Abstract
Virtual reality has been widely used in various industries, such as entertainment, communication, and healthcare, to mention a few. In the health industry, in combination with the brain–computer interfaces (BCIs), virtual reality could produce rehabilitation measures that may contribute novel strategies such as remote rehabilitation or telerehabilitation. The design and development of BCIs integrate different processes, including biosignals acquisition and processing, feature extraction and selection, classification of signals, and application of the technology to patients under rehabilitation treatments. This manuscript presents a literature review of the papers focused on the implementation of BCI and assistive technologies for remote rehabilitation based on virtual reality implementation. The purpose of this comprehensive review is to identify those studies that take advantage of virtual reality in combination with a biomedical technology to improve the performances of diverse rehabilitation processes. Various revisited studies provided a complete system for remote rehabilitation. These findings could lead to applying these models in diverse rehabilitation tasks.
1. Introduction
According to the World Health Organization (WHO), of the world population, over 1 billion people have a disability [1]. The International Society for Prosthetics and Orthotics has estimated that people needing prostheses or orthotics and related services represent 0.5% of the population in developing countries. However, in low- and middle-income countries, the rates of needing these services are increasing. For example, 75 million people need a wheelchair, being 1% of the world’s population. This type of requirement is known as a physical or motor disability. A physical disability, impairment, or reduced motor mobility limits the body’s movement. Motor mobility limitations can affect the upper and lower limbs, including the mobility difficulty of any limb or its loss. Such restriction could affect persons since birth, due to a syndrome/disease or by accident [2].
The rehabilitation concept is applied to a range of clinical methods to offer solutions to several disability conditions, including intervention to improve body functions (social, environmental, or physical) that allow the reinsertion of a person into society while intending to improve the quality of life. The rehabilitation evaluates the body functions, structures, activities, participation, environmental factors, and personal factors that can contribute to a person’s social interaction [3].
It is essential to emphasize the necessity of maintaining the continuity of the rehabilitation and therapeutic conditions. One of the goals of rehabilitation [3] is to reduce the effects of negative health conditions. Therefore, it must be conceived as a complete process (Figure 1 [3]) whose importance lies in improving health, reducing the costs of patient stays in hospitals, and improving the quality of life. If rehabilitation actions are not performed, this causes a delay and a deterioration in the patient’s health, and in general, diminishes the individual’s opportunity to fend for themselves and interact with society. One of the many variants for the implementation of rehabilitation is therapy. The therapy is responsible for preventing a loss or deterioration of the functions involving a disability and is composed of measures or applications such as physical exercises, education, consultancies for the correct therapy application, and assistive technologies.
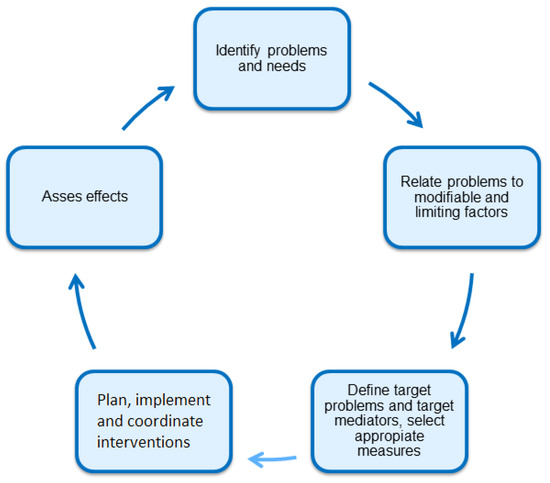
Figure 1.
Rehabilitation process.
Due to various conditions (such as the lockdown by COVID-19 and the increase in average life expectancy, among others), access to rehabilitation technologies has become difficult. Contradictorily, the need for rehabilitation options has risen during the same period. These facts, coupled with the condition that there are insufficient health professionals trained to deal with these problems, made it imperative to improve the conditions for access to rehabilitation facilities, techniques, strategies, and professionals. Notice that the number of people who are considered to receive therapy due to some disabilities is smaller than the number of people that suffer from a disability (around 50% of the population with a disability do not take measures to do an appropriate rehabilitation process). This is because, due to the many conditions, they cannot afford their therapy/treatment and cannot attend the therapy sessions due to isolation. Therefore, such cases were not considered in the data collection of a population group needing therapy, etc. [3].
Rehabilitation is a continuous effort among various sectors: health professionals, education specialists, the business sector, society in general, etc. However, unfortunately, there are places and conditions where the considered rehabilitation strategies are insufficient for the population. This condition implies that other actions must be taken to ensure proper rehabilitation evolution. Since the rehabilitation benefits increase when it is applied earlier, it is crucial to have the necessary human, economic, and technical resources for its application. Consequently, the medical services opt to use emerging assistive technologies such as remote rehabilitation (RR) or telerehabilitation [4] because they can be implemented using either portable or wearable systems, such as EEG-based BCIs, or robotic systems. RR is becoming an alternative to bring rehabilitation to larger human populations and maintain the same benefits in remote communities where the lack of health facilities and infrastructure is evident.
Implementing RR technologies has numerous advantages [5], such as providing the possibility of developing a rehabilitation strategy in places far away from a medical rehabilitation center and the opportunity to have a rehabilitation environment similar to the one in which daily activities take place, rather than in a rehabilitation-controlled facility. RR techniques also allow for monitoring health conditions and registering faster rehabilitation advances, among others. Additionally, this has some cons, such as the cost of the final system used for virtual rehabilitation, which could be expensive, or the impossibility of using an electrical supply and/or Internet in remote places such as mountains or rural environments.
In view of the increasing interest in RR, this document presents a review of the literature that contains various studies on the application of BCI and emerging technologies, such as virtual reality (VRy), for RR and its relative disciplines. The present research aims to identify relevant works and BCI integration techniques that have achieved the best practical application performance. This performance is measured using the information in different databases, the signal feature-extraction techniques of EEG, and the algorithms for the selection and classification of this type of signal. Previous studies [6] lead us to find the best models for this task and could bring us the opportunity to improve different tasks, and in the future, apply these models in other areas.
This document aims to comprehensively analyze the current results on BCI for virtual rehabilitation and remote technology on EEG for assistive devices. We propose this review, given the relevance of virtual rehabilitation for assistive devices and taking into account the lack of bibliography sources that integrate these technologies.
This review document is organized as follows: Section 1 presents a brief introduction to the concepts mentioned in the present work. Section 2 presents the research performed in Google Scholar, Web of Science, and Scopus. Section 3 provides a statement of the technology that allows a BCI and how these devices are used for rehabilitation. Section 4 presents the EEG databases most employed for BCI systems. Section 5 and Section 6 introduce the concepts of feature extraction and selection and the different techniques for obtaining them, respectively. Section 7 mentions the information about the machine learning (ML) techniques for EEG classification. In Section 8 are described the works related to BCI technology, and Section 9 explains how these BCIs are implemented in remote and virtual rehabilitation. Finally, Section 10 discusses how these emerging technologies could be used to improve the performances of BCIs and the consequent rehabilitation using virtual technologies.
2. Methodological Strategy
The present review is based on an exhaustive search that was performed to obtain information about using EEG signals to integrate a BCI and applying diverse technologies to implement RR. Searching scientific results was done using various motor engines, such as Google Scholar, Web of Science, and Scopus. The keywords used for the search and their combinations are listed below.
- Virtual rehabilitation.
- Remote rehabilitation.
- EEG BCI.
- Remote rehabilitation BCI.
- Machine learning BCI.
Two types of searches were done to filter the information. The first search was limited by a period that begins in 2018 and ends in the present year, 2022. This enabled the discovery of recent papers relevant to the general context of this study. A second filter allowed us to retrieve documents from before 2018. The CiteScore of Web of Science and the journal impact factor of the papers were used to obtain remarkable information.
The exclusion criteria removed studies of EMG signal classification BCI and other kinds of BCI that did not employ EEG signals as their main control input, and studies on BCI that are not related to RR or rehabilitation.
The PRISMA diagram on the searching criterion is portrayed in Figure 2 [7]. This figure explains the studies included in the present paper.
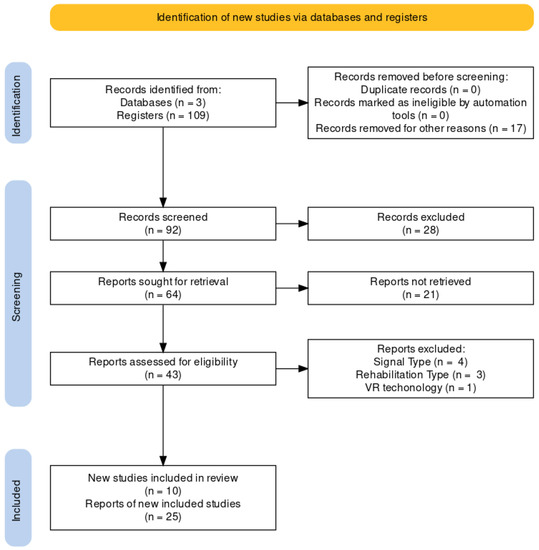
Figure 2.
PRISMA diagram of the present work.
Figure 3 represents the number of publications under the BCI topic over the last 20 years, which could bring information about the growth of the number of publications that alludes to this topic.
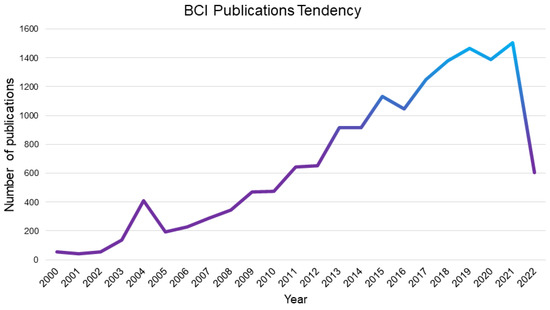
Figure 3.
BCI tendency of number of publication by year.
Figure 4 reflects the number of publications under “Virtual Rehabilitation and Assistive devices” in the period of 2011 to 2022.
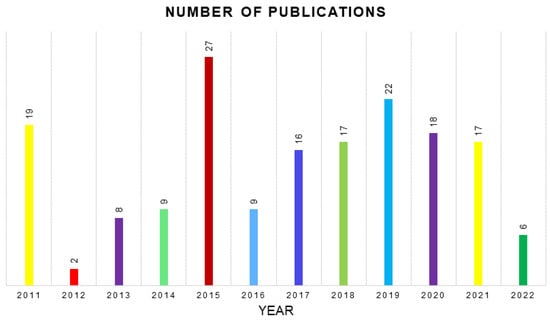
Figure 4.
Number of publications related to “Virtual Rehabilitation and Assistive devices” by year [8].
Figure 5 presents the literate map done with Litmaps application [9]. The articles here are presented as a node map, with 165 nodes, where a large number of citations represents a greater node size. The node connections represent the concept or area of the different used studies.
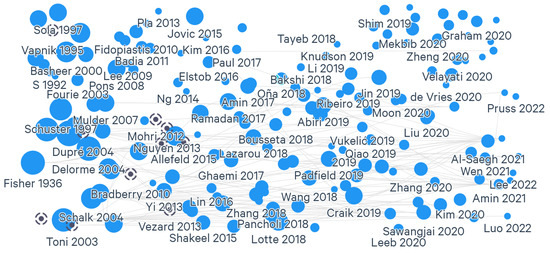
Figure 5.
