
Whole-Body Cryostimulation: A Rehabilitation Booster in Post-COVID Patients? A Case Series

 , ,
, ,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants, Inclusion and Exclusion Criteria
2.2. Whole-Body Cryostimulation Procedure
2.3. Rehabilitation Program
- A personalized nutritional program based on the patient’s nutritional history and the assessment of the resting energy expenditure. The optimal total daily intake and diet composition were defined by a clinical dietitian within the Istituto Auxologico Italiano. All patients were advised to continue the same diet after the discharge.
- Two 60-min daily physiotherapy sessions including personalized progressive aerobic training, postural control, and progressive strengthening exercises supervised by a physiotherapist. Aerobic sessions were monitored with the subjective perception of fatigue (Borg’s CR10 scale), and oxygen saturation (SpO2). Exercises were stopped when a score of 5 on the Borg scale was reached. The first aerobic session performed in the morning after WBC consisted of walking at a self-selected cadence. The second session performed in the afternoon consisted of arm-cranking at an intensity of 65% of HRmax according to the Karvonen equation ((220 − age) × 0.65). This approach was individualized according to the patient’s fitness, clinical status, and subjective perception of fatigue. Joint mobility and body weight strengthening exercises were performed according to the individual fitness level.
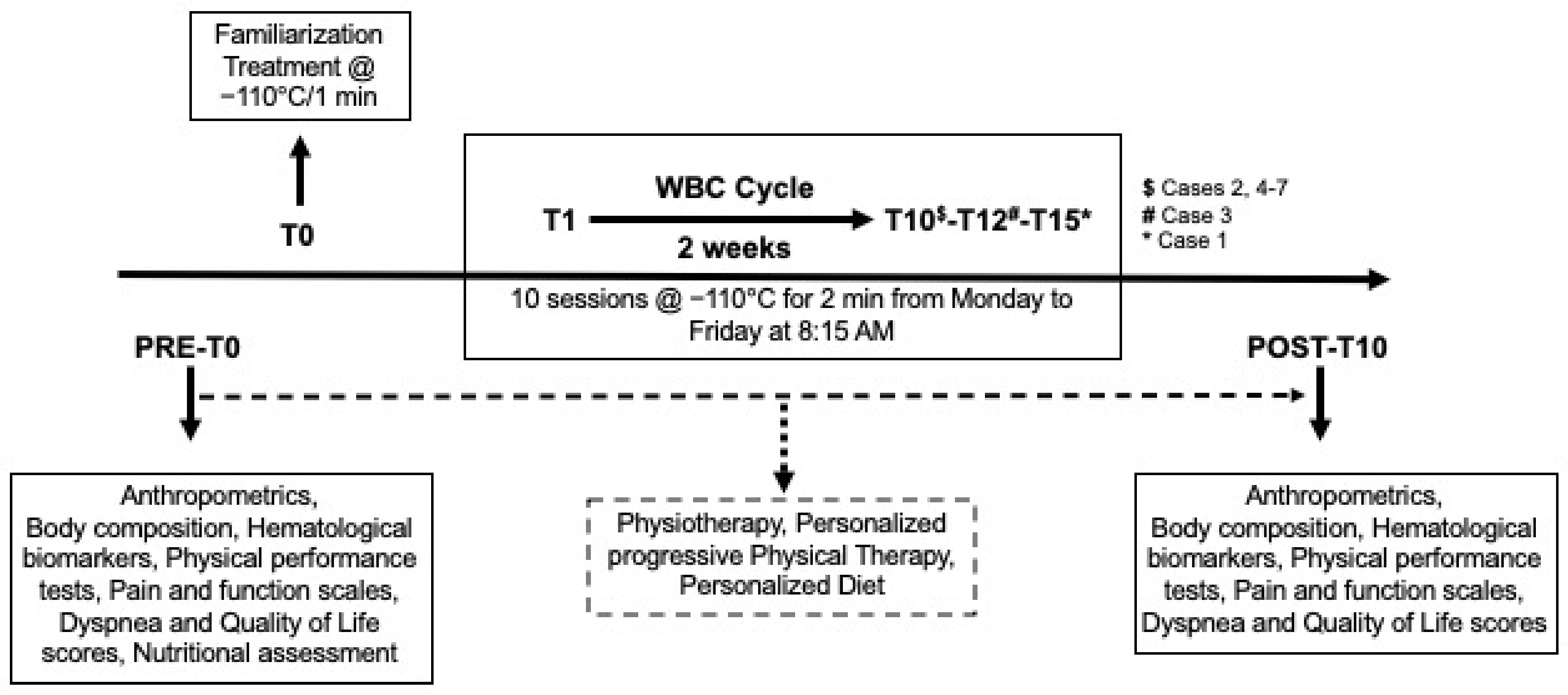
- A WBC cycle (10–15 sessions at −110 °C from Monday to Friday, at 8:15 A.M., before physical exercise classes and physiotherapy) using a cryochamber (Artic, CryoScience, Rome, Italy) (Figure 1). The safety profile of the device for both pulmonary [25] and cardiac function [26] had been previously demonstrated, and no adverse effects were reported under the conditions of use indicated. The first WBC session lasted 1 min at −110 °C to familiarize the patient with the cryochamber temperature, whereas all following treatments lasted 2 min. The patient’s skin surface temperature was measured before and after each treatment with an infrared thermometer (Fluke Corporation, Everett, WA, USA) at the neck, quadriceps, popliteal fossa, and calf level.
