Abstract
This case study focuses on scapula reconstruction using three-dimensional printing in a patient with low-grade osteosarcoma. Malignant tumors originating from the scapula often lead to destructive surgery, with poor functional status and quality of life for the patients. Using custom prosthetic technology through three-dimensional printing could be a possible solution for reconstruction with greater long-term functional outcomes. This study aims to assess the functional outcomes of the reconstruction. A 39-year-old patient with low-grade central osteosarcoma involving the lateral two-thirds of the scapula underwent a custom prosthetic reconstruction. The patient subsequently followed a rehabilitation protocol for 12 months. The results indicate that even though there was a slight decrease in the range of movement, and an increase in the disabilities of the arm, shoulder, and hand (DASH) score, no relevant increase in activities of daily living (ADL) disability was present at follow-up. The patient returned to carry out his daily activities without pain and with a minimal functional reduction in movement. In conclusion, three-dimensional prosthetic reconstruction is a valid alternative for scapula reconstruction, allowing excellent functional and aesthetic results in oncological cases.
1. Introduction
Conventional osteosarcoma (COS) is one of the most frequent primary solid malignancies of bone, characterized by malignant mesenchymal cells producing osteoid and immature bone [1,2,3]. Within the sphere of osteosarcomas, low-grade forms have higher survival rates; between these low-grade subtypes, a rare condition that accounts for 1–2% is low-grade central osteosarcoma (LGCOS). This neoplasm originates within the intramedullary cavity and consists of fibroblastic cells with low-grade nuclear atypia [3]. It typically affects the metaphysis of long bones but occasionally can develop in the axial skeleton [4,5]. The preoperative period can be more extended than conventional osteosarcoma due to the low symptoms (occasional pain, local swelling), exceeding 10 years in some cases with an average of >2 years [5,6]. The long intercurrent period before diagnosis often leads to an intramedullary expansive lytic growth with local areas of cortical destruction [7]. The prognosis is good when the LGCOS is widely respected: the metastatic rate is <5%, and 5 and 10-year overall survival rates are 90% and >80%, respectively [5,6,8]. Due to the need for surgery with wide resection margins, when the LGCOS affects the scapula, the problem of functional outcome arises.
Among the various possibilities of surgical treatment, the scapula prosthesis is considered an excellent compromise to maintain the function of the limb and an acceptable cosmetic appearance for the patient [9]. However, in some cases, the oncological involvement of the scapula is confined only to a circumscribed portion of the bone. In that case, three-dimensional (3D) printing could absolve the limits of radical surgery, allowing more accurate preoperative planning and more precise reconstruction of the anatomical part.
We are reporting the case of a 39 years-old patient affected by low-grade central osteosarcoma of the left scapula that underwent a partial scapulectomy and a reconstruction with an emi-endoprosthesis with the aid of 3D planning technology.
2. Detailed Case Description
2.1. Oncological Staging
A 39-year-old patient presented to our center with a history of progressive pain in the left shoulder. Four years before the presentation of symptoms, the patient underwent a CT scan and MRI of the shoulder for pain with the occasional finding of a lytic area around the glenoid of the left scapula; the neoformation was not further examined before he arrived at our center. At the clinical examination, no masses were detectable by the scapula palpation. The patient had no functional limitations in extension, flexion, abduction/adduction, or shoulder rotation. The surrounding skin had a normal temperature, good sensation, and blood circulation of the left upper extremities, with no redness signs or ulceration. No lymph nodes were appreciable in the axilla and upper extremity. The only symptom was occasional pain around the joint.
An X-ray of the left scapula was performed; an irregularity of the bone involving the glenoid area was detected and located in the S2 and partially the S1 region according to Malawer’s and Musculoskeletal Tumor Society classification [10,11] (Figure 1).

Figure 1.
X-ray of the left scapula at the presentation.
A CT scan of the shoulder indicated a lytic area extended from the glenoid cavity to the medial third of the scapula’s body, infiltrating the acromion process partially with a dimension of 70 × 45 mm (Figure 2).
