
Numerical and Experimental Investigations on Vocal Fold Approximation in Healthy and Simulated Unilateral Vocal Fold Paralysis


Abstract
1. Introduction
2. Materials and Methods
2.1. Surgical Methodology
2.1.1. Animals
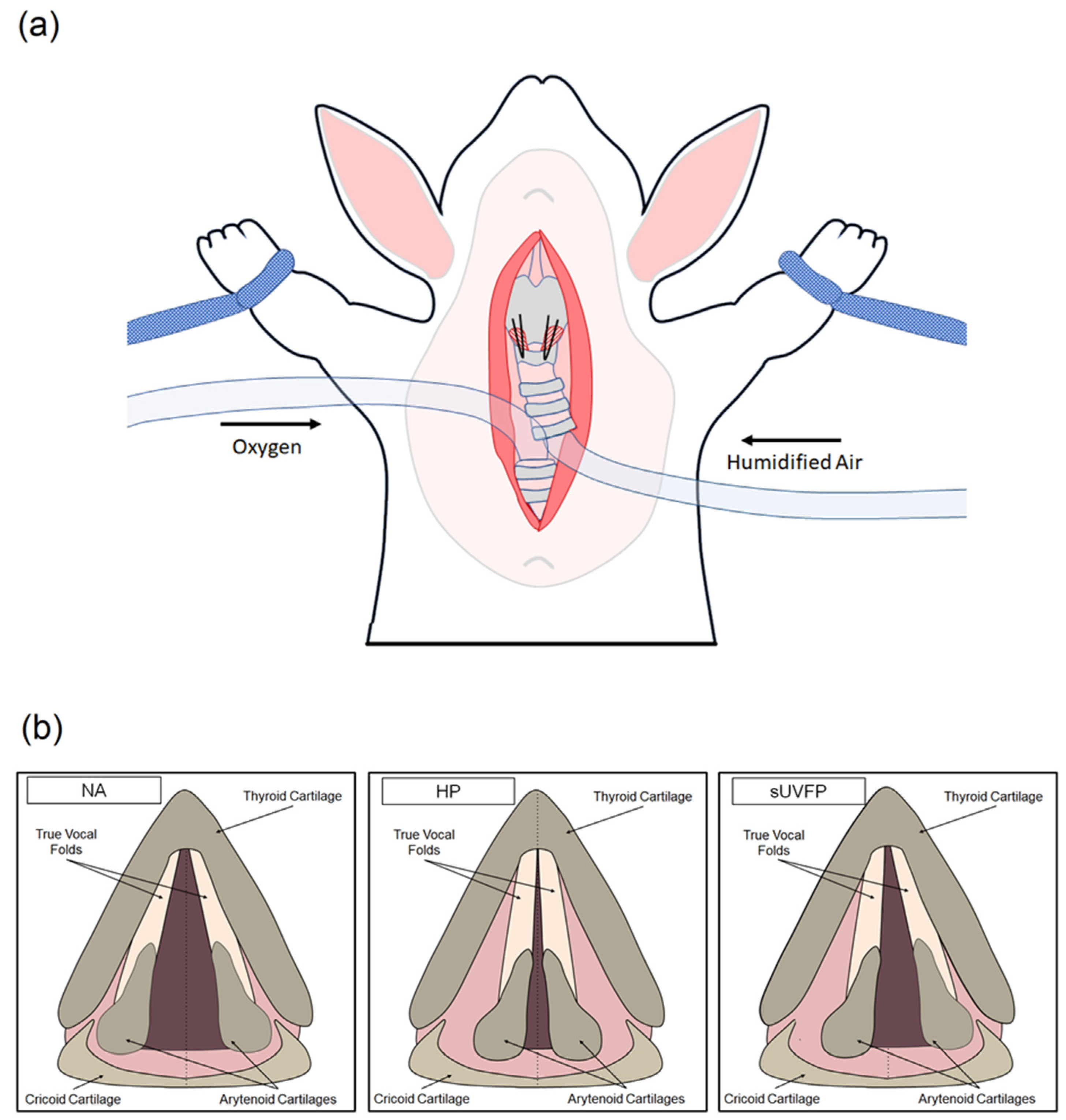
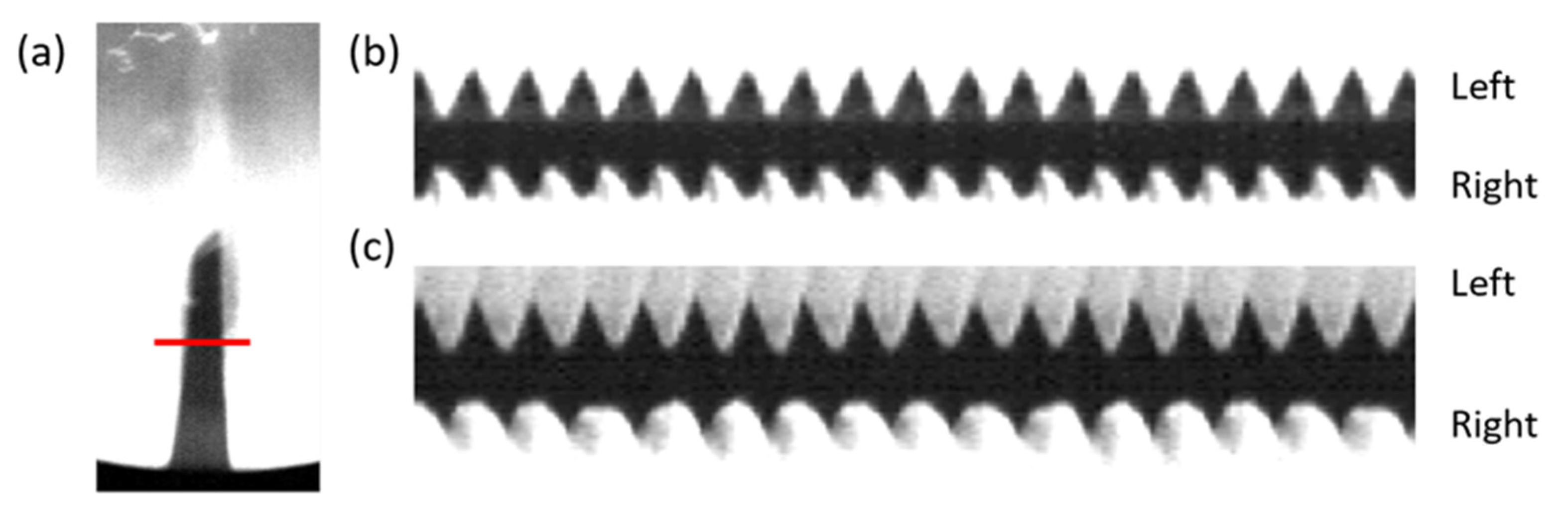
2.1.2. In Vivo Phonation
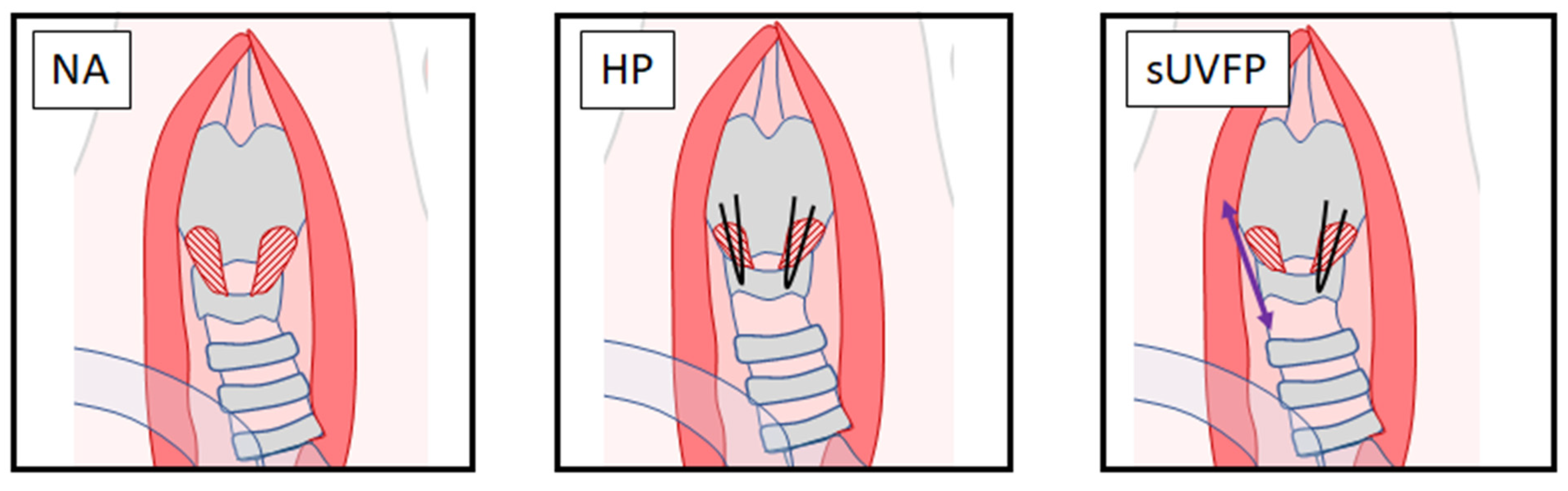
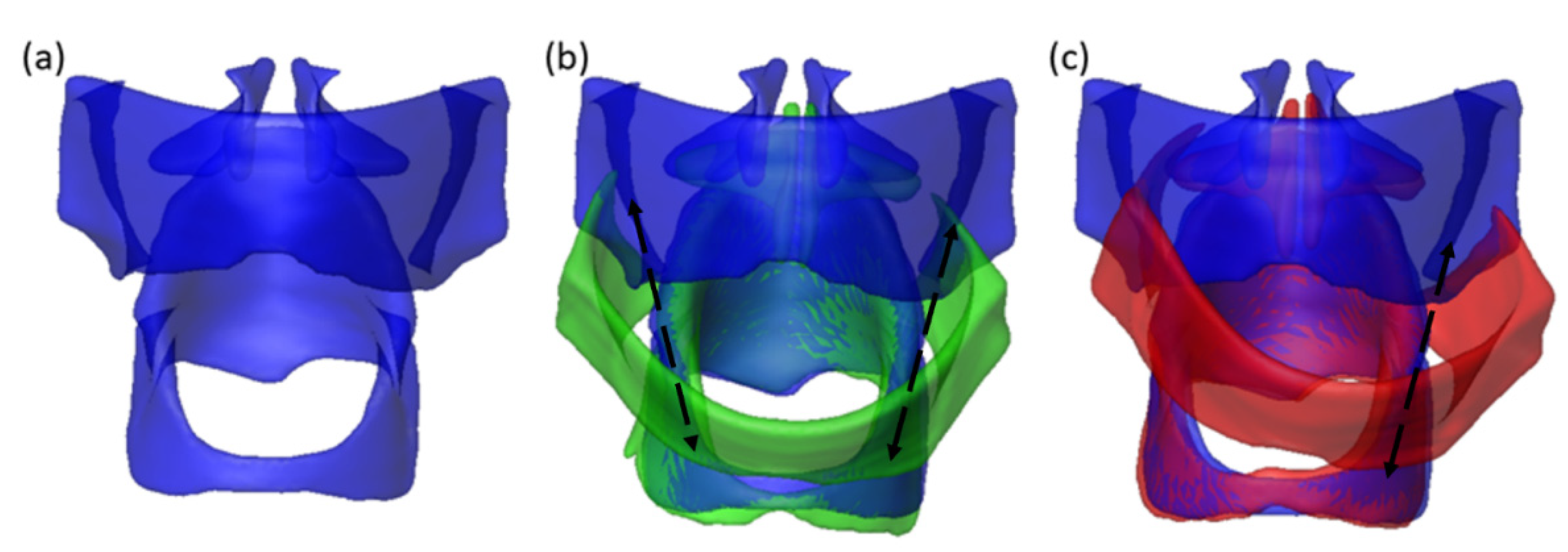
2.1.3. Cricothyroid Suture Approximation Laryngeal Conditions
2.1.4. Ex Vivo Cricothyroid Suture Approximation and MRI
2.2. Numerical Methodology
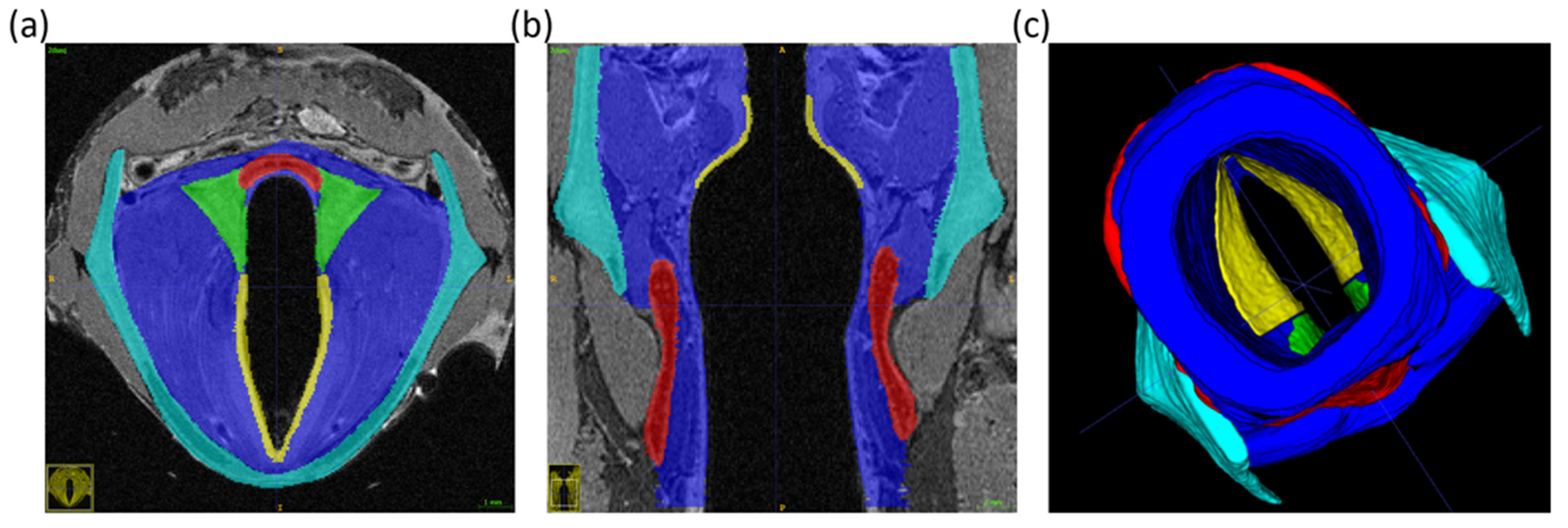
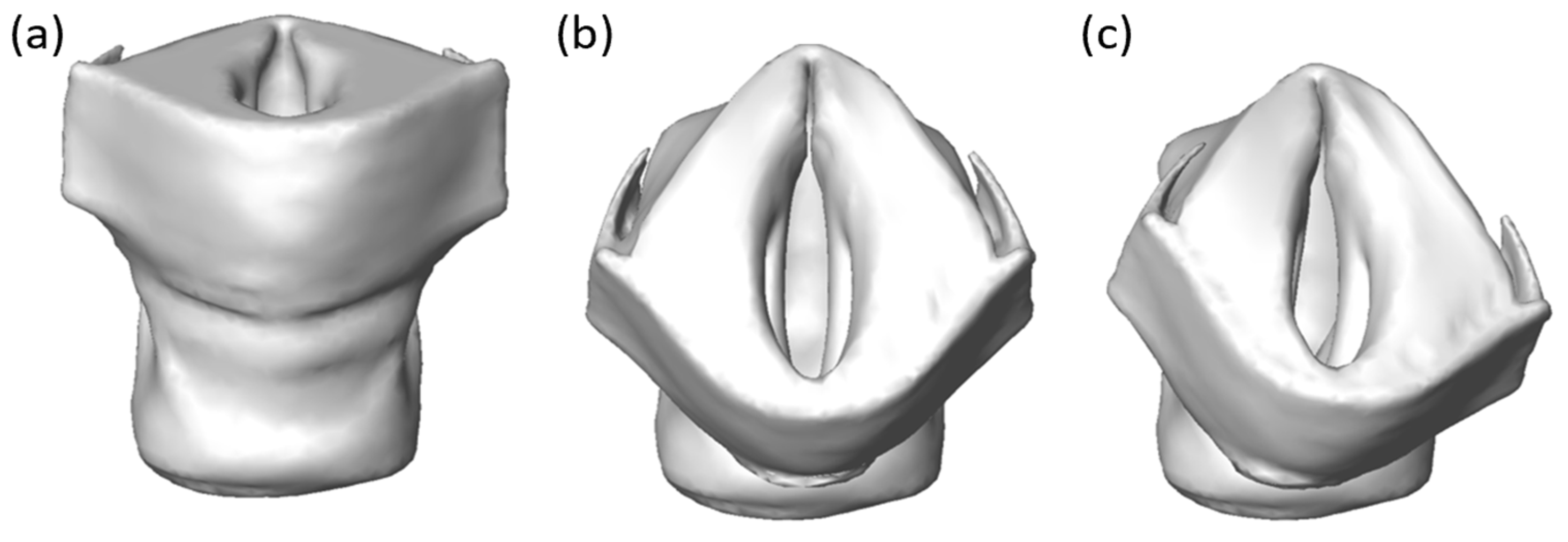
2.2.1. Vocal Fold Reconstruction from MRI Scan
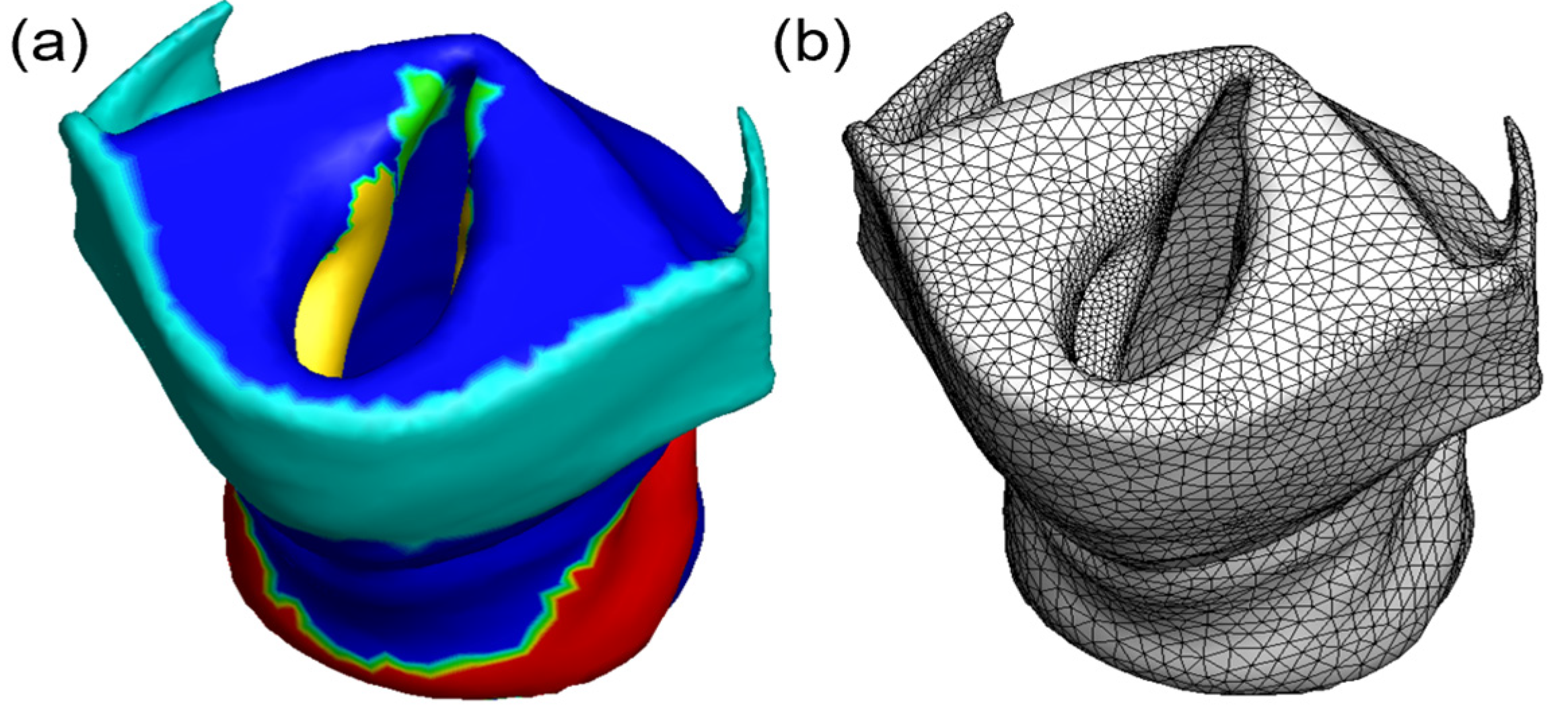
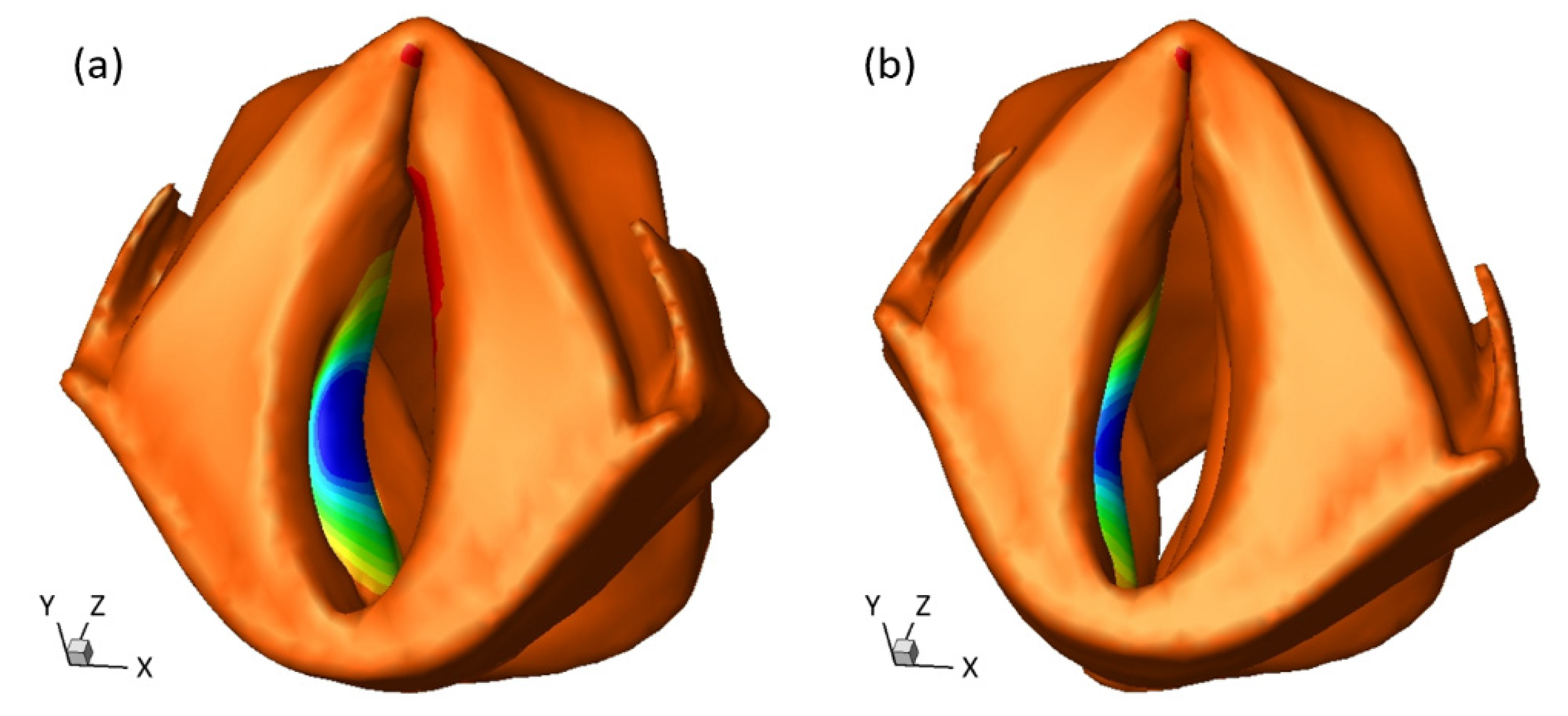
2.2.2. Vocal Fold Approximation Modeling
3. Results
3.1. In Vivo Phonation Test Results
3.2. Eigenfrequency of Approximated Vocal Fold
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CT | Computed tomography |
| FEM | Finite element modeling |
| HP | Healthy phonation |
| HSV | High-speed video |
| MRI | Magnetic resonance imaging |
| NA | Non-approximated |
| UVFP | Unilateral vocal fold paralysis |
| sUVFP | Simulated UVFP |
References
- Titze, I.R.; Jiang, J.; Drucker, D.G. Preliminaries to the body-cover theory of pitch control. J. Voice 1988, 1, 314–319. [Google Scholar] [CrossRef]
- Wilson, A.; Kimball, E.E.; Sayce, L.; Luo, H.; Khosla, S.M.; Rousseau, B. Medialization Laryngoplasty: A Review for Speech-Language Pathologists. J. Speech Lang. Hear. Res. 2021, 1–10. [Google Scholar] [CrossRef]
- Havas, T.; Lowinger, D.; Priestley, J. Unilateral Vocal Fold Paralysis: Causes, Options and Outcomes. ANZ J. Surg. 1999, 69, 509–513. [Google Scholar] [CrossRef]
