
Quality Evaluation Algorithm for Chest Compressions Based on OpenPose Model


Abstract
:1. Introduction
2. System Architecture
2.1. Design
2.2. Research
2.3. Key Motion Feature Assessment
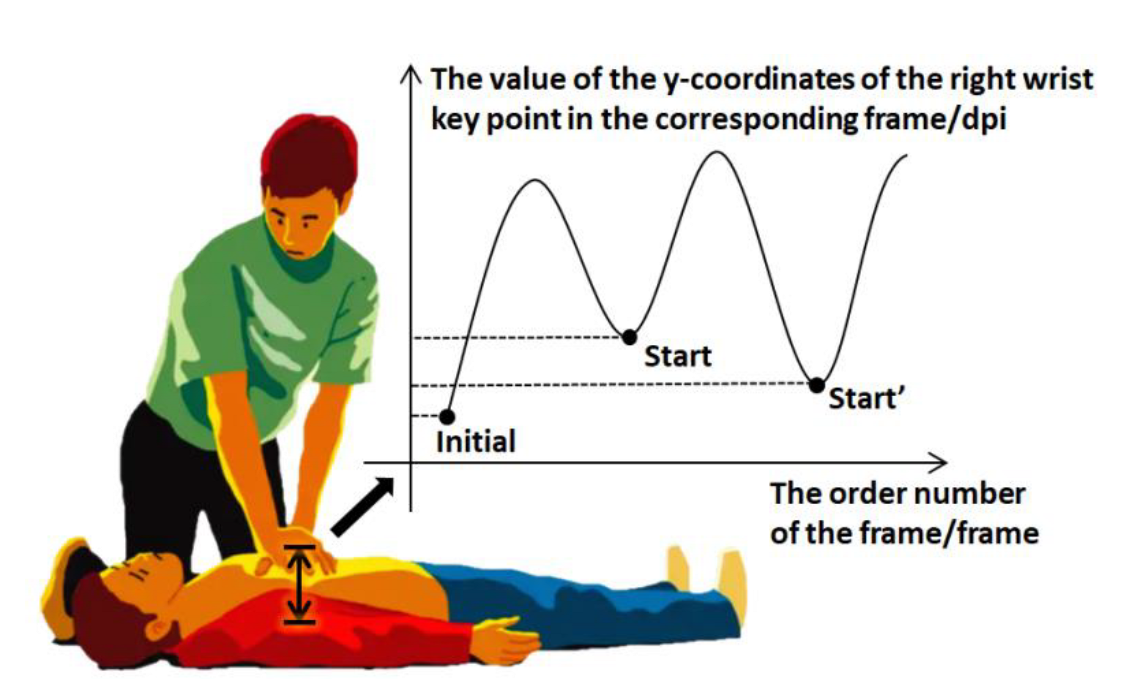
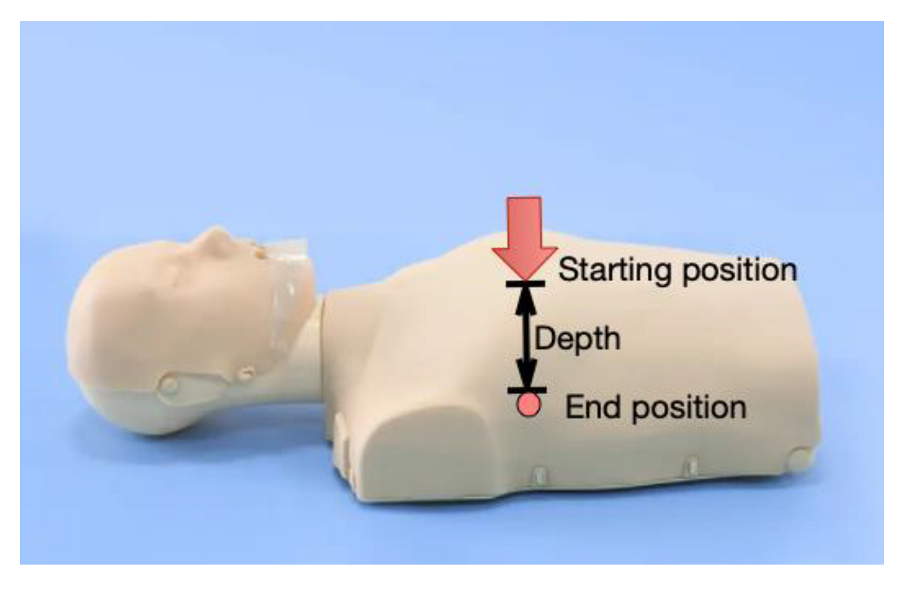
2.3.1. Depth of Compression
2.3.2. Chest Rebound
