
Clinical Evaluation of a Novel Premixed Tricalcium Silicate Containing Bioceramic Sealer Used with Warm Carrier-Based Technique: A 12-Month Prospective Pilot Study

 ,
,  ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
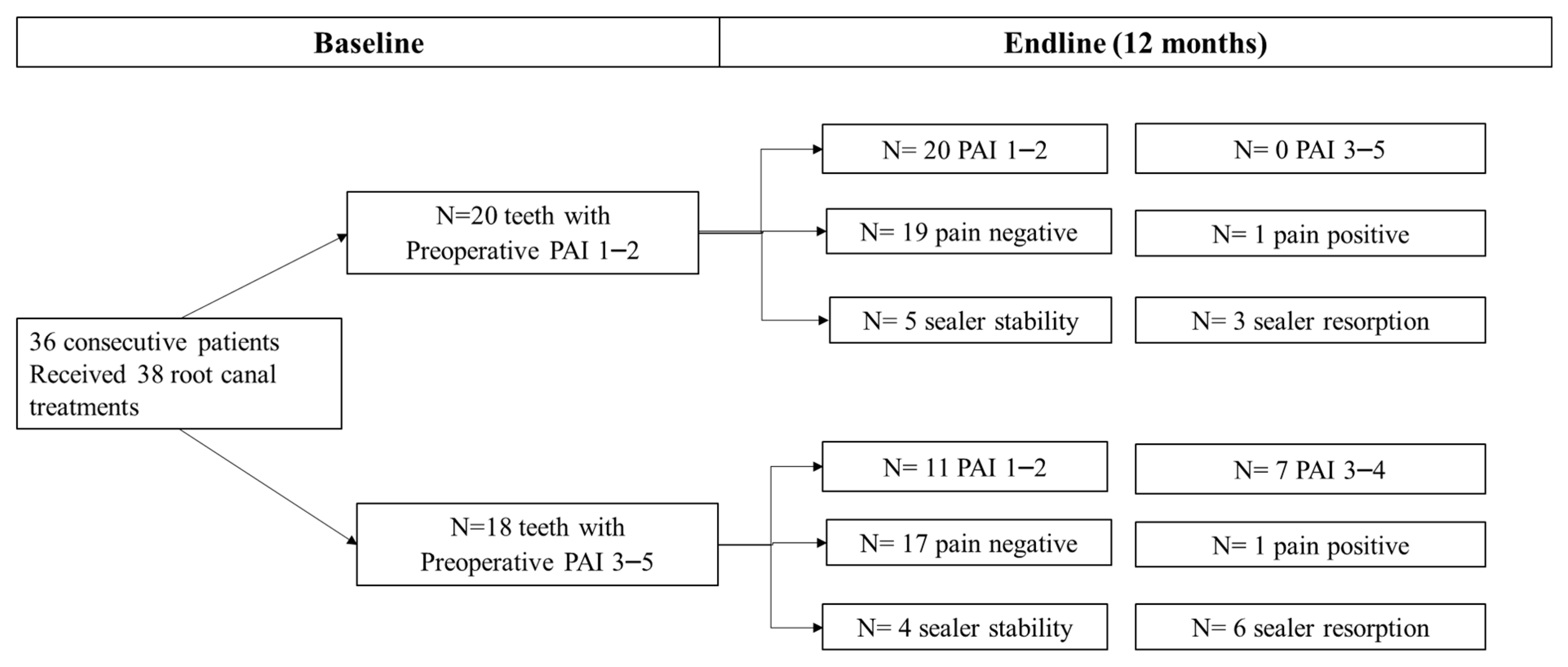
2.1. Study Design and Sample
2.2. Study Population
2.3. Primary Root Canal Treatment
2.4. Secondary Root Canal Treatment
2.5. Root Canal Filling Procedures
2.6. Tooth Restoration
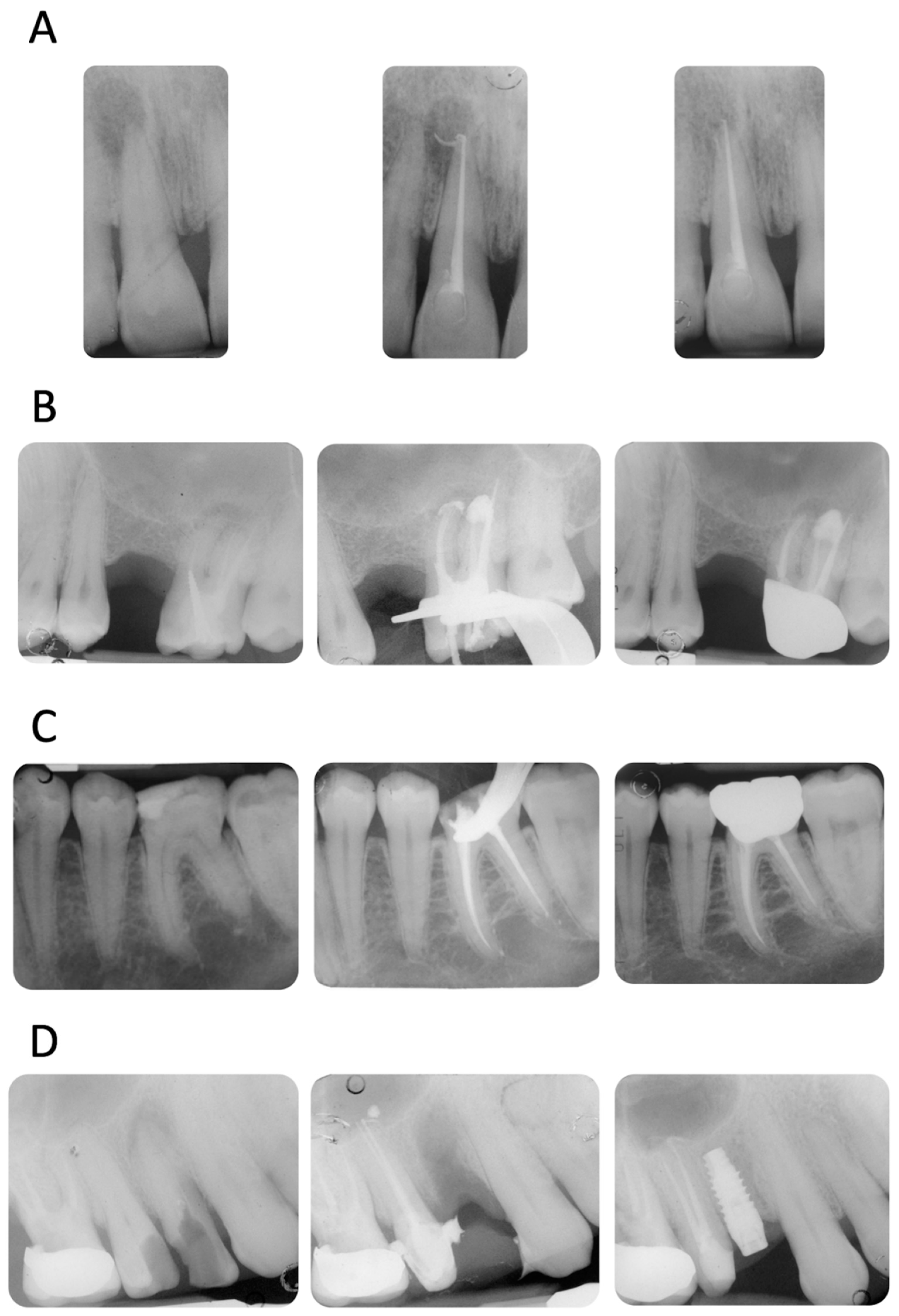
2.7. Radiological Evaluation
2.8. Post-Operative Pain Assessment
2.9. Statistical Methods
3. Results
Demographic Information
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mirfendereski, M.; Roth, K.; Bing, F.; Dubrowski, A.; Carnahan, H.; Azarpazhooh, A.; Basrani, B.; Torneck, C.D.; Friedman, S. Technique acquisition in the use of two thermoplasticized root filling methods by inexperienced dental students: A micro-CT analysis. J. Endod. 2009, 35, 1512–1517. [Google Scholar] [CrossRef] [PubMed]
- Pirani, C.; Zamparini, F.; Peters, O.A.; Iacono, F.; Gatto, M.R.; Generali, L.; Gandolfi, M.G.; Prati, C. The fate of root canals obturated with Thermafil: 10-year data for patients treated in a master program. Clin. Oral Investig. 2019, 23, 3367–3377. [Google Scholar] [CrossRef] [PubMed]
- Hale, R.; Gatti, R.; Glickman, G.N.; Opperman, L.A. Comparative analysis of carrier-based obturation and lateral compaction: A retrospective clinical outcomes study. Int. J. Dent. 2012, 2012, 954675. [Google Scholar] [CrossRef][Green Version]
- Demirci, G.K.; Caliskan, M.K. A prospective randomized comparative study of cold lateral condensation versus Core/Gutta-percha in teeth with periapical lesions. J. Endod. 2016, 42, 206–210. [Google Scholar] [CrossRef]
- Zhou, H.M.; Shen, Y.; Zheng, W.; Li, L.; Zheng, Y.F.; Haapasalo, M. Physical properties of 5 root canal sealers. J. Endod. 2013, 39, 1281–1286. [Google Scholar] [CrossRef]