2.4. Outcome Measures
3. Case Series
3.1. Case 1
Individual Rehabilitation Program Timeline
3.2. Case 2
Individual Rehabilitation Program Timeline
3.3. Case 3
Individual Rehabilitation Program Timeline
3.4. Case 4
Individual Rehabilitation Program Timeline
3.5. Case 5
Individual Rehabilitation Program Timeline
3.6. Case 6
Individual Rehabilitation Program Timeline
3.7. Case 7
Individual Rehabilitation Program Timeline
4. Summary of Results
5. Discussion
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations and Symbols
Appendix A. Main Contraindications for the WBC Treatment
References
- Bagnato, S.; Boccagni, C.; Marino, G.; Prestandrea, C.; D’Agostino, T.; Rubino, F. Critical Illness Myopathy after COVID-19. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2020, 99, 276–278. [Google Scholar] [CrossRef] [PubMed]
- Gobbi, M.; Bezzoli, E.; Ismelli, F.; Trotti, G.; Cortellezzi, S.; Meneguzzo, F.; Arreghini, M.; Seitanidis, I.; Brunani, A.; Aspesi, V.; et al. Skeletal Muscle Mass, Sarcopenia and Rehabilitation Outcomes in Post-Acute COVID-19 Patients. J. Clin. Med. 2021, 10, 5623. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Coronavirus Disease (COVID-19): Post COVID-19 Condition. Available online: https://www.who.int/news-room/questions-and-answers/item/coronavirus-disease-(covid-19)-post-covid-19-condition (accessed on 5 January 2022).
- Ceban, F.; Ling, S.; Lui, L.M.W.; Lee, Y.; Gill, H.; Teopiz, K.M.; Rodrigues, N.B.; Subramaniapillai, M.; Di Vincenzo, J.D.; Cao, B.; et al. Fatigue and Cognitive Impairment in Post-COVID-19 Syndrome: A Systematic Review and Meta-Analysis. Brain. Behav. Immun. 2021, 101, 93–135. [Google Scholar] [CrossRef] [PubMed]
- Dani, M.; Dirksen, A.; Taraborrelli, P.; Torocastro, M.; Panagopoulos, D.; Sutton, R.; Lim, P.B. Autonomic Dysfunction in ‘Long COVID’: Rationale, Physiology and Management Strategies. Clin. Med. J. R. Coll. Physicians 2021, 21, E63–E67. [Google Scholar] [CrossRef]
- Gupta, A.; Madhavan, M.V.; Sehgal, K.; Nair, N.; Mahajan, S.; Sehrawat, T.S.; Bikdeli, B.; Ahluwalia, N.; Ausiello, J.C.; Wan, E.Y.; et al. Extrapulmonary Manifestations of COVID-19. Nat. Med. 2020, 26, 1017–1032. [Google Scholar] [CrossRef]
- Higgins, V.; Sohaei, D.; Diamandis, E.P.; Prassas, I. COVID-19: From an Acute to Chronic Disease? Potential Long-Term Health Consequences. Crit. Rev. Clin. Lab. Sci. 2021, 58, 297–310. [Google Scholar] [CrossRef]
- Ferioli, M.; Prediletto, I.; Bensai, S.; Betti, S.; Daniele, F.; Di Scioscio, V.; Modolon, C.; Rimondi, M.R.; De Molo, C.; Serra, C.; et al. Spontaneous Evolution of COVID-19 Lung Sequelae: Results from a Double-Step Follow-Up. Respir. Int. Rev. Thorac. Dis. 2022, 101, 381–393. [Google Scholar] [CrossRef]