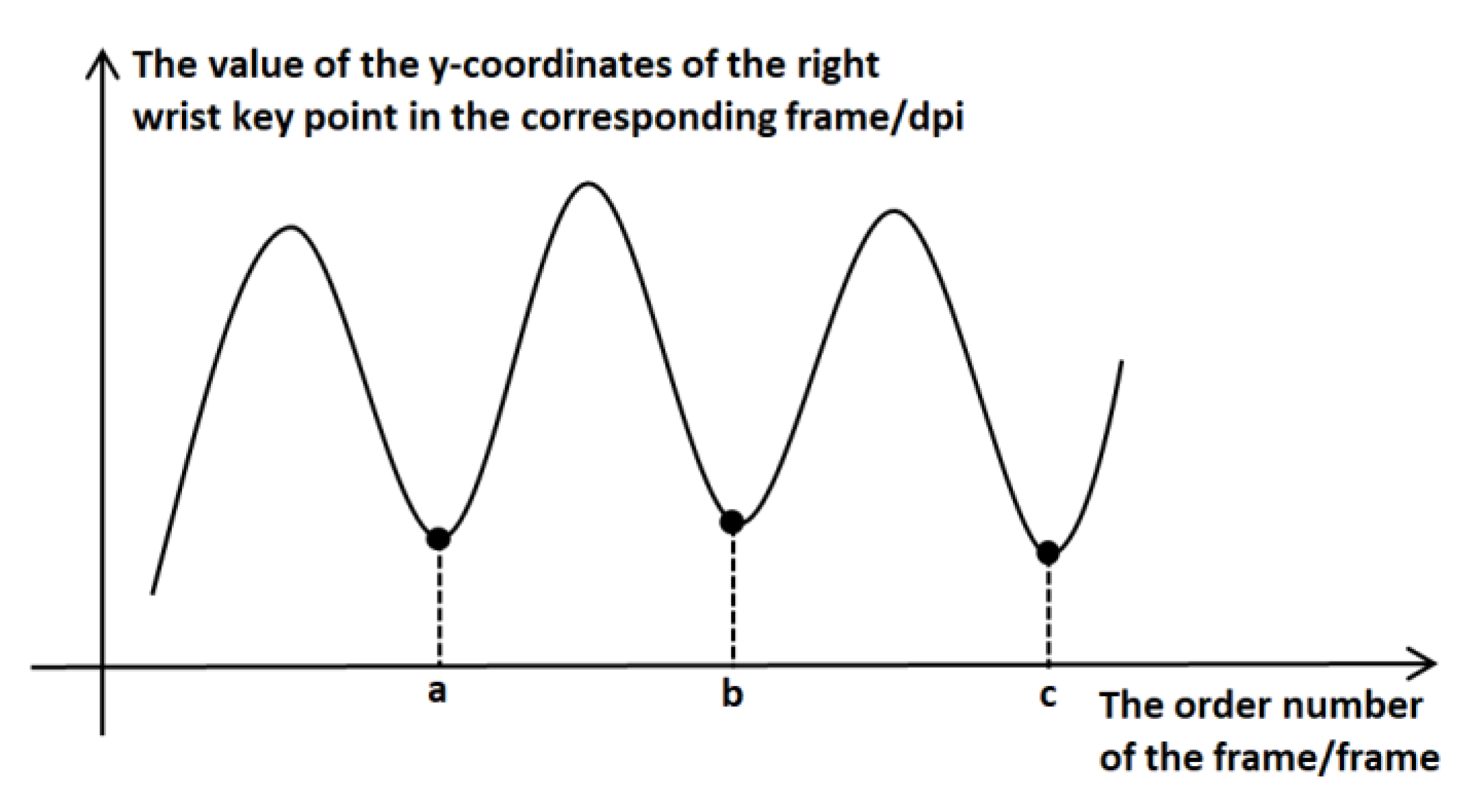
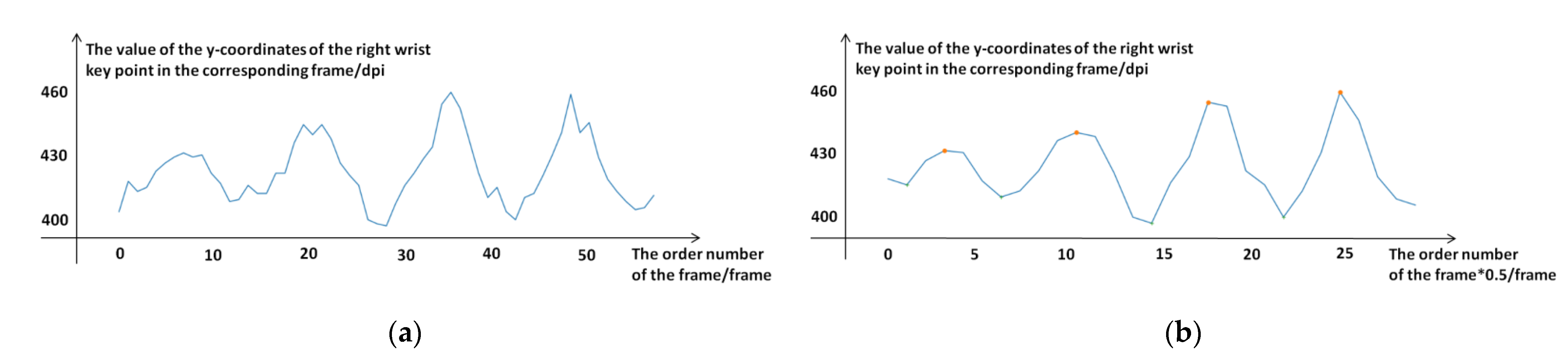
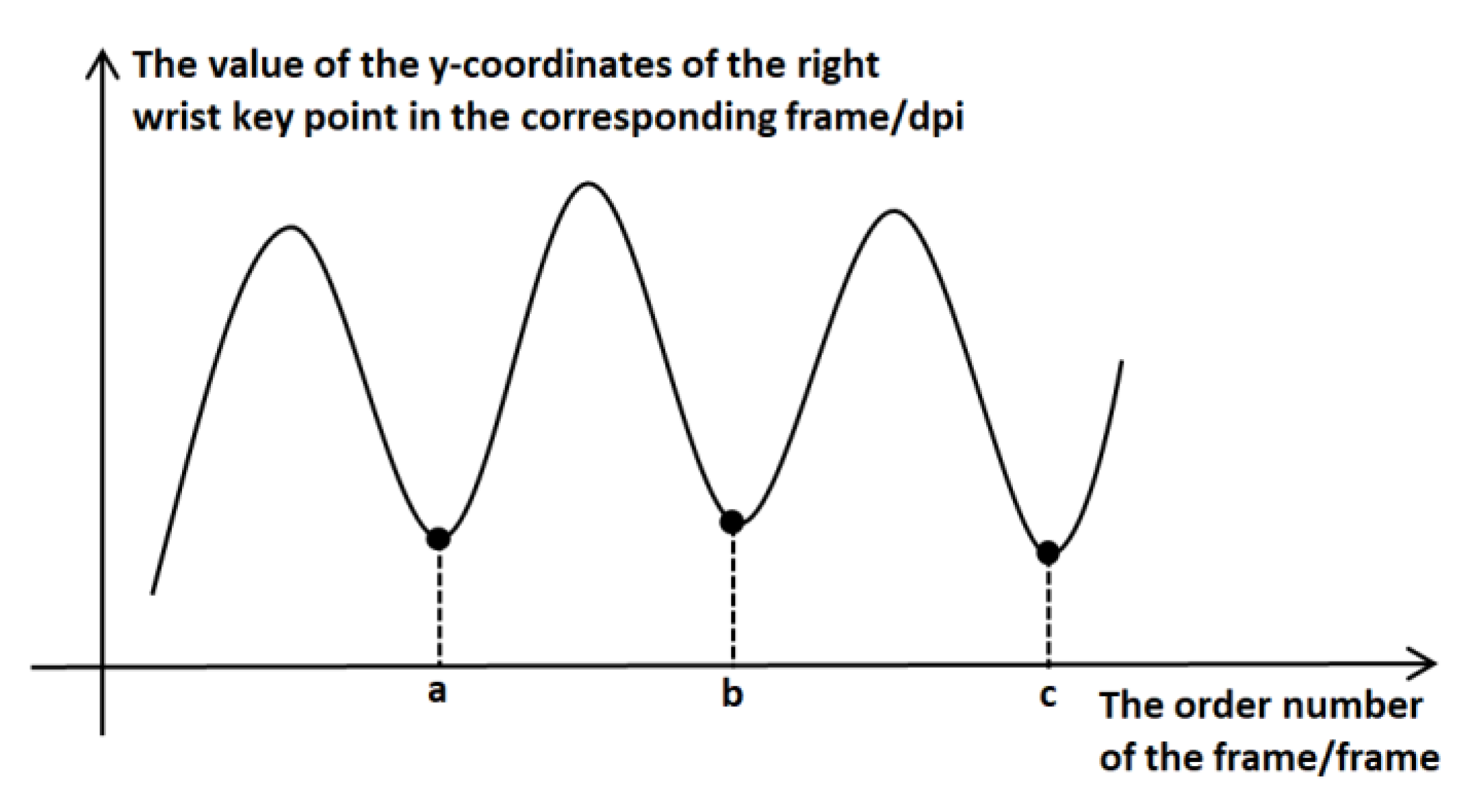
2.3.3. Frequency of Compression
