
Playing Football as a Risk Factor for Lower Leg Malalignment?—Comparing Lower Leg Axis of Male Adolescent Football Players and Referees

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Colyn, W.; Agricola, R.; Arnout, N.; Verhaar, J.A.N.; Bellemans, J. How does lower leg alignment differ between soccer players, other athletes, and non-athletic controls? Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 3619–3626. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, G.S.; Parekh, S.M.; Moses, J.; Fuller, C.; Scammell, B.; Batt, M.E.; Zhang, W.; Doherty, M. Prevalence of knee pain, radiographic osteoarthritis and arthroplasty in retired professional footballers compared with men in the general population: A cross-sectional study. Br. J. Sports Med. 2018, 52, 678–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kadam, U.T.; Croft, P.R. Clinical comorbidity in osteoarthritis: Associations with physical function in older patients in family practice. J. Rheumatol. 2007, 34, 1899–1904. [Google Scholar]
- Kadam, U.T.; Croft, P.R. Clinical multimorbidity and physical function in older adults: A record and health status linkage study in general practice. Fam. Pract. 2007, 24, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Sharma, L.; Song, J.; Felson, D.T.; Cahue, S.; Shamiyeh, E.; Dunlop, D.D. The role of knee alignment in disease progression and functional decline in knee osteoarthritis. JAMA 2001, 286, 188–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shohat, N.; Machluf, Y.; Farkash, R.; Finestone, A.S.; Chaiter, Y. Clinical Knee Alignment among Adolescents and Association with Body Mass Index: A Large Prevalence Study. Isr. Med. Assoc. J. 2018, 20, 75–79. [Google Scholar] [PubMed]
- Hunter, D.J.; Bierma-Zeinstra, S. Osteoarthritis. Lancet 2019, 393, 1745–1759. [Google Scholar] [CrossRef]
- Wallace, I.J.; Worthington, S.; Felson, D.T.; Jurmain, R.D.; Wren, K.T.; Maijanen, H.; Woods, R.J.; Lieberman, D.E. Knee osteoarthritis has doubled in prevalence since the mid-20th century. Proc. Natl. Acad. Sci. USA 2017, 114, 9332–9336. [Google Scholar] [CrossRef]
- Driban, J.B.; Hootman, J.M.; Sitler, M.R.; Harris, K.P.; Cattano, N.M. Is Participation in Certain Sports Associated With Knee Osteoarthritis? A Systematic Review. J. Athl. Train. 2017, 52, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Arliani, G.G.; Astur, D.C.; Yamada, R.K.F.; Yamada, A.F.; Miyashita, G.K.; Mandelbaum, B.; Cohen, M. Early osteoarthritis and reduced quality of life after retirement in former professional soccer players. Clinics 2014, 69, 589–594. [Google Scholar] [CrossRef]
- Van de Pol, G.J.; Arnold, M.P.; Verdonschot, N.; van Kampen, A. Varus alignment leads to increased forces in the anterior cruciate ligament. Am. J. Sports Med. 2009, 37. [Google Scholar] [CrossRef] [PubMed]
- Isın, A.; Melekoğlu, T. Genu varum and football participation: Does football participation affect lower extremity alignment in adolescents? Knee 2020, 27, 1801–1810. [Google Scholar] [CrossRef]
- Thaller, P.H.; Fürmetz, J.; Chen, F.; Degen, N.; Manz, K.M.; Wolf, F. Bowlegs and Intensive Football Training in Children and Adolescents. Dtsch. Arztebl. Int. 2018, 115, 401–408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abreu, A.V.D.; Barbosa, J.R.P.; Paiva, F.J.D. Alinhamento dos joelhos no plano frontal dos 12 aos 17 anos [Alignment of the knees in the frontal plane from 12 to 17 years]. Rev. Bras. Ortop. 1996, 31, 83–88. [Google Scholar]
