1. Introduction
Due to the COVID-19 pandemic and the extremely rapid increase in the number of infected people [
1], the medical world has had to consider adapting medical services by adopting new strategies for patient care and monitoring [
2,
3].
The COVID-19 disease took the medical world by surprise because, although this disease mainly affects the respiratory tract, the sequels also affect the heart, the brain and the digestive tract [
4]. At this point, we can say that COVID-19 is a disease of the whole body [
5].
Post-COVID-19 syndrome is a condition that is marked by the presence of symptoms (such as fatigue, cough, shortness of breath, headache or brain fog) which persist for an extended period of time (such as weeks or months) following a person’s initial recovery from a COVID-19 infection [
6].
The need for cardiopulmonary rehabilitation has increased with the COVID-19 pandemic due to the sequels developed as a result of this pathology [
7,
8,
9,
10]. Some studies have suggested that exercise should be applied in the acute phase for early and effective rehabilitation of COVID-19 patients with respiratory failure, while other studies propose the application of a three-stage exercise protocol, beginning in the inpatient phase, continues in the post-acute and continuous phase and at home after discharge for the good physical condition of the patients [
11].
At discharge, some studies have shown that most subjects with COVID-19 have cardiopulmonary sequels with reduced functional capacity, exercise tolerance and muscle strength, regardless of previous health condition/level and other pre-existing disabilities [
12,
13]. Increasing the exercise tolerance, decreasing the intensity/control of symptoms and improving the level of daily activity are the most documented benefits of cardiopulmonary rehabilitation [
14,
15]. In this case, cardiopulmonary rehabilitation in post-COVID-19 patients with cardiopulmonary sequels is necessary for them to have a normal life [
16,
17,
18].
Readers should exercise caution in applying rehabilitation with exercise training because of the risk of the post-exercise fatigue reported in some patients [
19]. Physiotherapists working with people with post-COVID-19 syndrome should determine the patient’s level of exercise tolerance to avoid exacerbation of symptoms after exertion [
20,
21].
2. Material and Methods
A literature review was performed according to the Preferred Reporting Items for Literature Reviews and Meta-Analyses (PRISMA) guidelines [
22].
A literature search was performed from January to April 2022, using the following medical subject headings terms and free-text terms: “post COVID-19 rehabilitation”, “post COVID sequels”, “modern technologies in post COVID cardiopulmonary rehabilitation” OR “telemedicine in COVID rehabilitation” and “monitoring devices used in cardiopulmonary rehabilitation”. Two authors independently performed all searches and removed duplicate records. A narrative synthesis of the selected articles was performed. Out of the 535 retrieved articles, the search resulted in a final total of 53 relevant published articles.
The aim of this study is to show that modern technologies have been a solid tool in the fight against cardiopulmonary sequels in patients infected with COVID-19.
3. Cardiopulmonary Rehabilitation
Cardiopulmonary sequels for post-COVID-19 patients are significant. Recent studies report patient desaturation and dyspnea during exercise in this category of patients. In this case, the therapeutic approach of the rehabilitation program should be based on the principles of cardiovascular and pulmonary rehabilitation with an emphasis on restoring functional capacity and increasing the muscular strength of patients [
23].
Prior to the pandemic, cardiopulmonary rehabilitation programs were available in two forms: center-based cardiac rehabilitation at the center and home-based cardiac rehabilitation at home, with an emphasis on rehabilitation in hospitals or specialized institutions for the proper supervision of patients [
24].
Since the Centers for Disease Control and Prevention recommends that all high-risk individuals, including those with cardiovascular risk factors, stay home to limit potential COVID-19 exposure, it changes the way the patient approaches the rehabilitation process changes. Rehabilitation programs in hospitals have been closed, suspended or discontinued, as many other elective and outpatient care activities have been suspended. In this way, the patients’ access to high-performance medical equipment used in cardiopulmonary rehabilitation has become limited. Complex medical equipment is used to monitor controlled heart rate, patient training heart rate and continuous ECG recording, which is required for the monitoring of heart rate, arrhythmias, decreased oxygen and blood pressure. A database for complete documentation is no longer available for home use.
At this time, attempts are being made to find solutions for remote cardiac rehabilitation to become a viable alternative. Current studies have demonstrated the efficacy of distance cardiopulmonary rehabilitation, improving patients’ short-term prognosis. At the moment, the solutions found are not necessarily related to e-health and telemedicine [
24].
4. Medical Technologies Used in Post-COVID-19 Cardiopulmonary Rehabilitation
4.1. Video Guides
There are few studies that specify the results of following a cardiopulmonary rehabilitation program at home through a video, although there are a large number of free videos on different platforms that offer cardiopulmonary rehabilitation programs. Old studies show us the benefit of cardiovascular rehabilitation at home following a program set by the attending physician [
25,
26].
Rosen K. et al. mentions that some patients who have participated in remote cardiopulmonary rehabilitation have been offered digital video disc (DVD) guides for rehabilitation at home. After discharge, patients were provided with a telephone consultation service by cardiologists and nurses, every 2 weeks for 5 months. The video addressed to patients explains at a basic level what heart failure is, presents some warm-up exercises, followed by aerobic exercises that can be applied both indoors and outdoors. Possible symptoms requiring emergency visits to the attending physician or the emergency department are also presented [
27].