Literature map of citations of the present work.
3. Overview of BCI Technology and BCI-Based Rehabilitation
Assistive technology is an object; piece of equipment; or commercial, homemade, or other product used to increase, maintain, or improve the functional capacities of individuals with some disability. These technologies can be as simple as glasses (to improve vision) or as complex as prosthetics, orthotics, and other devices dedicated to helping a person prevent loss of function or restore function. Among these technologies, BCI is a relevant technology due to its multiple applications in diverse rehabilitation methods. Figure 6 [10] reflects the different impairments and some of the technologies available to restore functions and improve life quality.
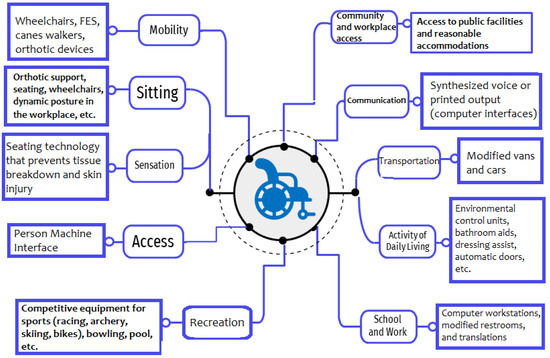
Figure 6.
Specific impairments and related technologies.
BCIs [11] are systems designed to study the brain’s electrophysiological response and encode, which permits a person to communicate with the environment. Various biosignals can support BCI [12]. Those signals reflect the information of the body. They could be measured and monitored through EEG information, functional magnetic resonance imaging (fMRI), magnetic resonance imaging (MRI), electrocorticography (ECoG), magnetoencephalography (MEG), and others.
For the implementation of BCI, EEG signals have gained great popularity among the different available biosignals due to their cost, real-time response, portability, and other factors mentioned in [13]. As EEG is a technique representing neurocognitive processes, this study captures the brain activity as a consequence of perception; talking, moving, and thinking are high-speed processes. Such a signal could be used in different BCI applications, as mentioned in [14], in various fields, such as gaming, arts, and health applications.
BCIs could be helpful for rehabilitation. They may help patients visualize the restoration through computerized systems and reduce the possibility of abandoning therapy by showing the patient a gradual but objective improvement. As a result of the pandemic (COVID-19), rehabilitation services were severely affected or disrupted [15]. Hence, BCIs can help people access their therapies, a possible solution for removing the mobility barrier; with these techniques, patients will not need to be transferred to a medical center for rehabilitation.
A human–computer interface is a connection between a person and a computer through technical devices, such as a suitable sensor. These systems have many design factors; one of the most important is the biosignal that triggers the system. Others are the algorithm that allows the classification of the signal, the way to control the system, and the final purpose or application of the rehabilitation system. For example, in [16] are highlighted not only the studies referred to as HCI or BCI that employ EEG signals, but those that use BCI triggered by electromyographic signals or a combination of both. Furthermore, some systems are triggered by other signals, such as EoG (electrooculography, the movement of the eye muscles).
BCIs are systems that connect a computer and a human user based on the power of the brain signals (EEG). This interconnection is the reason that justifies this technology gaining popularity in the rehabilitation field [17]. Some advantages of choosing EEG as a trigger signal for BCI are mentioned in [13], such as the fact that EEG study can capture the brain activity dynamics because many cognitive processes (such as perception, linguistic, motor, and cognition itself) are high-speed processes. Additionally, this study measured the neurocognitive processes directly of the neural activity through the voltage fluctuations representing the neurons’ biophysical changes. In contrast, there are a few disadvantages of analyzing EEG signals; most are related to the signal’s complexity and consequent processing.
4. Source of EEG Information and Data Handling
The importance of choosing a piece of input information associated with the BCI’s goal is enforced. Typically, this input information is composed of different public or private databases (such as [18])) containing a series of EEG recorded files. Descriptions of some of the most popular public databases can be found in the next lines.
4.1. Motor/Imagery Physionet
Motor Imagery Dataset by Physionet (Physionet) is a database consisting of 1500 recordings of 1–2 min obtained from 109 volunteers on 64 EEG channels using the BCI2000 system [19]. This database was used in the previous classification studies [20] with different features extracted from the raw information. Each subject performed 14 experimental runs with the following characteristics: two one-minute baseline runs (one with eyes open, one with eyes closed) and three experimental runs of two minutes of each of the following four tasks:
- Open and close the left or right fist.
- Imagine opening or closing the left or right fist.
- Open and close both fists or both feet.
- Imagine opening and closing both fists or both feet.
4.2. BCI Competition III
This is a collection of public datasets. Each dataset has an identification number and different characteristics. According to the official site, the goal of the “BCI Competition III is to validate signal processing, and classification methods for Brain–Computer Interfaces (BCIs)” [21]. The differences between the information of each dataset are the reason that is used in several investigations. Some of the most used datasets for BCI are described here:
- Dataset II (P300 speller paradigm). This set is a record of P300 evoked potentials focused on predicting a character out of 36 different characters (a 6-6 matrix). It comprises 36 classes, 64 EEG channels (0.1–60 Hz), 240 Hz sampling rate, 85 training trials, and 100 test trials recorded with the BCI2000 system.
- Dataset IIIa (motor imagery, multi-class). This dataset measures the kappa-coefficient motor imagery task with four classes (left hand, right hand, foot, tongue) from 3 subjects. It comprises four classes, 60 EEG channels (1–50 Hz), 250 Hz sampling rate, and 60 trials per class.
- Dataset IIIb (motor imagery with the non-stationary problem). Dataset IIIb consists of the three recordings S4, X11, and O3VR with 1080, 1080, and 640 trials. Due to a mistake, trials 1–160 and 161–320 in O3VR are equal. This means that in 2 × 75 (out of 640) trials, one can obtain the test set labels by looking at the label of the corresponding trials. In order to remove the repetition of testing data, the first 160 trials (containing another 43 testing trials) will not be considered in the final evaluation. Accordingly, the number of testing trials in O3VR will be reduced to 202 (out of 480).
- Dataset IVa (Motor imagery, small training sets). This set is focused on motor imagery tasks with two classes (right hand, foot) from 5 subjects; for two subjects, most trials are labeled (80% and 60%, respectively), and for the other three, less and less training data are given (30%, 20%, and 10%, respectively). It was created to probe the EEG classification with small data. The general composition is two classes, 118 EEG channels (0.05–200 Hz), 1000 Hz sampling rate, and 280 trials per subject.
- Dataset IVb (Motor imagery, uncued classifier application). It is training data for motor imagery with two classes (left hand, foot) from one subject, with continuous data intended to specify when the mental state changes from movement to movement. The labels are: −1 for the left hand, 1 foot, and 0 rest averaged over all samples. This is from 118 EEG channels (0.05–200 Hz), 1000 Hz sampling rate, 210 training trials, and 12 min of continuous EEG for testing.
As mentioned before, these datasets were used in different situations, according to the intention of the research. For example, Dataset IV (BCI III IV) was used in [22] and the Physionet dataset was used in [23], as can be seen in Table 1.

Table 1.
Databases’ characteristics.
Besides the described databases, there are some others available in the public sector that were designed under MI conditions. Some of these databases are used in other signal processing studies. For example, there exists BCI IV that is a composed of five datasets. Three of those data sources are focused on EEG signals with MI conditions. The study [22] used this source of information as part of a signal classification process for BCI creation. Other public available datasets are the GigaScience Database [35], which contains MI information on 52 subjects; the Grasp and Lift EEG Challenge [36] which contains information of 12 subjects and 10 series of trials of 6 motor tasks; and the High Gamma dataset that was used in [37]. In addition, there are some public EEG datasets focused on other paradigms and signals that can be mixed with the records of other types of signals (such as EMG).
Once the information sources are available, they must be processed to obtain the needed components that could processed in the BCI implementations. These processing tools include feature extraction and feature selection tools. These are described ahead in the next two sections.
5. Feature Extraction
Feature extraction is the method that recovers the critical information of unprocessed data sources. These features depend on the aim or scope of the research. Different feature-extraction techniques exist—for example, the ones related to the power bands, the techniques that extract information in the time domain, the ones focused on the frequency domain, and the combination of the two called time-domain techniques. Additionally, some techniques are related to spatial information, and others techniques involve information of noisy signals [38]. These techniques are listed (Figure 7) and described here.
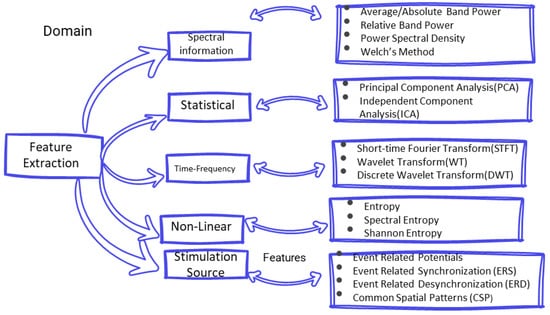
Figure 7.
Feature extraction techniques.
5.1. Spectral Information
The spectral information describes how the power of EEG signal varies in some specific frequency bands [39]. Frequency bands define the cerebral activity measured through the electrodes in the EEG study. These frequency bands are beta, alpha, theta, delta, and gamma. They work in below 3.5 Hz to above 30 Hz [40]. These power bands are obtained from the information that each channel record of the scalp surface. Usually, these bands allow one distinguish the energy that is related to a concentrate or sleep state.
- Average band power/absolute band power. One single number summarizes the given frequency band’s contribution to the signal’s overall power, which is useful in a machine-learning approach.
- Relative band power. It is the percentage of the total of the band’s frequency in the signal’s total. It is calculated on the mean of the band power.
- Power spectral density (PSD). PSD is defined by oscillatory activity and can be associated with the synchronous activity of motor units. This feature estimates how the total power of the signal is distributed over its frequency. It is important because many other features are obtained by applying a mathematical analysis of PSD [38].
- Welch’s method. In [41], it is described as an averaged periodogram of a signal. The method divides the signal into segments and overlaps these segments according to a window. Then, the discrete Fourier transform of each segment is calculated, and the average of the periodograms of it. The Welch method is yet another approach for spectral density estimation. For this method, one can use fast Fourier transformation or a periodogram. Despite the technique employed, two important facts must be considered: smaller data chunks of time series and their averaged PSD estimates.
5.2. Statistical Analysis
Many feature extraction methods for BCIs are based on the statistical information of EEG information. The two more extensively used are:
- Principal component analysis (PCA) is a dimensionality-reduction method that is often used to reduce the dimensionality of large data sets (such as in the case of EEG information), by transforming a large set of variables into a smaller one that still contains most of the information in the large set. Reducing the number of variables of a dataset naturally comes at the expense of accuracy [42].
- Independent component analysis [42] (ICA). This method is used when mixed signals are separated into individual component signals. Independent component analysis (ICA) is a statistical and computational technique for revealing hidden factors that underlie sets of random variables, measurements, or signals. ICA defines a generative model for the observed multivariate data, which is typically given as a large database of samples. In the model, the data variables are assumed to be linear mixtures of some unknown latent variables, and the mixing system is also unknown. The latent variables are assumed non-Gaussian and mutually independent, and they are called the independent components of the observed data. These independent components, also called sources or factors, can be found by ICA.