- Witvrouw, E.; Danneels, L.; Thijs, Y.; Cambier, D.; Bellemans, J. Does soccer participation lead to genu varum? Knee Surg. Sports Traumatol. Arthrosc. 2009, 17, 422–427. [Google Scholar] [CrossRef]
- Asadi, K.; Mirbolook, A.; Heidarzadeh, A.; Mardani Kivi, M.; Emami Meybodi, M.K.; Rouhi Rad, M. Association of Soccer and Genu Varum in Adolescents. Trauma. Mon. 2015, 20, e17184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreland, J.R.; Bassett, L.W.; Hanker, G.J. Radiographic analysis of the axial alignment of the lower extremity. J. Bone Joint Surg. Am. 1987, 69, 745–749. [Google Scholar] [CrossRef]
- Tang, W.M.; Zhu, Y.H.; Chiu, K.Y. Axial alignment of the lower extremity in Chinese adults. J. Bone Joint Surg. Am. 2000, 82, 1603–1608. [Google Scholar] [CrossRef] [Green Version]
- Della Villa, F.; Buckthorpe, M.; Grassi, A.; Nabiuzzi, A.; Tosarelli, F.; Zaffagnini, S.; Della Villa, S. Systematic video analysis of ACL injuries in professional male football (soccer): Injury mechanisms, situational patterns and biomechanics study on 134 consecutive cases. Br. J. Sports Med. 2020, 54, 1423–1432. [Google Scholar] [CrossRef]
- Prader, A.; Largo, R.H.; Molinari, L.; Issler, C. Physical growth of Swiss children from birth to 20 years of age. First Zurich longitudinal study of growth and development. Helv. Paediatr. Acta Suppl. 1989, 52, 1–125. [Google Scholar]
- Hinman, R.S.; May, R.L.; Crossley, K.M. Is there an alternative to the full-leg radiograph for determining knee joint alignment in osteoarthritis? Arthritis Rheum. 2006, 55, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Navali, A.M.; Bahari, L.A.S.; Nazari, B. A comparative assessment of alternatives to the full-leg radiograph for determining knee joint alignment. Sports Med. Arthrosc. Rehabil. Ther. Technol. 2012, 4, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brouwer, R.W.; Jakma, T.S.C.; Bierma-Zeinstra, S.M.A.; Ginai, A.Z.; Verhaar, J.A.N. The whole leg radiograph: Standing versus supine for determining axial alignment. Acta Orthop. Scand. 2003, 74, 565–568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.-C. Is clinical measurement of anatomic axis of the femur adequate? Acta Orthop. 2017, 88, 407–410. [Google Scholar] [CrossRef] [Green Version]
- Schmitt, H.; Kappel, H.; Moser, M.T.; Cardenas-Montemayor, E.; Engelleiter, K.; Kuni, B.; Clarius, M. Determining knee joint alignment using digital photographs. Knee Surg. Sports Traumatol. Arthrosc. 2008, 16, 776–780. [Google Scholar] [CrossRef] [PubMed]
- Sheehy, L.; Cooke, T.D.V.; McLean, L.; Culham, E. Standardized standing pelvis-to-floor photographs for the assessment of lower-extremity alignment. Osteoarthr. Cartil. 2015, 23, 379–382. [Google Scholar] [CrossRef] [Green Version]
- Paley, D.; Pfeil, J. [Principles of deformity correction around the knee]. Orthopade 2002, 29, 18–38. [Google Scholar] [CrossRef]
- Weston, M.; Castagna, C.; Impellizzeri, F.M.; Bizzini, M.; Williams, A.M.; Gregson, W. Science and medicine applied to soccer refereeing: An update. Sports Med. 2012, 42, 615–631. [Google Scholar] [CrossRef]
- Bavarian Football Association BFV. [The BFV Referee Training]. 2023. Available online: https://www.bfv.de/bildung-und-foerderung/schiedsrichterausbildung/schiedsrichterausbildung (accessed on 25 May 2023).
