
Microcirculatory and Metabolic Responses during Voluntary Cycle Ergometer Exercise with a Whole-Body Neuromuscular Electrical Stimulation Device


Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
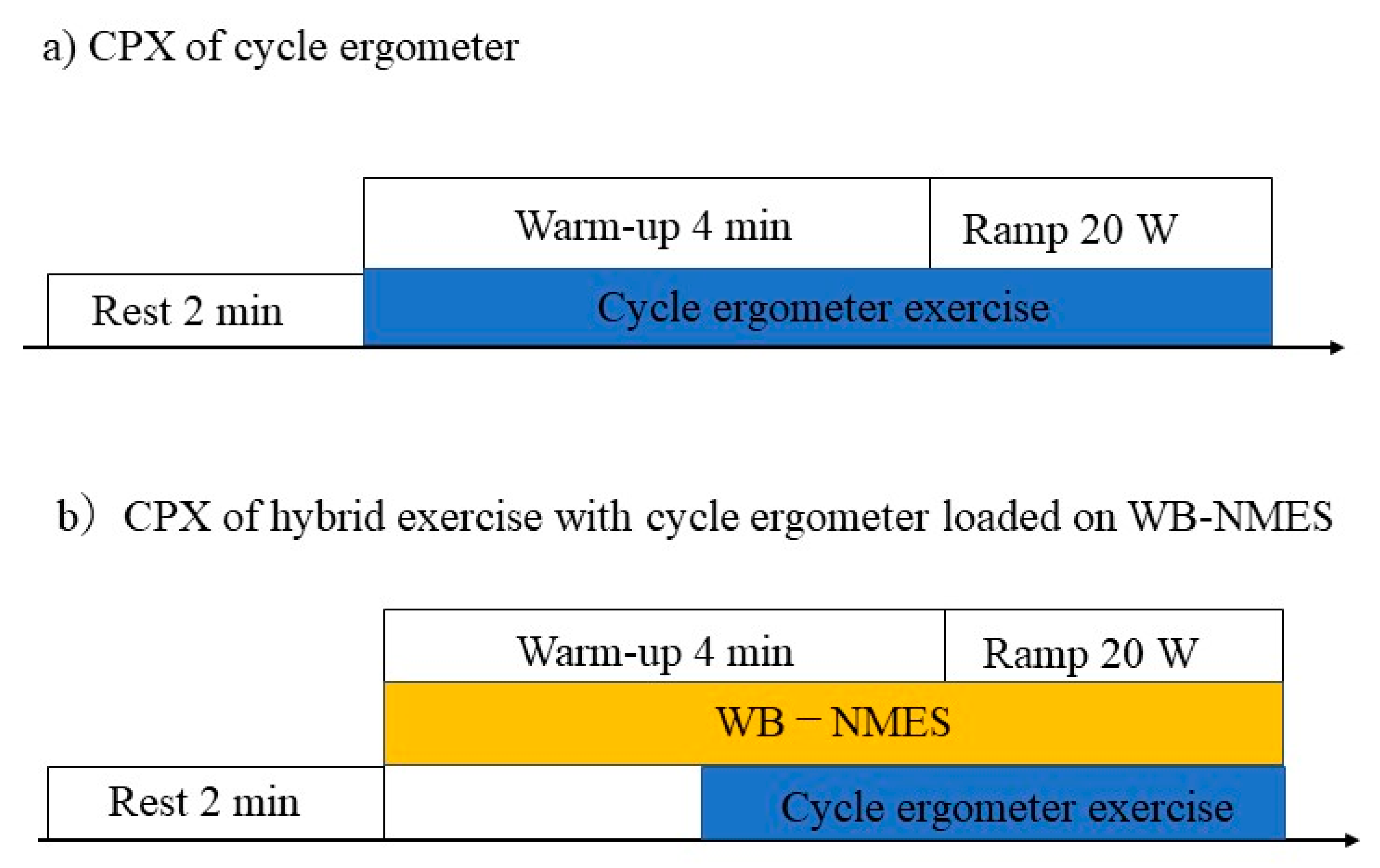
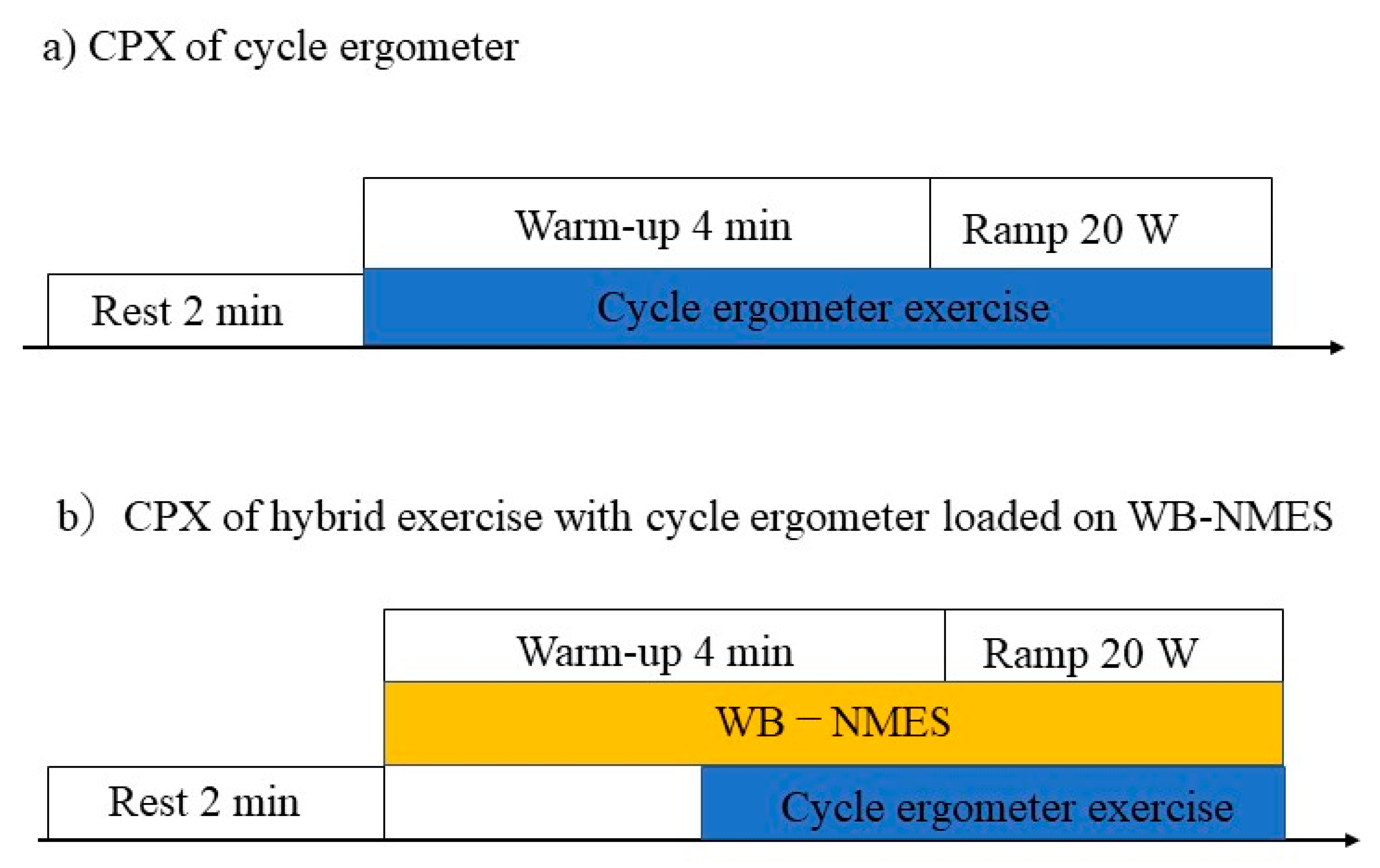
2.1. Study Design
2.2. Participants
2.3. Measurement
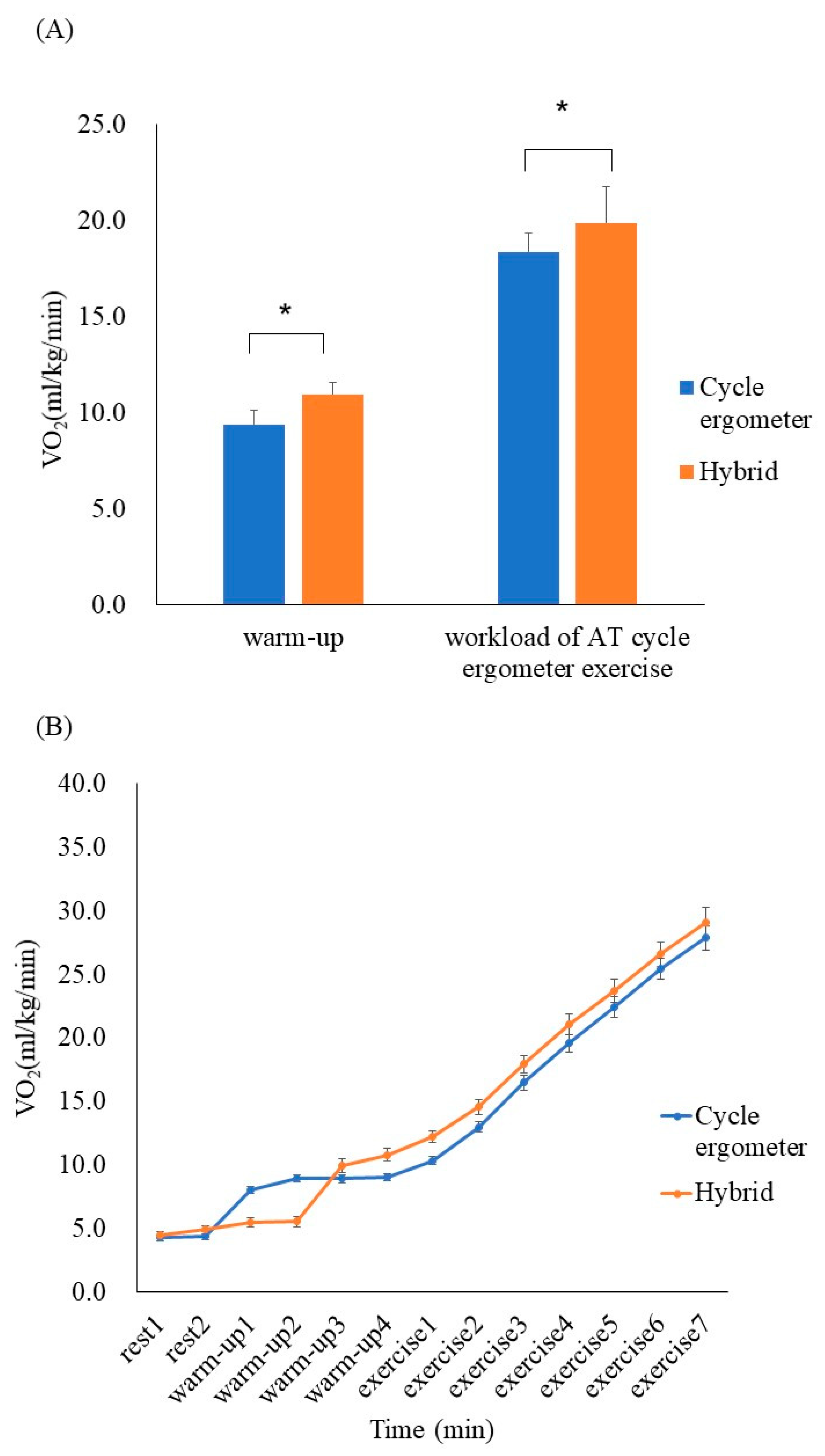
2.3.1. Cardiopulmonary Exercise Test
2.3.2. Ex Vivo Blood Fluidity Evaluation
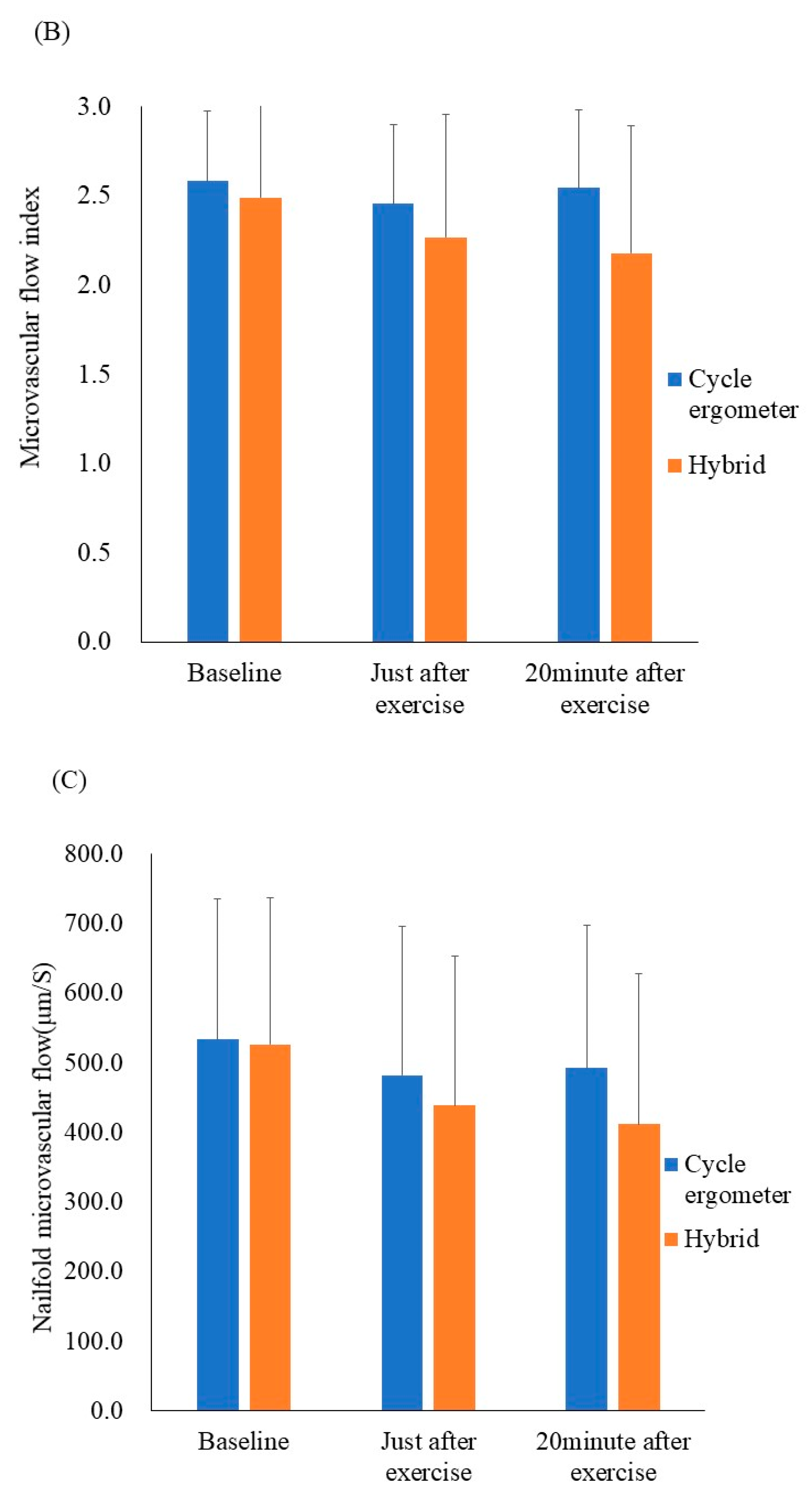
2.3.3. In Vivo Microcirculatory Evaluation
2.4. Study Protocol
2.5. Statistical Analysis
3. Results
Participants
4. Discussion
5. Limitation
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nuhr, M.J.; Pette, D.; Berger, R.; Quittan, M.; Crevenna, R.; Huelsman, M.; Wiesinger, G.F.; Moser, P.; Fialka-Moser, V.; Pacher, R. Beneficial effects of chronic low-frequency stimulation of thigh muscles in patients with advanced chronic heart failure. Eur. Heart J. 2004, 25, 136–143. [Google Scholar] [CrossRef] [Green Version]
- Kondo, T.; Yamada, S.; Tanimura, D.; Kazama, S.; Ishihara, T.; Shimojo, M.; Iwata, E.; Kondo, S.; Hiraiwa, H.; Kato, T.; et al. Neuromuscular electrical stimulation is feasible in patients with acute heart failure. ESC Heart Fail. 2019, 6, 975–982. [Google Scholar] [CrossRef]
- Kemmler, W.; Teschler, M.; Weissenfels, A.; Bebenek, M.; Von Stengel, S.; Kohl, M.; Freiberger, E.; Goisser, S.; Jakob, F.; Sieber, C.C.; et al. Whole-body electromyostimulation to fight sarcopenic obesity in community-dwelling older women at risk. Resultsof the randomized controlled FORMOsA-sarcopenic obesity study. Osteoporos. Int. 2016, 27, 3261–3270. [Google Scholar] [CrossRef]
