


Optimizing Adhesive Bonding to Caries Affected Dentin: A Comprehensive Systematic Review and Meta-Analysis of Dental Adhesive Strategies following Chemo-Mechanical Caries Removal


Abstract
1. Introduction
2. Materials and Methods
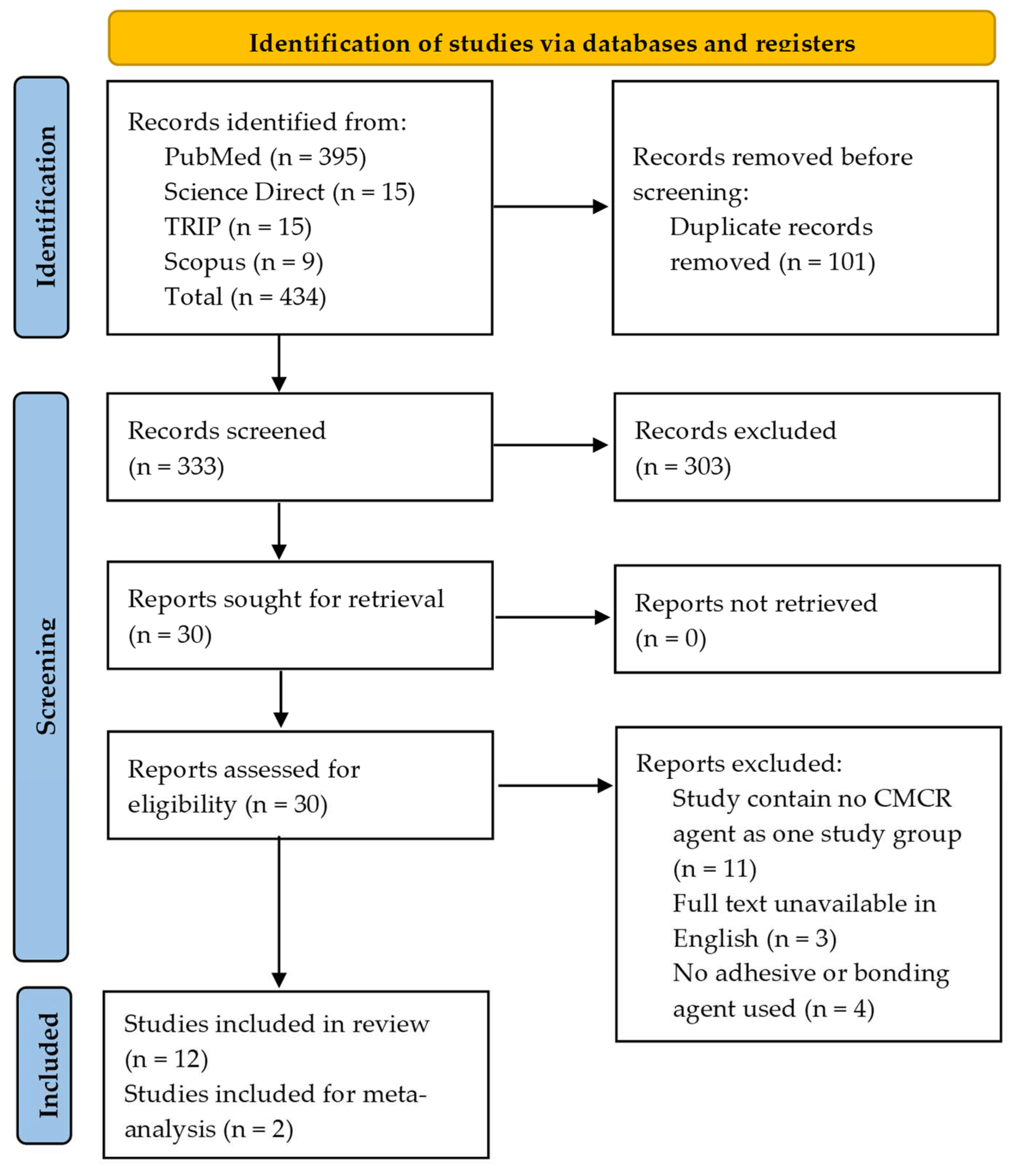
2.1. Search Strategy
2.2. Selection of Studies
2.3. Data Extraction
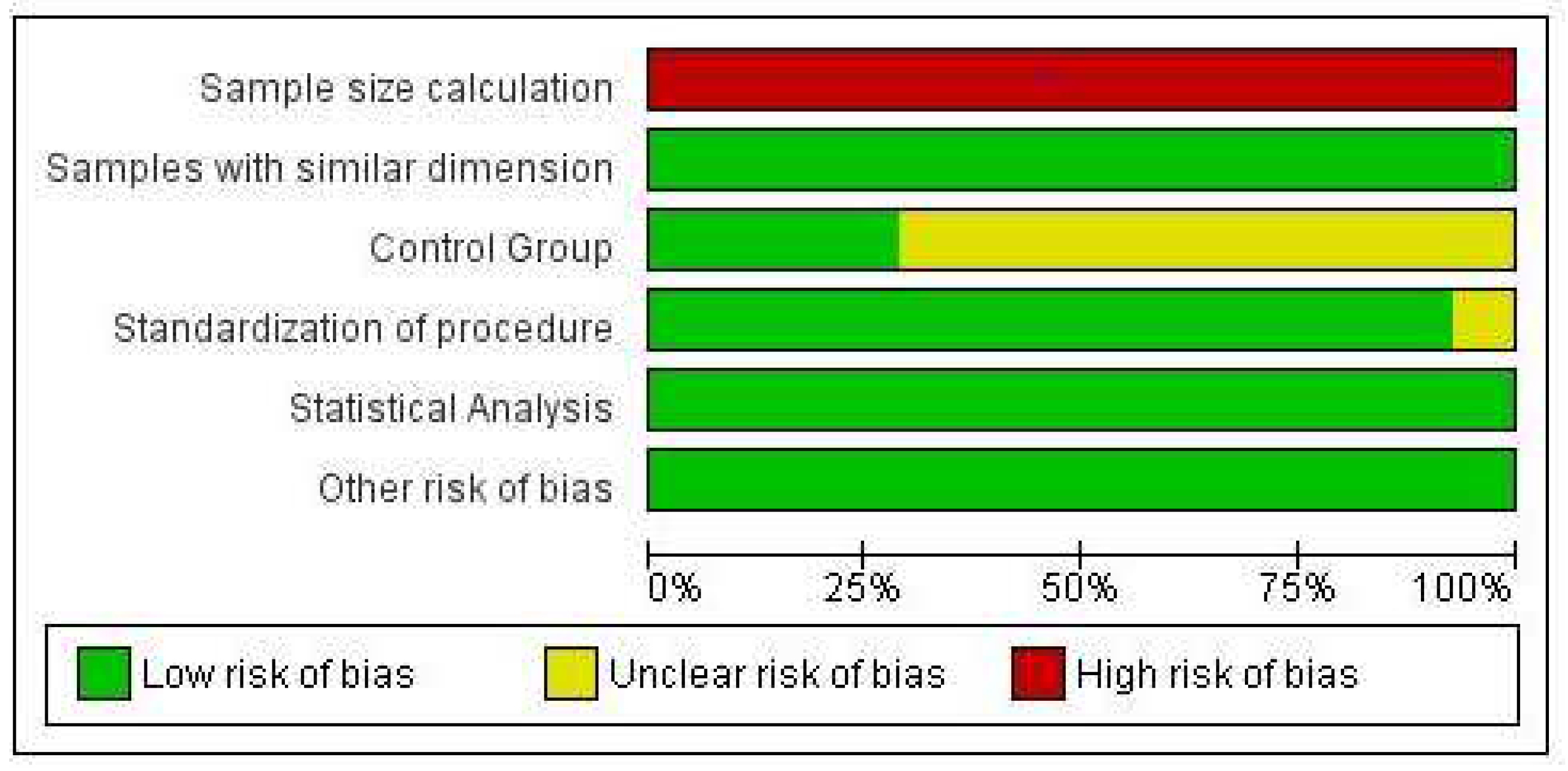
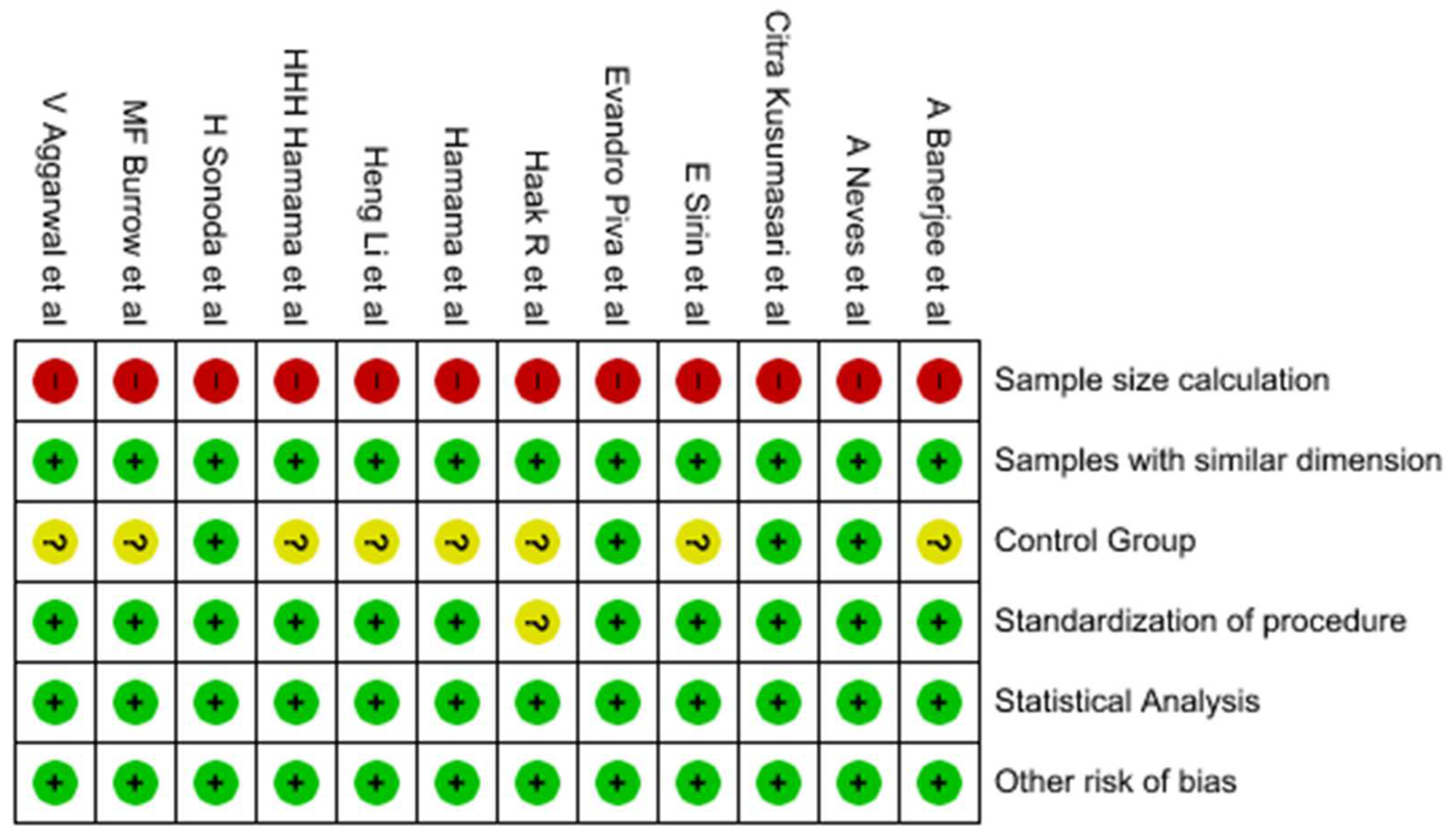
2.4. Assessment of Risk of Bias
2.5. Data Analysis
3. Results
3.1. Characteristics of Included Studies
3.2. Quality Assessment of Included Studies
3.3. Meta-Analysis
4. Discussion
5. Conclusions
- The use of chemo-mechanical caries removal agents did not significantly affect the bond strength of dental adhesives to caries-affected dentin;
- Two-step self-etch adhesives exhibited higher bond strength compared to etch-and-rinse adhesives when applied on caries-affected dentin. Unlike ER, which destroys collagen fibrils, SE preserves the collagen fibrils and hence superior performance;
- Both Carisolv and Papacarie showed corresponding bond strength to dentin when utilized in conjunction with self-etch dental adhesives.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fejerskov, O. Concepts of Dental Caries and Their Consequences for Understanding the Disease. Community Dent. Oral. Epidemiol. 1997, 25, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Pitts, N.B.; Zero, D.T.; Marsh, P.D.; Ekstrand, K.; Weintraub, J.A.; Ramos-Gomez, F.; Tagami, J.; Twetman, S.; Tsakos, G.; Ismail, A. Dental Caries. Nat. Rev. Dis. Prim. 2017, 3, 17030. [Google Scholar] [CrossRef] [PubMed]
- Butera, A.; Maiorani, C.; Morandini, A.; Simonini, M.; Morittu, S.; Trombini, J.; Scribante, A. Evaluation of Children Caries Risk Factors: A Narrative Review of Nutritional Aspects, Oral Hygiene Habits, and Bacterial Alterations. Children 2022, 9, 262. [Google Scholar] [CrossRef] [PubMed]
- Pierce, A.; Singh, S.; Lee, J.; Grant, C.; Cruz de Jesus, V.; Schroth, R.J. The Burden of Early Childhood Caries in Canadian Children and Associated Risk Factors. Front. Public Health 2019, 7, 328. [Google Scholar] [CrossRef] [PubMed]
- Benn, A.M.L.; Heng, N.C.K.; Thomson, W.M.; Broadbent, J.M. Plaque and Dental Caries Risk in Midlife. Caries Res. 2022, 56, 464–476. [Google Scholar] [CrossRef]
- Sonoda, H.; Banerjee, A.; Sherriff, M.; Tagami, J.; Watson, T.F. An in Vitro Investigation of Microtensile Bond Strengths of Two Dentine Adhesives to Caries-Affected Dentine. J. Dent. 2005, 33, 335–342. [Google Scholar] [CrossRef]
- Meraji, N.; Nekoofar, M.H.; Yazdi, K.A.; Sharifian, M.R.; Fakhari, N.; Camilleri, J. Bonding to Caries Affected Dentine. Dent. Mater. 2018, 34, e236–e245. [Google Scholar] [CrossRef]
- Nakajima, M.; Kunawarote, S.; Prasansuttiporn, T.; Tagami, J. Bonding to Caries-Affected Dentin. Jpn. Dent. Sci. Rev. 2011, 47, 102–114. [Google Scholar] [CrossRef]
- Burrow, M.F.; Bokas, J.; Tanumiharja, M.; Tyas, M.J. Microtensile Bond Strengths to Caries-Affected Dentine Treated with Carisolv. Aust. Dent. J. 2003, 48, 110–114. [Google Scholar] [CrossRef]
- Reddy, M.V.; Sai Shankar, A.; Pentakota, V.; Kolli, H.; Ganta, H.; Katari, P. Efficacy of Antimicrobial Property of Two Commercially Available Chemomechanical Caries Removal Agents (Carisolv and Papacarie): An Ex Vivo Study. J. Int. Soc. Prev. Community Dent. 2015, 5, 183. [Google Scholar] [CrossRef]
- Murdoch-Kinch, C.A.; McLEAN, M.E. Minimally Invasive Dentistry. J. Am. Dent. Assoc. 2003, 134, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Jingarwar, M.M.; Bajwa, N.K.; Pathak, A. Minimal Intervention Dentistry—A New Frontier in Clinical Dentistry. J. Clin. Diagn. Res. 2014, 8, ZE04–ZE08. [Google Scholar] [CrossRef]
- Naik, S.V.; Shashikiran, N.D.; Chaitra, N.L.; Syed, G. A Microtensile Bond Strength Evaluation of a Single-Bottle Adhesive to Caries-Affected Dentin in Conventional versus Minimal Invasive Caries Removal Techniques: An in-Vitro Study. Indian J. Dent. 2014, 5, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Showkat, N.; Singh, G.; Singla, K.; Sareen, K.; Chowdhury, C.; Jindal, L. Minimal Invasive Dentistry: Literature Review. J. Curr. Med. Res. Opin. 2020, 3, 631–636. [Google Scholar] [CrossRef]
- Ajai Minimally Invasive Dentistry—A Review. Available online: https://www.ijcommdent.com/article.asp?issn=2589-8388;year=2021;volume=9;issue=2;spage=97;epage=99;aulast=Ajai (accessed on 7 June 2023).