2.3.4. Position of Compression
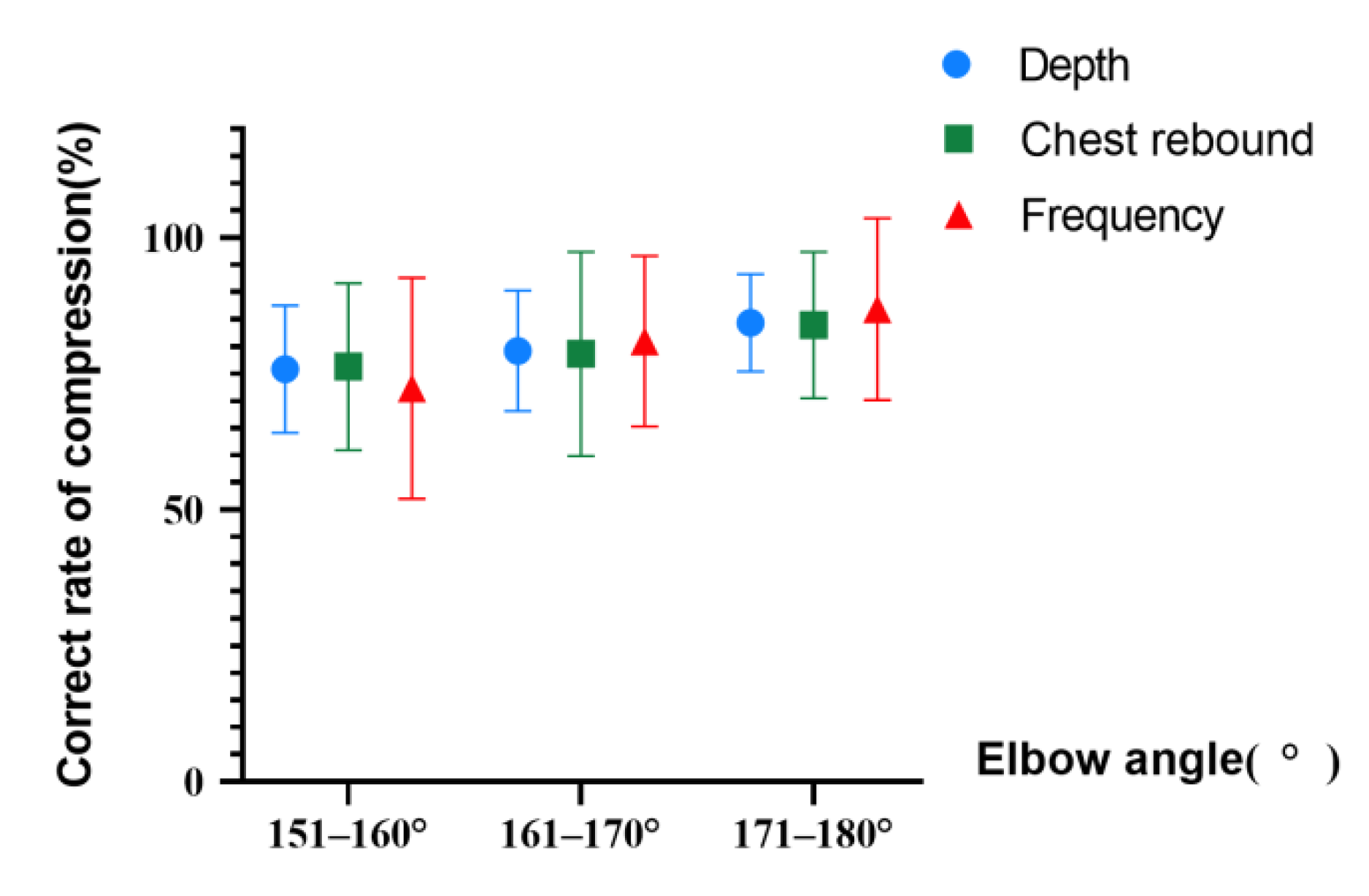
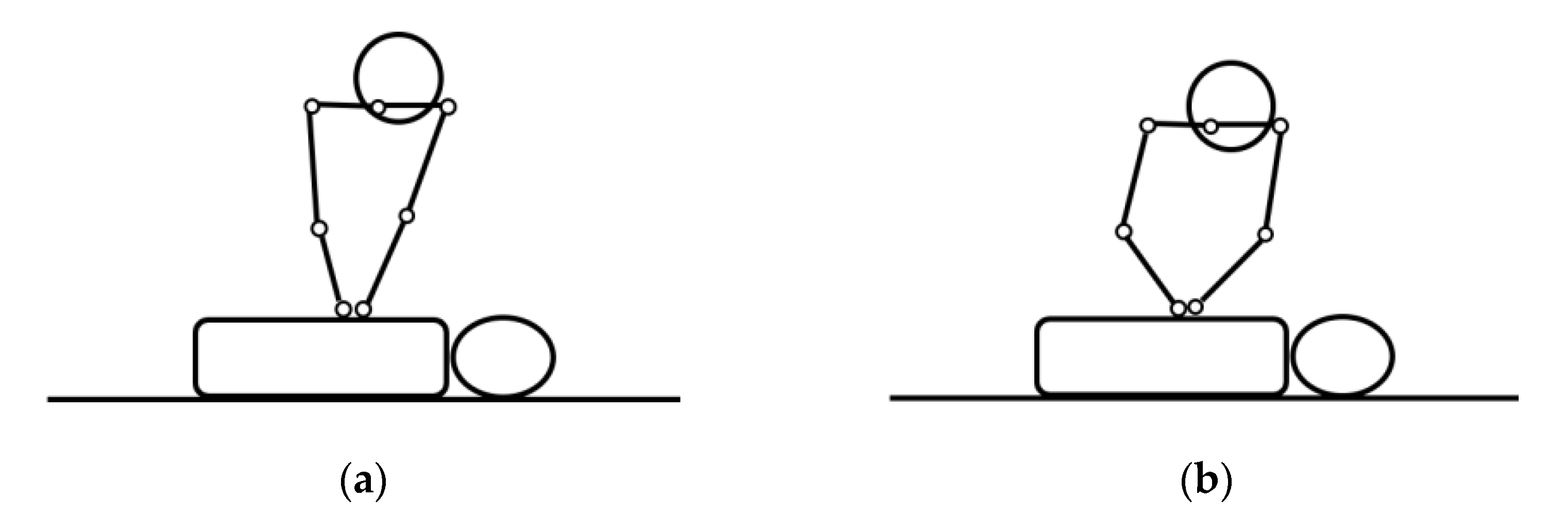
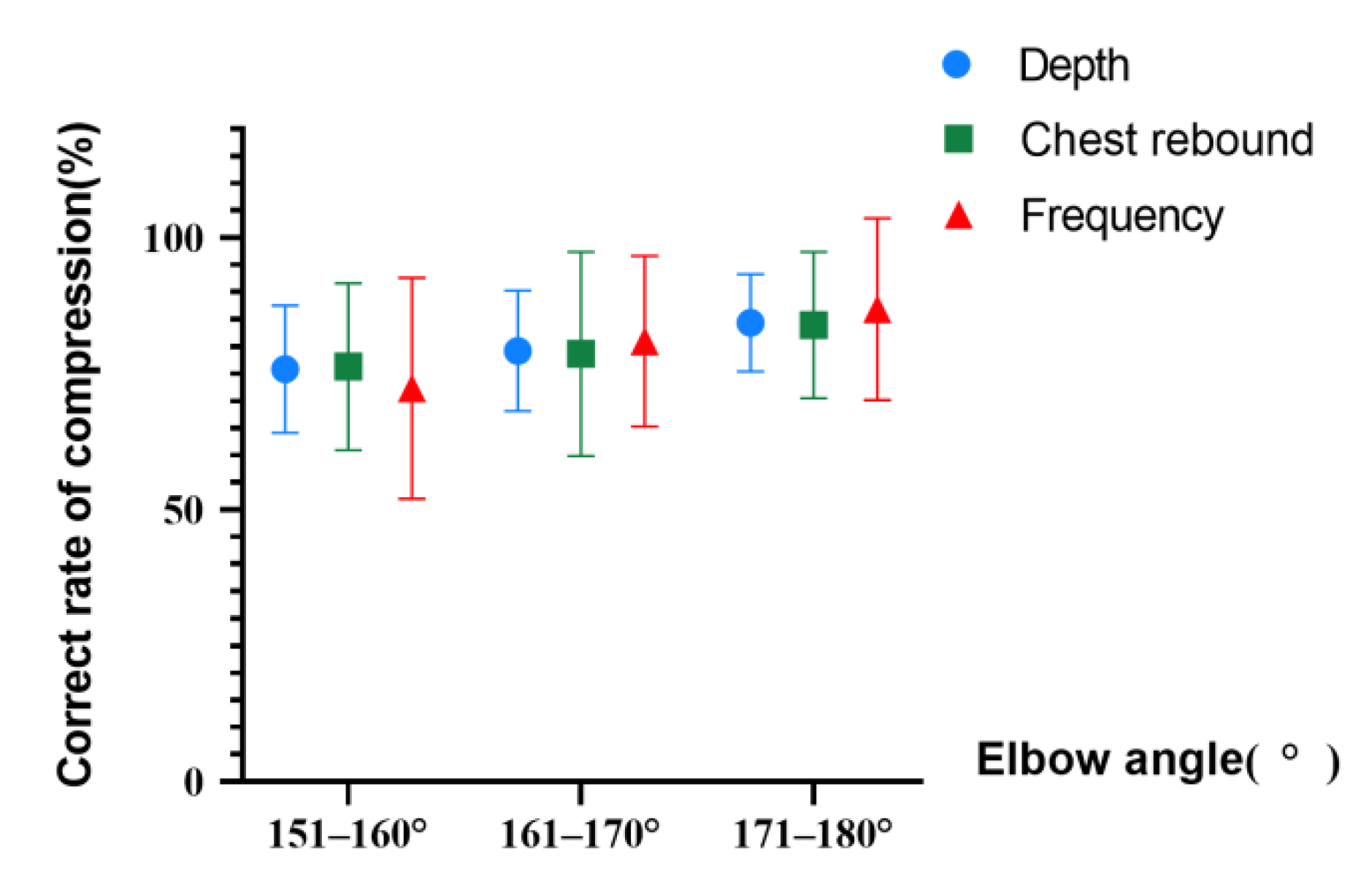
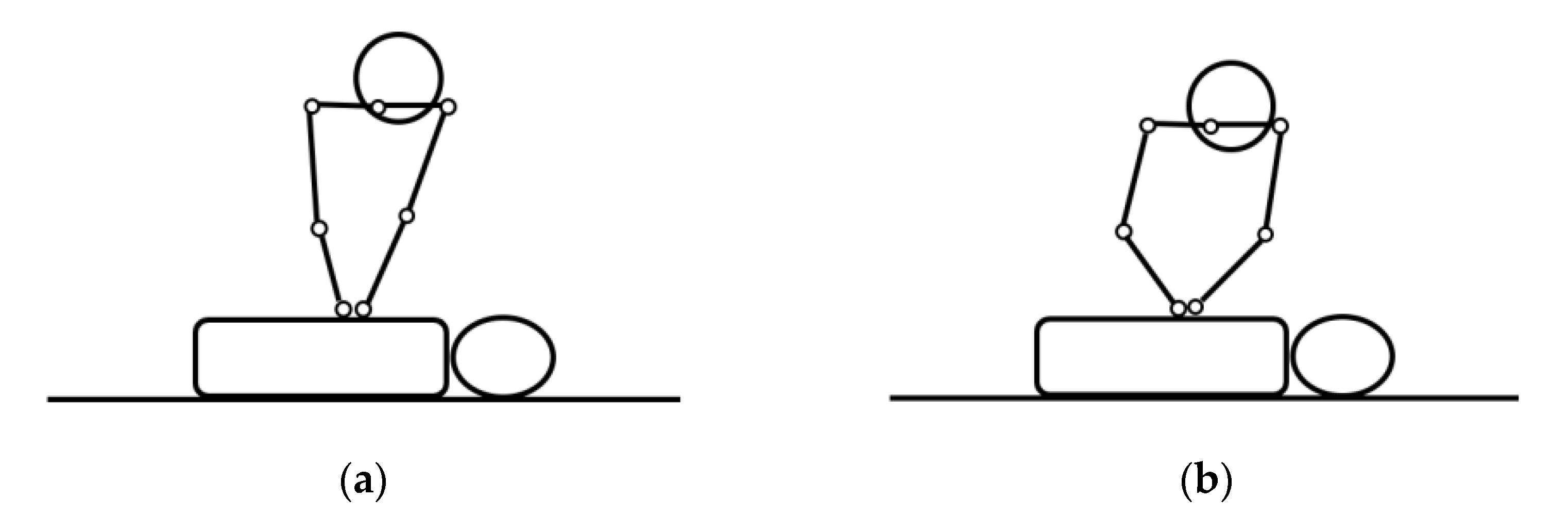