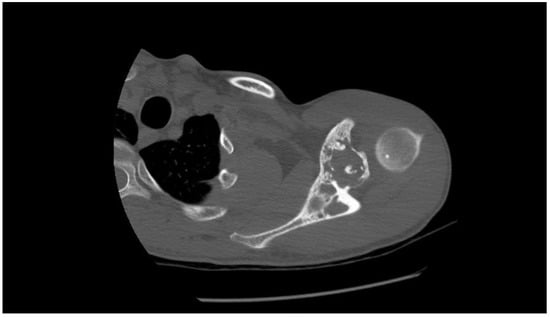
Figure 2.
CT scan of the left shoulder at the presentation.
Comparing the CT scan with the previous one performed, the neoplastic process was stable, without further bone extension. A CT-guided needle biopsy was executed, and the histological results suggested low-grade central osteosarcoma (Figure 3).
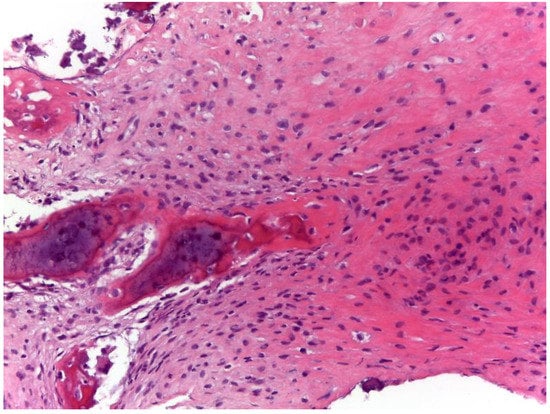
Figure 3.
Histologically, the lesion was composed of a hypocellular spindle cell proliferation with mild atypical nuclear features, in a collagenous matrix; parallel-aligned bone trabeculae were also present. The whole histological and genetical features were consistent with low-grade central osteosarcoma (Hematoxylin & Eosin, 20×).
The absence of metastases of the lungs, mediastinum, abdomen, or bones was confirmed by a thoracoabdominal CT scan. The final diagnosis turns out to be left scapula low-grade central osteosarcoma, scapular sites S1 and S2, Enneking IA stage [12], grade 2. This case has been discussed collegially with a board composed of oncologists, oncological orthopedic surgeons, radiologists, and pathologists; in consideration of the low malignancy of the neoplasm, the anatomical part with only an area of neoplastic invasion, the high functional request for a young active patient, a total scapulectomy with humeral suspension would have been too demolitive of a choice. However, wide margins were necessary to reduce the risk of local recurrence of malignancy. A partial scapulectomy with a customized reconstruction was agreed upon as a treatment for this patient.
2.2. Prostheses Project
The tumor area and surrounding anatomical structures were studied with a CT scan with 1 mm slices to achieve a representative 3D model. At the same time, MRI images were needed for an adequate evaluation of tumor extent within the bone (both medullary and cortically) and in surrounding soft tissues. Patient-specific instruments (PSIs) and implants were designed according to the planned resection strategy. The fabrication process for PSIs and custom implants is in charge of a company with specific expertise and industrial workflow for additive manufacturing. Commercial software, as well as Mimics® (Materialise, Leuven, Belgium) or Invesalius® (freeware), are mainly used for segmentation. PSIs can be molded in nylon or printed in titanium alloy according to the companies’ clinical needs. PSIs had bone-specific contact surfaces to fit into a unique position on the bony structure of the patient based on the shape of the bone acquired by the CT scan (Figure 4). PSIs were equipped with flat surfaces and holes to be pinned temporarily on the bone. The final PSI was printed in nylon or titanium and made sterile for operation.