- Prati, C.; Siboni, F.; Polimeni, A.; Bossu, M.; Gandolfi, M.G. Use of calcium-containing endodontic sealers as apical barrier in fluid-contaminated wide-open apices. J. Appl. Biomater. Funct. Mater. 2014, 12, 263–270. [Google Scholar] [CrossRef]
- Pace, R.; Giuliani, V.; Nieri, M.; Di Nasso, L.; Pagavino, G. Mineral trioxide aggregate as apical plug in teeth with necrotic pulp and immature apices: A 10-year case series. J. Endod. 2014, 40, 1250–1254. [Google Scholar] [CrossRef]
- Sanz, J.L.; López-García, S.; Rodríguez-Lozano, F.J.; Melo, M.; Lozano, A.; Llena, C.; Forner, L. Cytocompatibility and bioactive potential of AH Plus Bioceramic Sealer: An in vitro study. Int. Endod. J. 2022, 55, 1066–1080. [Google Scholar] [CrossRef]
- Chybowski, E.A.; Glickman, G.N.; Patel, Y.; Fleury, A.; Solomon, E.; He, J. Clinical Outcome of Non-Surgical Root Canal Treatment Using a Single-cone Technique with Endosequence Bioceramic Sealer: A Retrospective Analysis. J. Endod. 2018, 44, 941–945. [Google Scholar] [CrossRef]
- Angerame, D.; De Biasi, M.; Pecci, R.; Bedini, R. Filling ability of three variants of the single-cone technique with bioceramic sealer: A micro-computed tomography study. J. Mater. Sci. Mater. Med. 2020, 31, 91. [Google Scholar] [CrossRef]
- Prati, C.; Gandolfi, M.G. Calcium silicate bioactive cements: Biological perspectives and clinical applications. Dent. Mater. 2015, 31, 351–370. [Google Scholar] [CrossRef] [PubMed]
- Gandolfi, M.G.; Perut, F.; Ciapetti, G.; Mongiorgi, R.; Prati, C. New Portland cement-based materials for endodontics mixed with articaine solution: A study of cellular response. J. Endod. 2008, 34, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Gandolfi, M.G.; Siboni, F.; Botero, T.; Bossù, M.; Riccitiello, F.; Prati, C. Calcium silicate and calcium hydroxide materials for pulp capping: Biointeractivity, porosity, solubility and bioactivity of current formulations. J. Appl. Biomater. Funct. Mater. 2015, 13, 43–60. [Google Scholar] [CrossRef] [PubMed]
