
Assessment of Negative Gingival Recession: A Critical Component of Periodontal Diagnosis


Abstract
:1. Introduction
2. Normal Anatomy
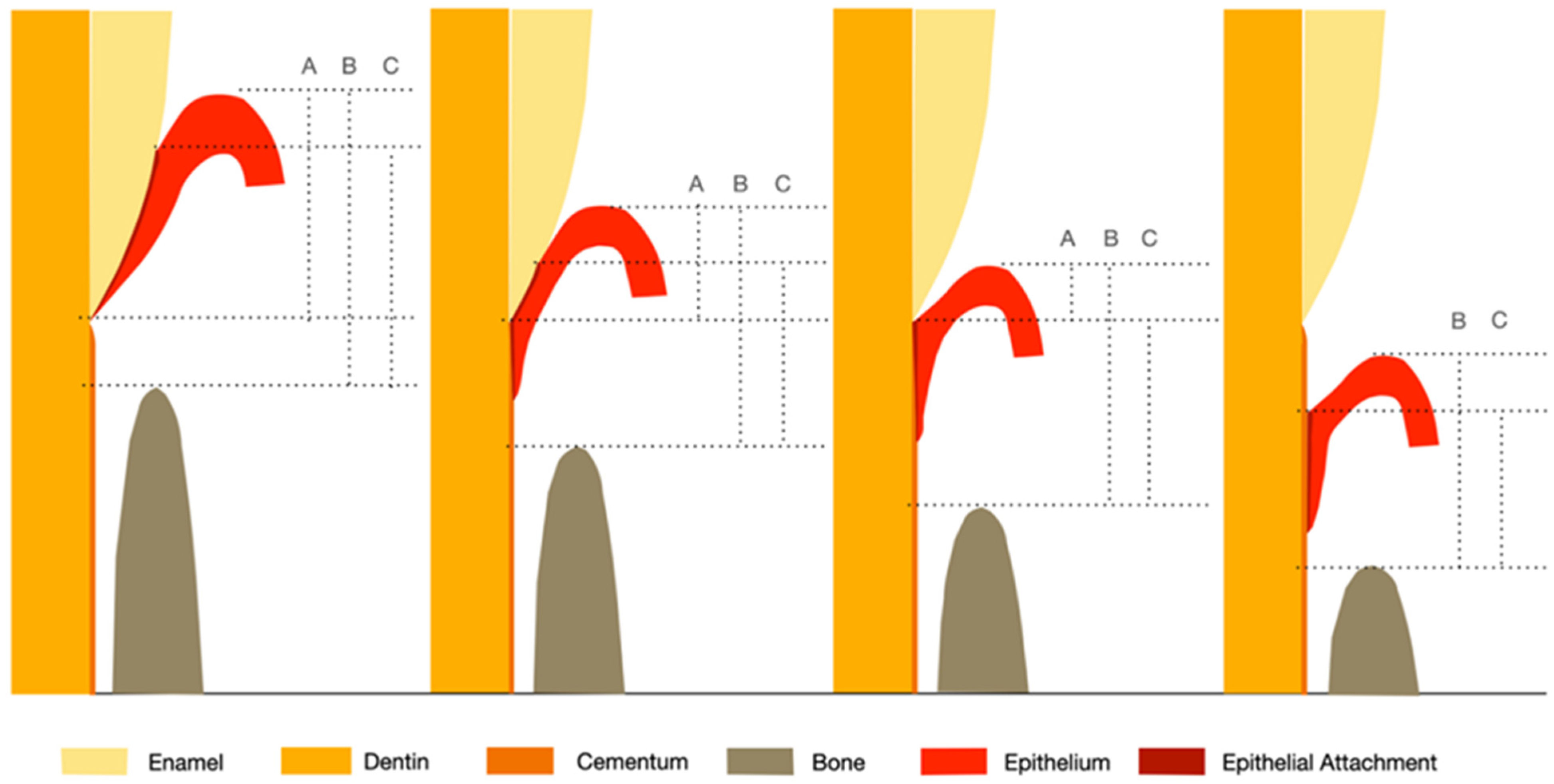
3. Altered Passive Eruption
4. Gingival Enlargement
5. Assessment of Clinical Attachment Loss
6. Clinical Assessment Approaches
6.1. Manual Instrumentation
6.2. Automated Instrumentation
6.3. Imaging Technologies
7. Conclusions
- Measuring the amount of gingiva recession, both negative and positive, is an integral part of determining the clinical attachment loss.