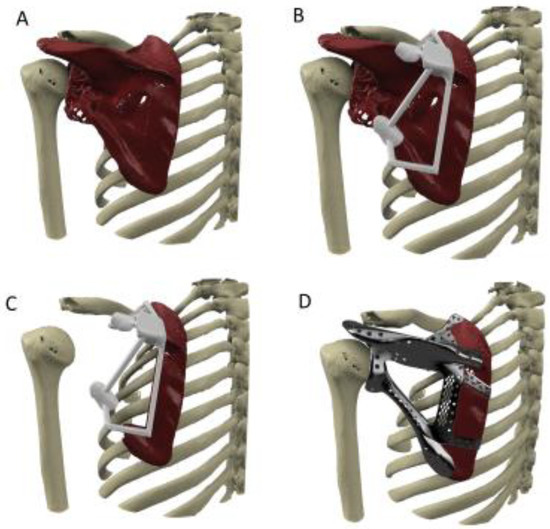
Figure 4.
Reconstructed 3D scapular tumor model (A) low-grade osteosarcoma of the left glenoid; (B) bone cutting using patient-specific cutting guide; (C) the virtual bone cut; (D) the virtual 3-D model of scapular prosthesis.
Before the definitive model, a virtual custom prosthesis was created, modeling on it the best fixation method of the implant on the existing bone, mirroring the opposite part. The Ti-6Al-4V implants were fabricated by depositing a few micron layers of titanium powder melted by electron beams technology (i.e., electron beam melting technique). Implant porosity was widely variable to increase the performance of the prostheses: macro-porosity was studied to lighten the implant, while micro-porosity could enhance the bone surface contact. These surfaces have pores with an average size of 0.7 mm, allowing the host bone to grow directly inside the implant spaces to achieve stable biological fixation. The prosthesis was provided with tools to allow fixation to the host bone and plates or rods, while the screws’ position and lengths were previously planned. Polished manufacture or a surface layer (polycaprolactone, PCL, poly-lactic acid, PLA) could be integrated into porous titanium structures for articular reconstruction.
2.3. Surgery
Intraoperatively, the patient was in the lateral position; the incision was taken from the coracoid process anteriorly to the inferior angle of the scapula posteriorly (Figure 5). The periscapular soft tissues were dissected, and the scapula was exposed completely.

Figure 5.
Preoperative patient planning (A–C).
After a complete bone dissection, the navigation template for osteotomy was attached to the anatomical landmarks, and the affected part of the scapula was removed without complications (Figure 6).
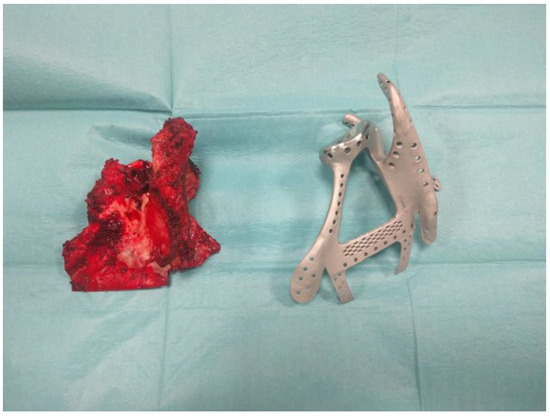
Figure 6.
Anatomical surgical specimen compared with the custom prosthesis.
Following the osteotomy, the hemi-prosthesis was combined with the remaining bone portion and fixed with screws to the medial part of the scapula; a Kirschner wire, supported by a surgical suture, was used to stabilize and make an arthrodesis of the acromion-clavicular joint. An intraoperative X-ray showed the perfect contact of the prostheses to the bone. Finally, we sutured the rotator cuff and periscapular muscles to the prostheses using the preformed holes. After various shoulder stability tests, the wound was sutured, and a Desault bandage was applied to be maintained for 20 days to obtain good healing.
2.4. Follow-Up
After removing the bandage, the patient underwent rehabilitation at our center’s Physical Medicine and Rehabilitation Unit. The wound was clean, without signs of infection, with no redness and low skin temperature (Figure 7).

Figure 7.