- Krustrup, P.; Bangsbo, J. Physiological demands of top-class soccer refereeing in relation to physical capacity: Effect of intense intermittent exercise training. J. Sports Sci. 2001, 19, 881–891. [Google Scholar] [CrossRef]
- Krutsch, W.; Lehmann, J.; Jansen, P.; Angele, P.; Fellner, B.; Achenbach, L.; Krutsch, V.; Nerlich, M.; Alt, V.; Loose, O. Prevention of severe knee injuries in men’s elite football by implementing specific training modules. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 519–527. [Google Scholar] [CrossRef]
- Loose, O.; Achenbach, L.; Fellner, B.; Lehmann, J.; Jansen, P.; Nerlich, M.; Angele, P.; Krutsch, W. Injury prevention and return to play strategies in elite football: No consent between players and team coaches. Arch. Orthop. Trauma. Surg. 2018, 138, 985–992. [Google Scholar] [CrossRef]
- Ekstrand, J.; Hägglund, M.; Waldén, M. Injury incidence and injury patterns in professional football: The UEFA injury study. Br. J. Sports Med. 2011, 45, 553–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krutsch, W.; Zeman, F.; Zellner, J.; Pfeifer, C.; Nerlich, M.; Angele, P. Increase in ACL and PCL injuries after implementation of a new professional football league. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 2271–2279. [Google Scholar] [CrossRef] [PubMed]
- Bizzini, M.; Junge, A.; Bahr, R.; Dvorak, J. Injuries and musculoskeletal complaints in referees--a complete survey in the top divisions of the swiss football league. Clin. J. Sport. Med. 2009, 19, 95–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szymski, D.; Opitz, S.; Pfeifer, C.; Rupp, M.; Angele, P.; Alt, V.; Krutsch, W.; Krutsch, V. High injury rates and weak injury prevention strategies in football referees at all levels of play. Scand. J. Med. Sci. Sports 2022, 32, 391–401. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Inclusion Criterions | Exclusion Criterions |
|---|---|
|
|
| FP | REF | p Value | ||
|---|---|---|---|---|
| n | 28 | 29 | ||
| age (years) | mean ± SD min–max | 17.4 ± 0.7 16–18 | 17.3 ± 1.0 15–19 | 0.73 |
| weight (kg) | mean ± SD min–max | 72.2 ± 8.8 58.1–97.4 | 72.2 ± 9.4 58.3–101.7 | 0.998 |
| height (cm) | mean ± SD min–max | 181.0 ± 6.2 168–197 | 179.6 ± 5.9 165–191 | 0.38 |
| BMI (kg/m2) | mean ± SD min–max | 22.0 ± 2.4 18.2–27.0 | 22.4 ± 2.6 17.4–30.0 | 0.61 |