Additionally, in the pre-processing step, we can find approaches to separate the source signal information of their components. Existing methods are classified as "blind methods". Blind methods are identified as a parallel of “unsupervised” methods because these types of techniques are based on output. Three types of algorithms are used based on the information that takes to do the analysis. These types are statistical independence of sources, positive, and sparsity [43]. Among these, there are algorithms such as ICA or PCA that allow obtaining the desired signal information, in the case of BCI the information related to the brain motor activity.
5.3. Time-Frequency
- Short-time Fourier transform. The short-time Fourier transform is based on how a signal can be sliced into several short data segments. In the end, all the segments can be concatenated from a spectral power in the time-frequency domain [41].
- Wavelet transform. According to [44], a discrete wavelet transform is “normally, defined as a non-redundant sampled CWT. The DWT aims to represent a discrete-time series, , as a set of (wavelet) coefficients”. This transformation can be represented as a filter bank of one half-band high pass and a half-band low pass component.
- Discrete wavelet transform (DWT). The DWT aims to represent a discrete-time series, , as a set of (wavelet) coefficients.
5.4. Non-Linear Methods
- Entropy. A measure of uncertainty; it represents the number of bits necessary to represent certain information [45] and can be used to measure the number of spectrum peaks, turning this into a mass function.
- Shannon entropy. It calculates a mass function that is related to the entropy values.
- Spectral entropy. It is a measure of the signal’s spectral power distribution based on the Shannon entropy calculation, where the normalized power distribution in the frequency domain is the probability distribution. According to [45], this entropy can be used as an estimate for voicing/unvoicing decisions; it is expected that flatter sub-bands will have higher entropy and the sub-bands where a formant will have low entropy. The mentioned work states that entropy is associated with a classifier’s output posterior’s distribution and can be used for different weighting streams in a multi-stream combination. In other applications, this entropy can represent an expected value of an output.
5.5. Feature Extraction Techniques for BCI according to the EEG Stimulation Source
The EEG analysis for BCI implementation adds new criteria to perform the feature extraction process. Mainly, these criteria are based on neuronal activity detection considering either internal or external brain stimulation.
If internal stimulation is analyzed, the (spontaneous) oscillatory activity is driving the feature extraction. In spontaneous systems, no external stimulation is required. Hence, BCI produces controlled actions based on the user mental activity.
Common spatial patterns (CSPs) is a filtering method to extract features from spontaneous activity based on multi-channel EEG information [46]. This is an algorithm that generates characteristics for classification [42]. The CSP generates weights for linear mapping where the variance (power) is optimized. The extracted power (by means of FFT, wavelet, etc.) is used as a feature.
In evoked systems, external stimulation is required, such as visual, auditory, or sensory stimulation. Therefore, feature extraction is enforced by the type and intensity of the external sources.
Mainly, the feature extraction methods when EEG is enforced by evoked potentials are event driven techniques. Additionally, there exist the event-related potentials that can be obtained by averaging EEG signals over a specific event type. Complmentarily, event-related synchronization (ERS) and event-related desynchronization (ERD) are common methods for detecting power changes in EEG information (promoter and inhibitor). The first is the increase in the activity in a particular band, and the second evaluates its decrease. These changes can be triggered by motor imagery, motor activity, and stimulation of the senses [14].
ERD/ERS produced by motor imagery cannot be classified in the evoked potentials. From [47] MI signals are of spontaneous type because they are generated based on a user’s imagination of performing a task.
6. Feature Selection
Feature selection (also called “dimension reduction”) is a process performed to determine a smaller group of characteristics that help complete information analysis. This is prone to reduce the computing time in the classification process and remarks on the features that could improve the classifier algorithm accuracy. There are different procedures and methods for feature selection. Being among the most popular, the metaheuristic procedure tries to answer an optimization model through heuristics (a search algorithm). It is used for selecting features from large sets of features because it can manage the severe dimensionality problem [47].
Likewise for the machine learning algorithms, the feature selection methods could be divided into unsupervised and supervised variants [48]. These methods are differentiated if there are labels available for characterized data. If the data possess a label, the feature selection could follow a supervised methodology; if not, it is considered an unsupervised feature selection. These methods are divided into four categories: filter, wrapper, hybrid, and embedded. The method selection depends on the data interaction in the algorithms, which define how the more critical features are extracted from the data.
The filter approach is based on statistical measures. The objective of this technique is to rank the features and hence isolate the most important information in databases. On the other hand, the wrapper approach makes a combination of information and evaluates it to find the most suitable for the system classification or the most relevant.
The hybrid methodology tries to combine a method that could generate a feature ranking and then use this list to evaluate the performance of the combination in the system. Finally, the embedded method integrates the selection process into the classification algorithm. The more visible algorithm is the decision tree, where the branches reflect the selection of certain information, and the growth process forms smaller subsets.
In [47], the systems that include a selection procedure for salient features achieve higher accuracy than the BCIs cases that are not involved in this process. The algorithms used for selecting features could be used for classification [49]. Additionally, there exists the manual feature selection, performed by a human expert, through direct observation, to label and remark on an important feature for the system. A list with some of the most used algorithms divided by their approach is presented as follows (Figure 8).
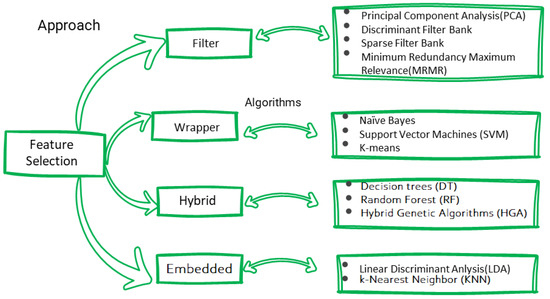
Figure 8.
Feature selection techniques.
6.1. Filter Approach
- Principal component analysis. PCA uses orthogonal transformations to set correlated variables into a set of linearly uncorrelated variables called principal components. This dimensional reduction [41] projects high-dimensional data along a direction for which the variance of the data is maximized in a linear subspace spanned by a small number of latent components.
- Discriminant filter bank. It overlaps frequency bands and uses a Fisher ratio to analyze each sub-brand’s band power to discriminant sub-bands. This analysis is performed on a single channel of EEG data [14].
- Sparse filter bank. It uses multiple frequency bands to optimize sparse patterns. To achieve this, the feature selection is completed using a supervised machine learning technique, such as Bayesians ones or super vector machines (SVMs) [14].
- MRMR (minimum redundancy maximum relevance). It is an algorithm that reduces redundant data within the database and maximizes the relevant information to classify [50].
6.2. Wrapper Approach
- Naïve Bayes. It is a family of simple probabilistic classifiers based on applying Bayes’ theorem, with strong independence assumptions between the features. That is why it is called naïve. This independence is calculated through distance metrics such as euclidean distance or cosine, to find the closest feature.
- Super vector machine (SVM). It is an algorithm that implements a kernel approach [14]. A kernel is a support vector that helps to separate classes in a hyperplane by representing the inputs in a space as inner products of another space. This type of algorithm has proven good accuracy for tasks that involve classification and regression [51].
- K-means. This algorithm aggregates observations by their similarity according to the response patterns.
6.3. Hybrid Approaches
- Decision trees. It is a classifier [14] that allows the creation of subgroups from the information; these final subgroups are called leaves. When the classification is tested, the tree makes “branches” with binary divisions and only retains the leaves where the group has a minor error.
- Random forest. This is a collection of decision trees; their branches are created according to the variable with a major association with the goal among the variables.
- Hybrid genetic algorithms. It is an iterative research method [52] inspired by the principles of natural selection, based on the generation of a population from the parents’ reproduction. The genetic algorithm optimized (find the maximum or minimum) an objective function using the natural selection principles through the function parameters.
6.4. Embedded Approaches
- Linear discriminant analysis (LDA). This algorithm is a statistical method defined by the probability of the joint discrete/categorical variables on their distribution. This algorithm [53] is the evolution of a statistical method designed to distinguish between classes of plants. It is defined by the probability of the joint discrete/categorical variables on their distribution.
- K-nearest neighbors (KNNs). The KNN algorithm classifies new values based on similarity [14]. This similarity is achieved using two centroids, and the distance is measured for all the observations. This is how the cluster is made; this centroid moves until the process end. This algorithm is used for data reduction because of its clustering ability.
Some studies of EEG signal classification use the cited algorithms in different combinations as input, selection, or classification algorithms. In addition, feature selection has been performed on raw EEG in the time domain. For example, the CNN algorithm [54] could be fed with signal values, calculated features, or images. This application provides a range for using this algorithm to find relationships between the signal information. Another algorithm that serves as an example is the ICA [47]. Some studies are mentioned as feature itself [55], and others as a part of the selection algorithms. Even though ICA is also used for noise reduction as a pre-processing algorithm, depending on the focus of the study and the type of information analyzed, recall that some studies of motor/imagery identification use raw signal information and other preferred calculated features. Additionally, the methodology of some studies, such as [56], refers to the absence of a normalization process or a feature selection process. The information considered in Table 2 refers to some studies and their connections with these techniques.
Table 2.
Feature extraction and feature selection techniques.
7. Automatic Classification Algorithms for EEG Signals
As the nature of EEG signals is oscillating and continuous (EEG is a representation of a mental state composed of electrical activity) [40]), it is complex to deal with the raw information of these signals. Such conditions motivate the design of information classification techniques to extract relevant information or features that could allow using EEG in BCI and RR. These techniques extract features or characteristics of the signals and are parts of the branch of a discipline called “signal processing”.
Classification is a process that assigns a category (or “class”) to an object (or information) [63]. This class is an attribute that contains a group of information with similarities yielding an intrinsic description of their relationship. Usually, to get the precise classification, the classes must be labeled. A label is a name that characterizes the input data associated with a certain class. This process depends on the information that the study pretends to highlight and categorize, such as the movement or the conscious state of a person. The extracted features are different for each BCI application. However, many studies focus on the relationship between movement and imagination because this feature could improve the accuracy and application of BCI, which directly impacts the rehabilitation process. Figure 9 reflects the BCI implementation processes; Table 3 shows different ML techniques for EEG classification.
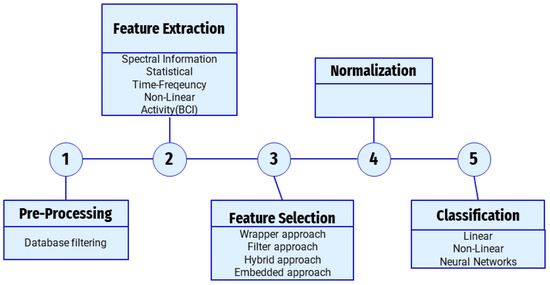
Figure 9.
BCI implementation process.
Machine learning is a form of applied statistics using computational power to estimate future values of a function [63]. This estimation is known as “learning”. This process involves from the categorization of certain data. As mentioned before, machine learning algorithms can be divided into supervised, unsupervised, and reinforcement learning [52]. The different machine learning algorithms are classified into “families”. These families are different in the way they rely on their mathematical methods for classifying data. The next section describes some of the families and the algorithms found in that category.