Clinical follow-up at 12 months: shoulder ROM was satisfactory, with an anterior elevation between 121 and 150°, abduction between 91° and 120°, external rotation, hand above the head, and internal rotation of hand posteriorly to the level of T12.
During the post-operative and 3 years X-ray no signs of implant loosening or shoulder instability were identified (Figure 8).

Figure 8.
Postoperative X-ray.
Initially, the patient started with a passive mobilization of the shoulder followed by active movements, muscular strengthening focused on dynamic stabilizers of the scapula complex, neuromuscular electrical stimulation (NMES), muscular proprioceptive facilitation, postural control, and proprioceptive exercises. The patient subsequently continued rehabilitation in his city of residence and resumed sporting activity in the pool.
The patient underwent a follow-up which included the execution of a clinical medical evaluation, an X-ray of the operated shoulder, and a CT scan of the chest every 3 months during the first two years, and every 4 months during the third and fourth follow-up years. Finally, during the fifth year, the controls were performed every 6 months. No signs of local relapse or distant metastases were reported. The follow-up is currently still in progress. At 6 months of follow-up, the patient showed a mechanical complication of the prostheses implant with the mobilization of the Kirschner wire; under the skin, near the coracoid process was palpable the extroflection of the metal wire, with no ulceration but with slight pain and esthetical discomfort for the patient. We decided to surgically remove the K-wire. No further mechanical complications occurred during the rest of the follow-up. The functional results of the operated shoulder were evaluated during the first 12 months of follow-up. The scores used were the Constant–Murley score (CMS) and the disabilities of the arm, shoulder, and hand (DASH) score; the first defines the level of pain and ability to carry out ordinary daily activities, using a scale from 0 to 100, where the higher value indicates a higher functional quality for the patient. The second score indicates the level of disability of the upper limb, using a scale from 0 to 100, where the highest value indicates a condition with less autonomy. Furthermore, to define the functionality of the operated shoulder muscles more securely, an electromyographic examination (EMG) was performed using the Cometa wireless EMG system [13].
At 12 postoperative months, the range of movement (ROM), measured by the Constant–Murley score [14,15], changed from 65 to 51 points (Table 1). The functional aspects where a change was highlighted are an overall reduction in mobility, the absence of pain, and lower strength in the abduction movement (Table 1). However, shoulder ROM was satisfactory, with an anterior elevation between 121 and 150°, abduction between 91° and 120°, external rotation, hand above the head, and internal rotation of hand posteriorly to the level of T12.

Table 1.
CMS and DASH score.
The DASH score [16,17] changed from 4.2% in the preoperative phase, in which the patient could perform almost all daily activities, except for slight pain and tingling when lifting heavy objects, to 11.7% in the postoperative phase. The problems most encountered resulted in the difficulty in unscrewing the cap of a jar, lifting an object over the head, lifting heavy objects, performing gardening work, washing the back, getting dressed, and engaging in some recreational activities [17]. Considering that the MCID for DASH was 10.2 points, no relevant increase in activities of daily living score (ADL) disability was present at follow-up.
Regarding the electromyographic activity of the shoulder muscles, the activity of the affected muscles did not show any activation anomalies preoperatively. After surgery, there was some difference in the timing of the activation of muscles, except for a slight activation delay of the anterior deltoid during the abduction. During the anterior flexion, the correct activation of the anterior deltoid at the first degrees of movement was observed. No significant changes were reported in the anterior dentate muscle, trapezius, pectoralis, and great dorsal muscles.
During the extra-rotation, there was an increase in the activation amplitude of the lower trapezius and middle trapezius; no variation in activity at the level of the great dorsal. At 12 months of follow-up, the patient returned to carry out his daily activities without pain and with a minimal functional reduction in movement. At 3 years of follow-up the patient is continuously disease free maintaining the same shoulder activity.