- Gandolfi, M.G.; Van Landuyt, K.; Taddei, P.; Modena, E.; Van Meerbeek, B.; Prati, C. Environmental scanning electron microscopy connected with energy dispersive x-ray analysis and Raman techniques to study ProRoot mineral trioxide aggregate and calcium silicate cements in wet conditions and in real time. J. Endod. 2010, 36, 851–857. [Google Scholar] [CrossRef]
- Gandolfi, M.G.; Siboni, F.; Primus, C.M.; Prati, C. Ion release, porosity, solubility, and bioactivity of MTA Plus tricalcium silicate. J. Endod. 2014, 40, 1632–1637. [Google Scholar] [CrossRef]
- Primus, C.M.; Tay, F.R.; Niu, L.N. Bioactive tri/dicalcium silicate cements for treatment of pulpal and periapical tissues. Acta Biomater. 2019, 96, 35–54. [Google Scholar] [CrossRef]
- Primus, C.; Gutmann, J.L.; Tay, F.R.; Fuks, A.B. Calcium silicate and calcium aluminate cements for dentistry reviewed. J. Am. Ceram. Soc. 2022, 105, 1841–1863. [Google Scholar] [CrossRef]
- Camilleri, J.; Atmeh, A.; Li, X.; Meschi, N. Present status and future directions: Hydraulic materials for endodontic use. Int. Endod. J. 2022, 55, 710–777. [Google Scholar] [CrossRef]
- Zamparini, F.; Prati, C.; Taddei, P.; Spinelli, A.; Di Foggia, M.; Gandolfi, M.G. Chemical-Physical Properties and Bioactivity of New Premixed Calcium Silicate-Bioceramic Root Canal Sealers. Int. J. Mol. Sci. 2022, 23, 13914. [Google Scholar] [CrossRef]
- Souza, L.C.; Neves, G.S.T.; Kirkpatrick, T.; Letra, A.; Silva, R. Physicochemical and Biological Properties of AH Plus Bioceramic. J. Endod. 2023, 49, 69–76. [Google Scholar] [CrossRef]
- Donnermeyer, D.; Schemkämper, P.; Bürklein, S.; Schäfer, E. Short and Long-Term Solubility, Alkalizing Effect, and Thermal Persistence of Premixed Calcium Silicate-Based Sealers: AH Plus Bioceramic Sealer vs. Total Fill BC Sealer. Materials 2022, 15, 7320. [Google Scholar] [CrossRef] [PubMed]
- Zavattini, A.; Knight, A.; Foschi, F.; Mannocci, F. Outcome of root canal treatments using a new calcium silicate root canal sealer: A non-randomized clinical trial. J. Clin. Med. 2020, 9, 782. [Google Scholar] [CrossRef] [PubMed]