7.1. Linear
- Logistic regression. It is a classification model that computes the probability of a discrete outcome of an input variable. Essentially, logistic regression is a linear regression algorithm with a logistic function added before the output. This logistic function allows the compression of the output into a range of values between 0 and 1; this feature stands out when performing binary classification.
7.2. Non-Linear
- Quadratic discriminant analysis (QDA). This classifier assumes that data follow a Gaussian distribution and uses a quadratic distribution surface.
7.3. Neural Networks
The neural network (NN) is a type of machine learning algorithm that can “learn” from input data. The mathematical conception of learning using NN considers the application of a matrix transformation of the input information by a matrix called “weight”. These weight changes are according to a bias, which make it possible for the algorithm to predict a new input [63]. This allows one not only to classify but also to cluster the information and predict future responses of a system [17].
- Recurrent neural networks (RNNs). According to [47], they are neural networks that have circulation behavior thought calculations, and their output depends on the current input and the previous output.
- Long short-term memory (LSTM). LSTM contains memory cells that can preserve previous output states. Horchreiter and J. Schmidhuber [64] described this architecture as capable of “using their feedback connections to store representations of recent input events in the form of activations”, which means that this type of NN can store information.
- Convolutional neural networks (CNNs). The CNN is deep neural network architecture that relies on a specialized linear operation known as convolution [65]. This type of network can be a suitable model for processing various signals: images, audio, videos, and EEG.
Table 3.
EEG classification with ML algorithms.
Table 3.
EEG classification with ML algorithms.
| Author | Year | Dataset | Algorithm | Accuracy% |
|---|---|---|---|---|
| Gahenemi et al. [22] | 2017 | BCI Competition IV. Nine healthy participants. Imagination | SVM Improved Binary Gravitation Search Algorithm (IBGSA) | 76.24% |
| Abdelfattah et al. [20] | 2018 | Physionet Motor Movement/Imaginary Dataset | Neuronal Network | 89.5% |
| Zhang et al. [23] | 2018 | Physionet Motor Movement/Imaginary Dataset | CRNN | 98% |
| Bousseta et al. [66] | 2018 | Four users of Emotiv. Four Imaginary movements: left hand, right hand, both feet. | SVM | 85.45% |
| Tianwein et al. [67] | 2019 | Left hand brains motor region pre-processing. | CNN | Random |
| Zhang et al. [60] | 2020 | Physionet Motor Movement/Imaginary Dataset | LSTM | 78.95% |
| Netzer et al. [68] | 2020 | Physionet Motor Movement/Imaginary Dataset | Common Spacial Pattern | 70% |
| Lui et al. [69] | 2020 | 32 persons. 4 physical activities: left hand, right hand, foot and tongue) | CNN, K-means | 91.83% |
| Ghumman et al. [62] | 2021 | BCI Competition IV dataset 2a | SVM-PK | 67.0% |
| Huang et al. [70] | 2022 | Physionet(20, 50,80, 109 Subjects) | LRT-CNN | 93.86% 98.94% 93.04% 92.41% |
| Khademi et al. [24] | 2022 | BCI Competition IV dataset 2a | CNN-LSTM | 92% |
| Ghadir & Ghulam [37] | 2022 | BCI Competition IV 2a and High Gamma Dataset | CNN (MBEEGNet) | 82.01% 95.11% |
8. Brain–Computer Interfaces
Implementing a BCI requires a control algorithm that could regulate the commands to the computer and could help to improve the interaction between the final user and the system. This is obtained because of the level of interaction between humans and machines decides how versatile and adaptable the robotic system is. For example, the authors of [71] created a BCI to perform a pre-established function. This allows the movement and functioning of various parts of the robot, monitoring to reach the gap between the information in real-time, and the information the BCI needs to work adequately. On the other hand, in the project of [72], a prosthetic arm with six DOF, including an elbow extension, was built. This device allows the opening and closure of the robotic arm; five subjects validated the control scheme.
Bandara et al. [18] built a BCI with a dataset from six healthy subjects performing tasks such as rest, move, and drink. This information feeds an SVM algorithm and a NN for the classification. The achieved accuracy of classification was 69.4% for the SV and 71.4% for the neural network. Another study was preformed [73] with a BCI hybrid model for EEG and EMG. This study was focused on persons with amputations. The used dataset was a previous one by Li et al. [74]. This BCI counts with a feature extraction process that includes AR, RMS, WL, WAMP FR, MMNF, MMDF, and entropy; has a feature selection process; and uses three classification algorithms, QDA, KNN, and SVM, achieving accuracies of 98.97%, 98.90%, and 94.82% respectively. In the BCI of [75], the researchers used an Emotiv Epcot device to record C3, C4, and Cz signals and information channels; calculate their DWT; and fed a BiLSTM algorithm that achieved an accuracy of 87.14%.
Table 4 presents studies focused on implementing BCI with control devices.
Table 4.
BCI studies.
For disabled people, the application of machine learning tools could lead to control systems without the necessity of impulsing the movement through a damaged or missing body part. This increases life quality and the chance to reintegrate into everyday activities without external help.
The increasing number of studies in recent years has created the necessity to review some of them, so there exist different reviews that are focused on the BCIs, their trigger signals, their methods of composition, and other important concepts. For example, Padfield and coauthors [14] present the techniques and challenges in BCI, explaining the different techniques for feature extraction, selection, and classification. Additionally, the work in [76] is more focused on the classification algorithms for EEG signals, such as adaptive classifiers, matrix, and tensor classifiers, transfer learning methods, and deep learning methods. On the other hand, the study of [77] focuses on the different BCI paradigms (P300, Evoked Potential, etc.) and how they are implemented. This work includes classification methods in the analysis of the paradigms. The review presented in [47] is about the deep learning algorithms that try to classify the motor/imagery condition of the signals of EEG and also presents trends and information about the feature extraction, signal classification, and normalization process. This review only contains papers that use EEG signals as a base. Craik et al. [54], through a systematic review, analyzes the deep learning techniques and the architectures of the algorithms for EEG classification, and the EEG frequencies and the tasks that the studies reflect. On the other hand, [78] shows information about the countries that develop BCI technologies, the paradigms of EGG (that in this study are called control signals), the concept of BCI being invasive or non-invasive, and the software that is useful for BCI implementation. Finally, the most recent review of EEG BCI is focused on the application of BCIs for the rehabilitation of a patient after a stroke; it specifies the clinical outcomes and how the studies were designed [79].
In [14], several suggested branches of BCI applications are proposed. One is application-oriented toward monitoring a mental state, and the other is oriented toward controlling or manipulating an external device. Additionally, these BCI can be found in diverse fields, such as entertainment, medical, art, and gaming (see Figure 10 [14]).
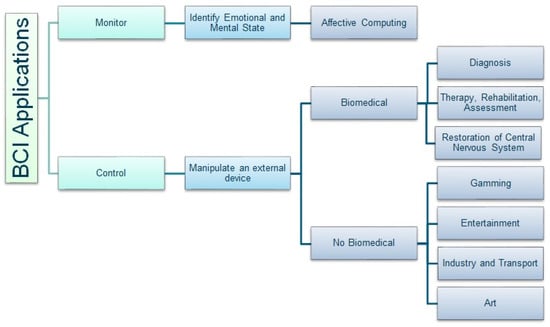
Figure 10.
BCI applications by their final uses.
Today many of these applications are non-invasive EEG applications, such as the ones described in [16], so the industry created EEG commercialized devices to register the signals. From the control point of view, these devices are categorized through their resolution: the number of channels or signals provided to find low, medium, or high-resolution devices. This resolution also determines the signal’s sample rate, the number of channels, and other characteristics. The non-invasive products are mostly “wearable” to enhance their wireless, portable, and affordable features [66]. These kinds of devices are used for the previously mentioned purposes. For example, the review work in [80] measures the commercial devices (such as Neuroskan and Emotive) of EEG and the fields where they were applied.
9. BCI Applications for Rehabilitation
9.1. Rehabilitation
The principal goal of rehabilitation is to provide a person with a way to fully integrate into society and live plenty in all dimensions: economic, social, educational, and healthy. To achieve this goal, the rehabilitation process involves various methods, techniques, strategies, and tools (as seen in Figure 6). The rehabilitation specialists, who are the healthcare professionals in charge of aiding people to recover from an illness or injury, are given the implementation of these strategies.
Examples of these professionals are physical therapists and occupational therapists. These specialists could aid in the recovery from different disabilities (sensory disability, communication disorders, difficulties in carrying out activities of daily living, etc.) through the descriptions of their illness and establishing rehabilitation tasks. Working together, they could create a standardized service system for rehabilitation. For proper functioning, these tools need information from the different measurements taken of a system to calculate a rehabilitation system’s performance. The rehabilitation process, for example, can be measured as the accomplishment of goals, a goal being the association of the ability to perform a specific task. For example, a person could perform some movements (such as a soft object lift), and the specialist could compare the result with the rehabilitation goal or information about the desired level of movement and measure the performance of the rehabilitation itself.
Among the rehabilitation specialists, there is a group focusing on mobility problems. Mobility encompasses the ability to move within a personal or public space and the difficulty of holding an object. The loss of the entire capacity of movement or having a dismissed capacity helps to understand the difference between the concepts of prosthetics and orthoses. While the former intends to provide a substitute for the ability or function and be able to recover it, the latter only provides help to the affected part.
One of the measures that help the mobility specialist is the Full Meyer Assessment Scale (FMA) [81]. This is an index to assess the sensor-motor impairment in individuals who have had a stroke. The scale contains other pairs of letters representing the measured body part; UE is for upper extremities, and LE is for lower extremities. The scale was studied extensively and has interesting psychometric properties. It assesses body function according to the International Classification of Functioning, Disability, and Health (ICF). The FMA motor assessment has a maximum score of 66 points for upper extremities and a maximum score of 34 points for lower extremities. These measures are recommended as core measures to be used in every stroke recovery and rehabilitation trial.
Additionally, there exist other measures focused on the characterization and performance of the system, not on the rehabilitation, that are helpful to assess the responses to rehabilitation goals. Measures such as the percentage of normality, a z-score, or a probabilistic number could define the ability of the system to meet the goal [10] and the success of practicing specific tasks of rehabilitation in order to bring a useful rehabilitation. This is the reason that could explain the two ways to measure the performance of the system through: (1) those tasks that characterize the human being and (2) those tasks that characterize the operation of the assistive system.
These rehabilitation systems, as mentioned before, could be as simple as a pair of glasses and as complex as a BCI. The success of the intervention does not depend on the complexity of the rehabilitation system but on the adequate implementation of the rehabilitation technologies.
Some recent studies have discussed the challenges of developing rehabilitation services and devices. For example, the study of Kamekov [82] is focused on the need for rehabilitation from a demographic, social, and geographical point of view. This review pretends to remark on the unmet needs in rehabilitation services and addresses the numerous barriers to accessing the rehabilitation process in developing countries. Another focus on rehabilitation is the integration of emerging technologies. In [83] are described ten years of health applications. These applications are useful for clinicians, patients, people interested in monitoring their lives state and health, and some that help implement telerehabilitation techniques. Finally, the review in [84] is focused on the proportion of older adults that can move outdoors and how rehabilitation could help to increase this activity through a review of 29 studies that talk about mobility programs for outdoor environments.