4.2. Hybrid Approach
In order to facilitate the transition to telemedicine, there are studies currently testing the application of a post-COVID-19 cardiopulmonary rehabilitation program with a hybrid approach at the patient level. In this case, the patients are initially offered cardiac rehabilitation in a recovery center and then the long-term maintenance exercises are performed at the patient’s home, using various medical technologies. The complicated part of these studies is the demonstration of the effectiveness of these hybrid systems. This involves active and ongoing contact between patients and professionals through traditional methods, such as home visits and telephone consultations, or the use of technology-based solutions, which include web-based video calling and social networking platforms [
28].
There are studies that aim to investigate the effectiveness and safety of the application of cardiopulmonary recovery programs at home, by the patient, without supervision. In this sense, issued application protocols include two parts: an aerobic training using an ergometer, which will be installed at the patients’ homes, and patient education using an e-learning system. Cardiovascular parameters will be monitored remotely during exercise through video chats. An e-learning system that will promote a better understanding of cardiovascular disease is used. The necessary devices for cardiopulmonary recovery such as calibrated ergometers and tablets will be made available free of charge to the patients enrolled in the program. The patients will perform anaerobic exercises at home using the ergometer for 30–40 min at least 3 times a week. During the exercise, an instructor will monitor the patient in real time (using interactive video tools and monitoring tools for various vital data) [
29].
It is necessary to use monitoring systems of some important parameters in order to ensure the safety of the patient at home during the implementation of the rehabilitation program.
M. Pinto et al. proposes the development of national public health programs designed to support health systems, in particular regional healthcare and patients cured of a COVID-19 infection, by providing a model for organizing a dedicated network for post-acute rehabilitation. The purpose of this network is to provide continuity of care from acute hospitalization to home rehabilitation. It proposes the evaluation of patients based on a minimum set of early assessment and onset tools of the treatment of post-COVID-19 disabilities. An important emphasis is placed on technological promotion in healthcare, and especially in tele-rehabilitation [
30].
4.3. Telemedicine-Based Cardiopulmonary Rehabilitation
The Internet and mobile applications are currently the most widely used technologies in cardiopulmonary rehabilitation, especially in the COVID-19 era, offering patients a wide range of programs. In this sense, it is expected that all groups of cardiac or cardiopulmonary patients will benefit from this type of treatment [
31].
In this case, more and more studies show that telemedicine has been applied as a screening option to provide treatment to patients. Telemedicine can be considered as personal protective equipment that reduces the risk of exposure and contamination for both patients and practitioners [
32].
The COVID-19 pandemic has highlighted the importance and usefulness of telemedicine in providing a way to connect patients and healthcare professionals when a personal consultation is not possible [
33]. Tele-consultations are a safe and effective way to assess suspected cases of COVID-19 and to guide the patient’s diagnosis and treatment, minimizing the risk of disease transmission. Telemedicine also allows many of the key clinical services to continue to operate regularly and without interruption during a public health emergency [
34]. Telemedicine legislation varies across countries, but any healthcare institution interested in implementing telemedicine services must assess its technological level before doing so [
35].
Digital health technologies use computing platforms, connectivity, software and sensors for health care and related uses [
36].
Post-COVID-19 cardiopulmonary tele-rehabilitation has been shown to be effective in several recent studies [
37]. Marcelo Dalbosco-Salas et al. developed a tele-rehabilitation program with a duration of 24 session [
38]. At the beginning and the end of the rehabilitation program, all patients were evaluated in a primary care center. The tele-rehabilitation sessions were done at the home of the patient. The program included a warm-up (5 min), breathing exercises (3 min), aerobic and/or strength exercises (20–30 min) and stretching (5 min). The protocol was based on the recommendations of the Colegio Profesional de Fisioterapeutas de la Comunidad de Madrid [
39] and on the recommendations of the American College of Sports Medicine [
40]. The recovery program included weekly phone calls to assess the patients. Physiotherapists performed exercises at the same time as the patients using the online environment and using household objects, constantly assessing the patient’s condition using the Borg scale [
41].
A. Gabriela da Silva Vieira et al. showed that breathing exercise programs offered by tele-rehabilitation may improve functional capacity and reduce dyspnea in both patients with COVID-19 in the acute phase and in post-COVID-19 disorders. Tele-rehabilitation seems to be a safe environment for the patient, considering that adverse events occurred were generally mild or moderate. Tele-rehabilitation has also been shown not to increase hospital readmissions in patients infected with COVID-19. Breathing exercises delivered by tele-rehabilitation improved the results of the 6-min walking test, the score on the dyspnea questionnaire and the effort perceived by the patient from 0 to 10 on the Borg Scale [
42].
Li J suggests scheduling home visits for patients included in a tele-rehabilitation program at the time of inclusion in the program, at 6 weeks (post-treatment) and at 24 weeks (follow-up). Additional assessments were used for dyspnea performed by consultation by mobile phone or WeChat voice call at 2 and 4 weeks. They also used the 6-min walk test and devices for the monitoring of blood pressure, heart rate, oxygen saturation and lung function [
43].