- Tenforde, M.W.; Kim, S.S.; Lindsell, C.J.; Billig Rose, E.; Shapiro, N.I.; Files, D.C.; Gibbs, K.W.; Erickson, H.L.; Steingrub, J.S.; Smithline, H.A.; et al. Symptom Duration and Risk Factors for Delayed Return to Usual Health Among Outpatients with COVID-19 in a Multistate Health Care Systems Network—United States, March–June 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 993–998. [Google Scholar] [CrossRef]
- Lam MH, B.; Wing, Y.K.; Yu MW, M.; Leung, C.M.; Ma, R.C.; Kong, A.P.; Lam, S.P. Mental morbidities and chronic fatigue in severe acute respiratory syndrome survivors: Long-term follow-up. Arch. Intern. Med. 2009, 169, 2142–2147. [Google Scholar] [CrossRef] [Green Version]
- Lopez, M.; Bell, K.; Annaswamy, T.; Juengst, S.; Ifejika, N. COVID-19 Guide for the Rehabilitation Clinician: A Review of Nonpulmonary Manifestations and Complications. Am. J. Phys. Med. Rehabil. 2020, 99, 669–676. [Google Scholar] [CrossRef]
- Hopkins, C.; Surda, P.; Whitehead, E.; Kumar, B.N. Early Recovery Following New Onset Anosmia during the COVID-19 Pandemic—An Observational Cohort Study. J. Otolaryngol.-Head Neck Surg. 2020, 49, 26. [Google Scholar] [CrossRef]
- Vitacca, M.; Lazzeri, M.; Guffanti, E.; Frigerio, P.; D’Abrosca, F.; Gianola, S.; Carone, M.; Paneroni, M.; Ceriana, P.; Pasqua, F.; et al. Italian Suggestions for Pulmonary Rehabilitation in COVID-19 Patients Recovering from Acute Respiratory Failure: Results of a Delphi Process. Monaldi Arch. Chest Dis. 2020, 90, 1–9. [Google Scholar] [CrossRef]
- Zhao, H.-M.; Xie, Y.-X.; Wang, C. Recommendations for Respiratory Rehabilitation in Adults with Coronavirus Disease 2019. Chin. Med. J. 2020, 133, 1595–1602. [Google Scholar] [CrossRef]
- Bettoni, L.; Bonomi, F.G.; Zani, V.; Manisco, L.; Indelicato, A.; Lanteri, P.; Banfi, G.; Lombardi, G. Effects of 15 Consecutive Cryotherapy Sessions on the Clinical Output of Fibromyalgic Patients. Clin. Rheumatol. 2013, 32, 1337–1345. [Google Scholar] [CrossRef]
- Hirvonen, H.E.; Mikkelsson, M.K.; Kautiainen, H.; Pohjolainen, T.H.; Leirisalo-Repo, M. Effectiveness of Different Cryotherapies on Pain and Disease Activity in Active Rheumatoid Arthritis. A Randomised Single Blinded Controlled Trial. Clin. Exp. Rheumatol. 2006, 24, 295–301. [Google Scholar]
- Mourot, L.; Cluzeau, C.; Regnard, J. Hyperbaric Gaseous Cryotherapy: Effects on Skin Temperature and Systemic Vasoconstriction. Arch. Phys. Med. Rehabil. 2007, 88, 1339–1343. [Google Scholar] [CrossRef]
- Stanek, A.; Cholewka, A.; Gadula, J.; Drzazga, Z.; Sieron, A.; Sieron-Stoltny, K. Can Whole-Body Cryotherapy with Subsequent Kinesiotherapy Procedures in Closed Type Cryogenic Chamber Improve BASDAI, BASFI, and Some Spine Mobility Parameters and Decrease Pain Intensity in Patients with Ankylosing Spondylitis? BioMed Res. Int. 2015, 2015, 404259. [Google Scholar] [CrossRef] [Green Version]
- Rymaszewska, J.; Ramsey, D.; Chładzińska-Kiejna, S. Whole-Body Cryotherapy as Adjunct Treatment of Depressive and Anxiety Disorders. Arch. Immunol. Ther. Exp. 2008, 56, 63–68. [Google Scholar] [CrossRef] [Green Version]