- Çehreli, Z.C.; Yazici, A.R.; Akca, T.; Özgünaltay, G. A Morphological and Micro-Tensile Bond Strength Evaluation of a Single-Bottle Adhesive to Caries-Affected Human Dentine after Four Different Caries Removal Techniques. J. Dent. 2003, 31, 429–435. [Google Scholar] [CrossRef]
- Bussadori, S.K.; de Godoy, C.H.L.; Alfaya, T.A.; Fernandes, K.P.S.; Mesquita-Ferrari, R.A.; Motta, L.J. Chemo-Mechanical Caries Removal with PapacarieTM: Case Series with 84 Reports and 12 Months of Follow-Up. J. Contemp. Dent. Pract. 2014, 15, 250–253. [Google Scholar] [CrossRef]
- Ganesh, M.; Parikh, D. Chemomechanical Caries Removal (CMCR) Agents: Review and Clinical Application in Primary Teeth. J. Dent. Oral Hyg. 2011, 3, 34–45. [Google Scholar]
- Singhal, P.; Vishwanathan, D.; Das, U.; Singhal, A. Carisolv as an Endodontic Irrigant in Deciduous Teeth: An SEM Study. Indian J. Dent. Res. 2012, 23, 120. [Google Scholar] [CrossRef]
- Motta, L.J.; Bussadori, S.K.; Campanelli, A.P.; da Silva, A.L.; Alfaya, T.A.; de Godoy, C.H.L.; de Lima Navarro, M.F. Efficacy of Papacarie® in Reduction of Residual Bacteria in Deciduous Teeth: A Randomized, Controlled Clinical Trial. Clinics 2014, 69, 319–322. [Google Scholar] [CrossRef]
- Maashi, M.S.; Elkhodary, H.M.; Alamoudi, N.M.; Bamashmous, N.O. Chemomechanical Caries Removal Methods: A Literature Review. Saudi Dent. J. 2023, 35, 233–243. [Google Scholar] [CrossRef]
- Perdigão, J.; Araujo, E.; Ramos, R.Q.; Gomes, G.; Pizzolotto, L. Adhesive Dentistry: Current Concepts and Clinical Considerations. J. Esthet. Restor. Dent. 2021, 33, 51–68. [Google Scholar] [CrossRef] [PubMed]
- Sofan, E.; Sofan, A.; Palaia, G.; Tenore, G.; Romeo, U.; Migliau, G. Classification Review of Dental Adhesive Systems: From the IV Generation to the Universal Type. Ann. Stomatol. 2017, 8, 1–17. [Google Scholar] [CrossRef]
- Breschi, L.; Maravic, T.; Cunha, S.R.; Comba, A.; Cadenaro, M.; Tjäderhane, L.; Pashley, D.H.; Tay, F.R.; Mazzoni, A. Dentin Bonding Systems: From Dentin Collagen Structure to Bond Preservation and Clinical Applications. Dent. Mater. 2018, 34, 78–96. [Google Scholar] [CrossRef] [PubMed]
- Murali, N.; Ganesh.S, B.; Roy, A. Self Etch Adhesives—An Update. Int. J. Res. Pharm. Sci. 2020, 11, 464–468. [Google Scholar] [CrossRef]
- Manihani, A.K.D.S.; Mulay, S.; Beri, L.; Shetty, R.; Gulati, S.; Dalsania, R. Effect of Total-Etch and Self-Etch Adhesives on the Bond Strength of Composite to Glass-Ionomer Cement/Resin-Modified Glass-Ionomer Cement in the Sandwich Technique—A Systematic Review. Dent. Res. J. 2021, 18, 72. [Google Scholar]
- Digole, V.R.; Warhadpande, M.M.; Dua, P.; Dakshindas, D. Comparative Evaluation of Clinical Performance of Two Self-Etch Adhesive Systems with Total-Etch Adhesive System in Noncarious Cervical Lesions: An in Vivo Study. J. Conserv. Dent. 2020, 23, 190–195. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Faggion, C.M. Guidelines for Reporting Pre-Clinical In Vitro Studies on Dental Materials. J. Evid. Based Dent. Pract. 2012, 12, 182–189. [Google Scholar] [CrossRef]
- Li, H.; Wang, W.-M.; Yu, S.-L.; Wen, Q. Morphological and Microtensile Bond Strength Evaluation of Three Adhesive Systems to Caries-Affected Human Dentine with Chemomechanical Caries Removal. J. Dent. 2011, 39, 332–339. [Google Scholar] [CrossRef]
- Kusumasari, C.; Abdou, A.; Nakajima, M.; Tagami, J. Deproteinization of Caries-Affected Dentin with Chemo-Mechanical Caries Removal Agents and Its Effect on Dentin Bonding with Self-Etch Adhesives. J. Dent. 2021, 109, 103665. [Google Scholar] [CrossRef]
- Hamama, H.; Yiu, C.; Burrow, M.F. Effect of Chemomechanical Caries Removal on Bonding of Resin-Modified Glass Ionomer Cement Adhesives to Caries-Affected Dentine. Aust. Dent. J. 2015, 60, 190–199. [Google Scholar] [CrossRef] [PubMed]
- Hamama, H.H.H.; Yiu, C.K.Y.; Burrow, M.F. Effect of Chemomechanical Caries Removal on Bonding of Self-Etching Adhesives to Caries-Affected Dentin. J. Adhes. Dent. 2014, 16, 507–516. [Google Scholar] [CrossRef]