Another method proposed by M. Paneroni et al. assumes that, upon admission to the tele-rehabilitation program that lasts a month, patients receive a pulse oximeter, a journal in which they will note their daily evolution and a leaflet and instructions with the types of exercises indicated. A physiotherapist contacts patients by video-call twice a week to monitor and determine the intensity of the exercise. Patients have a call center available 24/7. After a month, the patients in the program improve their exercise tolerance and dyspnea [
44].
Supervised multidisciplinary tele-rehabilitation programs must be included in the application of recovery programs for patients with COVID-19 after discharge from hospital. The implementation of these programs can lead to an effective assessment of the residual deficit [
45].
4.4. Virtual Reality in Cardiopulmonary Rehabilitation
Virtual reality (VR) could help patients in need of medical recovery. In the future, they could successfully perform the exercises at home, because the researchers will have been able to combine VR technology with 3D motion capture technology. VR offers high protocol customization capabilities, fully automatic reporting and tele-recovery functionality. It is designed as a “central hub” to which we connect a wide range of specialized peripheral devices, fully synchronized and integrated with this system, and being used as a clinical routine for recovery of a wide range of pathologies through numerous modules containing multiple clinically validated exercises [
46].
The application of virtual reality and video games has proven to be an adjunct tool in the conventional cardiopulmonary rehabilitation program. The results show that there was an increase in resistance to fatigue for the patient, an increased quality of life and a cessation of depression reported by patients [
47].
It has been observed that the application of virtual reality therapy on cardiac patients has significantly reduced the severity of depressive symptoms, anxiety and stress levels [
48].
Resources such as remote patient monitoring devices, artificial intelligence (AI), machine learning and block-chain systems must be combined to achieve complex lower cost cardiopulmonary rehabilitation programs [
49].
5. Patient Monitoring Devices Used at Home in COVID-19 Area
At this time, home rehabilitation programs use heart rate monitors to measure the heart rate during exercise sessions. Regarding this aspect, a reluctance of patients is reported, and some studies report only 35% of all patients were willing to use such a device at home. The study shows that reluctance does not take into account age, education or background. The study also reports that 68% of patients who did not use a heart rate monitor felt that heart rate monitoring was important during exercise at home. The same study shows that patients are not much more open to the application of modern technologies, reporting a number of 12% of patients who were willing to use a physical activity monitoring system such as counting steps and energy consumption. This monitoring has been made available through smart-watch devices or smartphone applications [