- Rosenthal, L.H.S.; Benninger, M.S.; Deeb, R.H. Vocal Fold Immobility: A Longitudinal Analysis of Etiology Over 20 Years. Laryngoscope 2007, 117, 1864–1870. [Google Scholar] [CrossRef]
- Sulica, L. The Natural History of Idiopathic Unilateral Vocal Fold Paralysis: Evidence and Problems. Laryngoscope 2008, 118, 1303–1307. [Google Scholar] [CrossRef]
- Francis, D.O.; McKiever, M.E.; Garrett, C.G.; Jacobson, B.; Penson, D.F. Assessment of patient experience with unilateral vocal fold immobility: A preliminary study. J. Voice 2014, 28, 636–643. [Google Scholar] [CrossRef]
- Kelchner, L.N.; Stemple, J.C.; Gerdeman, B.; Le Borgne, W.; Adam, S. Etiology, pathophysiology, treatment choices, and voice results for unilateral adductor vocal fold paralysis: A 3-year retrospective. J. Voice 1999, 13, 592–601. [Google Scholar] [CrossRef]
- Paniello, R.C.; Edgar, J.D.; Kallogjeri, D.; Piccirillo, J.F. Medialization versus reinnervation for unilateral vocal fold paralysis: A multicenter randomized clinical trial. Laryngoscope 2011, 121, 2172–2179. [Google Scholar] [CrossRef] [PubMed]
- Brunner, E.; Friedrich, G.; Kiesler, K.; Chibidziura-Priesching, J.; Gugatschka, M. Subjective Breathing Impairment in Unilateral Vocal Fold Paralysis. Folia Phoniatr. Logop. 2011, 63, 142–146. [Google Scholar] [CrossRef]
- Francis, D.O.; Ms, K.W.; Hovis, K.; Gelbard, A.; Merati, A.L.; Penson, D.F.; Netterville, J.L.; Garrett, C.G. Effect of injection augmentation on need for framework surgery in unilateral vocal fold paralysis. Laryngoscope 2016, 126, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Leder, S.B.; Suiter, D.M.; Duffey, D.; Judson, B.L. Vocal Fold Immobility and Aspiration Status: A Direct Replication Study. Dysphagia 2011, 27, 265–270. [Google Scholar] [CrossRef]