- Van Buuren, F.; Mellwig, K.P.; Prinz, C.; Körber, B.; Fründ, A.; Fritzsche, D.; Faber, L.; Kottmann, T.; Bogunovic, N.; Dahm, J.B.; et al. Electrical myostimulation improves left ventricular function and peak oxygen consumption in patients with chronic heart failure: Results from the exEMS study comparing different stimulation strategies. Clin. Res. Cardiol. 2013, 102, 523–534. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, K.; Taniguchi, Y.; Moritani, T. Metabolic and cardiovascular responses during voluntary pedaling exercise with electrical muscle stimulation. Eur. J. App. Physiol. 2014, 114, 1801–1807. [Google Scholar] [CrossRef]
- Watanabe, K.; Yoshida, T.; Ishikawa, T.; Kawade, S.; Moritani, T. Effect of the Combination of Whole-Body Neuromuscular Electrical Stimulation and Voluntary Exercise on Metabolic Responses in Human. Front. Physiol. 2019, 10, 291. [Google Scholar] [CrossRef]
- McCarthy, D.A.; Dale, M.M. The Leucocytosis of Exercise. A Review and Model. Sports Med. 1988, 6, 333–363. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, N.; Yasu, T.; Tsuboi, K.; Sugawara, Y.; Kubo, N.; Umemoto, T.; Arao, K.; Kawakami, M.; Momomura, S.-I. Effects of Submaximal Exercise on Blood Rheology and Sympathetic Nerve Activity. Circ. J. 2010, 74, 730–734. [Google Scholar] [CrossRef] [Green Version]
- Mayer, G.A. Blood Viscosity in Healthy Subjects and Patients with Coronary Heart Disease. Can. Med. Assoc. J. 1964, 91, 951–954. [Google Scholar] [PubMed]