3. Discussion
Malignant tumors of the scapula require surgery that is often highly destructive to obtain large surgical margins and reduce the risk of local recurrence. On some occasions, we find ourselves forced to perform complete scapulectomy operations with humeral suspension, with poor functional, motor, and aesthetic results for the patient [9]. Central low-grade osteosarcoma is one of those malignant forms which, though rarely, can affect the scapula [4,5]. However, it is a malignant tumor with slow growth that often results in bone destruction [7]. The removal with wide margins allows for good overall survival and local control of the disease [5,6,8]. This form of cancer mainly affects a young age group, around the third decade of life [8]. Patients affected by this malignancy often require high functional results for a return to daily activities, a return to sport, and a return to playful activities. With new reconstructive technologies in the medical field, limb salvage, where possible, has become of extreme importance. Moreover, previous studies have shown that over 90% of limb salvage interventions showed no difference in terms of survival in patients with malignant tumors [18].
Various surgical options have been tried over the years. Total scapulectomy associated with humeral suspension is one of the most used surgical options; however, the functional limits for the patient are known. Humeral suspension limits movement significantly, making it difficult to lift the arm over the head, perform internal and external rotations, and do weightlifting with the operated limb [9,19,20]. Moreover, as previously mentioned, the limits of the aesthetic outcome of this procedure must be considered.
The choice of scapula transplantation using homologous grafts has led to good functional results in the short and medium-term; however, bone resorptions occurred in long-term follow-ups, resulting in loss of scapular muscle strength associated with graft fractures [21]. Over the years, scapula endoprostheses have improved outcomes in patients suffering from scapula tumors in aesthetic and functional terms. However, the presence of prostheses that do not reflect the patient’s anatomical characteristics has determined functional motor aspects, which are good, but still need to be optimal [9,22]. Faced with the need to obtain increasingly complex reconstructive results, the introduction of custom reconstruction techniques using 3D printing has led to significant changes in surgical outcomes in oncological and reconstructive orthopedics. Furthermore, using customized cutting masks on the patient’s bone profile has increased the possibility of obtaining large surgical margins with increasingly complex osteotomies and subsequently allowing prosthetic reconstructions that adhere perfectly to the healthy portion of bone [23,24]. In our case, the presence of central low-grade osteosarcoma involving the scapula at the level of the glenoid cavity with the involvement of part of the body and with a partial extension at the level of the acromial and coracoid process (Malawer S1 and S2), set the limit of a total scapulectomy. However, the young age of the patient, and the presence of a low-grade disease, without further visceral and lymph node localizations, placed us in front of the need to find a more functional reconstructive alternative. A cutting guide enabled a complex osteotomy that spared the entire medial portion of the scapula while maintaining wide surgical margins. Subsequently, the 3D customization allowed the medial margin of the patient’s scapula to join to a prosthetic system that reconstructed the glenoid cavity, acromial, and coracoid processes and obtained excellent reconstructive results. The patient was followed up with a regular postoperative follow-up. After 12 months, the functional results were good, with extensive anterior elevation, abduction, and intra/extra rotation. The only complication was the mobilization of a Kirschner wire used for acromioclavicular stabilization. This event required the surgical removal of the wire after 6 months; however, following removal, no joint instabilities occurred. This complication allowed us to understand how, in a similar clinical condition, in which a scapular prosthetic reconstruction is required, different matching possibilities can be used at the level of the acromion–clavicular joint, for example, designing an ultra-congruent prosthetic facet joint, stabilized with only the use of trans-osseous sutures. Thanks to this complex reconstruction surgical technique, the patient has returned to a good quality of life, with slight limitations and without pain, and excellent local disease control results.
To conclude, however, restrictions remain in this study. First, the follow-up is currently still short (30 months) to define the outcome of this custom-made prosthesis. Moreover, designing a custom prosthesis through 3D printing takes a long time and has high production costs. Finally, it is necessary to develop a more extensive surgical series to clearly define, for the future, which are the ideal options for creating custom scapular prosthetic implants with a lower rate of complications.