9.2. Virtual Rehabilitation
VRh is the use of virtual reality and virtual environments within the rehabilitation process [4]. This can be described as a real-world simulation using a computer and its human–machine interface (HMI). Simulating a natural environment that seems real allows people to focus on rehabilitation tasks and facilitates therapy, as it is a controlled environment, in addition to the fact that said therapy can be carried out in non-clinical environments. The use of VRh therapy makes people more motivated and willing to continue with it.
VRh is differentiated from remote rehabilitation (RR) (also known as Telerehabilitation) because RR is the implementation of rehabilitation in places of difficult access, and VRh is the implementation of rehabilitation in a virtual environment. Together, they have the power to facilitate therapy services in rural settings and provide home therapy programs; this makes it easy to continue with therapy exercises and stay motivated.
The appearance of VRh commercial devices, such as those integrated with video game consoles, addresses one of the downsides of this technology, leading to the emergence of different types of applications, as described below.
Types of Virtual Rehabilitation
By the type of population
- Musculoskeletal virtual rehabilitation. Orthopedic patients who suffer from bone or muscle/ligament injury are the targets. This is the numerous group that needs rehabilitation.
- Post-stroke virtual rehabilitation. These patients survived a neural hemorrhage or blood clot to the brain, resulting in body paralysis.
- Cognitive VRh. Population or groups of individuals with various psychological disorders such as deficit/hyperactivity, eating disorders, post-traumatic stress, and phobias.
- Telerehabilation. As mentioned before, this type of rehabilitation is focused on a population far from their clinical or lives in places of difficult access.
By rehabilitation protocol
- Augmented virtual reality. The patients receive a mixture of conventional exercises with clinical or home equipment and a VRh regimen of simulation exercises.
- Virtual reality-based. This type of rehabilitation differs from the therapeutic approach and includes exercises that are similar to playing a video game.
One of the first attempts to introduce a therapy with the use of virtual reality or games in rehabilitation was made in 2008 by a group of occupational therapist at the Glenrose Rehabilitation Hospital [4], located downtown in Edmonton, Alberta, using a Wii console with Wii sports software.
In recent times, diverse studies that develop a rehabilitation service using virtual reality systems or technology greatly benefit because one of the intentions of using VRy in rehabilitation is that the user or patient enhances the treatment and avoids abandoning the therapy. In this context, the authors of [85] used Unity 3D software and Kinect device to develop a game that emulates a medieval village (that was called Physionland), showing through questionnaires that the patients are more willing to accept a therapy with the use of games and virtual reality.
Gamification rehabilitation is an important topic for VRh, and studies use this concept to deliver the service needed. For example, in the study of [86] the context of telerehabilitation or remote rehabilitation using the tools of exergames was found. The exergames are games designed to involve physical activity; this paper presents a case study for an exergame for the upper-limb rehabilitation of stroke patients, which is an important application of rehabilitation because, in 2016, researchers [87] designed a videogame in the Unity platform focused on the rehabilitation post-stroke of 12 participants divided into three groups. After various sessions, they measured the game and FMA UE scores, finding improvements in both measures. A couple of years later, in 2019, the team that presented [88] also proposed a VRh system to rehabilitate the upper limb after a stroke. To achieve this, they designed a VRy environment system using Unity3D for the modeling of six different scenarios that provide three different clinical rehabilitation actions, including grasping, forearm rotation, and daily life exercises (drinking, eating fruit, solving a jigsaw puzzle, catching a butterfly, playing volleyball, and pulling a radish). An actiCHamp recorded this activity for eight channels. This information then enabled the multisensory-feedback system—visual, auditory, and haptic—that helps patients constantly adjust their state to motor feedback/imagery.
Another study on the use of gamification could be found in [89]. This study showed the application of a Hololens system and a Kinect-developed VRy system based on gamification that could provide rehabilitation for patients post-stroke. This system comprises the therapist module that asses the exercises and the patient module that provides the exercises. This feedback accomplished 36.2% deviation vs. the movement. The group with no VRy feedback obtained 68.4% deviation. Another application of gamification can be seen in Chantera et al. [90], where a VRh system using Kinect to rehabilitate left-handed people working in industrial environments is proposed. Their applications determine the level of risk of injury that a left-handed employee has when using machinery designed for right-handed people. They used a laterality scale score from 30 to 50 points. If the score was above 35, the person was considered left-handed and at risk of injury.
Today, there are devices that provide rehabilitation. An example of a device that could implement a rehabilitation service can be seen in [91]. This study designed a device based on sensors that could deliver rehabilitation for upper limbs and hands. Another device can be seen in [87]. This work involved designing a video game in Unity software. The participants were divided into groups, and at the end of the intervention, the authors measured their FMA scores to assess the advantages of VRh and then adjusted the parameters of a robot device. Others can be found in the study of Graham et al. [92], which reviews nine studies that talk about the use of telerehabilitation in wheelchair assessment.
Table 5 are referring the mentioned studies about the use of VRy for rehabilitation.
Table 5.
Virtual rehabilitation implementation studies.
9.3. Remote and Assistive Technologies Based on BCI
In the prior sections, we established some studies of BCI and some studies that used virtual reality technology for the implementation of a rehabilitation process. The union of the two technologies allows the implementation of rehabilitation in a more natural way. The immersive characteristic of virtual reality BCI allows a patient to interact with an environment, augmenting the benefit of using BCI [93], and the control characteristics of a BCI prepare a patient to interact with an environment.
BCI-based robotic therapy has specific objectives according to [79] for the identification of the implementation of BCI technologies in robotic control of rehabilitation devices, a revisit of the BCI technology in terms of resolutions, and degrees of freedom (DOF) of the robotic devices and the clinical evaluation when using this systems of this type.
9.4. BCI Devices for Rehabilitation
BCI applications in the medical field have the purpose of manipulating an external device or monitoring a mental state, such as the devices designed to identify depression or other mental health issues. The BCI that allows manipulating external devices is composed of prostheses, orthoses, and exoskeletons [38]. These devices are focused in proportionate certain rehabilitation services and are limited by their configurations and purposes. These devices are described as follows:
- Functional electrical stimulation (FES). This type of orthesis uses functional electrical stimulation of the patient’s muscles to generate forces that can approximate the movement. The FES systems are categorized among the sources of control signals to trigger the regulation pattern, such as shoulder control, voice control, respiratory control, joystick control, position transducers, and a physical trigger. Electrical stimulation patterns complement these control strategies: A 1 to 3-channel surface electrode system, a multichannel surface stimulation system, a multichannel percutaneous system with intramuscular electrodes, and finally, the fully implanted systems with epimysial electrodes (electrodes that are sewn onto the surface of a muscle).
- Orthotics and exoskeletons. An orthosis is a mechanical structure that maps the anatomy of the human limb. Its purpose is to restore lost or weak function [42]; this is done by augmenting the function of the skeletomotor system or by controlling motion or altering the shape of a body tissue [10].Ortheses are classified by acronyms describing the joints they cross; for example, an AFO is an ankle–foot orthesis. The joints are the cervix (neck), upper limb, trunk, lower limb, and foot. Additionally, the classification is given by external interference; this category is divided into structural and functional. There are three major considerations in the design of an orthesis: the function, the structure, and the cosmesis (the aesthetics or appearance).Orthotic care involves external appliances designed to support, straighten, or improve the functioning of a body part; prosthetic interventions involve an artificial external replacement for a body part.
- Prosthetic and robotic devices. A prosthesis is an electromechanical device that substitutes for lost limbs after amputation. The robotic counterparts of prostheses take the form of electromechanical wearable robotics limbs and make it possible to replace the lost limb’s function in a way closer to the natural human function. This is achieved by the intelligent use of robotic technologies in terms of human–robot interaction and actuation [42]. Figure 11 [94] portrays some of the commercial devices that are triggered by electromyography biosignals.
 Figure 11. Sample of myoelectric commercial devices.
Figure 11. Sample of myoelectric commercial devices.
Rehabilitation requires an effective system [10] for restoring motor conditions. The features that could reflect the system’s reliability are different depending on the energy and cost of the system, the ability of a bodied subject to perform a task, the need to avoid disruption of normal activities, cosmetics, and practicality. The challenges to the implementation of BCI rehabilitation are various, such as the data acquisition method, the signal processing and classification, the realization of a robot device, the need to proportionate an adequate feedback environment, and the integration of all the elements [79].
The existence of different devices explains the variety of implementations in the studies of BCI for rehabilitation. For example, reference [11] shows the studies related to BCIs for motor impairment, and some BCI modalities, such as slow cortical potentials, sensorimotor rhythms, and P300, used as the operational mechanisms for post-stroke and spinal cord injury rehabilitation. On the other hand, the review of Bockbrader [95] remarks on some ethical implications of the use of BCI technologies, as a part of some studies of BCI implementation from the medical perspective. The focus of the review of Velayati [96] was a methodical one, so the number of studies reviewed (eight) was small, but the study portrays the effectiveness of telerehabilitation in the elderly population. Recently, in 2021, ref. [6] 39 studies were reviewed about BCI for rehabilitation. This study used statistical information about the paradigms that triggered the BCI mechanism and the diseases that the rehabilitation focused on. The most recent review about BCI rehabilitation was done by Müller-Putz [97], and is an interesting one because it is the recompilation of 6 years of investigation to develop a project the name “Feel Your Reach”. This project focuses on rehabilitating people with cervical SCI through the control of an assistive robotic arm for daily tasks using a non-invasive signal recording device.
This review recapitulates many studies, such as the one of Wang et al., who in 2018 [59] did research that used both EEG and EMG signals to reflect motion and fatigue patterns and bring feedback to the virtual system. They adapted a training scene based on the fatigue status. They used a Visual Studio developer to create the rehabilitation scene that consisted of “flying a plane”, “pushing a box”, and “Tetris”. The data passed through an SVM classifier to control the virtual environment. The effectiveness of the action for healthy people was reported to be 99.5%, and it was 94.75% for patients. A few later, Vourvopoulos et al. [98] applied a rehabilitation measure after a stroke by integrating an EEG BCI with VRy. A 60-year-old patient was teated for three weeks in a clinical setting. They measured the upper extremity scores using the full Meyer scale (FMA UE) and the brain plasticity. The team used a NeuroRow BCI-VRy System. The data acquisition used an Enobio 8, an 8-channel sensor. The virtual environment designed was a bat rowing atmosphere. The results reflected an FMA scale of 31 pre-rehabilitation, 40 post-rehabilitation, and 44 after one month (the follow-up score). Then, they used an LDA classifier to measure the performance through 10 sessions. The patient had 60% accuracy in the task versus the healthy group and used VRy with 76% accuracy; the non-VRy group reported 68% accuracy.
Li and Yang [74] proposed a virtual rehabilitation training system based on EMG and EEG. This system collects signals synchronously and obtains ERD/ERS (event-related desynchronization and synchronization). These coefficients use an SVM-PSO method to select the best combination of EEG-EMG to avoid fatigue using MSC Adams software that has the purpose of virtual prototyping. This makes the proposed exercise recognize a motion pattern.
In the present year, Pruss [99] created a virtual ambiance controlled by an assistance robot designed to help with household tasks. The paradigm P300 triggers this virtual device, which is controlled by an EEG signal recorded by a Unicorn Hybrid system.
In Table 6 are portrayed the different studies cited about BCI for rehabilitation.
Table 6.
Brain–computer interfaces with virtual rehabilitation.