50].
The use of digital technology in healthcare has transformed the way we use health data and health information.
The Sheba Medical Center in Israel has adopted an application that interfaces with various portable medical devices and patient monitoring devices. In this study, the heart rate, the number of steps as well as the daily use of the application were monitored in correlation with a set of aerobic exercises (min) indicated through the application. Remote heart rehabilitation and heart failure programs using Bluetooth technology have been created and are currently monitoring hundreds of patients remotely, which has helped increase patient satisfaction and helped increase compliance with physical activity, even in the global pandemic context. The progress and tasks assigned to the patient are tracked with the help of the application so that the patient is monitored without having to come to the hospital [
51,
52].
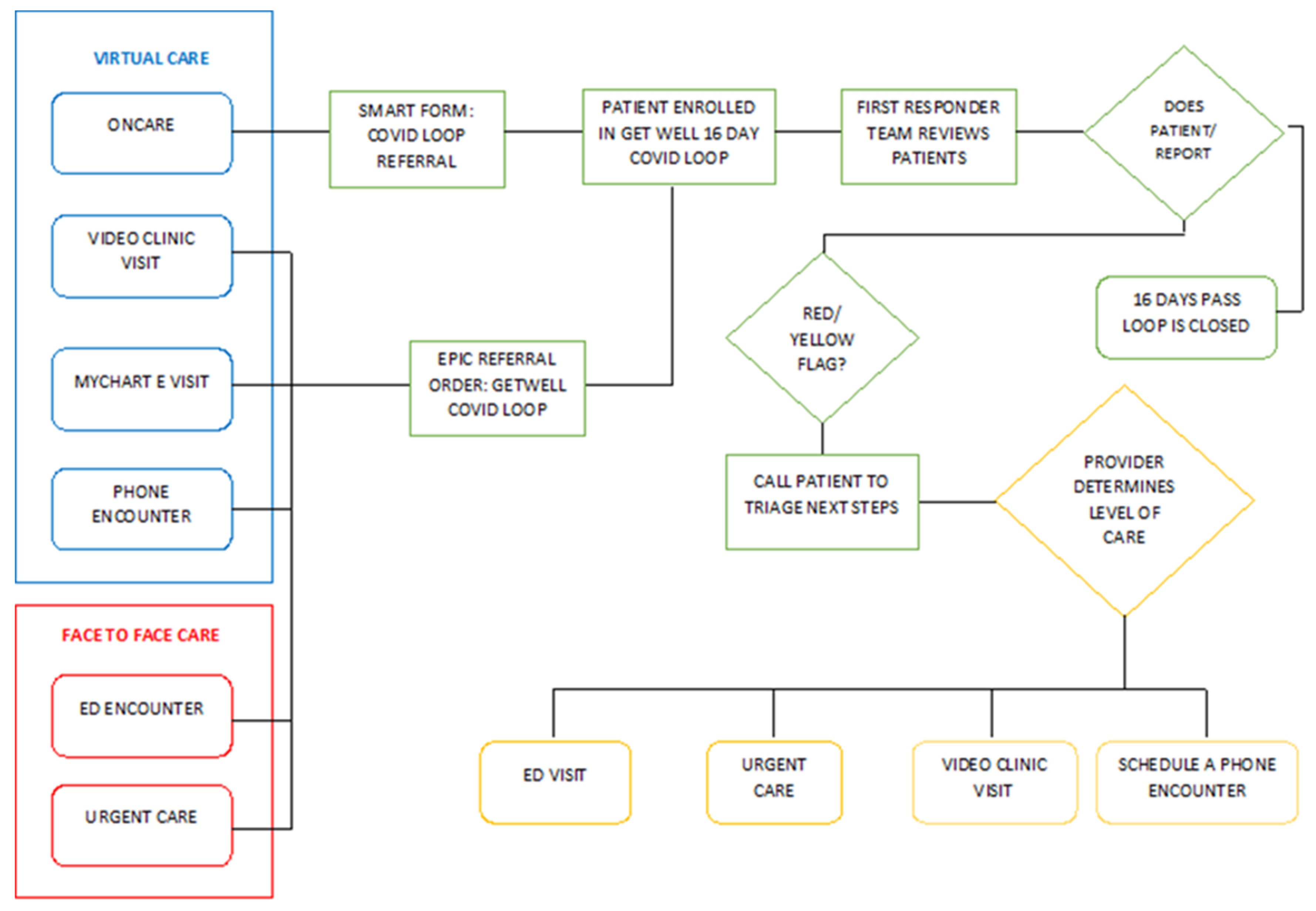
The University of Minnesota sought to assess the early lessons of a commitment and how the remote monitoring of patients can be achieved, thus developing a technological solution for patients with symptoms of the COVID-19 disease. Thus, remote monitoring of patients becomes a fast and efficient solution. The program involved patients who were offered educational materials and the opportunity to share their concerns. The development of the platform and the alerts were carried out with the help of some providers of a virtual care platform together with the medical students. They contributed to this platform by providing information about the patients’ conditions, monitoring the state of health and the vital parameters. The detection of these data resulted in over 2303 alerts, 4613 messages, 13 hospitalizations and 91 emergency room visits. The period in which the statistics were compiled was between 18 March and 20 April 2020, with 3701 patients enrolled in the program, of whom 2255 (60.93%) had symptoms of COVID-19.
This platform (
Figure 1) has provided patients with considerable support during the pandemic and of course a safe experience, while reducing COVID-19 exposure and excessive use of medical personnel. In conclusion, it can be highlighted that the remote monitoring of patients is an effective approach to managing the symptoms of COVID-19 at home and alerting medical staff in a very short time [
53].
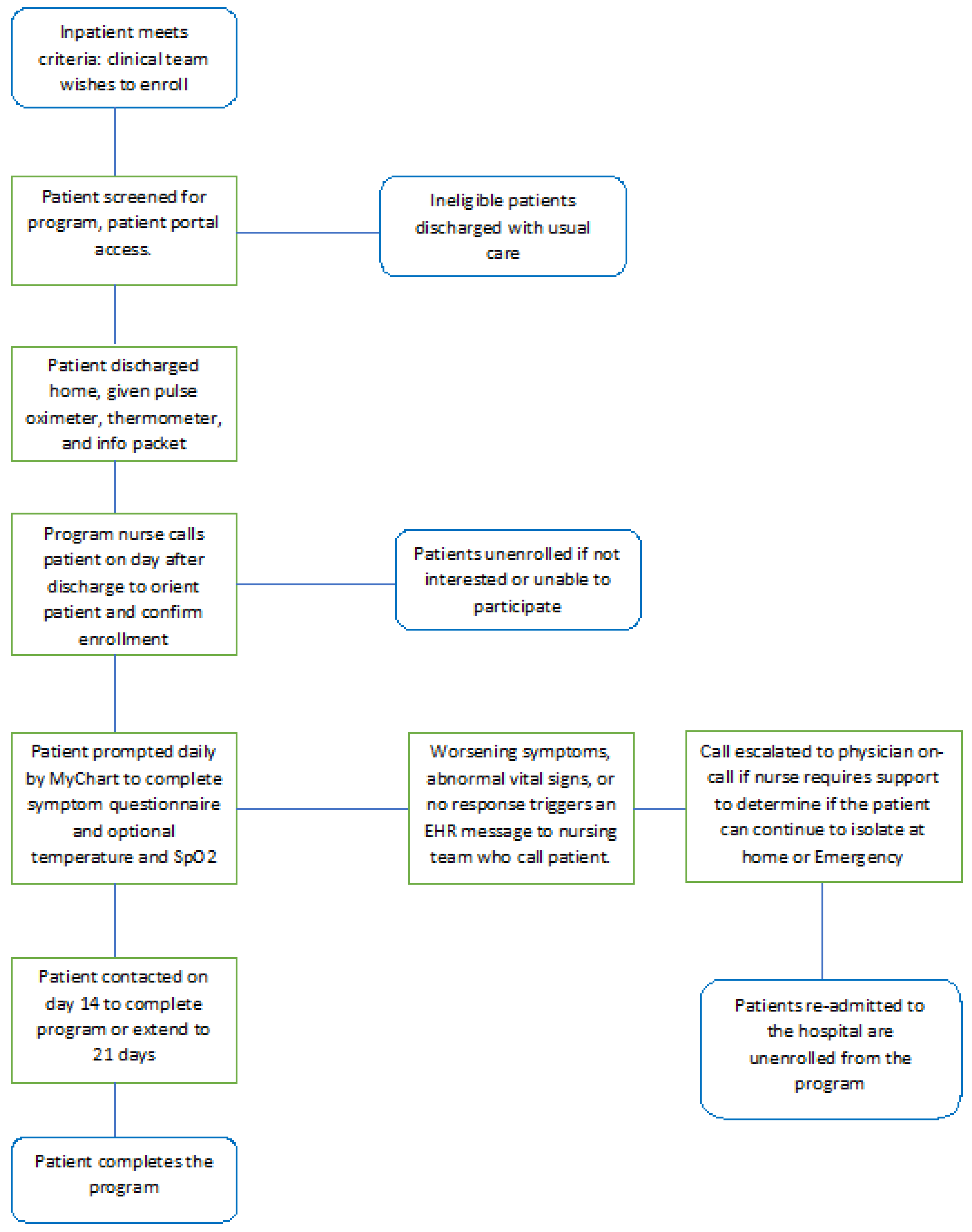
William J. set up a remote monitoring program for patients diagnosed with COVID-19, with the aim of monitoring them after discharge from the hospital [
50]. Thus, patients diagnosed with COVID-19 who were discharged from the hospital were selected. They were enrolled in the program and later received an application available for smartphone through which it is possible to record the data from the received pulse oximeter and thermometer.