- Miller, E.; Kostka, J.; Włodarczyk, T.; Dugué, B. Whole-Body Cryostimulation (Cryotherapy) Provides Benefits for Fatigue and Functional Status in Multiple Sclerosis Patients. A Case-Control Study. Acta Neurol. Scand. 2016, 134, 420–426. [Google Scholar] [CrossRef]
- Bouzigon, R.; Ravier, G.; Dugue, B.; Grappe, F. The Use of Whole-Body Cryostimulation to Improve the Quality of Sleep in Athletes During High Level Standard Competitions. Br. J. Sports Med. 2014, 48, 572. [Google Scholar] [CrossRef] [Green Version]
- Rose, C.; Edwards, K.M.; Siegler, J.; Graham, K.; Caillaud, C. Whole-Body Cryotherapy as a Recovery Technique after Exercise: A Review of the Literature. Int. J. Sports Med. 2017, 38, 1049–1060. [Google Scholar] [CrossRef] [Green Version]
- Vitenet, M.; Tubez, F.; Marreiro, A.; Polidori, G.; Taiar, R.; Legrand, F.; Boyer, F.C. Effect of Whole Body Cryotherapy Interventions on Health-Related Quality of Life in Fibromyalgia Patients: A Randomized Controlled Trial. Complement. Ther. Med. 2018, 36, 6–8. [Google Scholar] [CrossRef]
- Costello, J.T.; Baker, P.R.; Minett, G.M.; Bieuzen, F.; Stewart, I.B.; Bleakley, C. Whole-body Cryotherapy (Extreme Cold Air Exposure) for Preventing and Treating Muscle Soreness after Exercise in Adults. Cochrane Database Syst. Rev. 2015, 9, CD010789. [Google Scholar] [CrossRef] [Green Version]
- Smolander, J.; Westerlund, T.; Uusitalo, A.; Dugué, B.; Oksa, J.; Mikkelsson, M. Lung Function after Acute and Repeated Exposures to Extremely Cold Air (-110 Degrees C) during Whole-Body Cryotherapy. Clin. Physiol. Funct. Imaging 2006, 26, 232–234. [Google Scholar] [CrossRef]
- Banfi, G.; Melegati, G.; Barassi, A.; d’Eril, G.M. Effects of the Whole-Body Cryotherapy on NTproBNP, HsCRP and Troponin I in Athletes. J. Sci. Med. Sport 2009, 12, 609–610. [Google Scholar] [CrossRef]
- Bezzoli, E.; Andreotti, D.; Pianta, L.; Mascheroni, M.; Piccinno, L.; Puricelli, L.; Cimolin, V.; Salvadori, A.; Codecasa, F.; Capodaglio, P. Motor Control Exercises of the Lumbar-Pelvic Region Improve Respiratory Function in Obese Men. A Pilot Study. Disabil. Rehabil. 2018, 40, 152–158. [Google Scholar] [CrossRef]
- Ramani, C.; Davis, E.M.; Kim, J.S.; Provencio, J.J.; Enfield, K.B.; Kadl, A. Post-ICU COVID-19 Outcomes: A Case Series. Chest 2021, 159, 215–218. [Google Scholar] [CrossRef]
- Lubkowska, A.; Szyguła, Z.; Chlubek, D.; Banfi, G. The Effect of Prolonged Whole-Body Cryostimulation Treatment with Different Amounts of Sessions on Chosen pro- and Anti-Inflammatory Cytokines Levels in Healthy Men. Scand. J. Clin. Lab. Investig. 2011, 71, 419–425. [Google Scholar] [CrossRef]
- Bouzigon, R.; Dupuy, O.; Tiemessen, I.; De Nardi, M.; Bernard, J.-P.; Mihailovic, T.; Theurot, D.; Miller, E.D.; Lombardi, G.; Dugué, B.M. Cryostimulation for Post-Exercise Recovery in Athletes: A Consensus and Position Paper. Front. Sports Act. Living 2021, 3, 688828. [Google Scholar] [CrossRef]