- Bertroche, J.T.; Radder, M.; Kallogjeri, D.; Paniello, R.C.; Bradley, J.P. Patient-defined duration of benefit from juvederm (hyaluronic acid) used in injection laryngoplasty. Laryngoscope 2019, 129, 2744–2747. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.T.; Benyamini, L. Voice outcome after vocal fold injection augmentation with carboxymethyl cellulose versus calcium hydroxyapatite. J. Laryngol. Otol. 2020, 134, 263–269. [Google Scholar] [CrossRef]
- Fang, T.-J.; Li, H.-Y.; Gliklich, R.E.; Chen, Y.-H.; Wang, P.-C.; Chuang, H.-F. Outcomes of Fat Injection Laryngoplasty in Unilateral Vocal Cord Paralysis. Arch. Otolaryngol. Head Neck Surg. 2010, 136, 457. [Google Scholar] [CrossRef] [PubMed]
- Kwon, T.-K.; Rosen, C.A.; Gartner-Schmidt, J. Preliminary Results of a New Temporary Vocal Fold Injection Material. J. Voice 2005, 19, 668–673. [Google Scholar] [CrossRef]
- Mallur, P.S.; Morrison, M.P.; Postma, G.N.; Amin, M.R.; Rosen, C.A. Safety and efficacy of carboxymethylcellulose in the treatment of glottic insufficiency. Laryngoscope 2012, 122, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Zeitels, S.M.; Lombardo, P.J.; Chaves, J.L.; Faquin, W.C.; Hillman, R.E.; Heaton, J.T.; Kobler, J.B. Vocal Fold Injection of Absorbable Materials: A Histologic Analysis with Clinical Ramifications. Ann. Otol. Rhinol. Laryngol. 2019, 128, 71S–81S. [Google Scholar] [CrossRef] [PubMed]
- Zeleník, K.; Walderová, R.; Kučová, H.; Jančatová, D.; Komínek, P. Comparison of long-term voice outcomes after vocal fold augmentation using autologous fat injection by direct microlaryngoscopy versus office-based calcium hydroxylapatite injection. Eur. Arch. Oto Rhinol. Laryngol. 2017, 274, 3147–3151. [Google Scholar] [CrossRef]
