
Comparison of Bone Segmentation Software over Different Anatomical Parts

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Methods
2.1. CT Scan Collection
2.2. Segmentation Software Packages
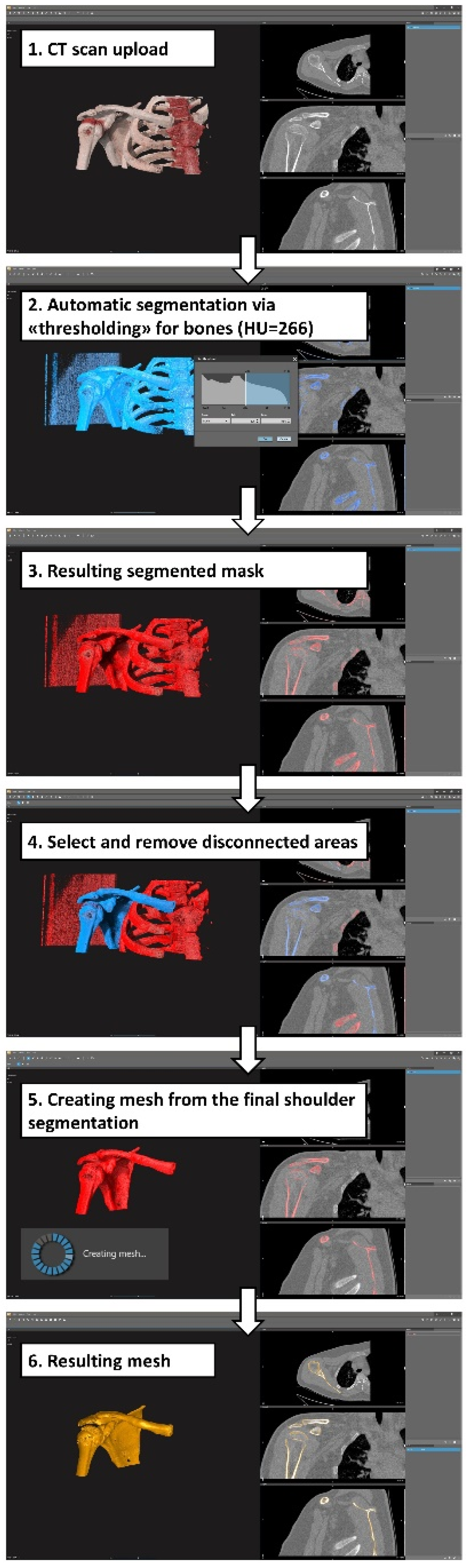
2.3. Medical Image Segmentation Process
2.4. Data Collection and Processing
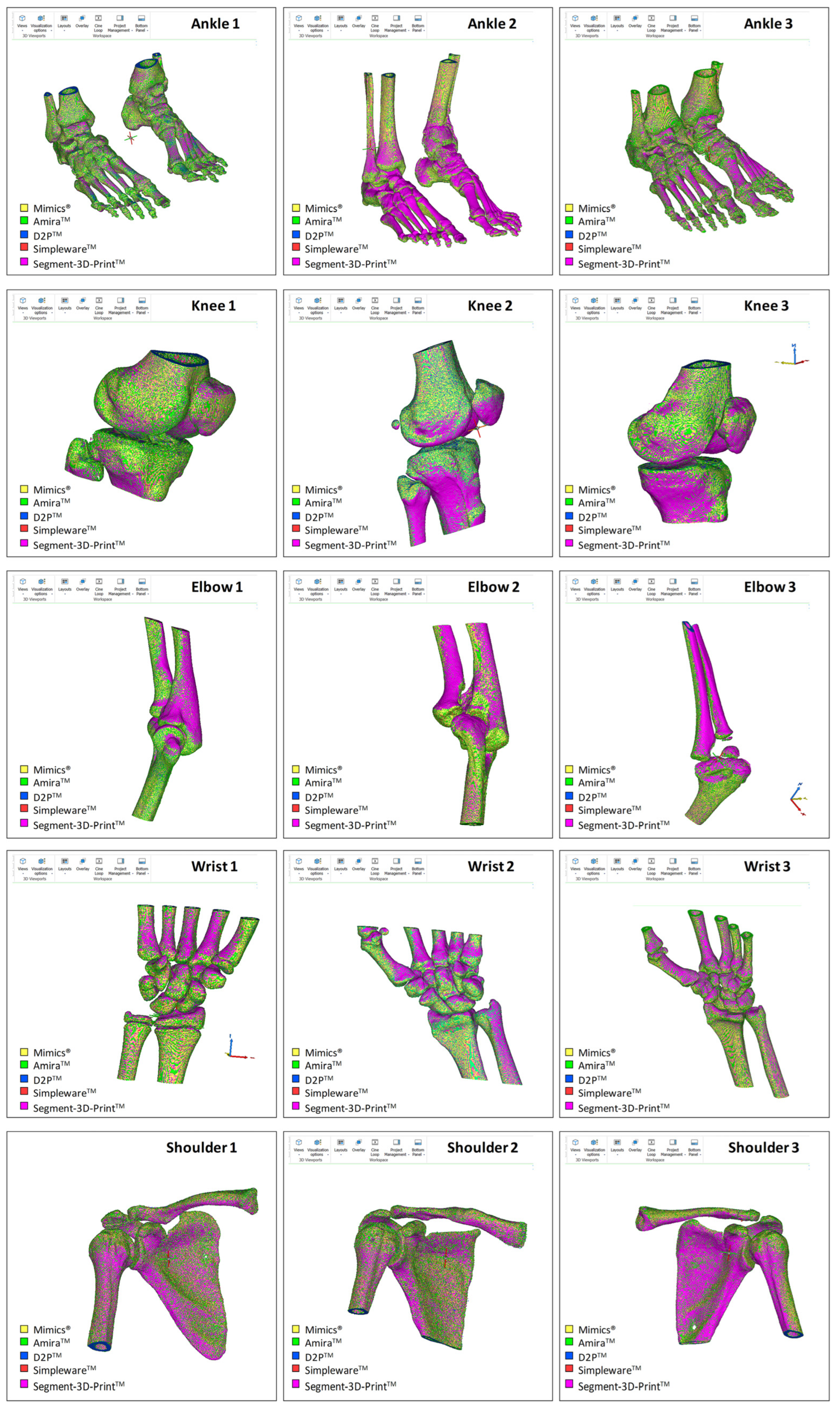
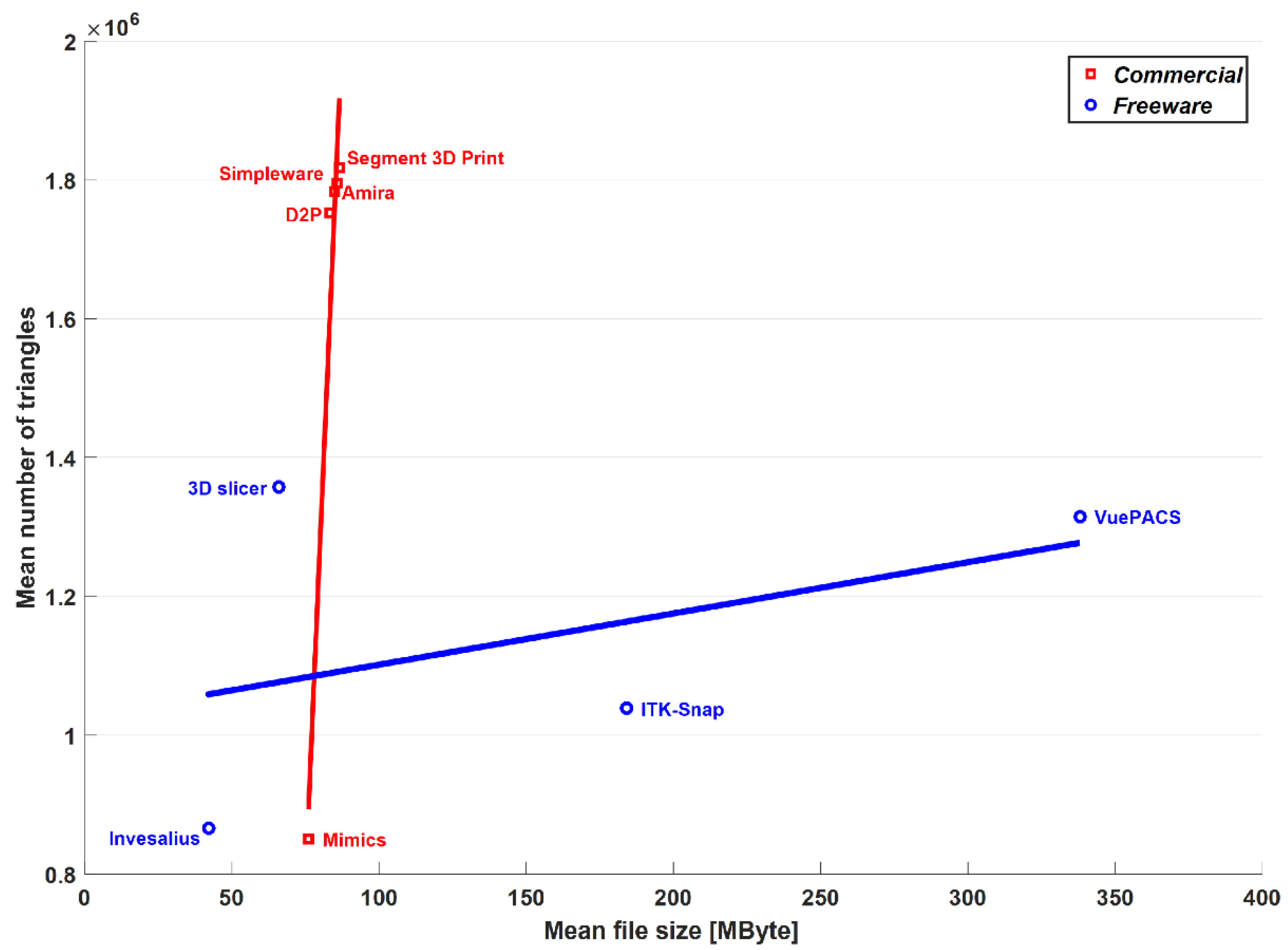
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nolte, D.; Tsang, C.K.; Zhang, K.Y.; Ding, Z.; Kedgley, A.E.; Bull, A.M.J. Non-linear scaling of a musculoskeletal model of the lower limb using statistical shape models. J. Biomech. 2016, 49, 3576–3581. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Besier, T.F. Accuracy of femur reconstruction from sparse geometric data using a statistical shape model. Comput. Methods Biomech. Biomed. Eng. 2017, 20, 566–576. [Google Scholar] [CrossRef] [PubMed]
- Nardini, F.; Belvedere, C.; Sancisi, N.; Conconi, M.; Leardini, A.; Durante, S.; Parenti Castelli, V. An Anatomical-Based Subject-Specific Model of In-Vivo Knee Joint 3D Kinematics From Medical Imaging. Appl. Sci. 2020, 10, 2100. [Google Scholar] [CrossRef] [Green Version]
- Osti, F.; Santi, G.M.; Neri, M.; Liverani, A.; Frizziero, L.; Stilli, S.; Maredi, E.; Zarantonello, P.; Gallone, G.; Stallone, S.; et al. CT Conversion Workflow for Intraoperative Usage of Bony Models: From DICOM Data to 3D Printed Models. Appl. Sci. 2019, 9, 708. [Google Scholar] [CrossRef] [Green Version]
- Belvedere, C.; Siegler, S.; Fortunato, A.; Caravaggi, P.; Liverani, E.; Durante, S.; Ensini, A.; Konow, T.; Leardini, A. New comprehensive procedure for custom-made total ankle replacements: Medical imaging, joint modeling, prosthesis design, and 3D printing. J. Orthop. Res. 2019, 37, 760–768. [Google Scholar] [CrossRef]
- Xia, R.Z.; Zhai, Z.J.; Chang, Y.Y.; Li, H.W. Clinical Applications of 3-Dimensional Printing Technology in Hip Joint. Orthop. Surg. 2019, 11, 533–544. [Google Scholar] [CrossRef] [Green Version]