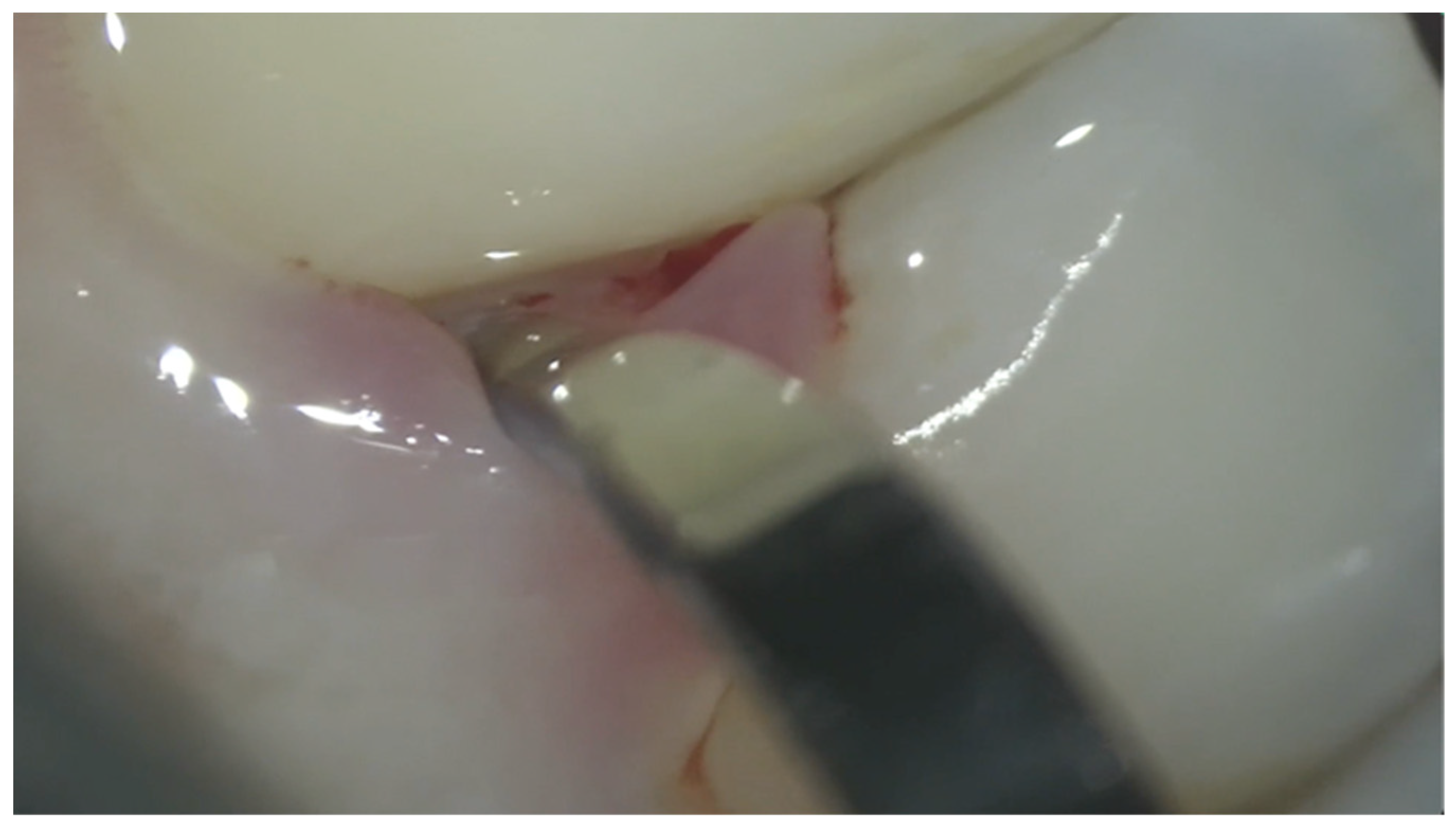
- Detecting the CEJ has proven to be a challenge clinically when the gingival margin is coronal to the CEJ. To properly diagnose the amount of negative gingival recession, understanding the normal site-specific anatomy is the first step.
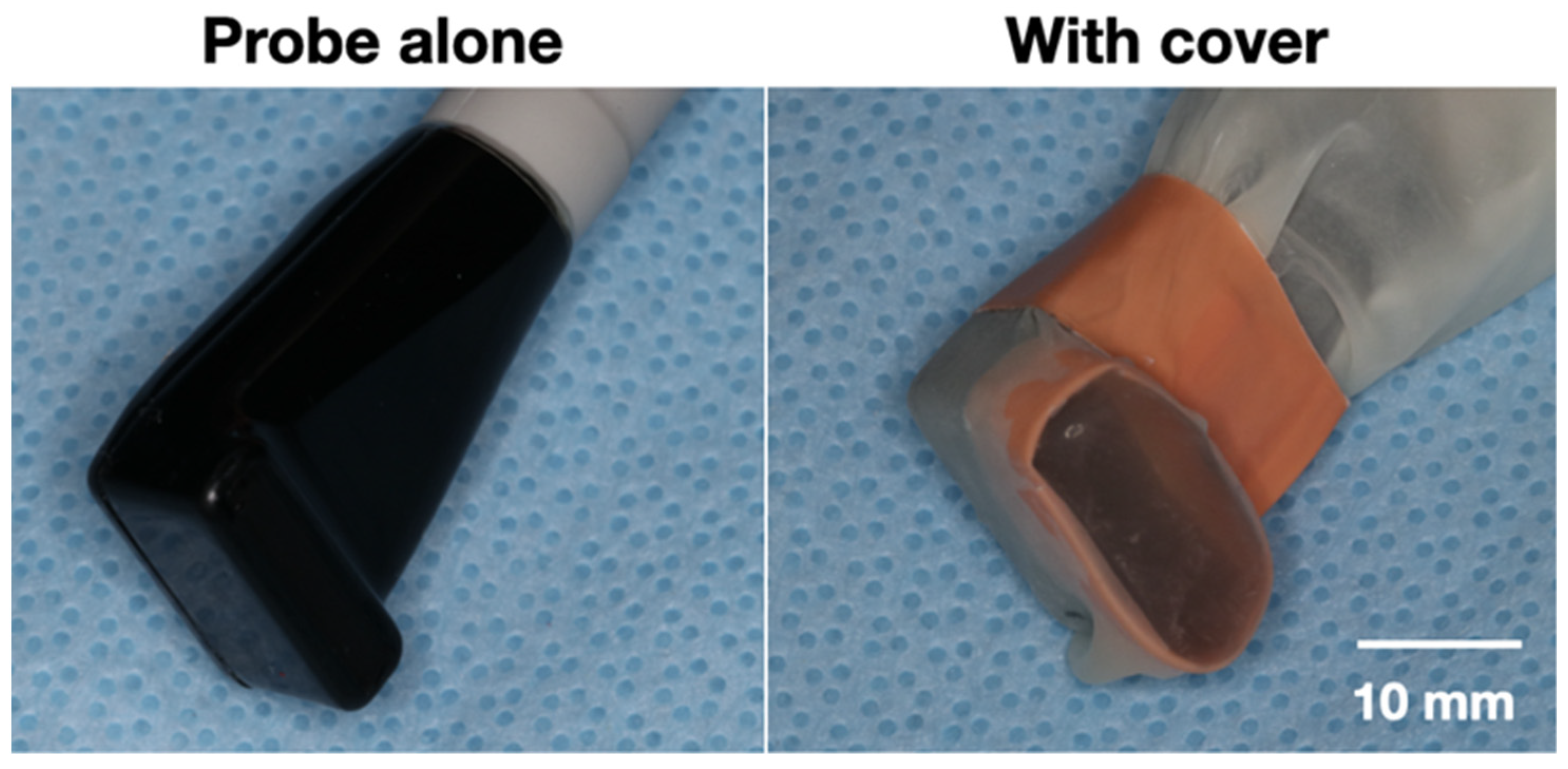
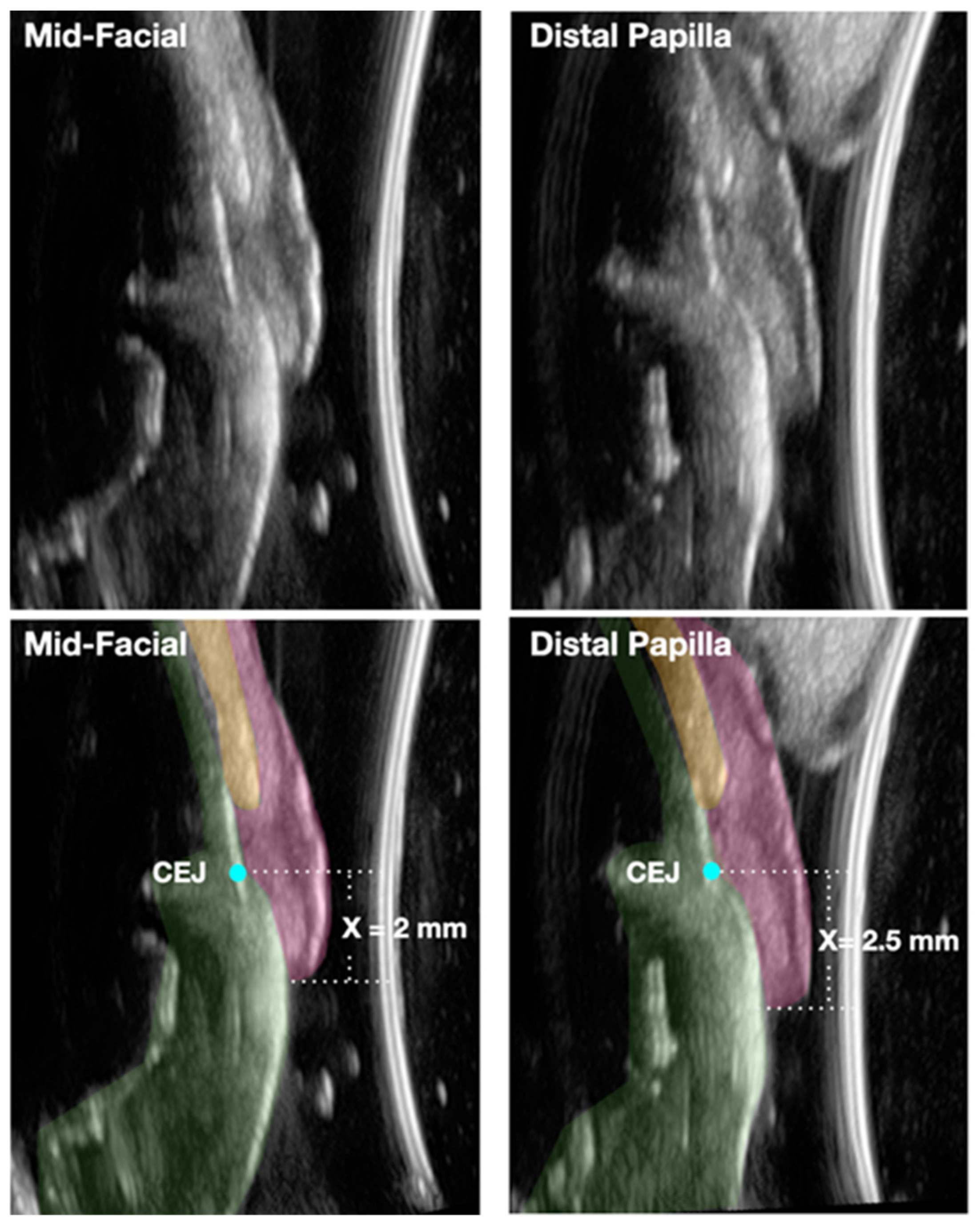
- With the aid of novel noninvasive and chairside ultrasound imaging and the high-magnification operating microscope, accurate and reproducible assessment of the negative gingival recession can become a reality that allows for early detection and intervention of periodontitis. These technologies could also prove to be valuable clinical and research tools in accurately detecting the amount of clinical attachment gain resulting from periodontal therapeutic modalities.