- Bianchi, V.E. Weight Loss Is a Critical Factor to Reduce Inflammation. Clin. Nutr. ESPEN 2018, 28, 21–35. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Admission | Discharge | ||
|---|---|---|---|
| Anthropometry and Body Composition | Weight (kg) | 61.8 | 63.2 |
| Height (cm) | 169 | 169 | |
| BMI (kg/m2) | 21.63 | 22.12 | |
| Hematological Biomarkers | ALT (U/L) | 204 | 14 |
| AST (U/L) | 167 | 14 | |
| GGT (U/L) | 387 | 91 | |
| CRP (mg/dL) | 0.3 | 0.1 | |
| ESR mg/dL | 34 | 18 | |
| Physical Performance | Handgrip strength (kg) | 16.6 | 17.5 |
| TUG (s) | Bedridden | 11.31 | |
| FIM scale | 73/126 | 124/126 | |
| VAS function | 90/100 | 10/100 | |
| Pain | VAS pain | 30/100 | 20/100 |
| Admission | Discharge | ||
|---|---|---|---|
| Anthropometry and Body Composition | Weight (kg) | 89.6 | 85 |
| Height (cm) | 164 | 164 | |
| BMI (kg/m2) | 33.31 | 31.6 | |
| Waist circumference | 111 | 105 | |
| FM (kg; %) | 44; 49.1 | 39.9; 46.3 | |
| FFM (kg; %) | 45.6; 50.9 | 46.3; 53.7 | |
| MM (kg; %) | 26.4; 29.5 | 28; 32.5 | |
| ASMM (kg; %) | 17.7 | 18 | |
| Hematological Biomarkers | ALT (U/L) | 22 | 26 |
| GGT (U/L) | 22 | 15 | |
| HBA1C (mmol/mL; %) | 62; 7.8 | 54; 7.1 | |
| Glucose (mg/dL) | 183 | 117 | |
| HDL (mg/dL) | 41 | 40 | |
| LDL (mg/dL) | 159 | 83 | |
| Triglycerides (mg/dL) | 256 | 164 | |
| Physical Performance | 6MWT | 495 | 565 |
| Handgrip strength (kg) | 23.4 | 23.2 | |
| TUG (s) | 8 | 7.54 | |
| FIM scale | 123/126 | 124/126 | |
| VAS function | 28/100 | 5/100 | |
| VAS pain | 22/100 | 6/100 | |
| Pain | VAS pain | 22/100 | 6/100 |
| Trunk Range of Motion | Extension ° | 10 | 10 |
| Flexion ° | 80 | 90 | |
| Left lateral bending ° | 20 | 25 | |
| Right lateral bending ° | 20 | 25 |
| Admission | Discharge | ||
|---|---|---|---|
| Anthropometry and Body Composition | Weight (kg) | 136.4 | 130.8 |
| Height (cm) | 182 | 182 | |
| BMI (kg/m2) | 41.18 | 39.49 | |
| Waist circumference | 138 | 127 | |
| FM (kg; %) | 76.9; 56.4 | 74.4; 56.5 | |
| FFM (kg; %) | 59.5; 43.6 | 57.2; 43.5 | |
| MM (kg; %) | 33.1; 24.3 | 31.2; 23.7 | |
| ASMM (kg; %) | 27.6 | 25 | |
| Hematological Biomarkers | ALT (U/L) | 16 | 16 |
| GGT (U/L) | 12 | 11 | |
| HBA1C (mmol/mL; %) | 37; 5.5 | 37; 5.5 | |
| Glucose (mg/dL) | 95 | 98 | |
| HDL (mg/dL) | 42 | 45 | |
| LDL (mg/dL) | 114 | 112 | |
| Triglycerides (mg/dL) | 220 | 179 | |
| Physical Performance | Handgrip strength (kg) | 15 | 15.6 |
| TUG (s) | 8 | 7 | |
| FIM scale | 105/126 | 119/126 | |
| VAS function | 50/100 | 18/100 | |
| EuroQol | 50/100 | 75/100 | |
| MRC dyspnea | 4/5 | 2/5 | |
| Pain | VAS Pain | 100/100 | 57/100 |
| Trunk Range of Motion | Extension ° | 20 | 20 |
| Flexion ° | 60 | 60 | |
| Left lateral bending ° | 30 | 25 | |
| Right lateral bending ° | 30 | 30 |