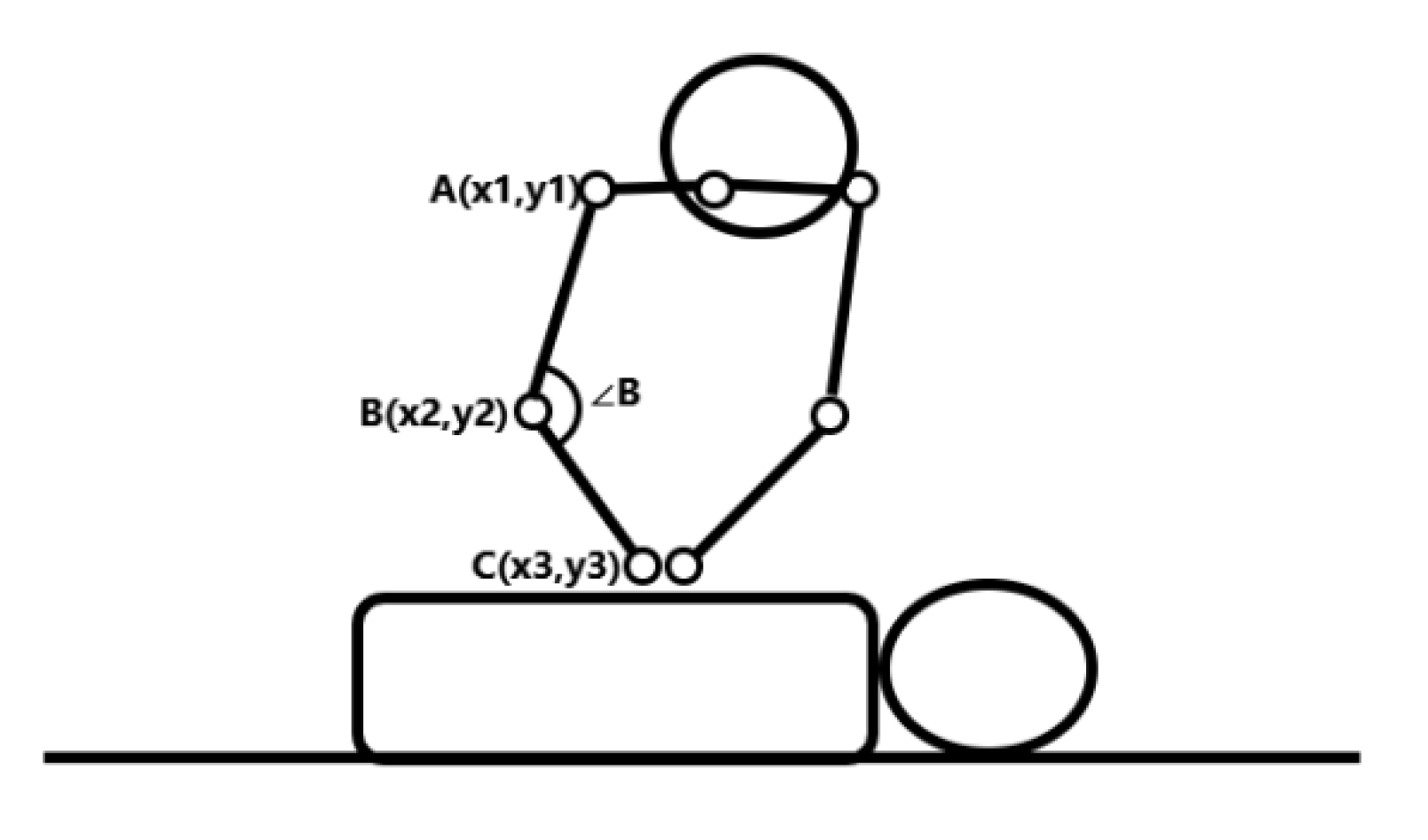
2.3.5. Elbow Angles
3. Results and Analysis
3.1. Experimental Environment and Methods
3.2. Results and Analysis
4. Conclusions
- In addition to detecting the general indicators of compression, we propose automated discrimination of operator posture for the first time.