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Listgarten, M.A. Re: Periodontal terminology. J. Periodontol. 1993, 64, 918. [Google Scholar] [PubMed]
- Ramfjord, S.P. Indices for prevalence and incidence of periodontal disease. J. Periodontol. 1959, 30, 51–59. [Google Scholar] [CrossRef] [Green Version]
- Vandana, K.; Gupta, I. The location of cemento enamel junction for CAL measurement: A clinical crisis. J. Indian Soc. Periodontol. 2009, 13, 12–15. [Google Scholar] [CrossRef]
- Badersten, A.; Nilvéaus, R.; Egelberg, J. Reproducibility of probing attachment level measurements. J. Clin. Periodontol. 1984, 11, 475–485. [Google Scholar] [CrossRef]
- Hug, H.U.; Van’t Hof, M.A.; Spanauf, A.J.; Renggli, H.H. Validity of clinical assessments related to the cemento-enamel junction. J. Dent. Res. 1983, 62, 825–829. [Google Scholar] [CrossRef]
- Maynard, J.G., Jr.; Wilson, R. Physiologic dimensions of the periodontium significant to the restorative dentist. J. Periodontol. 1979, 50, 170–174. [Google Scholar] [CrossRef] [PubMed]
- Sicher, H. Changing concepts of the supporting dental structures. Oral Surg. Oral Med. Oral Pathol. 1959, 12, 31–35. [Google Scholar] [CrossRef]
- Gargiulo, A.W.; Wentz, F.M.; Orban, B. Dimensions and relations of the dentogingival junction in humans. J. Periodontol. 1961, 32, 261–267. [Google Scholar] [CrossRef] [Green Version]
- Jepsen, S.; Caton, J.G.; Albandar, J.M.; Bissada, N.F.; Bouchard, P.; Cortellini, P.; Demirel, K.; de Sanctis, M.; Ercoli, C.; Fan, J. Periodontal manifestations of systemic diseases and developmental and acquired conditions: Consensus report of workgroup 3 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, S219–S229. [Google Scholar] [CrossRef]
- Gottlieb, B.; Orban, B. Active and passive continuous eruption of teeth. J. Dent. Res. 1933, 13, 214. [Google Scholar]
- Mele, M.; Felice, P.; Sharma, P.; Mazzotti, C.; Bellone, P.; Zucchelli, G. Esthetic treatment of altered passive eruption. Periodontology 2000 2018, 77, 65–83. [Google Scholar] [CrossRef] [PubMed]
- Newman, M.G.; Takei, H.; Klokkevold, P.R.; Carranza, F.A. Newman and Carranza’s Clinical Periodontology; Elsevier Health Sciences: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Ainamo, J.; Löe, H. Anatomical characteristics of gingiva. A clinical and microscopic study of the free and attached gingiva. J. Periodontol. 1966, 37, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Vacek, J.S.; Gher, M.E.; Assad, D.A.; Richardson, A.C.; Giambarresi, L.I. The dimensions of the human dentogingival junction. Int. J. Periodontics Restor. Dent. 1994, 14, 154–165. [Google Scholar]
- Schmidt, J.C.; Sahrmann, P.; Weiger, R.; Schmidlin, P.R.; Walter, C. Biologic width dimensions—A systematic review. J. Clin. Periodontol. 2013, 40, 493–504. [Google Scholar] [CrossRef] [PubMed]
- Ash, M.M.; Nelson, S.J. Wheeler’s Dental Anatomy, Physiology and Occlusion, 8th ed.; Saunder Elsevier: St. Louis, MO, USA, 2003; p. 259. [Google Scholar]
- Becker, W.; Ochsenbein, C.; Tibbetts, L.; Becker, B.E. Alveolar bone anatomic profiles as measured from dry skulls: Clinical ramifications. J. Clin. Periodontol. 1997, 24, 727–731. [Google Scholar] [CrossRef] [PubMed]
- Kois, J.C. Altering gingival levels: The restorative connection part I: Biologic variables. Int. J. Periodontics Restor. Dent. 1994, 6, 3–7. [Google Scholar] [CrossRef]
- Pontoriero, R.; Carnevale, G. Surgical crown lengthening: A 12-month clinical wound healing study. J. Periodontol. 2001, 72, 841–848. [Google Scholar] [CrossRef]
- Van der Velden, U. Regeneration of the interdental soft tissues following denudation procedures. J. Clin. Periodontol. 1982, 9, 455–459. [Google Scholar] [CrossRef]
- Tarnow, D.P.; Magner, A.W.; Fletcher, P. The effect of the distance from the contact point to the crest of bone on the presence or absence of the interproximal dental papilla. J. Periodontol. 1992, 63, 995–996. [Google Scholar] [CrossRef] [Green Version]
- Chow, Y.C.; Eber, R.M.; Tsao, Y.P.; Shotwell, J.L.; Wang, H.L. Factors associated with the appearance of gingival papillae. J. Clin. Periodontol. 2010, 37, 719–727. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.-H.; Cho, Y.-J.; Lee, J.-Y.; Kim, S.-J.; Choi, J.-I. An analysis on the factors responsible for relative position of interproximal papilla in healthy subjects. J. Periodontal Implant Sci. 2013, 43, 160–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandana, K.; Savitha, B. Thickness of gingiva in association with age, gender and dental arch location. J. Clin. Periodontol. 2005, 32, 828–830. [Google Scholar] [CrossRef]
- De Rouck, T.; Eghbali, R.; Collys, K.; De Bruyn, H.; Cosyn, J. The gingival biotype revisited: Transparency of the periodontal probe through the gingival margin as a method to discriminate thin from thick gingiva. J. Clin. Periodontol. 2009, 36, 428–433. [Google Scholar] [CrossRef]