- Aggarwal, V.; Singla, M.; Yadav, S.; Yadav, H. The Effect of Caries Excavation Methods on the Bond Strength of Etch-and-Rinse and Self-Etch Adhesives to Caries Affected Dentine. Aust. Dent. J. 2013, 58, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Sirin Karaarslan, E.; Yildiz, E.; Cebe, M.A.; Yegin, Z.; Ozturk, B. Evaluation of Micro-Tensile Bond Strength of Caries-Affected Human Dentine after Three Different Caries Removal Techniques. J. Dent. 2012, 40, 793–801. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, A.; Kellow, S.; Mannocci, F.; Cook, R.J.; Watson, T.F. An in Vitro Evaluation of Microtensile Bond Strengths of Two Adhesive Bonding Agents to Residual Dentine after Caries Removal Using Three Excavation Techniques. J. Dent. 2010, 38, 480–489. [Google Scholar] [CrossRef] [PubMed]
- Haak, R.; Wicht, M.J.; Noack, M.J. Does Chemomechanical Caries Removal Affect Dentine Adhesion? Eur. J. Oral Sci. 2000, 108, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Neves, A.d.A.; Coutinho, E.; Cardoso, M.V.; de Munck, J.; Van Meerbeek, B. Micro-Tensile Bond Strength and Interfacial Characterization of an Adhesive Bonded to Dentin Prepared by Contemporary Caries-Excavation Techniques. Dent. Mater. 2011, 27, 552–562. [Google Scholar] [CrossRef] [PubMed]
- Piva, E.; Ogliari, F.A.; de Moraes, R.R.; Corá, F.; Henn, S.; Correr-Sobrinho, L. Papain-Based Gel for Biochemical Caries Removal: Influence on Microtensile Bond Strength to Dentin. Braz. Oral Res. 2008, 22, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Meharry, M.; Moazzami, S.; Li, Y. Comparison of Enamel and Dentin Shear Bond Strengths of Current Dental Bonding Adhesives from Three Bond Generations. Oper. Dent. 2013, 38, E237–E245. [Google Scholar] [CrossRef]
- Reis, A.F.; Giannini, M.; Kavaguchi, A.; Soares, C.J.; Line, S.R.P. Comparison of Microtensile Bond Strength to Enamel and Dentin of Human, Bovine, and Porcine Teeth. J. Adhes. Dent. 2004, 6, 117–121. [Google Scholar]
- Bedran-Russo, A.; Leme-Kraus, A.A.; Vidal, C.M.P.; Teixeira, E.C. An Overview of Dental Adhesive Systems and the Dynamic Tooth–Adhesive Interface. Dent. Clin. N. Am. 2017, 61, 713–731. [Google Scholar] [CrossRef]
- Goldberg, M. Dentin Structure Composition and Mineralization. Front. Biosci. 2011, E3, 281. [Google Scholar] [CrossRef]
- Isolan, C.P.; Sarkis-Onofre, R.; Lima, G.S.; Moraes, R.R. Bonding to Sound and Caries-Affected Dentin: A Systematic Review and Meta-Analysis. J. Adhes. Dent. 2018, 20, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Pinna, R.; Maioli, M.; Eramo, S.; Mura, I.; Milia, E. Carious Affected Dentine: Its Behaviour in Adhesive Bonding. Aust. Dent. J. 2015, 60, 276–293. [Google Scholar] [CrossRef] [PubMed]
- Ekambaram, M.; Yiu, C.K.Y.; Matinlinna, J.P. Bonding of Resin Adhesives to Caries-Affected Dentin—A Systematic Review. Int. J. Adhes. Adhes. 2015, 61, 23–34. [Google Scholar] [CrossRef]
- Pugach, M.K.; Strother, J.; Darling, C.L.; Fried, D.; Gansky, S.A.; Marshall, S.J.; Marshall, G.W. Dentin Caries Zones: Mineral, Structure, and Properties. J. Dent. Res. 2009, 88, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Follak, A.; Miotti, L.; Lenzi, T.; Rocha, R.O.; Maxnuck Soares, F. The Impact of Artificially Caries-Affected Dentin on Bond Strength of Multi-Mode Adhesives. J. Conserv. Dent. 2018, 21, 136. [Google Scholar] [CrossRef]
- Viral, P.; Nagarathna, C.; Shakuntala, B.S. Chemomechanical Caries Removal in Primary Molars: Evaluation of Marginal Leakage and Shear Bond Strength in Bonded Restorations—An in Vitro Study. J. Clin. Pediatr. Dent. 2013, 37, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Bittencourt, S.; Pereira, J.; Rosa, A.; Oliveira, K.; Ghizoni, J.; Oliveira, M. Mineral Content Removal after Papacarie Application in Primary Teeth: A Quantitative Analysis. J. Clin. Pediatr. Dent. 2010, 34, 229–231. [Google Scholar] [CrossRef]
- Bussadori, S.K.; Castro, L.C.; Galvão, A.C. Papain Gel: A New Chemo-Mechanical Caries Removal Agent. J. Clin. Pediatr. Dent. 2006, 30, 115–119. [Google Scholar] [CrossRef]
- Beyth, N.; Mass, A.; Ziskind, D. Carisolv, a Change in the Perception of Caries Treatment—A Chemo-Mechanical Removal of Caries. Refu’at Ha-peh Veha-shinayim (1993) 2003, 20, 23–29, 78. [Google Scholar] [PubMed]
- Zawaideh, F.; Palamara, J.E.A.; Messer, L.B. Bonding of Resin Composite to Caries-Affected Dentin after Carisolv(®) Treatment. Pediatr. Dent. 2011, 33, 213–220. [Google Scholar] [PubMed]
- Hosoya, Y.; Shinkawa, H.; Marshall, G.W. Influence of Carisolv on Resin Adhesion for Two Different Adhesive Systems to Sound Human Primary Dentin and Young Permanent Dentin. J. Dent. 2005, 33, 283–291. [Google Scholar] [CrossRef]