- Zamparini, F.; Spinelli, A.; Cardinali, F.; Ausiello, P.; Gandolfi, M.G.; Prati, C. The Use of Premixed Calcium Silicate Bioceramic Sealer with Warm Carrier-Based Technique: A 2-Year Study for Patients Treated in a Master Program. J. Funct. Biomater. 2023, 14, 164. [Google Scholar] [CrossRef] [PubMed]
- Pontoriero, D.I.K.; Ferrari Cagidiaco, E.; Maccagnola, V.; Manfredini, D.; Ferrari, M. Outcomes of Endodontic-Treated Teeth Obturated with Bioceramic Sealers in Combination with Warm Gutta-Percha Obturation Techniques: A Prospective Clinical Study. J. Clin. Med. 2023, 12, 2867. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. J. Am. Med. Assoc. 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. STROBE Initiative Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Epidemiology 2007, 18, 805–835. [Google Scholar] [CrossRef]
- Dodson, T.B. A guide for preparing a patient-oriented research manuscript. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 104, 307–315. [Google Scholar] [CrossRef]
- Ørstavik, D.; Kerekes, K.; Eriksen, H.M. The periapical index: A scoring system for radiographic assessment of apical periodontitis. Endod. Dent. Traumatol. 1986, 2, 20–34. [Google Scholar] [CrossRef]
- Fonseca, B.; Coelho, M.S.; Bueno, C.E.D.S.; Fontana, C.E.; Martin, A.S.; Rocha, D.G.P. Assessment of Extrusion and Postoperative Pain of a Bioceramic and Resin-Based Root Canal Sealer. Eur. J. Dent. 2019, 13, 343–348. [Google Scholar] [CrossRef]
- Barnard, G.A. A new test for 2 × 2 tables. Nature 1945, 156, 177. [Google Scholar] [CrossRef]
- Lydersen, S.; Fagerland, M.W.; Laake, P. Recommended tests for association in 2 × 2 tables. Stat. Med. 2009, 28, 1159–1175. [Google Scholar] [CrossRef] [PubMed]
- Brown, L.D.; Cai, T.T.; Das Gupta, A. Interval estimation for a binomial proportion. Stat. Sci. 2001, 16, 101–133. [Google Scholar] [CrossRef]
- Calhoun, P. Exact: Unconditional Exact Test. R Package Version 3.2, 2022. Available online: https://CRAN.R-project.org/package=Exact (accessed on 18 October 2023).
