Scholar] [CrossRef]





| Dataset | No. of Sites/Projects | Population | Technique | Citation |
|---|---|---|---|---|
| Autism Brain Imaging Data Exchange I (ABIDE I) | 17 independent imaging sites | 539 subjects with ASD and 573 healthy controls (age 7–64 years) | sMRI, rs-fMRI | [31] |
| Autism Brain Imaging Data Exchange II (ABIDE II) | 19 independent imaging sites | 521 subjects with ASD and 593 healthy controls (age 5–64 years) | sMRI, rs-fMRI, DTI | [32] |
| IMaging-PsychiAtry Challenge (IMPAC) | - | 549 subjects with ASD 601 healthy controls (age 0–80 years) | sMRI, rs-fMRI | [33] |
| ADHD-200 Consortium | 8 independent imaging sites | 285 subjects with ADHD 491 healthy controls (age 7–21 years) | sMRI, rs-fMRI | [34] |
| UK Biobank | - | 500,000 subjects (age 40–69 years) | sMRI, rs-fMRI, DTI | [35] |
| National Database for Autism Research (NDAR) | hundreds of research projects | 117,573 subjects by age (57,510 affected subjects and 59,763 control subjects) | sMRI, rs-fMRI, DTI | [36] |
| Open fMRI | 95 datasets | 3375 subjects across all datasets | sMRI, rs-fMRI, task fMRI | [37] |
| International Consortium for Brain Mapping (ICBM) | - | 853 subjects (age 18–89 years) | sMRI, rs-fMRI, DTI | [38] |
| 1000 funtional connectome | 33 independent imaging sites | 1355 subjects (age 13–80 years) | rs-fMRI | [39] |
| The Adolescent Brain Cognitive Development (ABCD) Study | - | 12,000 subjects (age 9–10 years) | sMRI, rs-fMRI, task fMRI | [40] |
| ENIGMA ADHD working group | 34 cohorts | over 4000 subjects | sMRI, rs-fMRI, DTI | [41] |
| Philadelphia Neurodevelopmental Cohort (PNC) | - | 9500 subjects (age 8–21 years) | sMRI, rs-fMRI, task fMRI, DTI | [42] |
| Healthy Brain Network (HBN) | - | 10,000 subjects (age 5–21 years) | sMRI, rs-fMRI, task fMRI, DTI | [43] |
| Human Connectome Project Development (dHCP) | - | 1350 subjects (age 5–21 years) | sMRI, rs-fMRI, task fMRI | [44] |
| The UNC/UMN Baby Connectome Project (BCP) | 2 sites | 500 subjects (age 0–5 years ) | sMRI, rs-fMRI, DTI | [45] |
| Study | Year | Population | Technique | Preprocessing | Method | Results |
|---|---|---|---|---|---|---|
| [84] | 2017 | 115 infants (gestation age 24–32 weeks ) | DTI | In-house pipeline | CNN | MAE 2.17 weeks |
| [130] | 2019 | 317 MRI images of 112 infants age 2 weeks (8 to 35 days); 12 months (each ±2-weeks) and 3 years (each ±4-weeks). | sMRI | In-house pipeline | 3D CNN | Accuracy 98.4% classifying three age groups |
| [131] | 2019 | PNC Dataset: 857 subject (age 8–22 years) 20% as children 20% as young adult | rs-fMRII | SPM12 | MLP | Accuracy 96.64% predicting children and young adult |
| [132] | 2020 | ABIDE II dataset 382 subjects ADHD200 consortium 378 subjects | sMRI | SPM12 | 3D CNN | MAE 1.11 years (ABIDE II dataset) 1.16 years (ADHD200 consortium) |
| [127] | 2020 | 220 subjects (age 0–5 years) | sMRI | In-house pipeline | CNN | MAE 2.26 months |
| [129] | 2020 | PNC Dataset: 839 subject (age 8–21 years) | sMRI, rs-fMRI, DTI | SPM12, DPARSF, PANDA | MLP | MAE 0.381 ± 0.119 years |
| [128] | 2021 | 161 subjects (age 0–2 years) | sMRI | In-house pipeline | CNN | MAE 8.2 weeks |
| [133] | 2021 | 84 infants (age 8 days–3 years) | sMRI | In-house pipeline | CNN | Accuracy 90% |
| [134] | 2021 | 119 subjects (age 0–2 years) | sMRI | In-house pipeline | CNN | MAE 0.98 months |
| [135] | 2021 | 220 fetuses (gestation age 15.9–38.7 weeks) | sMRI | In-house pipeline | CNN | MAE 0.125 weeks |
| [136] | 2021 | 167 patients with Rolandic epilepsy (age 9.81 ± 2.55 years), 107 HC (age 9.43 ± 2.57 years) | sMRI | CAT12, SPM12 | CNN | MAE 1.05 years for HC 1.21 years for patients |
| [137] | 2022 | 524 infants (gestation age 23–42 weeks ) | sMRI, DTI | Neonatal specific segmentation pipeline | CNN | MAE 0.72 weeks (term-born) 2.21 weeks (preterm) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, M.; Nardi, C.; Zhang, H.; Ang, K.-K. Applications of Deep Learning to Neurodevelopment in Pediatric Imaging: Achievements and Challenges. Appl. Sci. 2023, 13, 2302. https://doi.org/10.3390/app13042302
Hu M, Nardi C, Zhang H, Ang K-K. Applications of Deep Learning to Neurodevelopment in Pediatric Imaging: Achievements and Challenges. Applied Sciences. 2023; 13(4):2302. https://doi.org/10.3390/app13042302
Chicago/Turabian StyleHu, Mengjiao, Cosimo Nardi, Haihong Zhang, and Kai-Keng Ang. 2023. "Applications of Deep Learning to Neurodevelopment in Pediatric Imaging: Achievements and Challenges" Applied Sciences 13, no. 4: 2302. https://doi.org/10.3390/app13042302
APA StyleHu, M., Nardi, C., Zhang, H., & Ang, K.-K. (2023). Applications of Deep Learning to Neurodevelopment in Pediatric Imaging: Achievements and Challenges. Applied Sciences, 13(4), 2302. https://doi.org/10.3390/app13042302