The patients filled in their personal data in the application to automatically report symptoms as well as O
2 saturation and temperature at the end of each day. Abnormal symptoms or vital signs that do not meet the optimal parameters are evaluated by medical staff. Descriptive statistics were used to describe the characteristics of the patient and the program. A mixed-effect logistic regression model was used to determine the chances of a combined emergency department goal. A total of 295 patients were enrolled in the program from five participating hospitals. Many enrolled patients (66%) completed the monitoring period without triggering an abnormal alert. Enrollment was associated with a low chance of re-admission or re-hospitalization (adjusted rate: 0.54; 95% confidence interval: 0.3–0.97;
p = 0.039). Sending without enrollment was not associated with a reduced chance of re-admission or re-hospitalization. In conclusion, this study of remote monitoring platforms of patients conducted during the COVID-19 pandemic (
Figure 2) provides a mechanism for monitoring patients in their home environment and reducing hospital use [
54]. At the same time, having a strong impact on the evolution of patients after discharge, they were associated with a low risk of re-illness, giving hospitals a scalable mechanism to monitor patients at home as quickly as possible [
55].
There has been an acceleration of scientific discoveries, data dissemination and the development of new medical technologies to help manage this pandemic [
55].
At the same time, the pandemic highlighted the need for seismic changes in care paradigms and technology, with considerations related to the digital divide and health literacy for digital health interventions (HR) to reach their full potential and improve health outcomes. Here we can focus on advances in telemedicine, remote patient monitoring (RPM) and emerging portable technologies.
In conclusion, it can be highlighted that the remote monitoring platforms bring a high contribution in the development of the medical assistance system. Also, on the recommendation of the Virtual Care Task Force for the expansion of virtual health services in Canada, both the medical staff and the IT staff together with the group of medical bioengineers were laid. Thus, the platform’s proposal is based on a model for the optimal implementation of digital innovations in the field of health with five principles, including data management, data security, digital biomarkers, useful artificial intelligence and clinical integration [
56].
6. Conclusions
Cardiopulmonary rehabilitation at home has emerged as a necessity following the COVID-19 pandemic, as many patients are reported with post-COVID-19 cardiopulmonary sequels.
This review shows a high rate of use of medical technologies and a high level of interest in home rehabilitation, both by patients and health care providers. Cardiopulmonary rehabilitation in the context of post-COVID-19 sequels can be guided remotely based on current technologies.
The technologies applied in rehabilitation programs in the context of COVID-19 can be divided into: video guides, hybrid approaches, telemedicine-based cardiopulmonary rehabilitation and virtual reality in cardiopulmonary rehabilitation.
In order to ensure a safe environment for patients and to have access to the patient’s physiological parameters during the recovery program, various studies report the use of medical monitoring equipment by the patient at home.
The conclusions we can draw from analyzing existing studies is that there are many question marks related to quantifying the effectiveness of technology-based cardiopulmonary training programs. Another aspect to consider is the possibility of conducting a market study on the type of approach preferred by patients; remote rehabilitation or rehabilitation programs using modern technologies in a special center.
Author Contributions
Conceptualization, R.F., C.L., C.C. and D.A.; methodology, I.O.; software, D.-A.I. and A.S.; validation, A.S., D.-A.I. and I.O.; formal analysis, C.L.; investigation, R.F. and A.S.; resources, R.F., C.L., C.C. and D.A.; data curation, R.F., C.L., C.C. and D.A.; writing—original draft preparation, R.F., C.L., C.C. and D.A.; writing—review and editing, C.L.; visualization, C.L. and I.O.; supervision, C.C. and A.S.; project administration, C.L.; funding acquisition, D.-A.I. All authors have equally contributed to this article as senior authors. All authors have read and agreed to the published version of the manuscript.