- Mohammed, D.T.I.; Salih, D.S.A. The Effect of Chemomechanical Caries Removal and Different Bonding Systems on Shear Bond Strength of Carious Dentin (In Vitro Study). Mustansiria Dent. J. 2011, 8, 115–126. [Google Scholar] [CrossRef]
- Hamama, H.; Yiu, C.; Burrow, M.; King, N. Chemical, Morphological and Microhardness Changes of Dentine after Chemomechanical Caries Removal. Aust. Dent. J. 2013, 58, 283–292. [Google Scholar] [CrossRef]
- Hossain, M.; Nakamura, Y.; Tamaki, Y.; Yamada, Y.; Jayawardena, J.A.; Matsumoto, K. Dentinal Composition and Knoop Hardness Measurements of Cavity Floor Following Carious Dentin Removal with Carisolv. Oper. Dent. 2003, 28, 346–351. [Google Scholar]
- Taniguchi, G.; Nakajima, M.; Hosaka, K.; Iwamoto, N.; Ikeda, M.; Foxton, R.M.; Tagami, J. Improving the Effect of NaOCl Pretreatment on Bonding to Caries-Affected Dentin Using Self-Etch Adhesives. J. Dent. 2009, 37, 769–775. [Google Scholar] [CrossRef]
- Bowen, R.L. Adhesive Bonding of Various Materials to Hard Tooth Tissues. III. Bonding to Dentin Improved by Pretreatment and the Use of Surface-Active Comonomer. J. Dent. Res. 1965, 44, 903–905. [Google Scholar] [CrossRef] [PubMed]
- Sirisha, K.; Rambabu, T.; Shankar, Y.; Ravikumar, P. Validity of Bond Strength Tests: A Critical Review: Part I. J. Conserv. Dent. 2014, 17, 305. [Google Scholar] [CrossRef] [PubMed]
- El Mourad, A.M. Assessment of Bonding Effectiveness of Adhesive Materials to Tooth Structure Using Bond Strength Test Methods: A Review of Literature. Open Dent. J. 2018, 12, 664–678. [Google Scholar] [CrossRef]
- Braga, R.R.; Meira, J.B.C.; Boaro, L.C.C.; Xavier, T.A. Adhesion to Tooth Structure: A Critical Review of “Macro” Test Methods. Dent. Mater. 2010, 26, e38–e49. [Google Scholar] [CrossRef]
- Zanatta, R.; Lungova, M.; Borges, A.; Torres, C.; Sydow, H.-G.; Wiegand, A. Microleakage and Shear Bond Strength of Composite Restorations Under Cycling Conditions. Oper. Dent. 2017, 42, E71–E80. [Google Scholar] [CrossRef] [PubMed]
- Abreu, A.; Loza, M.A.; Elias, A.; Mukhopadhyay, S.; Looney, S.; Rueggeberg, F.A. Tensile Bond Strength of an Adhesive Resin Cement to Different Alloys Having Various Surface Treatments. J. Prosthet. Dent. 2009, 101, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Sinhoreti, M.A.C.; Soares, E.F.; Abuna, G.F.; Correr Sobrinho, L.; Roulet, J.-F.; Geraldeli, S. Microtensile Bond Strength of Adhesive Systems in Different Dentin Regions on a Class II Cavity Configuration. Braz. Dent. J. 2017, 28, 474–481. [Google Scholar] [CrossRef]
- Sano, H.; Chowdhury, A.F.M.A.; Saikaew, P.; Matsumoto, M.; Hoshika, S.; Yamauti, M. The Microtensile Bond Strength Test: Its Historical Background and Application to Bond Testing. Jpn. Dent. Sci. Rev. 2020, 56, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Lula, E.C.d.O.; Leite, T.H.M.; Alves, C.M.C.; Santana, I.L.; Almeida, A.M.L.; Costa, J.F. Parameters That Influence Microtensile Bond Testing of Adhesive Systems. Rev. Gaúcha Odontol. 2014, 62, 65–70. [Google Scholar] [CrossRef]
- Dikmen, B.; Gurbuz, O.; Ozsoy, A.; Eren, M.M.; Cilingir, A.; Yucel, T. Effect of Different Antioxidants on the Microtensile Bond Strength of an Adhesive System to Sodium Hypochlorite-Treated Dentin. J. Adhes. Dent. 2015, 17, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Pashley, D.H.; Carvalho, R.M.; Sano, H.; Nakajima, M.; Yoshiyama, M.; Shono, Y.; Fernandes, C.A.; Tay, F. The Microtensile Bond Test: A Review. J. Adhes. Dent. 1999, 1, 299–309. [Google Scholar]
- Costa, A.R.; Garcia-Godoy, F.; Correr-Sobrinho, L.; Naves, L.Z.; Raposo, L.H.A.; de Carvalho, F.G.; Sinhoreti, M.A.C.; Puppin-Rontani, R.M. Influence of Different Dentin Substrate (Caries-Affected, Caries-Infected, Sound) on Long-Term ΜTBS. Braz. Dent. J. 2017, 28, 16–23. [Google Scholar] [CrossRef]
- Kotb, R.M.S.; Abdella, A.A.; El Kateb, M.A.; Ahmed, A.M. Clinical Evaluation of Papacarie in Primary Teeth. J. Clin. Pediatr. Dent. 2009, 34, 117–123. [Google Scholar] [CrossRef]
- Butera, A.; Maiorani, C.; Gallo, S.; Pascadopoli, M.; Quintini, M.; Lelli, M.; Tarterini, F.; Foltran, I.; Scribante, A. Biomimetic Action of Zinc Hydroxyapatite on Remineralization of Enamel and Dentin: A Review. Biomimetics 2023, 8, 71. [Google Scholar] [CrossRef] [PubMed]