- Donnermeyer, D.; Schäfer, E.; Bürklein, S. Real-time Intracanal Temperature Measurement during Different Obturation Techniques. J. Endod. 2018, 44, 1832–1836. [Google Scholar] [CrossRef]
- European Society of Endodontology. Quality guidelines for endodontic treatment: Consensus report of the European Society of Endodontology. Int. Endod. J. 2006, 39, 921–930. [Google Scholar] [CrossRef] [PubMed]
- Ricucci, D.; Rôças, I.N.; Alves, F.R.; Loghin, S.; Siqueira, J.F., Jr. Apically Extruded Sealers: Fate and Influence on Treatment Outcome. J. Endod. 2016, 42, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Martins, J.F.B.; Scheeren, B.; van der Waal, S.V. The Effect of Unintentional AH-Plus Sealer Extrusion on Resolution of Apical Periodontitis After Root Canal Treatment and Retreatment-A Retrospective Case-control Study. J. Endod. 2023, 49, 1262–1268. [Google Scholar] [CrossRef] [PubMed]
- Aminoshariae, A.; Kulild, J.C. The impact of sealer extrusion on endodontic outcome: A systematic review with meta-analysis. Aust. Endod. J. 2020, 46, 123–129. [Google Scholar] [CrossRef]
- Gandolfi, M.G.; Iezzi, G.; Piattelli, A.; Prati, C.; Scarano, A. Osteoinductive potential and bone-bonding ability of ProRoot MTA, MTA Plus and Biodentine in rabbit intramedullary model: Microchemical characterization and histological analysis. Dent. Mater. 2017, 33, 221–238. [Google Scholar] [CrossRef]
- Geurtsen, W.; Leyhausen, G. Biological aspects of root canal filling materials--histocompatibility, cytotoxicity, and mutagenicity. Clin. Oral. Investig. 1997, 1, 5–11. [Google Scholar] [CrossRef]
- Von Arx, T. Mineral Trioxide Aggregate (MTA) a success story in apical surgery. Swiss. Dent. J. 2016, 126, 573–595. [Google Scholar]
- Giacomino, C.M.; Wealleans, J.A.; Kuhn, N.; Diogenes, A. Comparative Biocompatibility and Osteogenic Potential of Two Bioceramic Sealers. J. Endod. 2019, 45, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Tay, F.R.; Pashley, D.H.; Rueggeberg, F.A.; Loushine, R.J.; Weller, R.N. Calcium phosphate phase transformation produced by the interaction of the portland cement component of white mineral trioxide aggregate with a phosphate-containing fluid. J. Endod. 2007, 33, 1347–1351. [Google Scholar] [CrossRef] [PubMed]
- Tay, F.R.; Pashley, D.H. Guided tissue remineralisation of partially demineralised human dentine. Biomaterials 2008, 29, 1127–1137. [Google Scholar] [CrossRef] [PubMed]
- Mekhdieva, E.; Del Fabbro, M.; Alovisi, M.; Comba, A.; Scotti, N.; Tumedei, M.; Carossa, M.; Berutti, E.; Pasqualini, D. Postoperative Pain following Root Canal Filling with Bioceramic vs. Traditional Filling Techniques: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2021, 10, 4509. [Google Scholar] [CrossRef] [PubMed]
- Drumond, J.P.S.C.; Maeda, W.; Nascimento, W.M.; Campos, D.L.; Prado, M.C.; de-Jesus-Soares, A.; Frozoni, M. Comparison of Postobturation Pain Experience after Apical Extrusion of Calcium Silicate- and Resin-Based Root Canal Sealers. J. Endod. 2021, 47, 1278–1284. [Google Scholar] [CrossRef] [PubMed]