9.5. Virtual Rehabilitation and BCI for the Optimal Use of Assistive Devices
Rehabilitation is not only used when a person has a certain level of damage, but also, some rehabilitation can be taken as a measure focused on preventing the need for more drastic health measures. For example, one review [100] compares 38 studies for devices working for upper and lower limb rehabilitation focused on the exoskeletons and virtual ambiances for rehabilitation. Additionally, the work of Ribero [101] talks about the upper limb prostheses and the technologies involved, such as the myoelectric devices (the ones triggered by EMG signals). Additionally, the final example given by [102] proposes a new framework to implement a more automated rehabilitation process for the upper limb using the information of robotic rehabilitation and to focus on the rehabilitation cycle. Table 4 refers to other studies that use BCI for devices.
These systems need the inclusion of different strategies to achieve these goals, and the researchers implement diverse devices (Table 7); for example, in 2018, a group of researchers [103] used a multifunctional robotic device (Universal Haptic Pantograph) to bring about rehabilitation. This robot was used to rehabilitate the shoulders, elbows, arms, and wrists of people with motor impairments due to stroke or ictus. This was combined with a software called Telereha that is equipped with a Compact Rio through a UDP protocol. The protocol allows the communication and the adjustment of the different rehabilitation tasks through a game to configure the rehabilitation. Additionally, in the same year, Cartagena [104] and company focused on developing an orthosis device that helps the flexion and traction of hand fingers. It is a mechatronic device with a fuzzy logic controller, a connection with Unity 3D for the virtual environment, and the use of a Raspberry Pi. It is a complete and relatively portable system for proportionate rehabilitation. The work of [105] focuses on the design and implementation of an exoskeleton for palmar extension for patients in post-stroke rehabilitation with the intention of regaining motor activities needed in daily activities.
Table 7.
BCI for virtual rehabilitation with assistive devices.
10. Discussion
The present work discusses the information from various papers related to implementing BCI for virtual rehabilitation with assistive devices. It portrays the different steps to implement a BCI, such as the biosignals that could be extracted (such as EEG or EMG) and the processes of feature extraction, feature selection, classification algorithms; and the types of BCIs and their applications.
This literature review allowed us to identify a research interest that is unexplored that could help to design a new BCI that could improve the performances of state-of-the-art works. That is, the existing works talk about rehabilitation and the tendency to implement telerehabilitation using BCI for upper and lower limb rehabilitation, but they do not mention the inconvenience of a VRy system. Additionally, there exist a great number of works of BCI implementations, but there are a few that reunite the concepts of rehabilitation and VRy.
Including these terms makes it difficult to design devices that could work together with interfaces to take rehabilitation measures properly. The telerehabilitation concept is not found in many works, and in recent times, it was necessary to do a lot of remote practices due to the COVID-19 pandemic, and many recommendations exist for creating this type of system. The exclusion criteria for works in the first instance seem to be not so specific, but the mentioned works are few compared to what is expected in consideration with all the existing works on BCIs. This is an important gap in applying the VRy and BCI technologies that can be used to implement the technologies that could lead to more friendly and cost-effective telerehabilitation.
11. Conclusions
The present work presented recent developments regarding EEG-based BCI and assistive technologies for RR based on VRy. Our findings reveal that real-time MI classification focused on BCI activation is a key component when developing systems for RR using VRy environments for impaired patients. These systems involve many design processes, techniques, and methods, where diverse areas such as signal processing and computer science are involved. It is important to remark that most of the revised published results have employed the databases Motor/Imagery Physionet, Dataset II (P300 speller paradigm), Dataset IIIa (Motor imagery, multi-class), Dataset IIIb (Motor imagery with the non-stationary problem), Dataset IVa (Motor imagery, small training sets), and Dataset IVb (Motor imagery, uncued classifier application) for developing and testing their proposed systems. These can be useful for new EEG-based BCIs to benchmark new algorithms. In addition, most manuscripts have tried a similar approach to treat the collected information, consisting mainly of feature extraction, feature selection, and a classification stage. Different algorithms have been tried for each stage, impacting the accuracy reported by the classification algorithm. Even though there are vast algorithm combinations—see Table 2 and Table 3—it is possible to infer that DWT is the feature-extraction technique that has obtained the best quality measures when working with EEG signals. These features have been tested based on different classification algorithms implemented for developing and implementing BCI. These studies considered CNN as the main tool to get higher accuracy in the classification outcomes.
After the classification stage, the proposed algorithms must be integrated into a VRy environment. Originally, the full VRy environment was used for rehabilitation when patients had limited movement of a body part due to an accident or medical procedure. However, in recent times, these environments have shown to be useful when training patients in the employment of prosthetic, orthotic, or other assistive technologies, allowing physicians to determine if the patient will be able to use these tools. They have the advantage of having the patient feel confident, which may allow him to learn faster. The advantages of the use of this kind of rehabilitation are mainly twofold; the first is related to the patient’s limited mobility, and the second is the application showing the patient his progress, which has been proven to motivate the patient not to leave the therapy.
Author Contributions
Conceptualization, A.G.L.-H., M.A.-P. and R.Q.F.-A.; methodology, A.G.L.-H., M.A.-P. and I.C.; formal analysis, A.G.L.-H., M.A.-P. and I.C.; investigation, A.G.L.-H., M.A.-P. and I.C.; data curation, L.M.A.-V. and M.G.-M.; writing—original draft preparation, A.G.L.-H.; writing—review and editing, A.G.L.-H., M.A.-P. and I.C.; visualization, A.G.L.-H., M.A.-P. and R.Q.F.-A.; supervision, M.A.-P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The support from CONACyT for the postgraduate studies of the first author is acknowledged (scholarship no. 827435). In addition, the authors would like to acknowledge the support of Tecnologico de Monterrey in the production and publication of this work.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ML | Machine Learning |
| EEG | Electroencephalography |
| EMG | Electromyography |
| STFT | Short Time Fourier Transform |
| PSD | Power Spectral Density |
| PCA | Principal Component Analysis |
| ICA | Independent Component Analysis |
| CSP | Common Spatial Patterns |
| DWT | Discrete Wavelet Transform |
| SVM | Support Vector Machines |
| KNN | Kean Nearest Neighbor |
| LSTM | Long Short Term Memory |
| RNN | Recurrent neural network |
| VRy | Virtual Reality |
| VRh | Virtual Rehabilitation |
| RR | Remote Rehabilitation |
| FMA | Full Meyer Assessment Scale |
References
- World Health Organization. Strengthening the Collection of Data on Disability; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Tsai Owens, M.S.; Biggs, B.K.; Fahrenkamp, A.C.; Geske, J.; Hofschulte, D.R.; Harbeck-Weber, C.; Fischer, P.R. Physical Symptoms, Distress, and Functional Disability in Youth With Chronic Orthostatic Intolerance. J. Pediatr. Psychol. 2022, 47, 1185–1194. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World report on disability (ISBN 978 92 4 068521 5). Retrieved Sept. 2011, 30, 2015. [Google Scholar]
- Halton, J. Virtual rehabilitation with video games: A new frontier for occupational therapy. Occup. Ther. Now 2008, 9, 12–14. [Google Scholar]
- Burdea, G.C. Virtual rehabilitation–benefits and challenges. Methods Inf. Med. 2003, 42, 519–523. [Google Scholar]
- Wen, D.; Fan, Y.; Hsu, S.H.; Xu, J.; Zhou, Y.; Tao, J.; Lan, X.; Li, F. Combining brain–computer interface and virtual reality for rehabilitation in neurological diseases: A narrative review. Ann. Phys. Rehabil. Med. 2021, 64, 101404. [Google Scholar] [CrossRef] [PubMed]
- Haddaway, N.R.; Page, M.J.; Pritchard, C.C.; McGuinness, L.A. PRISMA2020: An R package and Shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimised digital transparency and Open Synthesis. Campbell Syst. Rev. 2022, 18, e1230. [Google Scholar] [CrossRef]
- Web of Science. 2022. Available online: https://www.webofscience.com/wos/woscc/basic-search (accessed on 10 October 2022).
- Roughton, T. Interactive Generation of Path-Traced Lightmaps. Ph.D. Thesis, Victoria University of Wellington, Wellington, New Zealand, 2019. [Google Scholar]
- Bronzino, J.D. Biomedical Engineering Handbook 2; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2000; Volume 2. [Google Scholar]
- Lazarou, I.; Nikolopoulos, S.; Petrantonakis, P.C.; Kompatsiaris, I.; Tsolaki, M. EEG-based brain–computer interfaces for communication and rehabilitation of people with motor impairment: A novel approach of the 21st century. Front. Hum. Neurosci. 2018, 12, 14. [Google Scholar] [CrossRef]
- Ritter, A.B.; Hazelwood, V.; Valdevit, A.; Ascione, A.N. Biomedical Engineering Principles; CRC Press: Boca Raton, FL, USA, 2011. [Google Scholar]
- Cohen, M.X. Analyzing Neural Time Series Data: Theory and Practice; MIT Press: Cambridge, MA, USA, 2014. [Google Scholar]
- Padfield, N.; Zabalza, J.; Zhao, H.; Masero, V.; Ren, J. EEG-based brain–computer interfaces using motor-imagery: Techniques and challenges. Sensors 2019, 19, 1423. [Google Scholar] [CrossRef]
- WHO. Rehabilitation. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/rehabilitation (accessed on 12 October 2022).
- Rechy-Ramirez, E.J.; Hu, H. Bio-signal based control in assistive robots: A survey. Digit. Commun. Netw. 2015, 1, 85–101. [Google Scholar] [CrossRef]
- Bidgoly, A.J.; Bidgoly, H.J.; Arezoumand, Z. A survey on methods and challenges in EEG based authentication. Comput. Secur. 2020, 93, 101788. [Google Scholar] [CrossRef]
- Bandara, D.; Arata, J.; Kiguchi, K. A noninvasive brain–computer interface approach for predicting motion intention of activities of daily living tasks for an upper-limb wearable robot. Int. J. Adv. Robot. Syst. 2018, 15, 1729881418767310. [Google Scholar] [CrossRef]
- Goldberger, A.L.; Amaral, L.A.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.K.; Stanley, H.E. PhysioBank, PhysioToolkit, and PhysioNet: Components of a new research resource for complex physiologic signals. Circulation 2000, 101, e215–e220. [Google Scholar] [CrossRef]
- Abdelfattah, S.M.; Abdelrahman, G.M.; Wang, M. Augmenting the size of EEG datasets using generative adversarial networks. In Proceedings of the 2018 International Joint Conference on Neural Networks (IJCNN), Rio de Janeiro, Brazil, 8–13 July 2018; pp. 1–6. [Google Scholar]
- Blankertz, B.; Muller, K.R.; Krusienski, D.J.; Schalk, G.; Wolpaw, J.R.; Schlogl, A.; Pfurtscheller, G.; Millan, J.R.; Schroder, M.; Birbaumer, N. The BCI competition III: Validating alternative approaches to actual BCI problems. IEEE Trans. Neural Syst. Rehabil. Eng. 2006, 14, 153–159. [Google Scholar] [CrossRef]
- Ghaemi, A.; Rashedi, E.; Pourrahimi, A.M.; Kamandar, M.; Rahdari, F. Automatic channel selection in EEG signals for classification of left or right hand movement in Brain Computer Interfaces using improved binary gravitation search algorithm. Biomed. Signal Process. Control 2017, 33, 109–118. [Google Scholar] [CrossRef]
- Zhang, D.; Yao, L.; Zhang, X.; Wang, S.; Chen, W.; Boots, R.; Benatallah, B. Cascade and parallel convolutional recurrent neural networks on EEG-based intention recognition for brain computer interface. In Proceedings of the Thirty-Second AAAI Conference on Artificial Intelligence, New Orleans, LA, USA, 2–7 February 2018. [Google Scholar]
- Khademi, Z.; Ebrahimi, F.; Kordy, H.M. A transfer learning-based CNN and LSTM hybrid deep learning model to classify motor imagery EEG signals. Comput. Biol. Med. 2022, 143, 105288. [Google Scholar] [CrossRef] [PubMed]
- Lal, T.; Hinterberger, T.; Widman, G.; Schröder, M.; Hill, N.; Rosenstiel, W.; Elger, C.; Birbaumer, N.; Schölkopf, B. Methods towards invasive human brain computer interfaces. In Advances in Neural Information Processing Systems; MIT Press: Cambridge, MA, USA, 2004; Volume 17. [Google Scholar]
- Paul, S.; Zabir, I.; Sarker, T.; Fattah, S.A.; Shahnaz, C. Higher order statistics of bispectrum and MRP of ECoG signals for motor imagery tasks classification. In Proceedings of the 2017 IEEE Region 10 Symposium (TENSYMP), Cochin, India, 14–16 July 2017; pp. 1–4. [Google Scholar]
- Krusienski, D.; Schalk, G. Wadsworth BCI Dataset (P300 Evoked Potentials). BCI Compet. III Chall. 2004. Available online: https://www.bbci.de/competition/iii/ (accessed on 10 October 2022).