- Our algorithm is not affected by the surrounding environment. It uses a typical monocular RGB camera as a sensor to collect data, which has better applicability than a depth camera and has a lower cost.
- The performance of our algorithm is 94.58%, 71.57%, 94.00%, and 81.27% in accuracy, precision, recall and F-measure, respectively.
- The application of the HPE method in CPR assessment can not only reduce the problem of incorrect scores caused by an instructor’s lack of energy, but it can also allow trainees to understand their own mistakes in private practice to better master CPR techniques.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhang, S.; Hou, S.; Fan, H. Research Status of Intelligent Cardiopulmonary Resuscitation Equipment. Chin. Med. Equip. J. 2021, 42, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Neumar, R.W.; Shuster, M.; Callaway, C.W.; Gent, L.M.; Atkins, D.L.; Bhanji, F.; Brooks, S.C.; de Caen, A.R.; Donnino, M.W.; Ferrer, J.M. Part1: Executive summary: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2015, 132 (Suppl. 2), S315–S367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, J.; Dong, W.; Fan, H.; Fan, B. Status of researches on CPR manikins. Chin. Med. Equip. J. 2021, 42, 80–84. [Google Scholar]
- Alexandra, M.M.; Ryan, M.W.; Catherine, E.R.; Robert, A.B.; Robert, M.S. Physiology directed cardiopulmonary resuscitation:advances in precision monitoring during cardiac arrest. Curr. Opin. Crit. Care 2018, 24, 143–150. [Google Scholar]
- Ray, F.; Mary, P.C.; Ahamed, H.I. Evolution and revolution in cardiopulmonary resuscitation. Curr. Opin. Crit. Care 2017, 23, 183–187. [Google Scholar]
- Christopher, N.; Scott, G.; Jasmeet, S. Airway and ventilation management during cardiopulmonary resuscitation and after successful resuscitation. Crit. Care 2018, 22, 190. [Google Scholar]
- Ian, G.S.; Siobhan, P.B.; James, C.; Sheldon, C.; Graham, N.; Judy, P.; Blair, B.; Laurie, J.M.; Jonathan, L.; Erik, H.; et al. What is the role of chest compression depth during out-of-hospital cardiac arrest resuscitation. Crit. Care Med. 2012, 40, 1192–1198. [Google Scholar]
- Liu, Y.; Li, J.; Zhang, J.; Xu, Z. Research progress of two-dimensional human pose estimation based on deep learning. Comput. Eng. 2021, 47, 1–16. [Google Scholar]
- Cao, Z.; Simon, T.; Wei, S.; Sheikh, Y. Realtime Multi-person 2D Pose Estimation Using Part Affinity Fields. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 1302–1310. [Google Scholar]
- Panchal, A.R.; Bartos, J.A.; Cabaas, J.G.; Donnino, M.W.; Berg, K.M. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020, 142 (Suppl. 2), S366–S468. [Google Scholar] [CrossRef] [PubMed]
- Olasveengen, T.M.; Semeraro, F.; Ristagno, G.; Castren, M.; Handley, A.; Kuzovlev, A.; Monsieurs, K.G.; Raffay, V.; Smyth, M.; Soar, J.; et al. European Resuscitation Council Guidelines 2021: Basic Life Support. Resuscitation 2021, 161, 98–114. [Google Scholar] [CrossRef] [PubMed]
- Glikson, M.; Nielsen, J.C.; Kronborg, M.B. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: Developed by the Task Force on cardiac pacing and cardiac resynchronization therapy of the European Society of Cardiology (ESC) with the special contribution of the European Heart Rhythm Association (EHRA). Eur. Heart J. 2022, 42, 3427–3520. [Google Scholar]
- Richardson, A.S.C.; Tonna, J.E.; Nanjayya, V. Extracorporeal Cardiopulmonary Resuscitation in Adults. Interim Guideline Consensus Statement from the Extracorporeal Life Support Organization. ASAIO J. 2021, 67, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Ni, H.; Cao, S. Research and Implementation of Asynchronous Video Converter based on Linux. Appl. Mech. Mater. 2013, 241–244, 2596–2600. [Google Scholar] [CrossRef]