- Müller, H.P.; Heinecke, A.; Schaller, N.; Eger, T. Masticatory mucosa in subjects with different periodontal phenotypes. J. Clin. Periodontol. 2000, 27, 621–626. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.T.; Huang, N.C.; Wong, A.; Cobb, C.; Lee, S.; Mikail, Y.; Kao, R.T. Periodontal Risk Assessment Based on Dental and Gingival Morphology: A Comparative Analysis of African Versus Asian American Cohorts. Clin. Adv. Periodontics 2020, 10, 224–230. [Google Scholar] [CrossRef]
- Volchansky, A. Clinical definition for altered passive eruption. Br. Dent. J. 1979, 147, 292–293. [Google Scholar]
- Goldman, H.M.; Cohen, D.W. Periodontal Therapy; CV Mosby Company: Maryland Heights, MO, USA, 1973. [Google Scholar]
- Aghazada, R.; Marini, L.; Zeza, B.; Trezza, C.; Vestri, A.; Mariotti, A.; Pilloni, A. Experimental gingivitis in patients with and without altered passive eruption. J. Periodontol. 2020, 91, 938–946. [Google Scholar] [CrossRef]
- Alpiste-Illueca, F. Altered passive eruption (APE): A little-known clinical situation. Med. Oral Patol. Oral Cir. Bucal 2011, 16, e100–e104. [Google Scholar] [CrossRef] [Green Version]
- Volchansky, A.; Cleaton-Jones, P. Delayed passive eruption. A predisposing factor to Vincent’s infection. J. Dent. Assoc. S. Afr. 1974, 29, 291–294. [Google Scholar]
- Nart, J.; Carrió, N.; Valles, C.; Solís-Moreno, C.; Nart, M.; Reñé, R.; Esquinas, C.; Puigdollers, A. Prevalence of altered passive eruption in orthodontically treated and untreated patients. J. Periodontol. 2014, 85, e348–e353. [Google Scholar] [CrossRef]
- Alpiste-Illueca, F. Morphology and dimensions of the dentogingival unit in the altered passive eruption. Med. Oral Patol. Oral Cir. Bucal 2012, 17, e814–e820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evian, C.I.; Cutler, S.A.; Rosenberg, E.S.; Shah, R.K. Altered passive eruption: The undiagnosed entity. J. Am. Dent. Assoc. 1993, 124, 107–110. [Google Scholar] [CrossRef] [PubMed]
- Coslet, J.G.; Vanarsdall, R.; Weisgold, A. Diagnosis and classification of delayed passive eruption of the dentogingival junction in the adult. Alpha Omegan 1977, 70, 24–28. [Google Scholar]
- Bowers, G.M. A Study of the Width of Attached Gingiva. J. Periodontol. 1963, 34, 201–209. [Google Scholar] [CrossRef]
- Ragghianti Zangrando, M.S.; Veronesi, G.F.; Cardoso, M.V.; Michel, R.C.; Damante, C.A.; Sant’Ana, A.C.; de Rezende, M.L.; Greghi, S.L. Altered active and passive eruption: A modified classification. Clin. Adv. Periodontics 2017, 7, 51–56. [Google Scholar] [CrossRef]
- Kokich, V.O., Jr.; Kiyak, H.A.; Shapiro, P.A. Comparing the perception of dentists and lay people to altered dental esthetics. J. Esthet. Dent. 1999, 11, 311–324. [Google Scholar] [CrossRef] [PubMed]
- Sterrett, J.D.; Oliver, T.; Robinson, F.; Fortson, W.; Knaak, B.; Russell, C.M. Width/length ratios of normal clinical crowns of the maxillary anterior dentition in man. J. Clin. Periodontol. 1999, 26, 153–157. [Google Scholar] [CrossRef]
- Dolt, A.H.; Robbins, J.W. Altered passive eruption: An etiology of short clinical crowns. Quintessence Int. 1997, 28, 363–372. [Google Scholar]
- Garber, D.A.; Salama, M.A. The aesthetic smile: Diagnosis and treatment. Periodontology 2000 1996, 11, 18–28. [Google Scholar] [CrossRef]
- Silberberg, N.; Goldstein, M.; Smidt, A. Excessive gingival display–etiology, diagnosis, and treatment modalities. Quintessence Int. 2009, 40, 809–818. [Google Scholar]
- Zucchelli, G.; Gori, G. Altered Passive Eruption In: Mucogingival Esthetic Surgery; Quintessenza Edizioni: Milan, Italy, 2013. [Google Scholar]
- Murakami, S.; Mealey, B.L.; Mariotti, A.; Chapple, I.L. Dental plaque–induced gingival conditions. J. Clin. Periodontol. 2018, 45, S17–S27. [Google Scholar] [CrossRef] [PubMed]
- Holmstrup, P.; Plemons, J.; Meyle, J. Non–plaque-induced gingival diseases. J. Clin. Periodontol. 2018, 45, S28–S43. [Google Scholar] [CrossRef] [PubMed]
- Seymour, R.A.; Smith, D.G.; Turnbull, D.N. The effects of phenytoin and sodium valproate on the periodontal health of adult epileptic patients. J. Clin. Periodontol. 1985, 12, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Angelopoulos, A.P.; Goaz, P.W. Incidence of diphenylhydantoin gingival hyperplasia. Oral Surg. Oral Med. Oral Pathol. 1972, 34, 898–906. [Google Scholar] [CrossRef]
- McGaw, T.; Lam, S.; Coates, J. Cyclosporin-induced gingival overgrowth: Correlation with dental plaque scores, gingivitis scores, and cyclosporin levels in serum and saliva. Oral Surg. Oral Med. Oral Pathol. 1987, 64, 293–297. [Google Scholar] [CrossRef]