- Hoshiai, M.; Ochiai, K.; Tamura, Y.; Tsurumi, T.; Terashima, M.; Tamiya, H.; Maeno, E.; Mizuguchi, S.; Tomoe, T.; Kawabe, A.; et al. Effects of whole-body neuromuscular electrical stimulation device on hemodynamics, arrhythmia, and sublingual microcirculation. Heart Vessel. 2021, 36, 844–852. [Google Scholar] [CrossRef]
- Matsuse, H.; Shiba, N.; Takano, Y.; Yamada, S.; Ohshima, H.; Tagawa, Y. Cycling exercise to resist electrically stimulated antagonist increases oxygen uptake in males: Pilot study. J. Rehabil. Res. Dev. 2013, 50, 545. [Google Scholar] [CrossRef] [PubMed]
- Beaver, W.L.; Wasserman, K.; Whipp, B.J. A new method for detecting anaerobic threshold by gas exchange. J. Appl. Physiol. 1986, 60, 2020–2027. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, Y.; Sato, K.; Ohki, H.; Kaneko, T. Optically accessible microchannels formed in a single-crystal silicon substrate for studies of blood rheology. Microvasc. Res. 1992, 44, 226–240. [Google Scholar] [CrossRef]
- Yasu, T.; Mutoh, A.; Wada, H.; Kobayashi, M.; Kikuchi, Y.; Momomura, S.; Ueda, S. Renin-Angiotensin System Inhibitors Can Prevent Intravenous Lipid Infusion-Induced Myocardial Microvascular Dysfunction and Leukocyte Activation. Circ. J. 2018, 82, 494–501. [Google Scholar] [CrossRef] [Green Version]
- Shimizu, R.; Fukuda, H.; Kikuchi, Y.; Yanaka, H.; Hata, N.; Yamazaki, M.; Nakatani, Y.; Tamura, Y.; Yamakoshi, S.; Kawabe, A.; et al. Clinically feasible method for assessing leukocyte rheology in whole blood. Heart Vessel. 2020, 35, 268–277. [Google Scholar] [CrossRef] [Green Version]