Funding
This present manuscript’s article publishing charges were paid by the “Dunărea de Jos” University of Galati, 800008 Galati, Romania.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- WHO Reports. Available online: https://covid19.who.int (accessed on 20 March 2022).
- Mocanu, G.D.; Murariu, G.; Iordan, D.A.; Sandu, I.; Munteanu, M.O.A. The perception of the online teaching process during the COVID-19 pandemic for the students of the physical education and sports domain. Appl. Sci. 2021, 11, 5558. [Google Scholar] [CrossRef]
- Mocanu, G.D.; Murariu, G.; Georgescu, L.; Sandu, I. Investigating the Attitudes of First-Year Students of the Faculty of Physical Education and Sports of Galati towards Online Teaching Activities during the COVID-19 Pandemic. Appl. Sci. 2021, 11, 6328. [Google Scholar] [CrossRef]
- Baroiu, L.; Lese, A.C.; Stefanopol, I.A.; Iancu, A.; Dumitru, C.; Ciubara, A.B.; Bujoreanu, F.C.; Baroiu, N.; Ciubara, A.; Nechifor, A.; et al. The Role of D-Dimers in the Initial Evaluation of COVID-19. Ther. Clin. Risk Manag. 2022, 18, 323. [Google Scholar] [CrossRef]
- Hermann, M.; Pekacka-Egli, A.-M.; Witassek, F.; Baumgaertner, R.; Schoendorf, S.; Spielmanns, M. Feasibility and Efficacy of Cardiopulmonary Rehabilitation After COVID-19. Am. J. Phys. Med. Rehabil. 2020, 99, 10. [Google Scholar] [CrossRef] [PubMed]
- WHO Reports. Available online: https://www.who.int/news (accessed on 11 July 2022).
- The Novel Coronavirus Pneumonia Emergency Response Epidemiology Team. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19)—China, 2020. China CDC Wkly. 2020, 2, 113–122. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Farshidfar, F.; Koleini, N.; Ardehali, H. Cardiovascular complications of COVID-19. JCI Insight 2021, 6, e148980. [Google Scholar] [CrossRef]
- Sire, A.; Andrenelli, E.; Negrini, F.; Patrini, M.; Lazzarini, S.G.; Ceravolo, M.G. International Multiprofessional Steering Committee of Cochrane Rehabilitation REH-COVER Action. Rehabilitation and COVID-19: A rapid living systematic review by Cochrane Rehabilitation Field updated as of December 31st, 2020 and synthesis of the scientific literature of 2020. Eur. J. Phys. Rehabil. Med. 2021, 57, 181–188. [Google Scholar] [CrossRef]
- Xia, W.; Zhan, C.; Liu, S.; Yin, Z.; Wang, J.; Chong, Y.; Reinhardt, J.D. A telerehabilitation programme in post-discharge COVID-19 patients (TERECO): A randomised controlled trial. Thorax 2022, 77, 697–706. [Google Scholar]
- Thomas, E.; Gallagher, R.; Grace, S. Future-proofing cardiac rehabilitation: Transitioning services to telehealth during COVID-19. Eur. J. Prev. Cardiol. 2021, 28, 7. [Google Scholar] [CrossRef] [Green Version]
- Prvu Bettger, J.; Resnik, L.J. Telerehabilitation in the age of COVID-19: An opportunity for learning health system research. Phys. Ther. 2020, 100, 1913–1916. [Google Scholar] [CrossRef] [PubMed]
- Rehabilitation for Patients with COVID-19: Guidance for Occupational Therapists, Physical Therapists, Speech-Language Pathologists, and Assistants. McMaster Sch. Rehabil. Sci. Available online: https://srs-mcmaster.ca/wp-content/uploads/2020/04/Rehabilitation-for-Patients-with-COVID-19-Apr-08-2020.pdf (accessed on 5 March 2022).
- Brahmbhatt, D.H.; Ross, H.J.; Yasbanoo, M. Digital Technology Application for Improved Responses to Health Care Challenges: Lessons Learned from COVID-19. Can. J. Cardiol. 2021, 38, 279–291. [Google Scholar] [CrossRef] [PubMed]
- Werneke, M.W.; Deutscher, D.; Grigsby, D.; Tucker, C.A.; Mioduski, J.E.; Hayes, D. Telerehabilitation during the Covid-19 pandemic in outpatient rehabilitation settings: A descriptive study. Phys. Ther. 2021, 101, pzab110. [Google Scholar] [CrossRef] [PubMed]
- Royal Dutch Society for Physiotherapy 2020. KNGF Position Statement: Physiotherapy Recommendations in Patients with COVID-19; KNGF: Amersfoort, The Netherlands, 2020; Available online: https://www.kngf.nl/kennisplatform/guidelines (accessed on 10 March 2022).
- WHO. COVID-19 Clinical Management: Living Guidance; WHO: Geneva, Switzerland, 2021.