- Rakotomamonjy, A.; Guigue, V. BCI competition III: Dataset II-ensemble of SVMs for BCI P300 speller. IEEE Trans. Biomed. Eng. 2008, 55, 1147–1154. [Google Scholar] [CrossRef]
- Schlogl, A.; Filz, O.; Ramoser, H.; Pfurtscheller, G. GDF-A General Dataformat for Biosignals Version 1.25; University of Technology Graz: Graz, Austria, 2005. [Google Scholar]
- Jin, J.; Miao, Y.; Daly, I.; Zuo, C.; Hu, D.; Cichocki, A. Correlation-based channel selection and regularized feature optimization for MI-based BCI. Neural Netw. 2019, 118, 262–270. [Google Scholar] [CrossRef] [PubMed]
- Schlogl, A. Dataset IIIb: Non-stationary 2-class BCI data. BCI Compet. III. 2005. Available online: https://www.semanticscholar.org/paper/Dataset-IIIb%3A-Non-stationary-2-class-BCI-data/1fcef9d78134e09cd0fd1dc1f8df430fd000af8b (accessed on 10 October 2022).
- You, Y.; Chen, W.; Zhang, T. Motor imagery EEG classification based on flexible analytic wavelet transform. Biomed. Signal Process. Control 2020, 62, 102069. [Google Scholar] [CrossRef]
- Dornhege, G.; Blankertz, B.; Curio, G.; Muller, K.R. Boosting bit rates in noninvasive EEG single-trial classifications by feature combination and multiclass paradigms. IEEE Trans. Biomed. Eng. 2004, 51, 993–1002. [Google Scholar] [CrossRef] [PubMed]
- Millan, J.R. On the need for on-line learning in brain-computer interfaces. In Proceedings of the 2004 IEEE International Joint Conference on Neural Networks, Budapest, Hungary, 25–29 July 2004; pp. 2877–2882. [Google Scholar]
- Cho, H.; Ahn, M.; Ahn, S.; Kwon, M.; Jun, S.C. EEG datasets for motor imagery brain–computer interface. GigaScience 2017, 6, gix034. [Google Scholar] [CrossRef]
- Luciw, M.D.; Jarocka, E.; Edin, B.B. Multi-channel EEG recordings during 3936 grasp and lift trials with varying weight and friction. Sci. Data 2014, 1, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Altuwaijri, G.A.; Muhammad, G. A Multibranch of Convolutional Neural Network Models for Electroencephalogram-Based Motor Imagery Classification. Biosensors 2022, 12, 22. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.M.; Khan, A.A.; Farooq, O. Selection of Features and Classifiers for EMG-EEG-Based Upper Limb Assistive Devices—A Review. IEEE Rev. Biomed. Eng. 2019, 13, 248–260. [Google Scholar] [CrossRef]
- Clerc, M.; Bougrain, L.; Lotte, F. Brain-Computer Interfaces 1: Methods and Perspectives; John Wiley & Sons: Hoboken, NJ, USA, 2016. [Google Scholar]
- Carr, J.J.; Brown, J.M. Introduction to Biomedical Equipment Technology; Prentice Hall: Hoboken, NJ, USA, 2001. [Google Scholar]
- Hu, L.; Zhang, Z. EEG Signal Processing and Feature Extraction; Springer: Berlin/Heidelberg, Germany, 2019. [Google Scholar]
- Pons, J.L. Wearable Robots: Biomechatronic Exoskeletons; John Wiley & Sons: Hoboken, NJ, USA, 2008. [Google Scholar]
- Comon, P.; Jutten, C. Handbook of Blind Source Separation: Independent Component Analysis and Applications; Academic Press: Cambridge, MA, USA, 2010. [Google Scholar]
- Ewins, D.J.; Rao, S.S.; Braun, S.G. Encyclopedia of Vibration, Three-Volume Set; Academic Press: Cambridge, MA, USA, 2002. [Google Scholar]
- Misra, H.; Ikbal, S.; Bourlard, H.; Hermansky, H. Spectral entropy based feature for robust ASR. In Proceedings of the 2004 IEEE International Conference on Acoustics, Speech, and Signal Processing, Montreal, QC, Canada, 17–21 May 2004; Volume 1, pp. 1–193. [Google Scholar]
- Yi, W.; Qiu, S.; Qi, H.; Zhang, L.; Wan, B.; Ming, D. EEG feature comparison and classification of simple and compound limb motor imagery. J. Neuroeng. Rehabil. 2013, 10, 106. [Google Scholar] [CrossRef]
- Al-Saegh, A.; Dawwd, S.A.; Abdul-Jabbar, J.M. Deep learning for motor imagery EEG-based classification: A review. Biomed. Signal Process. Control 2021, 63, 102172. [Google Scholar] [CrossRef]
- Jović, A.; Brkić, K.; Bogunović, N. A review of feature selection methods with applications. In Proceedings of the 2015 38th International Convention on Information and Communication Technology, Electronics and Microelectronics (MIPRO), Opatija, Croatia, 25–29 May 2015; pp. 1200–1205. [Google Scholar] [CrossRef]
- Tayeb, Z.; Fedjaev, J.; Ghaboosi, N.; Richter, C.; Everding, L.; Qu, X.; Wu, Y.; Cheng, G.; Conradt, J. Validating deep neural networks for online decoding of motor imagery movements from EEG signals. Sensors 2019, 19, 210. [Google Scholar] [CrossRef]
- Ding, C.; Peng, H. Minimum redundancy feature selection from microarray gene expression data. J. Bioinform. Comput. Biol. 2005, 3, 185–205. [Google Scholar] [CrossRef] [PubMed]
- Boser, B.E.; Guyon, I.M.; Vapnik, V.N. A training algorithm for optimal margin classifiers. In Proceedings of the Fifth Annual Workshop on Computational Learning Theory, Pittsburgh, PA, USA, 27–29 July 1992; pp. 144–152. [Google Scholar]
- Cruz, P.P. Inteligencia Artificial Con Aplicaciones a la Ingeniería; Alfaomega: Kota Batam, Indonesia, 2011. [Google Scholar]
- Fisher, R.A. The use of multiple measurements in taxonomic problems. Ann. Eugen. 1936, 7, 179–188. [Google Scholar] [CrossRef]
- Craik, A.; He, Y.; Contreras-Vidal, J.L. Deep learning for electroencephalogram (EEG) classification tasks: A review. J. Neural Eng. 2019, 16, 031001. [Google Scholar] [CrossRef] [PubMed]
- Alomari, M.H.; Samaha, A.; AlKamha, K. Automated classification of L/R hand movement EEG signals using advanced feature extraction and machine learning. arXiv 2013, arXiv:1312.2877. [Google Scholar]
- Karimi, F.; Kofman, J.; Mrachacz-Kersting, N.; Farina, D.; Jiang, N. Detection of movement related cortical potentials from EEG using constrained ICA for brain–computer interface applications. Front. Neurosci. 2017, 11, 356. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Zhang, M.; Luo, X.; Yang, J. Combined long short-term memory based network employing wavelet coefficients for MI-EEG recognition. In Proceedings of the 2016 IEEE International Conference on Mechatronics and Automation, Harbin, China, 7–10 August 2016; pp. 1971–1976. [Google Scholar]
- Amin, H.U.; Mumtaz, W.; Subhani, A.R.; Saad, M.N.M.; Malik, A.S. Classification of EEG signals based on pattern recognition approach. Front. Comput. Neurosci. 2017, 11, 103. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Jiang, A.; Liu, X.; Shang, J.; Zhang, L. LSTM-based EEG classification in motor imagery tasks. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 2086–2095. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Davoodnia, V.; Sepas-Moghaddam, A.; Zhang, Y.; Etemad, A. Classification of Hand Movements from EEG using a Deep Attention-based LSTM Network. IEEE Sens. J. 2019, 20, 3113–3122. [Google Scholar] [CrossRef]
- Nagabushanam, P.; Thomas George, S.; Radha, S. EEG signal classification using LSTM and improved neural network algorithms. Soft Comput. 2020, 24, 9981–10003. [Google Scholar] [CrossRef]
- Ghumman, M.K.; Singh, S.; Singh, N.; Jindal, B. Optimization of parameters for improving the performance of EEG-based BCI system. J. Reliab. Intell. Environ. 2021, 7, 145–156. [Google Scholar] [CrossRef]
- Goodfellow, I.; Bengio, Y.; Courville, A. Deep Learning; MIT Press: Cambridge, MA, USA, 2016; Available online: http://www.deeplearningbook.org (accessed on 5 October 2022).