- Boerma, E.C.; Mathura, K.R.; Van Der Voort, P.H.J.; Spronk, P.E.; Ince, C. Quantifying bedside-derived imaging of microcirculatory abnormalities in septic patients: A prospective validation study. Crit. Care 2005, 9, R601–R606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Backer, D.; Hollenberg, S.; Boerma, C.; Goedhart, P.; Büchele, G.; Ospina-Tascon, G.; Dobbe, I.; Ince, C. How to evaluate the microcirculation: Report of a round table conference. Crit. Care 2007, 11, R101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massey, M.J.; Shapiro, N.I. A guide to human in vivo microcirculatory flow image analysis. Crit. Care 2015, 20, 35. [Google Scholar] [CrossRef] [Green Version]
- Paillard, T. Training Based on Electrical Stimulation Superimposed onto Voluntary Contraction Would be Relevant Only as Part of Submaximal Contractions in Healthy Subjects. Front. Physiol. 2018, 9, 1428. [Google Scholar] [CrossRef]
- Wahl, P.; Hein, M.; Achtzehn, S.; Bloch, W.; Mester, J. Acute effects of superimposed electromyostimulation during cycling on myokines and markers of muscle damage. J. Musculoskelet. Neuronal Interact. 2015, 15, 53–59. [Google Scholar]
- Bourey, R.E.; Santoro, S.A. Interactions of Exercise, Coagulation, Platelets, and Fibrinolysis—A Brief Review. Med. Sci. Sports Exer. 1988, 20, 439–446. [Google Scholar] [CrossRef]
- Van Wijck, K.; Lenaerts, K.; van Loon, L.J.; Peters, W.H.M.; Buurman, W.A.; DeJong, C.H.C. Exercise-Induced Splanchnic Hypoperfusion Results in Gut Dysfunction in Healthy Men. PLoS ONE 2011, 6, e22366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, X.; Weil, M.H.; Sun, S.; Tang, W.; Bisera, J.; Mason, E.J. Decreases in organ blood flows associated with increases in sublingual PCO2 during hemorrhagic shock. J. Appl. Physiol. 1998, 85, 2360–2364. [Google Scholar] [CrossRef]