4. Conclusions
For years, malignant scapula tumors have presented the limit of reconstructive techniques that maintain large surgical margins and good functional and aesthetic outcomes. Technological innovation in the orthopedic field has led to ever greater possibilities of limb-sparing. The introduction of customization technologies through 3D printing has further refined the orthopedic reconstructive capacity, enabling more complex osteotomies and reconstructions calibrated on the patient’s anatomical characteristics. Briefly, 3D printing prosthetics could fill patients’ surgical needs who require highly individualized reconstructions.
Author Contributions
Conceptualization, G.B. and G.T.; methodology, G.B. and G.T.; validation, G.B., M.G.B. and G.T.; investigation, G.T. and R.B.; resources, G.B.; data curation, G.B., G.T., M.G.B. and D.P.; writing—original draft preparation, G.B. and G.T.; writing—review and editing, R.L., G.T. and M.G.B.; visualization, G.B.; supervision, G.T.; project administration, G.B. and G.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. Ethical review and approval were waived for this study due to the nature of this research (retrospective observational case series and literature review).
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Acknowledgments
The authors would like to thank all the paramedic staff (nurses, radiologists, technicians) from our institution (IRCCS, Istituto Ortopedico Rizzoli) that helped during all the procedures included in this series. We would also like to show gratitude to Giulia Zoggia for her help with the English revision.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Arndt, C.A.; Crist, W.M. Common musculoskeletal tumors of childhood and adolescence. N. Engl. J. Med. 1999, 341, 342–352. [Google Scholar] [CrossRef]
- Sobin, L.H.; Fleming, I.D. TNM Classification of Malignant Tumors, fifth edition (1997). Union Internationale Contre le Cancer and the American Joint Committee on Cancer. Cancer 1997, 80, 1803–1804. [Google Scholar] [CrossRef]
- Choi, J.H.; Ro, J.Y. The 2020 WHO Classification of Tumors of Soft Tissue: Selected Changes and New Entities. Adv. Anat. Pathol. 2021, 28, 44–58. [Google Scholar] [CrossRef]
- Schwab, J.H.; Antonescu, C.R.; Athanasian, E.A.; Boland, P.J.; Healey, J.H.; Morris, C.D. A comparison of intramedullary and juxtacortical low-grade osteogenic sarcoma. Clin. Orthop. Relat. Res. 2008, 466, 1318–1322. [Google Scholar] [CrossRef] [PubMed]
- Malhas, A.M.; Sumathi, V.P.; James, S.L.; Menna, C.; Carter, S.R.; Tillman, R.M.; Jeys, L.; Grimer, R.J. Low-grade central osteosarcoma: A difficult condition to diagnose. Sarcoma 2012, 2012, 764796. [Google Scholar] [CrossRef]
- Choong, P.F.; Pritchard, D.J.; Rock, M.G.; Sim, F.H.; McLeod, R.A.; Unni, K.K. Low grade central osteogenic sarcoma. A long-term followup of 20 patients. Clin. Orthop. Relat. Res. 1996, 322, 198–206. [Google Scholar] [CrossRef]
- Andresen, K.J.; Sundaram, M.; Unni, K.K.; Sim, F.H. Imaging features of low-grade central osteosarcoma of the long bones and pelvis. Skelet. Radiol. 2004, 33, 373–379. [Google Scholar] [CrossRef]
- Kurt, A.M.; Unni, K.K.; McLeod, R.A.; Pritchard, D.J. Low-grade intraosseous osteosarcoma. Cancer 1990, 65, 1418–1428. [Google Scholar] [CrossRef] [PubMed]