- Galvez, M.; Asahi, T.; Baar, A.; Carcuro, G.; Cuchacovich, N.; Fuentes, J.A.; Mardones, R.; Montoya, C.E.; Negrin, R.; Otayza, F.; et al. Use of Three-dimensional Printing in Orthopaedic Surgical Planning. J. Am. Acad. Orthop. Surg. Glob. Res. Rev. 2018, 2, e071. [Google Scholar] [CrossRef]
- Parthasarathy, J. 3D modeling, custom implants and its future perspectives in craniofacial surgery. Ann. Maxillofac. Surg. 2014, 4, 9–18. [Google Scholar] [CrossRef] [Green Version]
- Malik, H.H.; Darwood, A.R.; Shaunak, S.; Kulatilake, P.; El-Hilly, A.A.; Mulki, O.; Baskaradas, A. Three-dimensional printing in surgery: A review of current surgical applications. J. Surg. Res. 2015, 199, 512–522. [Google Scholar] [CrossRef]
- Martelli, N.; Serrano, C.; van den Brink, H.; Pineau, J.; Prognon, P.; Borget, I.; El Batti, S. Advantages and disadvantages of 3-dimensional printing in surgery: A systematic review. Surgery 2016, 159, 1485–1500. [Google Scholar] [CrossRef]
- Auricchio, F.; Marconi, S. 3D printing: Clinical applications in orthopaedics and traumatology. EFORT Open Rev. 2016, 1, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Belvedere, C.; Cadossi, M.; Mazzotti, A.; Giannini, S.; Leardini, A. Fluoroscopic and Gait Analyses for the Functional Performance of a Custom-Made Total Talonavicular Replacement. J. Foot Ankle Surg. 2017, 56, 836–844. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, S.; Badiali, G.; Cercenelli, L.; Bortolani, B.; Marcelli, E.; Cipriani, R.; Contedini, F.; Marchetti, C.; Tarsitano, A. Combination of CAD/CAM and Augmented Reality in Free Fibula Bone Harvest. Plast. Reconstr. Surg. Glob. Open 2019, 7, e2510. [Google Scholar] [CrossRef] [PubMed]
- Bahraminasab, M. Challenges on optimization of 3D-printed bone scaffolds. Biomed. Eng. Online 2020, 19, 69. [Google Scholar] [CrossRef]
- Van Eijnatten, M.; van Dijk, R.; Dobbe, J.; Streekstra, G.; Koivisto, J.; Wolff, J. CT image segmentation methods for bone used in medical additive manufacturing. Med. Eng. Phys. 2018, 51, 6–16. [Google Scholar] [CrossRef]
- King, A.I. A review of biomechanical models. J. Biomech. Eng. 1984, 106, 97–104. [Google Scholar] [CrossRef]