- Pranskunas, A.; Arstikyte, J.; Pranskuniene, Z.; Bernatoniene, J.; Kiudulaite, I.; Vaitkaitiene, E.; Vaitkaitis, D.; Brazaitis, M. Time Evolution of Sublingual Microcirculatory Changes in Recreational Marathon Runners. BioMed Res. Int. 2017, 2017, 7120785. [Google Scholar] [CrossRef] [Green Version]
- Petrofsky, J.; Schwab, E.; Lo, T.; Cúneo, M.; George, J.; Kim, J.; Al-Malty, A. Effects of electrical stimulation on skin blood flow in controls and in and around stage III and IV wounds in hairy and non-hairy skin. Med. Sci. Monit. 2005, 11, CR309–CR316. [Google Scholar]
- Asadi, M.R.; Torkaman, G.; Hedayati, M.; Mohajeri-Tehrani, M.R.; Ahmadi, M.; Gohardani, R.F. Angiogenic effects of low-intensity cathodal direct current on ischemic diabetic foot ulcers: A randomized controlled trial. Diabetes Res. Clin. Pract. 2017, 127, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Stöllberger, C.; Finsterer, J. Side effects of whole-body electro-myo-stimulation. Wien. Med. Wochenschr. 2018, 169, 173–180. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (n = 15, mean ± SD) |
|---|---|
| Age (y) | 28.9 ± 5.1 |
| Male (%) | 10 (67%) |
| Height (cm) | 166.7 ± 7.5 |
| Weight (kg) | 64.7 ± 11.8 |
| BMI (kg/m2) | 23.2 ± 3.2 |
| Exercise Style | Load (W) | Minute Ventilation (L/mL) | VCO2 (L/mL) |
|---|---|---|---|
| Cycle ergometer | 161.2 ± 35.0 | 63.7 ± 14.8 | 2117.6 ± 463.3 |
| Hybrid | 162.1 ± 33.1 | 71.4 ± 16.3 | 2242.5 ± 468.1 * |