- Davisa, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’Em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef]
- Antoniou, V.; Davos, C.H.; Kapreli, E.; Batalik, L.; Panagiotakos, D.B.; Pepera, G. Effectiveness of Home-Based Cardiac Rehabilitation, Using Wearable Sensors, as a Multicomponent, Cutting-Edge Intervention: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 3772. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.H.; So, W.Y. Gender differences in home-based cardiac rehabilitation of post-percutaneous coronary intervention patients. Aging Clin. Exp. Res. 2021, 31, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Atsuko, N.; Naoko, T.; Momoko, K.; Kanako, H.; Naomi, M.; Fujiwara, T.; Hiroyuki, M.; Issei, K. Remote cardiac rehabilitation is a good alternative of outpatient cardiac rehabilitation in the COVID-19 era. Environ. Health Prev. Med. 2020, 25, 48. [Google Scholar]
- Kim, C.; Youn, J.E.; Choi, H.E. The effect of a self exercise program in cardiac rehabilitation for patients with coronary artery disease. Ann. Rehabil. Med. 2011, 35, 381–387. [Google Scholar] [CrossRef] [Green Version]
- Ades, P.A.; Keteyian, S.J.; Balady, G.J.; Houston-Miller, N.; Kitzman, D.W.; Mancini, D.M.; Rich, M.W. Cardiac rehabilitation exercise and self-care for chronic heart failure Review. JACC Heart Fail 2013, 1, 540–547. [Google Scholar] [CrossRef] [PubMed]
- Rosen, K.; Patel, M.; Lawrence, C.; Mooney, B. Delivering telerehabilitation to COVID-19 inpatients: A retrospective chart review suggests it is a viable option. HSS J. 2020, 16, 64–70. [Google Scholar] [CrossRef]
- Besnier, F.; Gayda, M.; Nigam, A.; Juneau, M.; Bherer, L. Cardiac rehabilitation during quarantine in COVID-19 pandemic: Challenges for center-based programs. Arch. Phys. Med. Rehabil. 2020, 101, 1835–1838. [Google Scholar] [CrossRef] [PubMed]
- Itoh, H.; Amiya, E.; Narita, K.; Shimbo, M.; Taya, M.; Komuro, I.; Hasegawa, T.; Makita, S.; Kimura, Y. Efficacy and Safety of Remote Cardiac Rehabilitation in the Recovery Phase of Cardiovascular Diseases: Protocol for a Multicenter, Nonrandomized, Single-Arm, Interventional Trial. JMIR Res. Protoc. 2021, 10, e30725. [Google Scholar] [CrossRef] [PubMed]
- Pinto, M.; Gimigliano, F.; De Simone, S.; Costa, M.; Bianchi, A.A.M.; Iolascon, G. Post-Acute COVID-19 Rehabilitation Network Proposal: From Intensive to Extensive and Home-Based IT Supported Services. Int. J. Environ. Res. Public Health 2020, 17, 9335. [Google Scholar] [CrossRef] [PubMed]
- Koceska, N.; Koceski, S.; Zobel, P.B.; Trajkovik, V.; Garcia, N.M. A Telemedicine Robot System for Assisted and Independent Living. Sensors 2019, 19, 834. [Google Scholar] [CrossRef] [Green Version]
- Nair, P. Editorial: Health Technologies and Innovations to Effectively Respond to the Covid-19 Pandemic. Front. Digit. Health 2022, 4, 849652. [Google Scholar] [CrossRef]
- Shaikh, A.; AlReshan, M.S.; Asiri, Y.; Sulaiman, A.; Alshahrani, H. Tele-COVID: A Telemedicine SOA-Based Architectural Design for COVID-19 Patients. CMC Comput. Mater. Contin. 2021, 67, 549–576. [Google Scholar] [CrossRef]
- Dalal, H.M.; Doherty, P.; Taylor, R.S. Cardiac rehabilitation. BMJ 2015, 351, h5000. [Google Scholar] [CrossRef] [Green Version]
- Verma, S. Early impact of CMS expansion of Medicare telehealth during COVID-19. Health Aff. Blog 2020, 15. [Google Scholar] [CrossRef]
- Index, Telehealth, Consumer Survey. Am. Well. 2019. Available online: https://static.americanwell.com/app/uploads/2019/07/American-Well-Telehealth-Index-2019-Consumer-Survey-eBook2.pdf (accessed on 20 March 2022).
- Cox, N.S.; Scrivener, K.; Holland, A.E.; Jolliffe, L.; Wighton, A.; Nelson, S.; McCredie, L.; Lannin, N.A. A brief intervention to support implementation of telerehabilitation by community rehabilitation services during COVID-19: A feasibility study. Arch. Phys. Med. Rehabil. 2021, 102, 789–795. [Google Scholar] [CrossRef] [PubMed]
- Dalbosco-Salas, M.; Torres-Castro, R.; Rojas Leyton, A.; Morales Zapata, F.; Henríquez Salazar, E.; Espinoza Bastías, G.; Beltrán Díaz, M.E.; Tapia Allers, K.; Mornhinweg Fonseca, D.; Vilaró, J. Effectiveness of a Primary Care Telerehabilitation Program for Post-COVID-19 Patients: A Feasibility Study. J. Clin. Med. 2021, 10, 4428. [Google Scholar] [CrossRef] [PubMed]
- Colegio Profesional de Fisioterapeutas de la Comunidad de Madrid Guía Recomendaciones de Fisioterapia Respiratoria y Ejercicio Terapéutico Para Personas Confinadas en Casa Y/O en Fase de Recuperación Domiciliaria del COVID-19. Available online: https://www.cfisiomad.org/pdf/publicacion_360.pdf (accessed on 10 July 2022).