| Admission | Discharge | ||
|---|---|---|---|
| Anthropometry and Body Composition | Weight (kg) | 116.2 | 109 |
| Height (cm) | 157.5 | 157.5 | |
| BMI (kg/m2) | 46.84 | 43.94 | |
| Waist circumference | 129 | 127 | |
| FM (kg; %) | 60.1; 51.7 | 57.4; 52.6 | |
| FFM (kg; %) | 56.1; 48.3 | 51.7; 47.4 | |
| MM (kg; %) | 38; 32.7 | 32.5; 29.8 | |
| ASMM (kg; %) | 23.8 | 21.4 | |
| Hematological Biomarkers | ALT (U/L) | 38 | 32 |
| AST (U/L) | 18 | 18 | |
| GGT (U/L) | 20 | 14 | |
| HBA1C (mmol/mL; %) | 37; 5.5 | 34; 5.3 | |
| Glucose (mg/dL) | 100 | 88 | |
| Insulin (mU/L) | 45.7 | 17.7 | |
| Total cholesterol (mg/dL) | 165 | 114 | |
| HDL (mg/dL) | 42 | 34 | |
| LDL (mg/dL) | 107 | 63 | |
| Triglycerides (mg/dL) | 130 | 87 | |
| Ferritin (μg/L) | 127 | 139 | |
| CRP (mg/dL) | 0.5 | 0.3 | |
| ESR (mg/dL) | 30 | 17 | |
| LDH (U/L) | 235 | 195 | |
| Physical Performance | Handgrip strength (kg) | 15.9 | 7.4 |
| TUG (s) | 9.42 | 7.40 | |
| FIM scale | 114/126 | 121/126 | |
| VAS function | 53/100 | 40/100 | |
| EuroQol | 30/100 | 50/100 | |
| MRC dyspnea | 3/5 | 2/5 | |
| Pain | VAS Pain | 53/100 | 40/100 |
| Trunk Range of Motion | Extension ° | 20 | 20 |
| Flexion ° | 60 | 60 | |
| Left lateral bending ° | 30 | 25 | |
| Right lateral bending ° | 30 | 30 |
| Admission | Discharge | ||
|---|---|---|---|
| Anthropometry and Body Composition | Weight (kg) | 88.5 | 85.4 |
| Height (cm) | 150 | 150 | |
| BMI (kg/m2) | 39.33 | 37.96 | |
| Waist circumference | 110 | 110 | |
| FM (kg; %) | 45.6; 51.5 | 39.7; 46.2 | |
| FFM (kg; %) | 42.9; 48.5 | 46.3; 53.8 | |
| MM (kg; %) | 20.9; 23.6 | 28.5; 33.1 | |
| ASMM (kg; %) | 22.3 | 17.6 | |
| Hematological Biomarkers | ALT (U/L) | 14 | 8 |
| AST (U/L) | 13 | 11 | |
| GGT (U/L) | 16 | 13 | |
| HBA1C (mmol/mL; %) | 39; 5.7 | 35; 5.4 | |
| Glucose (mg/dL) | 80 | 82 | |
| Insulin (mU/L) | 13 | 18.9 | |
| Total cholesterol (mg/dL) | 170 | 131 | |
| HDL (mg/dL) | 49 | 42 | |
| LDL (mg/dL) | 103 | 76 | |
| Triglycerides (mg/dL) | 141 | 94 | |
| Ferritin (μg/L) | 35 | 41 | |
| CRP (mg/dL) | 0.9 | 0.7 | |
| ESR (mg/dL) | 56 | 35 | |
| LDH (U/L) | 178 | 159 | |
| D-dimer (μg/L) | 798 | 478 | |
| Fibrinogen (mg/dL) | 453 | 340 | |
| Physical Performance | Handgrip strength (kg) | 16.6 | 16.2 |
| TUG (s) | 10.5 | 8.7 | |
| FIM scale | 124/126 | 124/126 | |
| VAS function | 49/100 | 29/100 | |
| EuroQol | 60/100 | 80/100 | |
| MRC dyspnea | 3/5 | 2/5 | |
| Pain | Vas pain | 50/100 | 28/100 |
| Trunk Range of Motion | Extension ° | 10 | 15 |
| Flexion ° | 50 | 80 | |
| Left lateral bending ° | 15 | 15 | |
| Right lateral bending ° | 15 | 15 |
| Admission | Discharge | ||
|---|---|---|---|
| Anthropometry and Body Composition | Weight (kg) | 140 | 134.8 |
| Height (cm) | 189 | 189 | |
| BMI (kg/m2) | 39.19 | 37.74 | |
| Waist circumference | 129 | 126 | |
| FM (kg; %) | 65.4; 47.3 | 60.7; 44.7 | |