- Hassell, T.; O’Donnell, J.; Pearlman, J.; Tesini, D.; Murphy, T.; Best, H. Phenytoin induced gingival overgrowth in institutionalized epileptics. J. Clin. Periodontol. 1984, 11, 242–253. [Google Scholar] [CrossRef]
- Beaumont, J.; Chesterman, J.; Kellett, M.; Durey, K. Gingival overgrowth: Part 1: Aetiology and clinical diagnosis. Br. Dent. J. 2017, 222, 85–91. [Google Scholar] [CrossRef]
- Dongari-Bagtzoglou, A. Drug-associated gingival enlargement. J. Periodontol. 2004, 75, 1424–1431. [Google Scholar] [CrossRef]
- Uzel, M.I.; Kantarci, A.; Hong, H.H.; Uygur, C.; Sheff, M.C.; Firatli, E.; Trackman, P.C. Connective tissue growth factor in drug-induced gingival overgrowth. J. Periodontol. 2001, 72, 921–931. [Google Scholar] [CrossRef]
- Armitage, G.C. Clinical evaluation of periodontal diseases. Periodontology 2000 1995, 7, 39–53. [Google Scholar] [CrossRef]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89, S173–S182. [Google Scholar] [CrossRef] [Green Version]
- Grossman, E.S.; Hargreaves, J.A. Variable cementoenamel junction in one person. J. Prosthet. Dent. 1991, 65, 93–97. [Google Scholar] [CrossRef]
- Watts, T. Constant force probing with and without a stent in untreated periodontal disease: The clinical reproducibility problem and possible sources of error. J. Clin. Periodontol. 1987, 14, 407–411. [Google Scholar] [CrossRef] [PubMed]
- Clerehugh, V.; Abdeia, R.; Hull, P.S. The effect of subgingival calculus on the validity of clinical probing measurements. J. Dent. 1996, 24, 329–333. [Google Scholar] [CrossRef]
- Bader, J.; Rozier, R.G.; McFall, W.T., Jr. The effect of crown receipt on measures of gingival status. J. Dent. Res. 1991, 70, 1386–1389. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89 (Suppl. 1), S159–S172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villata, L.; Baelum, V. Reproducibility of attachment level recordings using an electronic and a conventional probe. J. Periodontol. 1996, 67, 1292–1300. [Google Scholar] [CrossRef]
- Holtfreter, B.; Alte, D.; Schwahn, C.; Desvarieux, M.; Kocher, T. Effects of different manual periodontal probes on periodontal measurements. J. Clin. Periodontol. 2012, 39, 1032–1041. [Google Scholar] [CrossRef] [Green Version]
- Garnick, J.J.; Silverstein, L. Periodontal probing: Probe tip diameter. J. Periodontol. 2000, 71, 96–103. [Google Scholar] [CrossRef]
- Atassi, F.; Newman, H.N.; Bulman, J.S. Probe tine diameter and probing depth. J. Clin. Periodontol. 1992, 19, 301–304. [Google Scholar] [CrossRef]
- van der Velden, U. Probing force and the relationship of the probe tip to the periodontal tissues. J. Clin. Periodontol. 1979, 6, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Persson, G.R. Effects of line-angle versus midproximal periodontal probing measurements on prevalence estimates of periodontal disease. J. Periodontal. Res. 1991, 26, 527–529. [Google Scholar] [CrossRef] [PubMed]
- Grossi, S.G.; Dunford, R.G.; Ho, A.; Koch, G.; Machtei, E.E.; Genco, R.J. Sources of error for periodontal probing measurements. J. Periodontal. Res. 1996, 31, 330–336. [Google Scholar] [CrossRef]
- Watts, T.L. Probing site configuration in patients with untreated periodontitis. A study of horizontal positional error. J. Clin. Periodontol. 1989, 16, 529–533. [Google Scholar] [CrossRef] [PubMed]
- van der Velden, U. Influence of periodontal health on probing depth and bleeding tendency. J. Clin. Periodontol. 1980, 7, 129–139. [Google Scholar] [CrossRef]
- Listgarten, M.A. Periodontal probing: What does it mean? J. Clin. Periodontol. 1980, 7, 165–176. [Google Scholar] [CrossRef]
- Armitage, G.C. Manual periodontal probing in supportive periodontal treatment. Periodontology 2000 1996, 12, 33–39. [Google Scholar] [CrossRef]
- Goodson, J.M. Clinical measurements of periodontitis. J. Clin. Periodontol. 1986, 13, 446–460. [Google Scholar] [CrossRef]
- Hill, E.G.; Slate, E.H.; Wiegand, R.E.; Grossi, S.G.; Salinas, C.F. Study design for calibration of clinical examiners measuring periodontal parameters. J. Periodontol. 2006, 77, 1129–1141. [Google Scholar] [CrossRef]
- Glavind, L.; Löe, H. Errors in the clinical assessment of periodontal destruction. J. Periodontal. Res. 1967, 2, 180–184. [Google Scholar] [CrossRef]
- Kingman, A.; Löe, H.; Ånerud, Å.; Boysen, H. Errors in measuring parameters associated with periodontal health and disease. J. Periodontol. 1991, 62, 477–486. [Google Scholar] [CrossRef] [PubMed]
- Barendregt, D.S.; van der Velden, U.; Timmerman, M.F.; Bulthuis, H.M.; van der Weijden, F. Detection of the cemento-enamel junction with three different probes: An “in vitro” model. J. Clin. Periodontol. 2009, 36, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, G.; Wilton, J.; Curtis, M.; Maiden, M.; Gillett, I.; Wilson, D.; Sterne, J.; Johnson, N. Detection of high-risk groups and individuals for periodontal diseases: Clinical assessment of the periodontium. J. Clin. Periodontol. 1988, 15, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Corraini, P.; Baelum, V.; Lopez, R. Reliability of direct and indirect clinical attachment level measurements. J. Clin. Periodontol. 2013, 40, 896–905. [Google Scholar] [CrossRef]