- Buonavoglia, A.; Zamparini, F.; Lanave, G.; Pellegrini, F.; Diakoudi, G.; Spinelli, A.; Lucente, M.S.; Camero, M.; Vasinioti, V.I.; Gandolfi, M.G.; et al. Endodontic Microbial Communities in Apical Periodontitis. J. Endod. 2023, 49, 178–189. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| (a) |
| 1. Age 18–75 years |
| 2. Healthy status (ASA 1 or 2) |
| 3. At least one tooth affected by endodontic pathology (pulpitis, pulp necrosis, re-exacerbated lesions with a previous root canal treatment) |
| (b) |
| 1. Teeth with less than 2 walls of crown structural integrity |
| 2. Teeth used as abutments for fixed rehabilitation |
| 3. Presence of active periodontal disease (PPD > 4 mm, general BoP > 25% of the sites) |
| 4. Wide apexes (>40 diameters) or absence of radiographic pulp chamber |
| 5. Any systemic pathology that could compromise bone healing or the immune response (i.e., diabetes) |
| 6. Pregnancy or breastfeeding |
| 7. Heavy smoking (>15 cigarettes/day) |
| 8. Exposure to radiation therapy focused on the head and neck region and malignant disease directly involving the jaws. |
| 9. Lack of occlusal contacts |
| Characteristic | All (n = 38) |
|---|---|
| Sex | |
| Male | 16 (42%) |
| Female | 22 (58%) |
| Age group | |
| <30 | 6 (16%) |
| 30–54 | 17 (45%) |
| ≥55 | 15 (39%) |
| Tooth type | |
| Anterior | 6 (16%) |
| Premolar | 14 (37%) |
| Molar | 18 (47%) |
| Tooth location | |
| Maxilla | 26 (68%) |
| Mandible | 12 (32%) |
| Diagnosis | |
| Pulpitis | 20 (53%) |
| Pulp necrosis | 8 (21%) |
| Re-exacerbated lesion | 10 (26%) |
| Baseline PAI | |
| 1–2 | 20 (53%) |
| ≥3 | 18 (47%) |
| Endodontic treatment | |
| Root canal treatment | 28 (74%) |
| Re-treatment | 10 (26%) |
| Obturation | |
| Underfilled | 4 (11%) |
| Adequate filling | 30 (79%) |
| Overfilled | 4 (11%) |
| Extrusion | |
| No | 20 (53%) |
| Yes | 18 (47%) |
| Extrusion, mm | |
| No extrusion | 20 (53%) |
| 0.1–2.0 | 9 (24%) |
| 2.1–5.0 | 6 (16%) |
| >5.0 | 3 (8%) |
| Sealer Resorption * | |
| No | 9 (50%) |
| Yes | 9 (50%) |
| (a) | ||||
| Characteristic | Healed | Healing | Diff. in % s | p-Value |
| (n = 31) | (n = 7) | (95% CI) | ||
| Sex | ||||
| Male | 13 (42%) | 3 (43%) | ||
| Female | 18 (58%) | 4 (57%) | +1 (−31, +38) | 0.840 |
| Age group | ||||
| <30 | 5 (16%) | 1 (14%) | +2 (−36, +24) | 0.923 |
| 30–54 | 13 (42%) | 4 (57%) | −15 (−47, +22) | 0.550 |
| ≥55 | 13 (42%) | 2 (29%) | +13 (−28, +41) | 0.497 |
| Tooth type | ||||
| Anterior | 3 (10%) | 3 (43%) | −33 (−65, −3) | 0.029 * |
| Premolar | 13 (42%) | 1 (14%) | +28 (−13, +50) | 0.202 |
| Molar | 15 (48%) | 3 (43%) | +5 (−32, +37) | 1.000 |
| Tooth location | ||||
| Maxilla | 22 (71%) | 4 (57%) | ||
| Mandible | 9 (29%) | 3 (43%) | −14 (−18, +48) | 0.529 |
| Diagnosis | ||||
| Pulpitis | 18 (58%) | 2 (29%) | +29 (−12, +57) | 0.185 |
| Pulp necrosis | 4 (13%) | 4 (57%) | −44 (−73, −9) | 0.012 * |
| Re-exacerbated lesion | 9 (29%) | 1 (14%) | +15 (−25, +36) | 0.472 |
| Baseline PAI | ||||
| 1–2 | 20 (65%) | 0 (0.0%) | ||
| ≥3 | 11 (35%) | 7 (100%) | −65 (−79, −25) | 0.001 * |
| Endodontic treatment | ||||
| Root canal treatment | 22 (71%) | 6 (86%) | ||