- Hong, G.; Shanchen, Z.; Yilin, X. DanceVis: Toward better understanding of online cheer and dance training. J. Vis. 2021, 25, 158–174. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Park, H.; Baek, J.; Kim, J. Imagery based Parametric Classification of Correct and Incorrect Motion for Push-up Counter Using OpenPose. In Proceedings of the IEEE International Conference on Automation Science and Engineering (CASE), Hong Kong, China, 20–21 August 2020; pp. 1389–1394. [Google Scholar]
- Siao, F.; Chiu, C.; Chiu, C. Managing cardiac arrest with refractory ventricular fibrillation in the emergency department: Conventional cardiopulmonary resuscitation versus extracorporeal cardiopulmonary resuscitation. Resuscitation 2015, 92, 70–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Georgiou, M.; Papathanassoglou, E.; Xanthos, T. Systematic review of the mechanisms driving effective blood flow during adult CPR. Resuscitation 2014, 5, 1586–1593. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Ruiz, M.; Silva, J.T.; San-Juan, R.; Dios, B.D.; García-Luján, R.; López-Medrano, F.; Lizasoain, M.; Aguado, J.M. Aspergillus tracheobronchitis: Report of 8 cases and review of the literature. Med. Baltim. 2012, 91, 261–273. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Observation Indicators | 151–160° | 161–170° | 171–180° | p |
|---|---|---|---|---|
| Average depth (mm) | 50.62 ± 5.16 | 52.48 ± 5.39 | 53.79 ± 5.54 | >0.05 |
| Average frequency (times/min) | 99 | 106 | 117 | <0.05 |
| Correct rate of depth (%) | 75.82 ± 11.68 | 79.21 ± 11.10 | 84.35 ± 8.97 | <0.05 |
| Full rebound rate (%) | 76.32 ± 15.32 | 78.64 ± 18.73 | 83.96 ± 13.47 | <0.05 |
| Correct rate of frequency (%) | 72.32 ± 20.32 | 80.96 ± 15.67 | 86.89 ± 16.73 | <0.05 |
| Correct rate of compression position (%) | 100 ± 0.00 | 100 ± 0.00 | 100 ± 0.00 | >0.05 |
| Indicators | Desired Value Range | Sub-Requirement | Overall Requirement |
|---|---|---|---|
| Operating position | The midpoint of the connection between the two nipples | The correct rate is more than 70% | Every indicator should be qualified |
| Elbow straightness | 171–180° | The correct rate of the left and right elbows should both reach more than 70% | |
| Frequency | 100–120 times/min | The correct rate is more than 70% | |
| Depth | 5–6 cm | ||
| Chest rebound | Must be fully rebound |
| Action Type | The Number of Successes per Person in 30 Trials | The Success Rate/% | ||||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | ||
| Correct | 29 | 27 | 28 | 29 | 28 | 94.00% |
| Elbow-flexing | 28 | 30 | 28 | 28 | 28 | 94.67% |
| Too deep | 27 | 28 | 27 | 29 | 29 | 93.33% |
| Too shallow | 30 | 28 | 29 | 29 | 30 | 97.33% |
| Too fast | 28 | 27 | 28 | 28 | 27 | 92.00% |
| Too slow | 29 | 30 | 30 | 29 | 30 | 98.67% |
| Insufficient chest rebound | 30 | 29 | 28 | 28 | 29 | 96.00% |
| Wrong operating position | 26 | 28 | 27 | 28 | 27 | 90.67% |
| Parameter | Value | Parameter | Value |
|---|---|---|---|
| TP | 0.118 | Accuracy | 94.58% |
| FP | 0.047 | Precision | 71.57% |
| FN | 0.008 | Recall | 94.00% |
| TN | 0.828 | F-measure | 81.27% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, S.; Jin, J.; Wang, C.; Dong, W.; Fan, B. Quality Evaluation Algorithm for Chest Compressions Based on OpenPose Model. Appl. Sci. 2022, 12, 4847. https://doi.org/10.3390/app12104847
Zhang S, Jin J, Wang C, Dong W, Fan B. Quality Evaluation Algorithm for Chest Compressions Based on OpenPose Model. Applied Sciences. 2022; 12(10):4847. https://doi.org/10.3390/app12104847
Chicago/Turabian StyleZhang, Siqi, Jie Jin, Chaofang Wang, Wenlong Dong, and Bin Fan. 2022. "Quality Evaluation Algorithm for Chest Compressions Based on OpenPose Model" Applied Sciences 12, no. 10: 4847. https://doi.org/10.3390/app12104847
APA StyleZhang, S., Jin, J., Wang, C., Dong, W., & Fan, B. (2022). Quality Evaluation Algorithm for Chest Compressions Based on OpenPose Model. Applied Sciences, 12(10), 4847. https://doi.org/10.3390/app12104847