- American College of Sports Medicine. ACSM’s Gudelines for Exercise Testing and Prescription, 11th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2021; Available online: https://www.acsm.org/read-research/books/acsms-guidelines-for-exercise-testing-and-prescription (accessed on 10 July 2022).
- Bestall, J.; Paul, E.A.; Garrod, R.; Garnham, R.; Jones, P.W.; Wedzicha, J.A. Usefulness of the medical research council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax 1999, 54, 581–586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Vieira, A.G.; Pinto, A.C.P.N.; Garcia, B.M.S.P.; Eid, R.A.C.; Mól, C.G.; Nawa, R.K. Telerehabilitation improves physical function and reduces dyspnoea in people with COVID-19 and post-COVID-19 conditions: A systematic review. J. Physiother. 2022, 68, 90–98. [Google Scholar] [CrossRef] [PubMed]
- British Society of Rehabilitation Medicine. Rehabilitation in the wake of Covid-19. A phoenix from the ashes. BSRM 2020. Available online: www.bsrm.org.uk/downloads/covid19bsrmissue1-published-27-4-2020.pdf (accessed on 5 March 2022).
- Paneroni, M.; Vitacca, M.; Bernocchi, P.; Bertacchini, L.; Scalvini, S. Feasibility of tele-rehabilitation in survivors of COVID-19 pneumonia. Pulmonology 2022, 28, 152–154. [Google Scholar] [CrossRef]
- Salawu, A.; Green, A.; Crooks, M.G.; Brixey, N.; Ross, D.H.; Sivan, M. A Proposal for Multidisciplinary Tele-Rehabilitation in the Assessment and Rehabilitation of COVID-19 Survivors. Int. J. Environ. Res. Public Health 2020, 17, 4890. [Google Scholar] [CrossRef] [PubMed]
- Lin, S. The present and future of team documentation: The role of patients, families, and artificial intelligence. Mayo Clin. Proc. 2020, 95, 852–855. [Google Scholar] [CrossRef] [PubMed]
- García-Bravo, S.; Cano-de-la-Cuerda, R.; Domínguez-Paniagua, J.; Campuzano-Ruiz, R.; Barreñada-Copete, E.; López-Navas, M.J.; Araujo-Narváez, A.; García-Bravo, C.; Florez-Garcia, M.; Botas-Rodríguez, J.; et al. Effects of Virtual Reality on Cardiac Rehabilitation Programs for Ischemic Heart Disease: A Randomized Pilot Clinical Trial. Int. J. Environ. Res. Public Health 2020, 17, 8472. [Google Scholar] [CrossRef] [PubMed]
- Szczepańska-Gieracha, J.; Jóźwik, S.; Cieślik, B.; Mazurek, J.; Gajda, R. Immersive Virtual Reality Therapy as a Support for Cardiac Rehabilitation: A Pilot Randomized-Controlled Trial. Cyberpsychol. Behav. Soc. Netw. 2021, 24, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.S.; Dalal, H.M.; McDonagh, S.T.J. The role of cardiac rehabilitation in improving cardiovascular outcomes. Nat. Rev. Cardiol. 2022, 19, 180–194. [Google Scholar] [CrossRef]
- Barker-Davies, R.M.; O’Sullivan, O.; Senaratne, K.P.P.; Baker, P.; Mark, C.; Shreshth, D.-D.; Henrietta, E.; Duncan, G.; Michael, G.; Sarah, L.; et al. The Stanford Hall consensus statement for post-COVID-19 rehabilitation. Br. J. Sports Med. 2020, 54, 949–959. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://magazine.cardiology2.com/feb2020/the_transformative_evolution (accessed on 5 March 2022).
- Zhang, Y.; Lu, M. A review of recent advancements in soft and flexible robots for medical applications. Int. J. Med. Robot. Comput. Assist. Surg. 2020, 16, e2096. [Google Scholar] [CrossRef] [PubMed]
- William, J.G.; Daniel, H.; Avital, D.; Herrick, N.F.; Jessica, J.; David, M.L.; Laura, M.; Sousa, D.; Su, M.Y.; Boxer, R. Remote Patient Monitoring Program for Hospital Discharged COVID-19. Appl. Clin. Inform. 2020, 11, 792–801. [Google Scholar] [CrossRef]
- Tucker, A.; Susan, P.; Gretchen, H.; Elizabeth, L.; Joshua, A.T.; Stephanie, B.; Sameer, B.; Genevieve, B.M. Rapid implementation of a COVID-19 remote patient monitoring program. J. Am. Med. Inform. Assoc. 2020, 27, 1326–1330. [Google Scholar] [CrossRef]
- Zhao, H.M.; Xie, Y.X.; Wang, C. Recommendations for respiratory rehabilitation in adults with coronavirus disease 2019. Chin. Med. J. 2020, 133, 1595–1602. [Google Scholar] [CrossRef] [PubMed]
- Royal College of Occupational Therapists. Guidance: A Quick Guide for Occupational Therapists—Rehabilitation for People Recovering from COVID-19. 2020. Available online: https://www.rcot.co.uk/sites/default/files/Quick%20guide%20for%20OTs%20People%20recovering%20from%20COVID-19.pdf (accessed on 6 June 2022).
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).



 ,
, 



{kind=link}
{kind=link}