- Cohen, J.T.; Bates, D.D.; Postma, G.N. Revision Gore-Tex Medialization Laryngoplasty. Otolaryngol. Neck Surg. 2004, 131, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Maragos, N.E. Revision Thyroplasty. Ann. Otol. Rhinol. Laryngol. 2001, 110, 1087–1092. [Google Scholar] [CrossRef]
- Netterville, J.L.; Stone, R.E.; Civantos, F.J.; Luken, E.S.; Ossoff, R.H. Silastic Medialization and Arytenoid Adduction: The Vanderbilt Experience. Ann. Otol. Rhinol. Laryngol. 1993, 102, 413–424. [Google Scholar] [CrossRef]
- Parker, N.P.; Barbu, A.M.; Hillman, R.E.; Zeitels, S.M.; Burns, J.A. Revision Transcervical Medialization Laryngoplasty for Unilateral Vocal Fold Paralysis. Otolaryngol. Neck Surg. 2015, 153, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Woo, P.; Pearl, A.W.; Hsiung, M.-W.; Som, P. Failed medialization laryngoplasty: Management by revision surgery. Otolaryngol. Neck Surg. 2001, 124, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Green, D.C.; Berke, G.S.; Ward, P.H. Vocal Fold Medialization by Surgical Augmentation versus Arytenoid Adduction in the in vivo Canine Model. Ann. Otol. Rhinol. Laryngol. 1991, 100, 280–287. [Google Scholar] [CrossRef]
- Hiroto, I. Surgical voice improvement for unilateral recurrent laryngeal nerve paralysis. Otologia 1976, 22, 473–474. [Google Scholar]
- Orestes, M.I.; Neubauer, J.; Sofer, E.; Salinas, J.; Chhetri, D.K. Phonatory effects of type I thyroplasty implant shape and depth of medialization in unilateral vocal fold paralysis. Laryngoscope 2014, 124, 2791–2796. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Nasseri, S.S.; Maragos, N.E. Combination thyroplasty and the “twisted larynx:” combined type IV and type I thyroplasty for superior laryngeal nerve weakness. J. Voice 2000, 14, 104–111. [Google Scholar] [CrossRef]