- Leardini, A.; Belvedere, C.; Nardini, F.; Sancisi, N.; Conconi, M.; Parenti-Castelli, V. Kinematic models of lower limb joints for musculo-skeletal modelling and optimization in gait analysis. J. Biomech. 2017, 62, 77–86. [Google Scholar] [CrossRef]
- Galbusera, F.; Cina, A.; Panico, M.; Albano, D.; Messina, C. Image-based biomechanical models of the musculoskeletal system. Eur. Radiol. Exp. 2020, 4, 49. [Google Scholar] [CrossRef]
- An, G.; Hong, L.; Zhou, X.B.; Yang, Q.; Li, M.Q.; Tang, X.Y. Accuracy and efficiency of computer-aided anatomical analysis using 3D visualization software based on semi-automated and automated segmentations. Ann. Anat. 2017, 210, 76–83. [Google Scholar] [CrossRef]
- Bucking, T.M.; Hill, E.R.; Robertson, J.L.; Maneas, E.; Plumb, A.A.; Nikitichev, D.I. From medical imaging data to 3D printed anatomical models. PLoS ONE 2017, 12, e0178540. [Google Scholar] [CrossRef] [Green Version]
- Durastanti, G.; Leardini, A.; Siegler, S.; Durante, S.; Bazzocchi, A.; Belvedere, C. Comparison of cartilage and bone morphological models of the ankle joint derived from different medical imaging technologies. Quant. Imaging Med. Surg. 2019, 9, 1368–1382. [Google Scholar] [CrossRef] [PubMed]
- Kresanova, Z.; Kostolny, J. Comparison of Software for Medical Segmentation. Cent. Eur. Res. J. 2018, 4, 66–80. [Google Scholar]
- Tan, C.J.; Parr, W.C.H.; Walsh, W.R.; Makara, M.; Johnson, K.A. Influence of Scan Resolution, Thresholding, and Reconstruction Algorithm on Computed Tomography-Based Kinematic Measurements. J. Biomech. Eng. 2017, 139, 104503. [Google Scholar] [CrossRef] [PubMed]
- Huotilainen, E.; Jaanimets, R.; Valasek, J.; Marcian, P.; Salmi, M.; Tuomi, J.; Makitie, A.; Wolff, J. Inaccuracies in additive manufactured medical skull models caused by the DICOM to STL conversion process. J. Craniomaxillofac. Surg. 2014, 42, e259–e265. [Google Scholar] [CrossRef]
- Matsiushevich, K.; Belvedere, C.; Leardini, A.; Durante, S. Quantitative comparison of freeware software for bone mesh from DICOM files. J. Biomech. 2019, 84, 247–251. [Google Scholar] [CrossRef]