- Abuna, G.; Feitosa, V.P.; Correr, A.B.; Cama, G.; Giannini, M.; Sinhoreti, M.A.; Pashley, D.H.; Sauro, S. Bonding Performance of Experimental Bioactive/Biomimetic Self-Etch Adhesives Doped with Calcium-Phosphate Fillers and Biomimetic Analogs of Phosphoproteins. J. Dent. 2016, 52, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Ashtijoo, Z.; Pishevar, L.; MalekipourMalekipour, M.-R.; Khodaei, M.; Sabouri, Z. Comparative Evaluation of Incorporation Calcium Silicate and Calcium Phosphate Nanoparticles on Biomimetic Dentin Remineralization and Bioactivity in an Etch-and-Rinse Adhesive System. J. Clin. Exp. Dent. 2022, 14, e903–e910. [Google Scholar] [CrossRef] [PubMed]
- Braga, R.R.; Fronza, B.M. The Use of Bioactive Particles and Biomimetic Analogues for Increasing the Longevity of Resin-Dentin Interfaces: A Literature Review. Dent. Mater. J. 2020, 39, 62–68. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population | Extracted human teeth with dental caries involving dentin removed with a chemo-mechanical removal agent |
| Intervention | Dental adhesives/Bonding agent (BA) application |
| Comparison | Etch-and-rinse, self-etch, and RMGIC adhesives |
| Primary Outcome | Assess the effect of CMCR agents on the bond strength of dental adhesives |
| Secondary Outcome | Analysis of failure mode of adhesives to CAD after using CMCR |
| Database | Keywords |
|---|---|
| PubMed | (((((“dental caries”[All Fields]) OR (“tooth cavity”[All Fields])) OR (“tooth cavities”[All Fields])) OR (“deep dental caries”[All Fields])) OR (“infected dentin”[All Fields])) OR (“affected dentin”[All Fields]) AND ((((((((((“chemomechanical caries removal”[All Fields]) OR (“atraumatic restorative treatment”[All Fields])) OR (“chemomechanical caries removal agents”[All Fields])) OR (“papacarie”[All Fields])) OR (“carie care”[All Fields])) OR (“brix3000”[All Fields])) OR (“carisolv”[All Fields])) OR (“caridex”[All Fields])) OR (“minimal invasive dentistry”[All Fields])) OR (minimal invasive caries excavation) OR (noninvasive dentistry) AND ((((“dental adhesives”[All Fields]) OR (“self-etch adhesives”[All Fields])) OR (“total etch adhesives”[All Fields])) OR (“resin-modified glass ionomer adhesive”[All Fields])) AND “bonding strength”[All Fields] OR (“bond strength”[All Fields]) OR (“adhesive strength”[All Fields]) OR (“binding strength”[All Fields]) OR (“cohesive strength”[All Fields]) OR (“binding force”[All Fields]) OR (“adhesive force”[All Fields])) OR (tooth bonding strength) OR (“microtensile bond strength”[All Fields]) OR (“microshear bond strength”[All Fields]) |
| TRIP | Caries, caries removal, bonding agent, bond strength |
| Scopus | Caries AND chemomechanical AND caries AND removal AND instruments AND dental adhesive AND bond AND strength |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| In vitro studies | Review articles, case reports, anecdotes, letters to editors, clinical studies, observational studies |
| Studies performed in permanent human teeth only | Animal studies |
| Studies on dentin bond strength of dental adhesives to CAD after using CMCR agents | Studies on agents applied on dentin other than CMCR agents |
| Studies either comparing two or more CMCR agents or comparing different bonding agents using one CMCR agent. | Articles not relevant to the topic |
| Studies published after January 2000 | Studies published before January 2000 |
| CMCR Agent | Composition | Article |
|---|---|---|
| Carisolv™ | 0.95% sodium hypochlorite, three amino acids (glutamic acid, leucine, lysine), pH = 11 | Kusumasari et al., 2021 [31] |
| Hamama et al., 2015 [32] | ||
| Hamama et al., 2014 [33] | ||
| Aggarwal et al., 2013 [34] | ||
| Sirin Karaarslan et al., 2012 [35] | ||
| Li et al., 2011 [30] | ||
| Neves et al., 2011 [38] | ||
| Banerjee et al., 2010 [36] | ||
| Sonoda et al., 2005 [6] | ||
| Burrow et al., 2003 [9] | ||
| Haak et al., 2000 [37] | ||
| Papacarie™ | Papain enzyme, chloramine, toluidine blue, salts, preservatives, thickeners, stabilizers, and deionized water. (pH = 9.2) | Kusumasari et al., 2021 [31] |
| Hamama et al., 2015 [32] | ||
| Hamama et al., 2014 [33] | ||
| Piva et al., 2008 [39] | ||
| SFC-V (“Biosolv”) | pepsin, phosphoric acid/sodium biphosphate buffer | Banerjee et al., 2010 [36] |
| SFC-VIII | a moderately acidic buffered solution of pepsin | Neves et al., 2011 [38] |
| Type of DA | Steps in Application of DA | DA System | Composition of DA | Manufacturer Instructions for Application | Author |
|---|---|---|---|---|---|