- Shaw, G.Y.; Searl, J.P.; Hoover, L.A. Diagnosis and treatment of unilateral cricothyroid muscle paralysis with a modified Isshiki type 4 thyroplasty. Otolaryngol. Neck Surg. 1995, 113, 679–688. [Google Scholar] [CrossRef]
- Novaleski, C.K.; Kojima, T.; Chang, S.; Luo, H.; Valenzuela, C.V.; Rousseau, B. Nonstimulated rabbit phonation model: Cricothyroid approximation. Laryngoscope 2016, 126, 1589–1594. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.; Novaleski, C.K.; Kojima, T.; Mizuta, M.; Luo, H.; Rousseau, B. Subject-Specific Computational Modeling of Evoked Rabbit Phonation. J. Biomech. Eng. 2016, 138, 011005–0110056. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.; Tian, F.-B.; Luo, H.; Doyle, J.F.; Rousseau, B. The Role of Finite Displacements in Vocal Fold Modeling. J. Biomech. Eng. 2013, 135, 111008. [Google Scholar] [CrossRef]
- Li, Z.; Chen, Y.; Chang, S.; Luo, H. A Reduced-Order Flow Model for Fluid–Structure Interaction Simulation of Vocal Fold Vibration. J. Biomech. Eng. 2020, 142, 0210051–02100510. [Google Scholar] [CrossRef]
- Luo, H.; Mittal, R.; Bielamowicz, S.A. Analysis of flow-structure interaction in the larynx during phonation using an immersed-boundary method. J. Acoust. Soc. Am. 2009, 126, 816–824. [Google Scholar] [CrossRef]
- Sadeghi, H.; Kniesburges, S.; Falk, S.; Kaltenbacher, M.; Schützenberger, A.; Döllinger, M. Towards a Clinically Applicable Computational Larynx Model. Appl. Sci. 2019, 9, 2288. [Google Scholar] [CrossRef]
- Xue, Q.; Zheng, X.; Mittal, R.; Bielamowicz, S. Subject-specific computational modeling of human phonation. J. Acoust. Soc. Am. 2014, 135, 1445–1456. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Wang, X.; Krane, M.; Zhang, L.T. Fully-coupled aeroelastic simulation with fluid compressibility—For application to vocal fold vibration. Comput. Methods Appl. Mech. Eng. 2017, 315, 584–606. [Google Scholar] [CrossRef]