- Pritsch, T.; Bickels, J.; Wu, C.C.; Squires, M.H.; Malawer, M.M. Is scapular endoprosthesis functionally superior to humeral suspension? Clin. Orthop. Relat. Res. 2007, 456, 188–195. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, M.I.; Sim, F.H.; Chao, E.Y. Limb salvage for neoplasms of the shoulder girdle. Intermediate reconstructive and functional results. J. Bone Jt. Surg. Am. 1996, 78, 1872–1888. [Google Scholar] [CrossRef]
- Malawer, M.M.; Meller, I.; Dunham, W.K. A new surgical classification system for shoulder-girdle resections. Analysis of 38 patients. Clin. Orthop. Relat. Res. 1991, 267, 33–44. [Google Scholar] [CrossRef]
- Enneking, W.F.; Spanier, S.S.; Goodman, M.A. A system for the surgical staging of musculoskeletal sarcoma. 1980. Clin. Orthop. Relat. Res. 2003, 415, 4–18. [Google Scholar] [CrossRef] [PubMed]
- Parel, I.; Jaspers, E.; de Baets, L.; Amoresano, A.; Cutti, A.G. Motion analysis of the shoulder in adults: Kinematics and electromyography for the clinical practice. Eur. J. Phys. Rehabil. Med. 2016, 52, 575–582. [Google Scholar] [PubMed]
- Yian, E.H.; Ramappa, A.J.; Arneberg, O.; Gerber, C. The Constant score in normal shoulders. J. Shoulder Elb. Surg. 2005, 14, 128–133. [Google Scholar] [CrossRef]
- Constant, C.R.; Murley, A.H. A clinical method of functional assessment of the shoulder. Clin. Orthop. Relat. Res. 1987, 214, 160–164. [Google Scholar] [CrossRef]
- Padua, R.; Padua, L.; Ceccarelli, E.; Romanini, E.; Zanoli, G.; Amadio, P.; Campi, A. Italian version of the Disability of the Arm, Shoulder and Hand (DASH) questionnaire. Cross-cultural adaptation and validation. J. Hand Surg. Br. 2003, 28, 179–186. [Google Scholar] [CrossRef]
- Franchignoni, F.; Vercelli, S.; Giordano, A.; Sartorio, F.; Bravini, E.; Ferriero, G. Minimal clinically important difference of the disabilities of the arm, shoulder and hand outcome measure (DASH) and its shortened version (QuickDASH). J. Orthop. Sports Phys. Ther. 2014, 44, 30–39. [Google Scholar] [CrossRef]
- Wodajo, F.M.; Bickels, J.; Wittig, J.; Malawer, M. Complex reconstruction in the management of extremity sarcomas. Curr. Opin. Oncol. 2003, 15, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.-F.; Yu, X.-C.; Xu, M.; Hu, Y.-C.; Liu, X.-P. Functional Results and Emotional Acceptance after Scapulectomy for Malignant Shoulder Tumors. Orthop. Surg. 2016, 8, 186–195. [Google Scholar] [CrossRef]
- Vahanan, N.M.; Mohanlal, P.; Bose, J.C.; Gangadharan, R.; Karthisundar, V. The functional and oncological results after scapulectomy for scapular tumours: 2–16-year results. Int. Orthop. 2007, 31, 831–836. [Google Scholar] [CrossRef]
- Zhang, K.; Duan, H.; Xiang, Z.; Tu, C. Surgical technique and clinical results for scapular allograft reconstruction following resection of scapular tumors. J. Exp. Clin. Cancer Res. 2009, 28, 45. [Google Scholar] [CrossRef] [PubMed]
- Min, L.; Zhou, Y.; Tang, F.; Zhang, W.; Luo, Y.; Duan, H.; Tu, C. Reconstruction with scapular hemiarthroplasty endoprosthesis after scapulectomy for malignant tumour. Int. Orthop. 2017, 41, 1057–1063. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, G.; Frisoni, T.; Spazzoli, B.; Lucchese, A.; Donati, D. Computer assisted surgery and 3d printing in orthopaedic oncology: A lesson learned by cranio-maxillo-facial surgery. Appl. Sci. 2021, 11, 8584. [Google Scholar] [CrossRef]
- Deng, L.; Zhao, X.; Wei, C.; Qu, W.; Yu, L.; Zhu, S. Application of a three-dimensional printed segmental scapula prosthesis in the treatment of scapula tumors. J. Int. Med. Res. 2019, 47, 5873–5882. [Google Scholar] [CrossRef] [PubMed]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).