| ER | 3-step | Single Bond (3M ESPE, St Paul, MN, USA) | Dimethacrylates, HEMA, polyalkenoid acidcopolymer, 5 nm silane treated colloidal silica, ethanol, water, photoinitiator. |
| Aggarwal et al., 2013 [34] |
| Adper Scotchbond 1XT (3M ESPE, Germany) | 2 hydroxy ethylmethacrylate (HEMA), Polyalkenoic acid copolymer, Bis-phenol A diglycidylmethacrylate (Bis-GMA), Water camphorquinone, Ethanol |
| Banerjee et al., 2010 [36] | ||
| 2-step | Adper Single Bond 2 (3M ESPE, Germany) | Bis-GMA, HEMA, dimethacrylates, ethanol, water, photoinitiator, methacrylate, functional copolymer of polyacrylic and poly(itaconic) acids, 10 wt% of 5 nm-diameter spherical silica particles (pH = 4.1) |
| Sirin Karaarslan et al., 2012 [35] | |
| One-Step (Renew Bisco, Schaumburg, IL, USA) | BPDMA, HEMA, acetone (pH = 4.1) |
| Li et al., 2011 [30] | ||
| Prime and Bond NT (Dentsply) | PENTA, UDMA, nanofiller, cethylamine hydrofluoride, acetone |
| Li et al., 2011 [30]; Piva et al., 2008 [39]; Sonoda et al., 2005 [6]; Haak et al., 2000 [37] | ||
| Mild SE (pH ≥ 2) | 2-step | One Coat Self-Etching Bond, (Coltene Whaledent, Altstatten, Switzerland) pH = 2.5 | Primer: water, HEMA, acrylamidosulfonic acid, glycerol mono- and dimethacrylate, methacrylized polyalkenoate. Bonding: HEMA, glycerol mono- and dimethacrylate, UDMA, methacrylized polyalkenoate, camphoroquinone. |
| Aggarwal et al., 2013 [34]; Burrow et al., 2003 [9] |
| Clearfil SE Bond (Kuraray Co, Osaka, Japan) pH = 2 | Dimethacrylate, dl-camphorquinone, N,N-diethanol-p-toluidine, water; Adhesive Resin: MDP, Bis-GMA, HEMA, hydrophobic dimethacrylate, dl-camphorquinone, N,N-diethanol-p toluidine, silanated colloidal silica | Kusumasari et al., 2021 [31]; Hamama et al., 2014 [33]; Sirin Karaarslan et al., 2012 [35]; Neves et al., 2011 [38]; Piva et al., 2008 [39]; Burrow et al., 2003 [9] | |||
| Clearfil Protect Bond (Kuraray Medical Inc, Tokyo, Japan) pH = 4.5 | MDP, HEMA, Hydrophilic dimethacrylate, Water, Bis-GMA, Hydrophobic dimethacrylate, DL-Camphorquinone, N,N-Diethanol-p-toluidine | Sonoda et al., 2005 [6] | |||
| Intermediate SE | Syntac SC (Vivadent, Schann, Liechtenstein) pH = 1.6 | 2 HEMA, methacrylic acid modified polyacrylic acid, maleic acid, water, fluoride |
| Haak et al., 2000 [37] | |
| Filtek Silorane adhesive pH = 2.7 | 3 Silorane (3,4-epoxycyclohexylethylcyclo polymethylsiloxane, bis-3,4-epoxycyclohexylethyl-phenylmethylsilane); Fillers: Quartz (silane layer), radiopaque yttrium fluoride filler |
| Banerjee et al., 2010 [36] | ||
| Mild SE | 1-step | Adper Easy Bond Self-Etch Adhesive (3M ESPE, St Paul, MN, USA) pH = 2.3 | Methacrylated phosphoric esters, dimethacrylates, 2-HEMA, polyalkenoid acid copolymer, colloidal silica, ethanol, water, photoinitiator. |
| Aggarwal et al., 2013 [34] |
| Clearfil Universal Bond Quick ER (Kuraray Noritake Dental Inc., Tokyo, Japan) pH = 2.3 | 10-MDP, Bis-GMA, HEMA, hydrophilic amide monomer, colloidal silica, ethanol, dl-CQ, accelerators, water, sodium fluoride. (pH = 2.5) Primer: 10-MDP, 2-HEMA, hydrophilic aliphatic dimethacrylate, dl-CQ, water |
| Kusumasari et al., 2021 [31] | ||
| Clearfil S3 (Kuraray Medical Inc, Tokyo, Japan) pH = 2.7 | 10-MDP, bis-GMA, HEMA, di-camphorquinone, ethanol, water, silanated colloidal silica | Hamama et al., 2014 [33] | |||
| Intermediate SE (pH = 1.5) | G-Bond (GC Corporation Tokyo, Japan) pH = 1.5 | 4-MET, UDMA, dimethacrylate component, phosphoric ester monomer, acetone, water | Sirin Karaarslan et al., 2012 [35] | ||
| Strong SE (pH ≤ 1) | Etch&Prime 3.0 (Degussa AG) pH = 0.76 | HEMA, pyrophosphate monomer, photoinitiators, ethanol, water | Haak et al., 2000 [37] | ||
| Adper Prompt-L-Pop (AD-3M ESPE, St. Paul, MN, USA) pH = 0.8 | Methacrylated phosphoric acid HEMA-esters, Bis-GMA, initiators based on camphorquinone, and stabilizers | Banerjee et al., 2010 [36] | |||
| RMGIA | Self-adhesive material | Fuji II LC (GC International) | Fluoroaluminium silicate glass, polyacrylic acid, HEMA |
| Burrow et al., 2003 [9] |
| Fuji Bond LC (GC Corp, Tokyo, Japan) | Powder: 90–100%, Alumino-fluoro-silicate glass (amorphous); Liquid: 20–30% distilled water, 20–30% PAA, 25–35% HEMA, 5–10% UDMA, and less than 1% Camphorquinone | Hamama et al., 2015 [32] | |||
| Riva Bond LC (SDI, Bayswater, Australia) | Compartment 1: 95–100% Fluoroaluminosilicate glass powder; Compartment 2: 15–25% PAA, 1–5% Tartaric Acid 25–40% HEMA, 5–15% Dimethacrylate Cross-linker 10–20% Acidic Monomer |