- Lee, L.; Liew, S. A survey of medical image processing tools. In Proceedings of the 4th International Conference on Software Engineering and Computer Systems (ICSECS), Kuantan, Malaysia, 27–29 June 2011; pp. 171–176. [Google Scholar]
- Argüello, D.; Sánchez Acevedo, H.G.; González-Estrada, O.A. Comparison of segmentation tools for structural analysis of bone tissues by finite elements. J. Phys. 2019, 1386, 012113. [Google Scholar] [CrossRef]
- Virzi, A.; Muller, C.O.; Marret, J.B.; Mille, E.; Berteloot, L.; Grevent, D.; Boddaert, N.; Gori, P.; Sarnacki, S.; Bloch, I. Comprehensive Review of 3D Segmentation Software Tools for MRI Usable for Pelvic Surgery Planning. J. Digit. Imaging 2020, 33, 99–110. [Google Scholar] [CrossRef]
- Fourie, Z.; Damstra, J.; Schepers, R.H.; Gerrits, P.O.; Ren, Y. Segmentation process significantly influences the accuracy of 3D surface models derived from cone beam computed tomography. Eur. J. Radiol. 2012, 81, e524–e530. [Google Scholar] [CrossRef]
- Kamio, T.; Suzuki, M.; Asaumi, R.; Kawai, T. DICOM segmentation and STL creation for 3D printing: A process and software package comparison for osseous anatomy. 3D Print Med. 2020, 6, 17. [Google Scholar] [CrossRef]
- Ahn, C.; Bui, T.D.; Lee, Y.W.; Shin, J.; Park, H. Fully automated, level set-based segmentation for knee MRIs using an adaptive force function and template: Data from the osteoarthritis initiative. Biomed. Eng. Online 2016, 15, 99. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Jian, F.; Wu, H.; Li, H. An improved level set method for vertebra CT image segmentation. Biomed. Eng. Online 2013, 12, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sander, I.M.; McGoldrick, M.T.; Helms, M.N.; Betts, A.; van Avermaete, A.; Owers, E.; Doney, E.; Liepert, T.; Niebur, G.; Liepert, D.; et al. Three-dimensional printing of X-ray computed tomography datasets with multiple materials using open-source data processing. Anat. Sci. Educ. 2017, 10, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Becker, K.; Lipprandt, M.; Röhrig, R.; Neumuth, T. Digital health—Software as a medical device in focus of the medical device regulation (MDR). IT Inf. Technol. 2019, 61, 211–218. [Google Scholar] [CrossRef]