| FP | REF | p Value | ||
|---|---|---|---|---|
| n | 28 | 29 | ||
| overall exposure per week (min) | mean ± SD | 274 ± 72 | 285 ± 94 | 0.61 |
| training exposure per week (min) | mean ± SD | 245 ± 76 | 182 ± 90 | 0.006 |
| match exposure (matches/season) (min/week) (1 match ≙ 90 min) | mean ± SD | 16.6 ± 7.8 29 ± 14 | 44.0 ± 21.9 76 ± 37 | <0.001 |
| seasons actively played (n) | mean ± SD | 12.0 ± 2.4 | 3.3 ± 1.6 | <0.001 |
| FP | REF | p Value | ||
|---|---|---|---|---|
| n | 28 | 29 | ||
| ICD/IMD (mm) | mean ± SD | 17 ± 25 | 13 ± 27 | 0.55 |
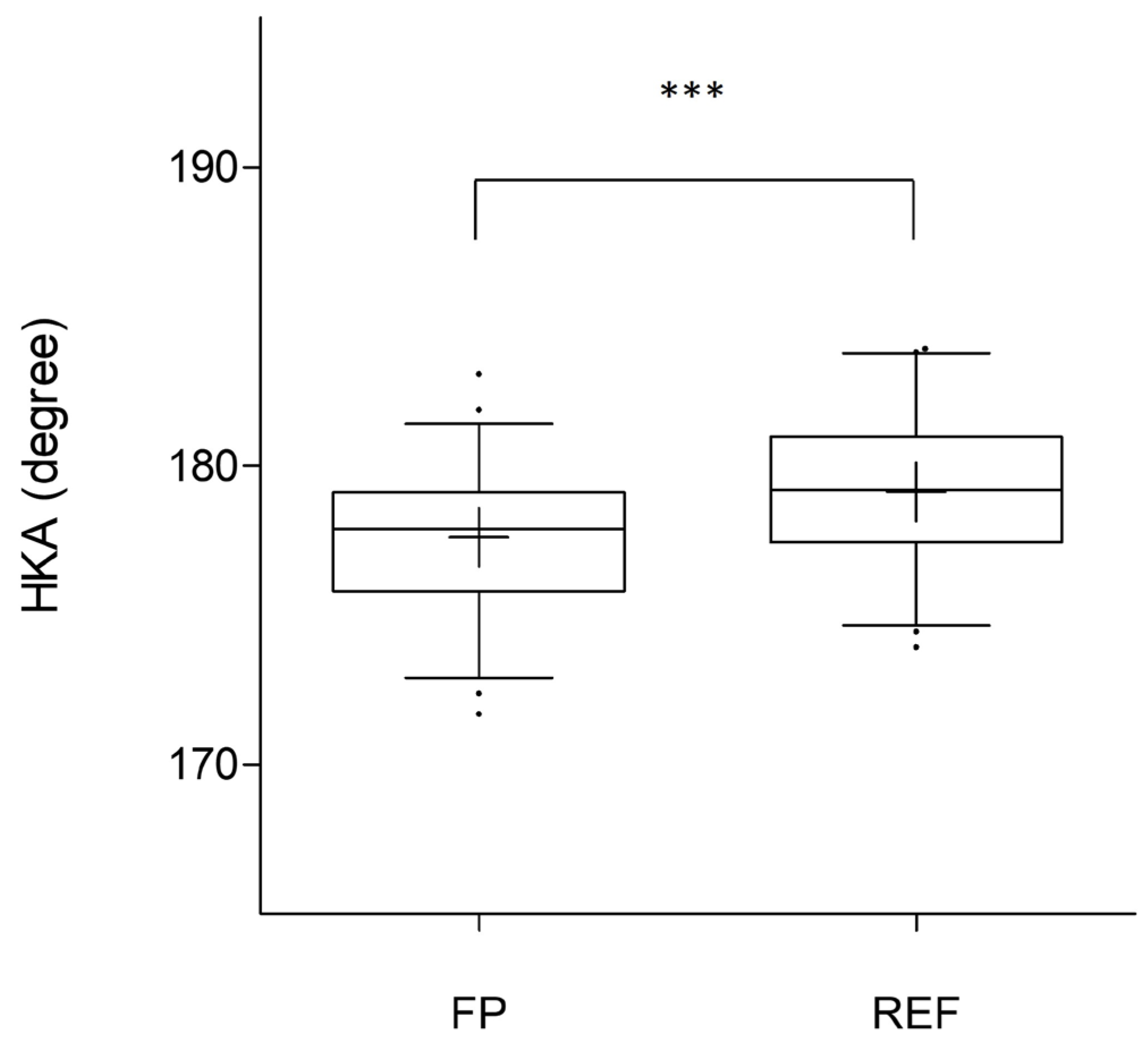
| HKA overall (degree) | mean ± SD | 177.6 ± 2.4 1 | 179.1 ± 2.4 1 | <0.001 |
| HKA dominant (degree) | mean ± SD | 177.8 ± 2.4 | 179.3 ± 2.5 | 0.031 |
| HKA nondominant (degree) | mean ± SD | 177.4 ± 2.4 | 179.0 ± 2.4 | 0.015 |
| Thigh circumference overall (cm) | mean ± SD | 51.9 ± 3.3 1 | 49.5 ± 3.6 1 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Memmel, C.; Denzlein, A.; Szymski, D.; Huber, L.; Achenbach, L.; Gerling, S.; Alt, V.; Krutsch, W.; Koch, M. Playing Football as a Risk Factor for Lower Leg Malalignment?—Comparing Lower Leg Axis of Male Adolescent Football Players and Referees. Appl. Sci. 2023, 13, 7928. https://doi.org/10.3390/app13137928
Memmel C, Denzlein A, Szymski D, Huber L, Achenbach L, Gerling S, Alt V, Krutsch W, Koch M. Playing Football as a Risk Factor for Lower Leg Malalignment?—Comparing Lower Leg Axis of Male Adolescent Football Players and Referees. Applied Sciences. 2023; 13(13):7928. https://doi.org/10.3390/app13137928
Chicago/Turabian StyleMemmel, Clemens, André Denzlein, Dominik Szymski, Lorenz Huber, Leonard Achenbach, Stephan Gerling, Volker Alt, Werner Krutsch, and Matthias Koch. 2023. "Playing Football as a Risk Factor for Lower Leg Malalignment?—Comparing Lower Leg Axis of Male Adolescent Football Players and Referees" Applied Sciences 13, no. 13: 7928. https://doi.org/10.3390/app13137928
APA StyleMemmel, C., Denzlein, A., Szymski, D., Huber, L., Achenbach, L., Gerling, S., Alt, V., Krutsch, W., & Koch, M. (2023). Playing Football as a Risk Factor for Lower Leg Malalignment?—Comparing Lower Leg Axis of Male Adolescent Football Players and Referees. Applied Sciences, 13(13), 7928. https://doi.org/10.3390/app13137928