| Cycle Ergometer Exercise | |||
|---|---|---|---|
| - | Baseline (n = 15) | Just after Exercise (n = 15) | 20 min after Exercise (n = 15) |
| Variables | Mean ± SD | Mean ± SD | Mean ± SD |
| Systolic blood pressure (mmHg) | 121.1 ± 14.9 | 172.5 ± 34.4 * | 116.1 ± 12.7 |
| Diastolic blood pressure (mmHg) | 76.9 ± 16.3 | 69.7 ± 18.7 | 77.5 ± 12.5 |
| Heart rate (beats per min) | 78.7 ± 9.5 | 169.6 ± 13.6 ** | 92.7 ± 12.4 ## |
| Lactic acid (mmol/L) | 1.8 ± 0.5 | 10.4 ± 2.3 ** | 6.7 ± 2.2 ** |
| Blood glucose level (mg/dL) | 100.4 ± 10.3 | 89.8 ± 15.5 | 84.1 ± 11.6 ## |
| White blood cells (103/µL) | 6.4 ± 1.5 | 9.0 ± 2.1 ** | 7.0 ± 1.6 ## |
| Platelets (103/µL) | 234.1 ± 36.8 | 270.9 ± 36.6 ** | 248.9 ± 38.2 ## |
| Hematocrit (%) | 42.2 ± 3.7 | 46.0 ± 4.2 ** | 43.8 ± 4 ## |
| Diacron-reactive oxygen metabolites (U. CARR) | 303.6 ± 64.2 | 321.7 ± 64.8 | 317.1 ± 67.2 |
| Biological antioxidant potential (μmol/L) | 2447.3 ± 486.3 | 2592.0 ± 320.2 | 2603.0 ± 278.3 |
| Total vessel density of small vessels (mm/mm2) | 11.8 ± 2.2 | 12.3 ± 1.5 | 12.3 ± 2.4 |
| Perfused vessel density (mm/mm2) | 9.2 ± 2.6 | 9.6 ± 1.5 | 9.5 ± 2.7 |
| Percentage of perfused small vessels (%) | 80.3 ± 15.4 | 80.2 ± 10.7 | 78.7 ± 15.9 |
| Hybrid (Cycle Ergometer + WB-ENMS) | |||
|---|---|---|---|
| - | Baseline (n = 15) | Just after Exercise (n = 15) | 20 min after Exercise (n = 15) |
| Variables | Mean ± SD | Mean ± SD | Mean ± SD |
| Systolic blood pressure (mmHg) | 118.3 ± 11.3 | 160.0 ± 23.4 ** | 116.9 ± 11.8 |
| Diastolic blood pressure (mmHg) | 72.7 ± 16.6 | 77.3 ± 17.3 | 78.7 ± 10.3 |