- Jeffcoat, M.K.; Jeffcoat, R.L.; Jens, S.C.; Captain, K. A new periodontal probe with automated cemento-enamel junction detection. J. Clin. Periodontol. 1986, 13, 276–280. [Google Scholar] [CrossRef]
- Jeffcoat, M.K.; Jeffcoat, R.L.; Captain, K. A periodontal probe with automated cemento--enamel junction detection-design and clinical trials. IEEE Trans. Biomed. Eng. 1991, 38, 330–333. [Google Scholar] [CrossRef]
- Preshaw, P.M.; Kupp, L.; Hefti, A.F.; Mariotti, A. Measurement of clinical attachment levels using a constant-force periodontal probe modified to detect the cemento-enamel junction. J. Clin. Periodontol. 1999, 26, 434–440. [Google Scholar] [CrossRef]
- Karpinia, K.; Magnusson, I.; Gibbs, C.; Yang, M.C. Accuracy of probing attachment levels using a CEJ probe versus traditional probes. J. Clin. Periodontol. 2004, 31, 173–176. [Google Scholar] [CrossRef]
- Deepa, R.; Prakash, S. Accuracy of probing attachment levels using a new computerized cemento-enamel junction probe. J. Indian Soc. Periodontol. 2012, 16, 74–79. [Google Scholar] [CrossRef]
- Haffajee, A.D.; Socransky, S.S.; Goodson, J.M. Clinical parameters as predictors of destructive periodontal disease activity. J. Clin. Periodontol. 1983, 10, 257–265. [Google Scholar] [CrossRef]
- Gibbs, C.H.; Hirschfeld, J.W.; Lee, J.G.; Low, S.B.; Magnusson, I.; Thousand, R.R.; Yerneni, P.; Clark, W.B. Description and clinical evaluation of a new computerized periodontal probe—The Florida probe. J. Clin. Periodontol. 1988, 15, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.F.; Leknes, K.N.; Zimmerman, G.J.; Sigurdsson, T.J.; Wikesjö, U.M.; Selvig, K.A. Intra-and inter-examiner reproducibility in constant force probing. J. Clin. Periodontol. 1995, 22, 918–922. [Google Scholar] [CrossRef] [PubMed]
- Hefti, A.F. Periodontal Probing. Crit. Rev. Oral Biol. Med. 1997, 8, 336–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trombelli, L.; Farina, R.; Silva, C.O.; Tatakis, D.N. Plaque-induced gingivitis: Case definition and diagnostic considerations. J. Periodontol. 2018, 89 (Suppl. 1), S46–S73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quirynen, M.; Callens, A.; van Steenberghe, D.; Nys, M. Clinical evaluation of a constant force electronic probe. J. Periodontol. 1993, 64, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Perry, D.A.; Taggart, E.J.; Leung, A.; Newburn, E. Comparison of a conventional probe with electronic and manual pressure-regulated probes. J. Periodontol. 1994, 65, 908–913. [Google Scholar] [CrossRef]
- Bareja, H.; Bansal, M.; Naveen Kumar, P.G. Comparative assessment of conventional periodontal probes and CEJ handpiece of electronic probes in the diagnosis and primary care of periodontal disease. J. Fam. Med. Prim. Care 2021, 10, 692–698. [Google Scholar] [CrossRef]
- Brezniak, N.; Goren, S.; Zoizner, R.; Shochat, T.; Dinbar, A.; Wasserstein, A.; Heller, M. The accuracy of the cementoenamel junction identification on periapical films. Angle Orthod. 2004, 74, 496–500. [Google Scholar] [CrossRef]
- Patcas, R.; Markic, G.; Müller, L.; Ullrich, O.; Peltomäki, T.; Kellenberger, C.J.; Karlo, C.A. Accuracy of linear intraoral measurements using cone beam CT and multidetector CT: A tale of two CTs. Dentomaxillofac. Radiol. 2012, 41, 637–644. [Google Scholar] [CrossRef] [Green Version]
- Ghorayeb, S.R.; Bertoncini, C.A.; Hinders, M.K. Ultrasonography in dentistry. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2008, 55, 1256–1266. [Google Scholar] [CrossRef]
- Lynch, J.; Hinders, M. Ultrasonic device for measuring periodontal attachment levels. Rev. Sci. Instrum. 2002, 73, 2686–2693. [Google Scholar] [CrossRef] [Green Version]
- Tsiolis, F.I.; Needleman, I.G.; Griffiths, G.S. Periodontal ultrasonography. J. Clin. Periodontol. 2003, 30, 849–854. [Google Scholar] [CrossRef] [PubMed]
- Chifor, R.; HedeÅŸiu, M.; Bolfa, P.; Catoi, C.; Crisan, M.; Serbanescu, A.; Badea, A.F.; Moga, I. The evaluation of 20 MHz ultrasonography, computed tomography scans as compared to direct microscopy for periodontal system assessment. Med. Ultrason. 2011, 13, 120–126. [Google Scholar] [PubMed]
- Nguyen, K.-C.T.; Le, L.H.; Kaipatur, N.R.; Zheng, R.; Lou, E.H.; Major, P.W. High-resolution ultrasonic imaging of dento-periodontal tissues using a multi-element phased array system. Ann. Biomed. Eng. 2016, 44, 2874–2886. [Google Scholar] [CrossRef]