- Wallner, J.; Schwaiger, M.; Hochegger, K.; Gsaxner, C.; Zemann, W.; Egger, J. A review on multiplatform evaluations of semi-automatic open-source based image segmentation for cranio-maxillofacial surgery. Comput. Methods Programs Biomed. 2019, 182, 105102. [Google Scholar] [CrossRef]
- Soodmand, E.; Kluess, D.; Varady, P.A.; Cichon, R.; Schwarze, M.; Gehweiler, D.; Niemeyer, F.; Pahr, D.; Woiczinski, M. Interlaboratory comparison of femur surface reconstruction from CT data compared to reference optical 3D scan. Biomed. Eng. Online 2018, 17, 29. [Google Scholar] [CrossRef] [Green Version]
- Ortolani, M.; Leardini, A.; Pavani, C.; Scicolone, S.; Girolami, M.; Bevoni, R.; Lullini, G.; Durante, S.; Berti, L.; Belvedere, C. Angular and linear measurements of adult flexible flatfoot via weight-bearing CT scans and 3D bone reconstruction tools. Sci. Rep. 2021, 11, 16139. [Google Scholar] [CrossRef]
- De Carvalho, K.A.M.; Walt, J.S.; Ehret, A.; Tazegul, T.E.; Dibbern, K.; Mansur, N.S.B.; Lalevee, M.; de Cesar Netto, C. Comparison between Weightbearing-CT semiautomatic and manual measurements in Hallux Valgus. Foot Ankle Surg. 2022, 28, 518–525. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Mimics (v. 24.0) | Amira (v. 2019.4) | D2P (v. 1.0.2.2055) | Simpleware (v. 2021.06) | Segment 3D Print (v. 3.3 R 9056) | |
|---|---|---|---|---|---|
| Recommended Processor | Intel Core i7 or equivalent | Intel64/AMD64 architecture | Intel Core i7 | Intel Core i7 or equivalent | Any processor supporting CUDA-enabled graphics |
| Minimum RAM [GB] | 4 | 2 | 16 | 16 | 16 |
| Minimum HDD space [GB] | 5 | Not reported * | 500 | 100 | 5 |
| Supported Operating System | Windows 10 Pro/Enterprise version 1803, 1809, 1903, 1909, 2009 (64-bit) or Windows Server 2019 Standard version 10.0, | Windows 7/8/10 (64-bit) Linux x86_64 (64-bit): CentOS 7 Mac OS X High Sierra (10.13) and Mac OS X Mojave (10.14) | Windows 7 or 10 (64 bit) | Windows 10/Windows Server 2016 Linux *:
| Windows 10 (64 bit) |