| Hamama et al., 2015 [32] |
| Author | CMCR Agent | Time of Exposure | Sample Type | Sample Size | Storage Conditions | Bond Strength Test Used | Tensile Rate |
|---|---|---|---|---|---|---|---|
| Kusumasari et al., 2021 [31] | Carisolv and Papacarie | 60 s | Extracted human molars with occlusal carious lesions | 40 | 24 h water storage | μTBS | 1 mm/min |
| Hamama et al., 2015 [32] | 30 s | Permanent molars exhibiting moderate cavitation on the occlusal surface into dentine | 75 | distilled water at 37 °C for 24 h | 1 mm/min | ||
| Hamama et al., 2014 [33] | Carious permanent molars exhibiting frank cavitation into dentin | 48 | distilled water at 37 °C for 24 h | 1 mm/min | |||
| Aggarwal et al., 2013 [34] | Carisolv | Extracted, non-restored human maxillary and mandibular third molars with occlusal dental caries | 30 | distilled water at 37 °C for 24 h | 0.5 mm/min | ||
| Sirin Karaarslan et al., 2012 [35] | Permanent cavitated human molar teeth | 45 | immersion in water at 37 °C for 24 h | 1 mm/min | |||
| Li et al., 2011 [30] | Extracted human third molars with moderate occlusal caries | distilled water at 37 °C for 24 h | 1 mm/min | ||||
| Sonoda et al., 2005 [6] | 30 s | Extracted adult human molars | 20 | One day stored in tap water at room temperature | 0.2 mm/min | ||
| Burrow et al., 2003 [9] | Freshly extracted human molars with occlusal caries | 31 | water at 37 °C for 24 h | 1 mm/min | |||
| Neves et al., 2011 [38] | Carisolv; Exp. SFC-VIII + instrument | Non-restored molar presenting caries lesions on the occlusal surface that presumably involve dentin | 35 | 24-h storage in water at 36 °C, | 1 mm/min | ||
| Banerjee et al., 2010 [36] | Carisolv; SFC-V (“Biosolv”) | 40 s; SFC-V was introduced into the cavity and was immediately agitated. | Extracted, human cavitated carious molars | 51 | hydrated four-week storage | 1 mm/min | |
| Piva et al., 2008 [39] | Papacarie | 30 s | Cavitated human molar teeth | 40 | 37 °C in distilled water for 24 h | 1 mm/min | |
| Haak et al., 2000 [37] | Carisolv | Extracted human molars with occlusal caries | 121 | immersed in water at 37 °C for 24 h | SBS | 1 mm/min |
| Author | CMCR Agent | Bonding Agent | Bond Strength to CAD (Mean ± SD) [MPa] | Conclusion |
|---|---|---|---|---|
| Aggarwal et al. 2013 [34] | Carisolv | Single-Bond (ER) | 31.1 ± 2.7 | Carisolv did not affect the μTBS values of different adhesive systems tested on CAD. The ER adhesive and two-bottle SE system showed significantly μTBS than the single-bottle SE system. |
| Adper Easy Bond (SE) | 23.4 ± 2.2 | |||
| One Coat (SE) | 33.1 ± 3.8 | |||
| Sirin Karaarslan et al., 2012 [35] | Adper Single Bond 2 (ER) | 11.7 ± 5 | The technique used to remove caries influenced the μTBS to CAD created by the dentin adhesive systems. CMCR techniques may be suggested when choosing a two-step SE adhesive. | |
| Clearfil SE Bond (SE) | 19 ± 5.4 | |||
| G-Bond (SE) | 14.4 ± 3.7 | |||
| Li et al., 2011 [30] | Prime and Bond NT (ER) | 17.22 ± 7.95 | CMCR did not influence the bond strengths of the adhesive systems used in this study to CAD. The highest bond strength was achieved with the application of the ER adhesive system. | |
| ONE-STEP (ER) | 25.4 ± 8.44 | |||
| Adper Prompt L-Pop (SE) | 17.96 ± 8.33 | |||
| Banerjee et al., 2010 [36] | Scotchbond (ER) | 126.11 ± 37.53 | Using three different caries excavation techniques (Carisolv ™ gel, SFC-V, and hand excavation) has no effect on adhesive bond strengths to residual carious dentin. | |
| Filtek Silorane Bond (ER) | 134.49 ± 38.43 | |||
| Sonoda et al., 2005 [6] | Clearfil Protect Bond (SE) | 31.10 ± 9.21 | Carisolv gel excavation did not compromise bond strengths to CAD in either group tested. | |
| Prime and Bond NT (ER) | 26.99 ± 11.69 | |||
| Burrow et al., 2003 [9] | Clearfil SE Bond (SE) | 28.7 ± 6.9 | Carious dentin treated with Carisolv did not affect the adhesion of the adhesive restorative materials tested in this study, except Fuji II LC. | |
| One Coat Bond (ER) | 27.4 ± 6.4 | |||
| Fuji II LC | 16.4 ± 5.6 | |||
| Fuji IX | 13.4 ± 3.9 | |||
| Haak et al., 2000 [37] | NRC/Prime and Bond NT (ER) | 13.4 ± 3.2 | CMCR has no negative impact on bonding modern adhesive systems to dentin. | |
| Prime and Bond NT (ER) | 20.8 ± 5.1 | |||
| Syntac SC (SE) | 21.4 ± 5.4 | |||