- Chen, Y.; Li, Z.; Chang, S.; Rousseau, B.; Luo, H. A reduced-order flow model for vocal fold vibration: From idealized to subject-specific models. J. Fluids Struct. 2020, 94, 102940. [Google Scholar] [CrossRef] [PubMed]
- Mittal, R.; Erath, B.D.; Plesniak, M.W. Fluid Dynamics of Human Phonation and Speech. Annu. Rev. Fluid Mech. 2013, 45, 437–467. [Google Scholar] [CrossRef]
- Swanson, E.R.; Ohno, T.; Abdollahian, D.; Rousseau, B. Effects of raised-intensity phonation on inflammatory mediator gene expression in normal rabbit vocal fold. Otolaryngol. Neck Surg. 2010, 143, 567–572. [Google Scholar] [CrossRef]
- Alipour, F.; Brücker, C.; Cook, D.D.; Gömmel, A.; Kaltenbacher, M.; Mattheus, W.; Mongeau, L.; Nauman, E.; Schwarze, R.; Tokuda, I.; et al. Mathematical Models and Numerical Schemes for the Simulation of Human Phonation. Curr. Bioinform. 2011, 6, 323–343. [Google Scholar] [CrossRef][Green Version]
- Zhang, Z.; Kreiman, J.; Gerratt, B.R.; Garellek, M. Acoustic and perceptual effects of changes in body layer stiffness in symmetric and asymmetric vocal fold modelsa. J. Acoust. Soc. Am. 2013, 133, 453–462. [Google Scholar] [CrossRef] [PubMed]
- Birk, V.; Kniesburges, S.; Semmler, M.; Berry, D.A.; Bohr, C.; Döllinger, M.; Schützenberger, A. Influence of glottal closure on the phonatory process in ex vivo porcine larynges. J. Acoust. Soc. Am. 2017, 142, 2197–2207. [Google Scholar] [CrossRef]
- Döllinger, M.; Berry, D.A.; Kniesburges, S. Dynamic vocal fold parameters with changing adduction inex-vivohemilarynx experiments. J. Acoust. Soc. Am. 2016, 139, 2372–2385. [Google Scholar] [CrossRef] [PubMed]