- Chifor, R.; Badea, M.E.; Hedesiu, M.; Serbanescu, A.; Badea, A.F. Experimental model for measuring and characterisation of the dento-alveolar system using high frequencies ultrasound techniques. Med. Ultrason. 2010, 12, 127–132. [Google Scholar]
- Mahmoud, A.M.; Ngan, P.; Crout, R.; Mukdadi, O.M. High-resolution 3D ultrasound jawbone surface imaging for diagnosis of periodontal bony defects: An in vitro study. Ann. Biomed. Eng. 2010, 38, 3409–3422. [Google Scholar] [CrossRef]
- Chan, H.-L.; Sinjab, K.; Chung, M.-P.; Chiang, Y.-C.; Wang, H.-L.; Giannobile, W.V.; Kripfgans, O.D. Non-invasive evaluation of facial crestal bone with ultrasonography. PLoS ONE 2017, 12, e0171237. [Google Scholar] [CrossRef] [Green Version]
- Zimbran, A.; Dudea, S.M.; Dudea, D. Evaluation of periodontal tissues using 40MHz ultrasonography. preliminary report. Med. Ultrason. 2013, 15, 6–9. [Google Scholar] [CrossRef]
- Salmon, B.; Le Denmat, D. Intraoral ultrasonography: Development of a specific high-frequency probe and clinical pilot study. Clin. Oral Investig. 2012, 16, 643–649. [Google Scholar] [CrossRef]
- Nguyen, K.-C.T.; Yan, Y.; Kaipatur, N.R.; Major, P.W.; Lou, E.H.; Punithakumar, K.; Le, L.H. Computer-Assisted Detection of Cemento-Enamel Junction in Intraoral Ultrasonographs. Appl. Sci. 2021, 11, 5850. [Google Scholar] [CrossRef]
- Tattan, M.; Sinjab, K.; Lee, E.; Arnett, M.; Oh, T.J.; Wang, H.L.; Chan, H.L.; Kripfgans, O.D. Ultrasonography for chairside evaluation of periodontal structures: A pilot study. J. Periodontol. 2020, 91, 890–899. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, K.-C.T.; Le, L.H.; Kaipatur, N.R.; Major, P.W. Imaging the cemento-enamel junction using a 20-MHz ultrasonic transducer. Ultrasound Med. Biol. 2016, 42, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, R.; Sinjab, K.; Pan, Y.C.; Soki, F.; Chan, H.L.; Kripfgans, O. Comprehensive peri-implant tissue evaluation with ultrasonography and cone-beam computed tomography: A pilot study. Clin. Oral Implant. Res. 2021, 32, 777–785. [Google Scholar] [CrossRef]
- Chan, H.L.; Sinjab, K.; Li, J.; Chen, Z.; Wang, H.L.; Kripfgans, O.D. Ultrasonography for noninvasive and real-time evaluation of peri-implant tissue dimensions. J. Clin. Periodontol. 2018, 45, 986–995. [Google Scholar] [CrossRef] [PubMed]
- Magnusson, I.; Listgarten, M.A. Histological evaluation of probing depth following periodontal treatment. J. Clin. Periodontol. 1980, 7, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Fowler, C.; Garrett, S.; Crigger, M.; Egelberg, J. Histologic probe position in treated and untreated human periodontal tissues. J. Clin. Periodontol. 1982, 9, 373–385. [Google Scholar] [CrossRef] [PubMed]
- Armitage, G.C.; Svanberg, G.K.; Löe, H. Microscopic evaluation of clinical measurements of connective tissue attachment levels. J. Clin. Periodontol. 1977, 4, 173–190. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Passive Eruption Phase | I | II | III | IV |
|---|---|---|---|---|
| Mean age in years | 24.5 | 31.4 | 32.3 | 39.7 |
| Negative gingival recession (mm) | 2.15 | 1.29 | 0.6 | - |
| Total dentogingival junction (mm) | 3.23 | 2.78 | 2.41 | 2.53 |
| Supracrestal tissue attachment (mm) | 2.43 | 2.17 | 1.8 | 1.77 |
| Advantages | Disadvantages | |
|---|---|---|
| Periodontal probing | Easy, economical, quick | Prone to visual and tactile error |
| 2D radiography | Economical | Only detect interproximal CEJ, poor soft-tissue contrast resolution, errors related to image-acquisition angle |
| 3D radiography | CEJ is identifiable at bucco/lingual and interproximal sites | Ionization, expensive, poor soft-tissue contrast, lower image resolution |
| Ultrasound imaging | Noninvasive, nonionizing, chairside, providing digital image including dimension from gingiva margin to CEJ | Coupling agent needed, time-consuming, technique-sensitive |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, I.-C.; Chan, H.-L.; Johnson, G.K.; Elangovan, S. Assessment of Negative Gingival Recession: A Critical Component of Periodontal Diagnosis. Appl. Sci. 2022, 12, 7015. https://doi.org/10.3390/app12147015
Wang I-C, Chan H-L, Johnson GK, Elangovan S. Assessment of Negative Gingival Recession: A Critical Component of Periodontal Diagnosis. Applied Sciences. 2022; 12(14):7015. https://doi.org/10.3390/app12147015
Chicago/Turabian StyleWang, I-Ching, Hsun-Liang Chan, Georgia K. Johnson, and Satheesh Elangovan. 2022. "Assessment of Negative Gingival Recession: A Critical Component of Periodontal Diagnosis" Applied Sciences 12, no. 14: 7015. https://doi.org/10.3390/app12147015
APA StyleWang, I.-C., Chan, H.-L., Johnson, G. K., & Elangovan, S. (2022). Assessment of Negative Gingival Recession: A Critical Component of Periodontal Diagnosis. Applied Sciences, 12(14), 7015. https://doi.org/10.3390/app12147015