| Re-treatment | 9 (29%) | 1 (14%) | +15 (−25, +36) | 0.472 |
| (b) | ||||
| Characteristic | Healed | Healing | Diff. in % s | p-Value |
| (n = 31) | (n = 7) | (95% CI) | ||
| Obturation | ||||
| Underfilled | 4 (13%) | 0 (0%) | +13 (−22, +27) | 0.604 |
| Adequate | 24 (77%) | 6 (86%) | −9 (−30, +31) | 0.757 |
| Overfilled | 3 (10%) | 1 (14%) | −4 (−41, +15) | 0.439 |
| Sealer Extrusion | ||||
| No | 17 (55%) | 3 (43%) | ||
| Yes | 14 (45%) | 4 (57%) | −12 (−44, +25) | 0.623 |
| Sealer Extrusion, mm | ||||
| No extrusion | 17 (55%) | 3 (43%) | +12 (−25, +44) | 0.623 |
| 0.1–2.0 | 8 (26%) | 1 (14%) | +12 (−28, +33) | 0.630 |
| 2.1–5.0 | 4 (13%) | 2 (29%) | −16 (−53, +10) | 0.221 |
| >5.0 | 2 (6%) | 1 (14%) | −8 (−44, +11) | 0.285 |
| Sealer Resorption † | ||||
| No | 8 (57%) | 1 (25%) | ||
| Yes | 6 (43%) | 3 (75%) | −32 (−67, +19) | 0.333 |
| Characteristics | All | Healed | Healing | Diff. in %s | p-Value |
|---|---|---|---|---|---|
| (n = 38) | (n = 31) | (n = 7) | (95% CI) | ||
| One-day pain | |||||
| No | 32 (84%) | 28 (90%) | 4 (57%) | ||
| Yes † | 6 (16%) | 3 (10%) | 3 (43%) | −33 (−65, −3) | 0.029 * |
| One-week pain | |||||
| No | 34 (89%) | 30 (97%) | 4 (57%) | ||
| Yes † | 4 (11%) | 1 (3%) | 3 (43%) | −40 (−72, −11) | 0.007 * |
| One-month pain | |||||
| No | 34 (89%) | 30 (97%) | 4 (57%) | ||
| Yes † | 4 (11%) | 1 (3%) | 3 (43%) | −40 (−72, −11) | 0.007 * |
| Twelve-month pain | |||||
| No | 36 (95%) | 31 (100%) | 5 (71%) | ||
| Yes † | 2 (5%) | 0 (0%) | 2 (29%) | −29 (−66, −5) | 0.011 * |
| No Pain (0) | Mild (1–2) | Moderate (3–7) | Severe (8–10) | |
|---|---|---|---|---|
| One day | 32 (84%) | 3 (8%) | 3 (8%) | 0 (0%) |
| One week | 34 (89%) | 4 (11%) | 0 (0%) | 0 (0%) |
| One month | 34 (89%) | 4 (11%) | 0 (0%) | 0 (0%) |
| Twelve months | 36 (95%) | 2 (5%) | 0 (0%) | 0 (0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spinelli, A.; Zamparini, F.; Lenzi, J.; Gandolfi, M.G.; Prati, C. Clinical Evaluation of a Novel Premixed Tricalcium Silicate Containing Bioceramic Sealer Used with Warm Carrier-Based Technique: A 12-Month Prospective Pilot Study. Appl. Sci. 2023, 13, 11835. https://doi.org/10.3390/app132111835
Spinelli A, Zamparini F, Lenzi J, Gandolfi MG, Prati C. Clinical Evaluation of a Novel Premixed Tricalcium Silicate Containing Bioceramic Sealer Used with Warm Carrier-Based Technique: A 12-Month Prospective Pilot Study. Applied Sciences. 2023; 13(21):11835. https://doi.org/10.3390/app132111835
Chicago/Turabian StyleSpinelli, Andrea, Fausto Zamparini, Jacopo Lenzi, Maria Giovanna Gandolfi, and Carlo Prati. 2023. "Clinical Evaluation of a Novel Premixed Tricalcium Silicate Containing Bioceramic Sealer Used with Warm Carrier-Based Technique: A 12-Month Prospective Pilot Study" Applied Sciences 13, no. 21: 11835. https://doi.org/10.3390/app132111835
APA StyleSpinelli, A., Zamparini, F., Lenzi, J., Gandolfi, M. G., & Prati, C. (2023). Clinical Evaluation of a Novel Premixed Tricalcium Silicate Containing Bioceramic Sealer Used with Warm Carrier-Based Technique: A 12-Month Prospective Pilot Study. Applied Sciences, 13(21), 11835. https://doi.org/10.3390/app132111835