- Goodyer, E.; Müller, F.; Licht, K.; Hess, M. In vivo measurement of the shear modulus of the human vocal fold: Interim results from eight patients. Eur. Arch. Oto Rhino. Laryngol. 2007, 264, 631–635. [Google Scholar] [CrossRef]
- Hadwin, P.J.; Motie-Shirazi, M.; Erath, B.D.; Peterson, S.D. Bayesian Inference of Vocal Fold Material Properties from Glottal Area Waveforms Using a 2D Finite Element Model. Appl. Sci. 2019, 9, 2735. [Google Scholar] [CrossRef]
- Hunter, E.J.; Titze, I.R.; Alipour, F. A three-dimensional model of vocal fold abduction/adduction. J. Acoust. Soc. Am. 2004, 115, 1747–1759. [Google Scholar] [CrossRef]
- Lamprecht, R.; Maghzinajafabadi, M.; Semmler, M.; Sutor, A. Imaging the Vocal Folds: A Feasibility Study on Strain Imaging and Elastography of Porcine Vocal Folds. Appl. Sci. 2019, 9, 2729. [Google Scholar] [CrossRef]
- Maghzinajafabadi, M.; Lamprecht, R.; Sutor, M.S.A.A.; Semmler, M.; Sutor, A. Acoustic Pressure Pipette Aspiration Method Combined with Finite Element Analysis for Isotropic Materials. Appl. Sci. 2019, 9, 3875. [Google Scholar] [CrossRef]
- Chen, T.; Chodara, A.M.; Sprecher, A.J.; Fang, F.; Song, W.; Tao, C.; Jiang, J.J. A New Method of Reconstructing the Human Laryngeal Architecture Using Micro-MRI. J. Voice 2012, 26, 555–562. [Google Scholar] [CrossRef]
- Hoffman, M.R.; Glab, R.; Gunderson, M.; Maytag, A.L.; Yang, D.T.; Jiang, J.J.; Dailey, S.H. Functional and Histological Evaluation following Canine Vocal Fold Reconstruction Using Composite Thyroid Ala Perichondrium Flaps. Otolaryngol. Neck Surg. 2015, 153, 79–87. [Google Scholar] [CrossRef]
- U.S. Department of Agriculture. Animal Care: Animal Welfare Act and Animal Welfare Regulations. (n.d.). Available online: www.ascr.usda.gov/fling-program-discrimination (accessed on 31 December 2020).