- Hochreiter, S.; Schmidhuber, J. Long short-term memory. Neural Comput. 1997, 9, 1735–1780. [Google Scholar] [CrossRef]
- LeCun, Y.; Bottou, L.; Bengio, Y.; Haffner, P. Gradient-based learning applied to document recognition. Proc. IEEE 1998, 86, 2278–2324. [Google Scholar] [CrossRef]
- Bousseta, R.; El Ouakouak, I.; Gharbi, M.; Regragui, F. EEG based brain computer interface for controlling a robot arm movement through thought. Irbm 2018, 39, 129–135. [Google Scholar] [CrossRef]
- Shi, T.; Ren, L.; Cui, W. Feature recognition of motor imaging EEG signals based on deep learning. Pers. Ubiquitous Comput. 2019, 23, 499–510. [Google Scholar] [CrossRef]
- Netzer, E.; Frid, A.; Feldman, D. Real-time EEG classification via coresets for BCI applications. Eng. Appl. Artif. Intell. 2020, 89, 103455. [Google Scholar] [CrossRef]
- Liu, M.; Zhou, M.; Zhang, T.; Xiong, N. Semi-supervised learning quantization algorithm with deep features for motor imagery EEG Recognition in smart healthcare application. Appl. Soft Comput. 2020, 89, 106071. [Google Scholar] [CrossRef]
- Huang, W.; Chang, W.; Yan, G.; Yang, Z.; Luo, H.; Pei, H. EEG-based motor imagery classification using convolutional neural networks with local reparameterization trick. Expert Syst. Appl. 2022, 187, 115968. [Google Scholar] [CrossRef]
- Vassilyev, S.; Kelina, A.Y.; Kudinov, Y.I.; Pashchenko, F. Intelligent control systems. Procedia Comput. Sci. 2017, 103, 623–628. [Google Scholar] [CrossRef]
- Ruhunage, I.; Perera, C.J.; Nisal, K.; Subodha, J.; Lalitharatne, T.D. EMG signal controlled transhumerai prosthetic with EEG-SSVEP based approch for hand open/close. In Proceedings of the 2017 IEEE International Conference on Systems, Man, and Cybernetics (SMC), Banff, AB, Canada, 5–8 October 2017; pp. 3169–3174. [Google Scholar]
- Aly, H.I.; Youssef, S.; Fathy, C. Hybrid brain computer interface for movement control of upper limb prostheses. In Proceedings of the 2018 International Conference on Biomedical Engineering and Applications (ICBEA), Funchal, Portugal, 9–12 July 2018; pp. 1–6. [Google Scholar]
- Li, S.; Yang, J. Study on Brain Electromyography Rehabilitation System Based on Data Fusion and Virtual Rehabilitation Simulation. J. Med. Syst. 2019, 43, 22. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.S.; She, B.H. A BCI system with motor imagery based on bidirectional long-short term memory. IOP Conf. Ser. Mater. Sci. Eng. 2020, 719, 012026. [Google Scholar] [CrossRef]
- Lotte, F.; Bougrain, L.; Cichocki, A.; Clerc, M.; Congedo, M.; Rakotomamonjy, A.; Yger, F. A review of classification algorithms for EEG-based brain–computer interfaces: A 10 year update. J. Neural Eng. 2018, 15, 031005. [Google Scholar] [CrossRef]
- Abiri, R.; Borhani, S.; Sellers, E.W.; Jiang, Y.; Zhao, X. A comprehensive review of EEG-based brain–computer interface paradigms. J. Neural Eng. 2019, 16, 011001. [Google Scholar] [CrossRef]
- Ramadan, R.A.; Vasilakos, A.V. Brain computer interface: Control signals review. Neurocomputing 2017, 223, 26–44. [Google Scholar] [CrossRef]
- Baniqued, P.D.E.; Stanyer, E.C.; Awais, M.; Alazmani, A.; Jackson, A.E.; Mon-Williams, M.A.; Mushtaq, F.; Holt, R.J. Brain–computer interface robotics for hand rehabilitation after stroke: A systematic review. J. Neuroeng. Rehabil. 2021, 18, 1–25. [Google Scholar] [CrossRef]
- Sawangjai, P.; Hompoonsup, S.; Leelaarporn, P.; Kongwudhikunakorn, S.; Wilaiprasitporn, T. Consumer grade EEG measuring sensors as research tools: A review. IEEE Sens. J. 2019, 20, 3996–4024. [Google Scholar] [CrossRef]
- Fugl-Meyer, A.R.; Jääskö, L.; Leyman, I.; Olsson, S.; Steglind, S. A method for evaluation of physical performance. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar] [PubMed]
- Kamenov, K.; Mills, J.A.; Chatterji, S.; Cieza, A. Needs and unmet needs for rehabilitation services: A scoping review. Disabil. Rehabil. 2019, 41, 1227–1237. [Google Scholar] [CrossRef] [PubMed]
- Nussbaum, R.; Kelly, C.; Quinby, E.; Mac, A.; Parmanto, B.; Dicianno, B.E. Systematic review of mobile health applications in rehabilitation. Arch. Phys. Med. Rehabil. 2019, 100, 115–127. [Google Scholar] [CrossRef]
- Geohagen, O.; Hamer, L.; Lowton, A.; Guerra, S.; Milton-Cole, R.; Ellery, P.; Martin, F.C.; Lamb, S.E.; Sackley, C.; Sheehan, K.J. The effectiveness of rehabilitation interventions including outdoor mobility on older adults’ physical activity, endurance, outdoor mobility and falls-related self-efficacy: Systematic review and meta-analysis. Age Ageing 2022, 51, afac120. [Google Scholar] [CrossRef]
- Martins, T.; Carvalho, V.; Soares, F. Physioland-A serious game for rehabilitation of patients with neurological diseases. In Online Engineering & Internet of Things; Springer: Berlin/Heidelberg, Germany, 2018; pp. 628–642. [Google Scholar]
- Gómez-Portes, C.; Vallejo, D.; Molina, A.I.; Lacave, C. Automatic Generation of Customised Exergames for Home Rehabilitation Based on Physical Mobility Constraints and Key Performance Indicators. In Intelligent Environments 2020; IOS Press: Clifton, NJ, USA, 2020; pp. 29–38. [Google Scholar]
- Lin, B.S.; Hsu, H.C.; Jan, G.E.; Chen, J.L. An interactive upper-limb post-stroke rehabilitation system integrating BCI-based attention monitoring and virtual reality feedback. In Proceedings of the 2016 Third International Conference on Computing Measurement Control and Sensor Network (CMCSN), Matsue, Japan, 20–22 May 2016; pp. 44–47. [Google Scholar]
- Wang, W.; Yang, B.; Guan, C.; Li, B. A VR combined with MI-BCI application for upper limb rehabilitation of stroke. In Proceedings of the 2019 IEEE MTT-S International Microwave Biomedical Conference (IMBioC), Nanjing, China, 6–8 May 2019; Volume 1, pp. 1–4. [Google Scholar]
- Gmez-Portes, C.; Carneros-Prado, D.; Albusac, J.; Castro-Schez, J.J.; Glez-Morcillo, C.; Vallejo, D. PhyRe Up! A System Based on Mixed Reality and Gamification to Provide Home Rehabilitation for Stroke Patients. IEEE Access 2021, 9, 139122–139137. [Google Scholar] [CrossRef]
- Chantera, M.; Morillo, P.; Vallejo-Huanga, D. Virtual rehabilitation platform for left-handed people working in industrial environments. In Advances in Intelligent Systems and Computing, Proceedings of the International Conference on Applied Human Factors and Ergonomics, Virtual, 16–20 July 2020; Springer: Cham, Switzerland, 2020; pp. 900–906. [Google Scholar]
- Tradigo, G.; Vizza, P.; Guzzi, P.H.; Fragomeni, G.; Ammendolia, A.; Veltri, P. A programmable device to guide rehabilitation patients: Design, testing and data collection. In Proceedings of the 2020 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Seoul, Republic of Korea, 16–19 December 2020; pp. 1487–1491. [Google Scholar]
- Graham, F.; Boland, P.; Grainger, R.; Wallace, S. Telehealth delivery of remote assessment of wheelchair and seating needs for adults and children: A scoping review. Disabil. Rehabil. 2020, 42, 3538–3548. [Google Scholar] [CrossRef]
- Leeb, R.; Pérez-Marcos, D. Brain-computer interfaces and virtual reality for neurorehabilitation. Handb. Clin. Neurol. 2020, 168, 183–197. [Google Scholar]
- Pasquina, P.F.; Perry, B.N.; Miller, M.E.; Ling, G.S.; Tsao, J.W. Recent advances in bioelectric prostheses. Neurol. Clin. Pract. 2015, 5, 164–170. [Google Scholar] [CrossRef]
- Bockbrader, M.A.; Francisco, G.; Lee, R.; Olson, J.; Solinsky, R.; Boninger, M.L. Brain computer interfaces in rehabilitation medicine. PM&R 2018, 10, S233–S243. [Google Scholar]
- Velayati, F.; Ayatollahi, H.; Hemmat, M. A systematic review of the effectiveness of telerehabilitation interventions for therapeutic purposes in the elderly. Methods Inf. Med. 2020, 59, 104–109. [Google Scholar] [CrossRef]
- Müller-Putz, G.R.; Kobler, R.J.; Pereira, J.; Lopes-Dias, C.; Hehenberger, L.; Mondini, V.; Martínez-Cagigal, V.; Srisrisawang, N.; Pulferer, H.; Batistić, L.; et al. Feel your reach: An EEG-based framework to continuously detect goal-directed movements and error processing to gate kinesthetic feedback informed artificial arm control. Front. Hum. Neurosci. 2022, 16, 110. [Google Scholar] [CrossRef] [PubMed]
- Vourvopoulos, A.; Jorge, C.; Abreu, R.; Figueiredo, P.; Fernandes, J.C.; Bermudez i Badia, S. Efficacy and brain imaging correlates of an immersive motor imagery BCI-driven VR system for upper limb motor rehabilitation: A clinical case report. Front. Hum. Neurosci. 2019, 13, 244. [Google Scholar] [CrossRef] [PubMed]
- Pruss, E.; Prinsen, J.; Vrins, A.; Ceccato, C.; Alimardani, M. A BCI-controlled Robot Assistant for Navigation and Object Manipulation in a VR Smart Home Environment. In Proceedings of the 15th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2022), Online, 9–11 February 2022; pp. 231–237. [Google Scholar]
- Al-Quraishi, M.S.; Elamvazuthi, I.; Daud, S.A.; Parasuraman, S.; Borboni, A. EEG-based control for upper and lower limb exoskeletons and prostheses: A systematic review. Sensors 2018, 18, 3342. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, J.; Mota, F.; Cavalcante, T.; Nogueira, I.; Gondim, V.; Albuquerque, V.; Alexandria, A. Analysis of man-machine interfaces in upper-limb prosthesis: A review. Robotics 2019, 8, 16. [Google Scholar] [CrossRef]
- Oña, E.; Cano-de La Cuerda, R.; Sánchez-Herrera, P.; Balaguer, C.; Jardón, A. A review of robotics in neurorehabilitation: Towards an automated process for upper limb. J. Healthc. Eng. 2018, 2018, 9758939. [Google Scholar] [CrossRef]
- Mancisidor, A.; Zubizarreta, A.; Cabanes, I.; Bengoa, P.; Jung, J.H. Dispositivo robótico multifuncional para la rehabilitación de las extremidades superiores. Rev. Iberoam. Autom. E Inform. Ind. 2018, 15, 180–191. [Google Scholar] [CrossRef]
- Cartagena, P.D.; Naranjo, J.E.; Garcia, C.A.; Beltran, C.; Castro, M.; Garcia, M.V. Virtual reality-based system for hand rehabilitation using an exoskeletal orthosis. In Lecture Notes in Computer Science, Proceedings of the International Conference on Augmented Reality, Virtual Reality and Computer Graphics, Otranto, Italy, 24–27 June 2018; Springer: Cham, Switzerland, 2018; pp. 105–117. [Google Scholar]
- Ou, Y.K.; Wang, Y.L.; Chang, H.C.; Chen, C.C. Design and development of a wearable exoskeleton system for stroke rehabilitation. Healthcare 2020, 8, 18. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).