| PPA/Syntac SC (SE) | 18.6 ± 4.6 | |||
| Etch and Prime 3.0 (SE) | 17.3 ± 3.3 | |||
| Kusumasari et al., 2021 [31] | Clearfil SE Bond 2 (SE) | 47.35 ± 5.7 | Smear layer deproteinization using CMCR agents (Papacarie and Carisolv) is an effective pre-treatment to improve the μTBS of two-step SE adhesives, particularly to CAD. | |
| Universal Bond Quick ER (SE) | 42.25 ± 8.3 | |||
| Hamama et al., 2015 [32] | PA/Fuji Bond LC (RMGIC adhesive) | 22.58 ± 4.25 | Tested CMCR agents have no adverse effect on the adhesion of RMGIA to both sound dentin and CAD. Dentin surface treatment with 37% phosphoric acid for 5 s has no detrimental effects on the bonding of RMGI adhesives to dentin when compared with either PAA solution for 10 s. RMGIA bonded well to both sound dentin and CAD. | |
| 25–30%PAA/Fuji Bond LC | 15.4 ± 1.69 | |||
| 25–30% PAA/Riva Bond LC | 14.5 ± 5 | |||
| 20% PAA + 3% AlCl3/Fuji Bond LC | 20.4 ± 2.2 | |||
| PA/Riva Bond LC | 15.3 ± 1.9 | |||
| Hamama et al., 2014 [33] | Clearfil SE Bond (SE) | 30.8 ± 2.7 | CMCR did not affect the bonding of SE adhesives to CAD. | |
| Clearfil S3 Bond (SE) | 20.1 ± 2.2 | |||
| Neves et al., 2011 [38] | Clearfil SE Bond | 41.7 ± 11.7 | Carisolv resulted in the highest TBS to “residual caries-excavated” dentin, followed by the use of a tungsten-carbide-bur in conjunction with Caries Detector. | |
| SFC-VIII | 46 ± 11.5 | |||
| Piva et al., 2008 [39] | Papacarie | Clearfil SE Bond (SE) | 10.9 ± 2.3 | The bond strength of the SE adhesive to CAD was negatively affected by chemo-mechanical excavation using the papain-based gel. |
| Prime and Bond NT (ER) | 8.3 ± 8.3 | |||
| Kusumasari et al., 2021 [31] | Clearfil SE Bond 2 (SE) | 46.56 ± 3.5 | ||
| Universal Bond Quick ER (SE) | 45.19 ± 5.9 | |||
| Hamama et al., 2015 [32] | PA/Fuji Bond LC (RMGIC adhesive) | 21.44 ± 4.94 | ||
| 25–30% PAA/Fuji Bond LC | 15.9 ± 1.66 | |||
| 25–30% PAA/Riva Bond LC | 15.5 ± 3.9 | |||
| 20% PAA + 3% AlCl3/Fuji Bond LC | 16.1 ± 3.1 | |||
| PA/Riva Bond LC | 18.2 ± 3.1 | |||
| Hamama et al., 2014 [33] | Clearfil SE Bond (SE) | 31.5 ± 2.8 | ||
| Clearfil S3 Bond (SE) | 23.2 ± 1.9 | |||
| Banerjee et al., 2010 [36] | SFC-V (Biosolv) | Scotchbond (ER) | 264.71 ± 79.3 | Utilizing three distinct caries extraction methods (Carisolv ™ gel, SFC-V, and hand excavation) has no effect on adhesive bond strengths to residual carious dentin. |
| Author | Type of Failure Mode of Bonding Agents after CMCR Application | |
|---|---|---|
| Self-Etch Adhesives | Etch-and-Rinse Adhesives | |
| Hamama et al. (2015) [32] | Cohesive | Na |
| Hamama et al. (2014) [33] | Cohesive | Na |
| Neves et al. (2011) [38] | Cohesive | Na |
| Banerjee et al. (2010) [36] | Adhesive | Cohesive |
| Sonoda et al. (2005) [6] | Adhesive | Cohesive |
| Burrow et al. (2003) [9] | Cohesive | Na |
| Sirin Karaarslan et al. (2012) [35] | Adhesive | Adhesive |
| Li et al. (2011) [30] | Adhesive | Adhesive |
| Piva et al. (2008) [39] | Adhesive | Adhesive |
| Haak et al. (2000) [37] | Adhesive | Adhesive |
| Kusumasari et al. (2021) [31] | Mixed | Na |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohanty, P.R.; Mishra, L.; Saczuk, K.; Lapinska, B. Optimizing Adhesive Bonding to Caries Affected Dentin: A Comprehensive Systematic Review and Meta-Analysis of Dental Adhesive Strategies following Chemo-Mechanical Caries Removal. Appl. Sci. 2023, 13, 7295. https://doi.org/10.3390/app13127295
Mohanty PR, Mishra L, Saczuk K, Lapinska B. Optimizing Adhesive Bonding to Caries Affected Dentin: A Comprehensive Systematic Review and Meta-Analysis of Dental Adhesive Strategies following Chemo-Mechanical Caries Removal. Applied Sciences. 2023; 13(12):7295. https://doi.org/10.3390/app13127295
Chicago/Turabian StyleMohanty, Pooja R., Lora Mishra, Klara Saczuk, and Barbara Lapinska. 2023. "Optimizing Adhesive Bonding to Caries Affected Dentin: A Comprehensive Systematic Review and Meta-Analysis of Dental Adhesive Strategies following Chemo-Mechanical Caries Removal" Applied Sciences 13, no. 12: 7295. https://doi.org/10.3390/app13127295
APA StyleMohanty, P. R., Mishra, L., Saczuk, K., & Lapinska, B. (2023). Optimizing Adhesive Bonding to Caries Affected Dentin: A Comprehensive Systematic Review and Meta-Analysis of Dental Adhesive Strategies following Chemo-Mechanical Caries Removal. Applied Sciences, 13(12), 7295. https://doi.org/10.3390/app13127295