- National Research Council. Guide for the Care and Use of Laboratory Animals; National Academies Press: Cambridge, MA, USA, 2011.
- Sayce, L.J.; E Powell, M.; E Kimball, E.; Chen, P.; Gartling, G.J.; Rousseau, B. Continuous Rate Infusion of Ketamine Hydrochloride and Dexmedetomidine for Maintenance of Anesthesia during Laryngotracheal Surgery in New Zealand White Rabbits (Oryctolagus cuniculus). J. Am. Assoc. Lab. Anim. Sci. 2020, 59, 176–185. [Google Scholar] [CrossRef]
- Hirano, M. Phonosurgery. Basic and clinical investigations. Otology (Fukuoka) 1975, 21, 239–242. [Google Scholar]
- Tian, F.-B.; Dai, H.; Luo, H.; Doyle, J.F.; Rousseau, B. Fluid–structure interaction involving large deformations: 3D simulations and applications to biological systems. J. Comput. Phys. 2014, 258, 451–469. [Google Scholar] [CrossRef]
- Alipour, F.; Berry, D.A.; Titze, I.R. A finite-element model of vocal-fold vibration. J. Acoust. Soc. Am. 2000, 108, 3003–3012. [Google Scholar] [CrossRef]
- Rousseau, B.; Hirano, S.; Chan, R.W.; Welham, N.V.; Thibeault, S.L.; Ford, C.N.; Bless, D.M. Characterization of chronic vocal fold scarring in a rabbit model. J. Voice 2004, 18, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Thibeault, S.L.; Gray, S.D.; Bless, D.M.; Chan, R.W.; Ford, C.N. Histologic and rheologic characterization of vocal fold scarring. J. Voice 2002, 16, 96–104. [Google Scholar] [CrossRef]
- Yin, J.; Zhang, Z. The influence of thyroarytenoid and cricothyroid muscle activation on vocal fold stiffness and eigenfrequencies. J. Acoust. Soc. Am. 2013, 133, 2972–2983. [Google Scholar] [CrossRef]
- Caballero, M.; Bernal-Sprekelsen, M.; Calvo, C.; Farré, X.; Alós, L. Autologous elastic cartilage for laryngoplasty: Histologic evaluation in a rabbit model. Ann. Otol. Rhinol. Laryngol. 2003, 112, 734–739. [Google Scholar] [CrossRef] [PubMed]
- Berry, D.A. Mechanisms of modal and nonmodal phonation. J. Phon. 2001, 29, 431–450. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Right (Hz) | Left (Hz) | Difference | ||
|---|---|---|---|---|
| Subject 1 | HP | 875 | 875 | <1% |
| sUVFP | 815 | 908 | 11% | |
| Subject 2 | HP | 660 | 660 | <1% |
| sUVFP | 605 | 670 | 10% | |
| Subject 3 | HP | 763 | 763 | <1% |
| sUVFP | 650 | 722 | 11% | |
| Young’s Modulus (kPa) | Poisson’s Ratio | Density (kg/m3) | |
|---|---|---|---|
| Vocal fold body | 10 | 0.4 | 1000 |
| Vocal fold cover | 1 | 0.4 | 1000 |
| Cartilages | 500 | 0.4 | 1000 |
| Right(Hz) | Left (Hz) | Difference | ||
|---|---|---|---|---|
| Sample 1 | NA | 334 | 333 | <1% |
| HP | 605 | 597 | 1% | |
| sUVFP | 560 | 610 | 9% | |
| Sample 2 | NA | 302 | 300 | <1% |
| HP | 533 | 531 | <1% | |
| sUVFP | 499 | 535 | 7% | |
| Sample 3 | NA | 329 | 330 | <1% |
| HP | 609 | 608 | <1% | |
| sUVFP | 506 | 550 | 9% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Z.; Wilson, A.; Sayce, L.; Avhad, A.; Rousseau, B.; Luo, H. Numerical and Experimental Investigations on Vocal Fold Approximation in Healthy and Simulated Unilateral Vocal Fold Paralysis. Appl. Sci. 2021, 11, 1817. https://doi.org/10.3390/app11041817
Li Z, Wilson A, Sayce L, Avhad A, Rousseau B, Luo H. Numerical and Experimental Investigations on Vocal Fold Approximation in Healthy and Simulated Unilateral Vocal Fold Paralysis. Applied Sciences. 2021; 11(4):1817. https://doi.org/10.3390/app11041817
Chicago/Turabian StyleLi, Zheng, Azure Wilson, Lea Sayce, Amit Avhad, Bernard Rousseau, and Haoxiang Luo. 2021. "Numerical and Experimental Investigations on Vocal Fold Approximation in Healthy and Simulated Unilateral Vocal Fold Paralysis" Applied Sciences 11, no. 4: 1817. https://doi.org/10.3390/app11041817
APA StyleLi, Z., Wilson, A., Sayce, L., Avhad, A., Rousseau, B., & Luo, H. (2021). Numerical and Experimental Investigations on Vocal Fold Approximation in Healthy and Simulated Unilateral Vocal Fold Paralysis. Applied Sciences, 11(4), 1817. https://doi.org/10.3390/app11041817