| Mimics (v.24.0) | Amira (v. 2019.4) | D2P (v. 1.0.2.2055) | Simpleware (v. 2021.06) | Segment 3D Print (v3.3 R 9056) | |
|---|---|---|---|---|---|
| Time to import [s] | 1.4 ± 0.5 (1–2) | 2.4 ± 1.5 (1–5) | 2.1 ± 0.3 (2–3) | 2.5 ± 0.7 (1–4) | 3.7 ± 1.1 (2–6) |
| Time to create the model [s] | 5.8 ± 3.9 (2–14) | 2.1 ± 0.4 (2–3) | 11.1 ± 4.3 (4–19) | 5.2 ± 2.4 (3–10) | 23.9 ± 13.3 (9–55) |
| Number of triangles | 849,995 ± 633,670 (203,616–2,219,446) | 1,782,831.6 ± 1,145,476 (532,574–3,843,000) | 1,752,240 ± 1,120,912 (526,460–3,764,380) | 1,796,269 ± 1,132,502 (568,436–3,834,908) | 1,816,860 ± 1,107,694 (576,532–4,200,338) |
| File size [megabytes] | 76.0 ± 48.8 (23.9–163) | 84.8 ± 54.5 (25.3–183) | 83.4 ± 53.3 (25.1–179) | 85.5 ± 53.9 (27.1–182) | 86.5 ± 52.7 (27.4–200) |
| Number of triangles per MByte | 10,433.4 ± 2111.5 (6650–13616) | 21,019.2 ± 51.2 (20,973–21,165) | 21,004.8 ± 32.0 (20,971–21,077) | 21,003.1 ± 48.2 (20,889–21,088) | 21,005.5 ± 31.1 (20,972–21,079) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belvedere, C.; Ortolani, M.; Marcelli, E.; Bortolani, B.; Matsiushevich, K.; Durante, S.; Cercenelli, L.; Leardini, A. Comparison of Bone Segmentation Software over Different Anatomical Parts. Appl. Sci. 2022, 12, 6097. https://doi.org/10.3390/app12126097
Belvedere C, Ortolani M, Marcelli E, Bortolani B, Matsiushevich K, Durante S, Cercenelli L, Leardini A. Comparison of Bone Segmentation Software over Different Anatomical Parts. Applied Sciences. 2022; 12(12):6097. https://doi.org/10.3390/app12126097
Chicago/Turabian StyleBelvedere, Claudio, Maurizio Ortolani, Emanuela Marcelli, Barbara Bortolani, Katsiaryna Matsiushevich, Stefano Durante, Laura Cercenelli, and Alberto Leardini. 2022. "Comparison of Bone Segmentation Software over Different Anatomical Parts" Applied Sciences 12, no. 12: 6097. https://doi.org/10.3390/app12126097
APA StyleBelvedere, C., Ortolani, M., Marcelli, E., Bortolani, B., Matsiushevich, K., Durante, S., Cercenelli, L., & Leardini, A. (2022). Comparison of Bone Segmentation Software over Different Anatomical Parts. Applied Sciences, 12(12), 6097. https://doi.org/10.3390/app12126097