| FFM (kg; %) | 72.9; 52.7 | 75.1; 55.3 | |
| MM (kg; %) | 50.4; 36.4 | 44.4; 75.1 | |
| ASMM (kg; %) | 30.7 | 30.6 | |
| Hematological Biomarkers | ALT (U/L) | 51 | 70 |
| AST (U/L) | 31 | 44 | |
| GGT (U/L) | 26 | 20 | |
| HBA1C (mmol/mL; %) | 50; 6.7 | 44; 6.2 | |
| Glucose (mg/dL) | 151 | 117 | |
| Total cholesterol (mg/dL) | 192 | 182 | |
| HDL (mg/dL) | 48 | 39 | |
| LDL (mg/dL) | 122 | 122 | |
| Triglycerides (mg/dL) | 174 | 134 | |
| Ferritin (μg/L) | 639 | 531 | |
| CRP (mg/dL) | 1.1 | 0.1 | |
| ESR (mg/dL) | 20 | 13 | |
| LDH (U/L) | 216 | 193 | |
| D-dimer (μg/L) | 514 | 435 | |
| Physical Performance | 6MWT (m) | 510 | 568 |
| Handgrip strength (kg) | 49.8 | 49.3 | |
| VAS function | 25/100 | 3/100 | |
| EuroQol | 70/100 | 90/100 | |
| MRC dyspnea | 1/5 | 0/5 |
| Admission | Discharge | ||
|---|---|---|---|
| Anthropometry and Body Composition | Weight (kg) | 111.4 | 108.1 |
| Height (cm) | 168 | 168 | |
| BMI (kg/m2) | 39.47 | 38.3 | |
| Waist circumference | 136 | 124 | |
| FM (kg; %) | 57.3; 34.1 | 55.5; 51.2 | |
| FFM (kg; %) | 52.0; 31.0 | 52.9; 48.8 | |
| MM (kg; %) | 29.8; 27.3 | 29.3; 27 | |
| ASMM (kg; %) | 21.1 | 22.0 | |
| Hematological Biomarkers | ALT (U/L) | 30 | 41 |
| AST (U/L) | 19 | 24 | |
| GGT (U/L) | 21 | 17 | |
| HBA1C (mmol/mL; %) | 40; 5.8 | 40;5.8 | |
| Glucose (mg/dL) | 117 | 99 | |
| Insulin (mU/L) | 33.2 | 24.1 | |
| Total cholesterol (mg/dL) | 271 | 124 | |
| HDL (mg/dL) | 56 | 46 | |
| LDL (mg/dL) | 180 | 62 | |
| Triglycerides (mg/dL) | 141 | 87 | |
| CRP (mg/dL) | 0.0 | 0.0 | |
| ESR (mg/dL) | 13 | 2 | |
| Physical Performance | TUG (s) | 6.54 | 10.18 |
| FIM | 123/126 | 124/126 | |
| VAS function | 65/100 | 0/100 | |
| EuroQol | 57/100 | 60/100 | |
| MRC dyspnea | 1/5 | 0/5 | |
| Pain | VAS pain | 48/100 | 30/100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piterà, P.; Gobbi, M.; Fontana, J.M.; Cattaldo, S.; Massucci, M.; Capodaglio, P. Whole-Body Cryostimulation: A Rehabilitation Booster in Post-COVID Patients? A Case Series. Appl. Sci. 2022, 12, 4830. https://doi.org/10.3390/app12104830
Piterà P, Gobbi M, Fontana JM, Cattaldo S, Massucci M, Capodaglio P. Whole-Body Cryostimulation: A Rehabilitation Booster in Post-COVID Patients? A Case Series. Applied Sciences. 2022; 12(10):4830. https://doi.org/10.3390/app12104830
Chicago/Turabian StylePiterà, Paolo, Michele Gobbi, Jacopo Maria Fontana, Stefania Cattaldo, Maurizio Massucci, and Paolo Capodaglio. 2022. "Whole-Body Cryostimulation: A Rehabilitation Booster in Post-COVID Patients? A Case Series" Applied Sciences 12, no. 10: 4830. https://doi.org/10.3390/app12104830
APA StylePiterà, P., Gobbi, M., Fontana, J. M., Cattaldo, S., Massucci, M., & Capodaglio, P. (2022). Whole-Body Cryostimulation: A Rehabilitation Booster in Post-COVID Patients? A Case Series. Applied Sciences, 12(10), 4830. https://doi.org/10.3390/app12104830