| Heart rate (Beats per min) | 80.9 ± 14.5 | 156.8 ± 11.7 ** | 90.3 ± 11.6 ## |
| Lactic acid (mmol/L) | 1.6 ± 0.2 | 11.1 ± 2.9 ** | 6.8 ± 1.9 ** |
| Blood glucose level (mg/dL) | 101.8 ± 15.9 | 88.0 ± 15.7 ** | 82.3 ± 10.7 ** |
| White blood cells (103/µL) | 6.2 ± 1.5 | 8.6 ± 1.9 ** | 6.7 ± 1.6 ## |
| Platelets (103/µL) | 238.5 ± 37.9 | 272.6 ± 0.1 ** | 250.2 ± 38.1 # |
| Hematocrit (%) | 41.9 ± 3.2 | 46.3 ± 4.2 ** | 44.1 ± 4.0 ## |
| Diacron-reactive oxygen metabolites (U. CARR) | 303.8 ± 73.3 | 328.8 ± 66.5 | 319.5 ± 68.7 |
| Biological antioxidant potential (μmol/L) | 2407.9 ± 332.9 | 2771.0 ± 481.8 * | 2707.5 ± 494.4 |
| Total vessel density of small vessels (mm/mm2) | 10.9 ± 1.8 | 12.3 ± 1.9 | 12.1 ± 2.5 |
| Perfused vessel density (mm/mm2) | 7.8 ± 2.3 | 8.7 ± 2.5 | 8.1 ± 3.6 |
| Percentage of perfused small vessels (%) | 73.6 ± 1 | 73.4 ± 19.0 | 62.3 ± 19.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ochiai, K.; Tamura, Y.; Terashima, M.; Tsurumi, T.; Yasu, T. Microcirculatory and Metabolic Responses during Voluntary Cycle Ergometer Exercise with a Whole-Body Neuromuscular Electrical Stimulation Device. Appl. Sci. 2021, 11, 12048. https://doi.org/10.3390/app112412048
Ochiai K, Tamura Y, Terashima M, Tsurumi T, Yasu T. Microcirculatory and Metabolic Responses during Voluntary Cycle Ergometer Exercise with a Whole-Body Neuromuscular Electrical Stimulation Device. Applied Sciences. 2021; 11(24):12048. https://doi.org/10.3390/app112412048
Chicago/Turabian StyleOchiai, Kaori, Yuma Tamura, Masato Terashima, Tomoki Tsurumi, and Takanori Yasu. 2021. "Microcirculatory and Metabolic Responses during Voluntary Cycle Ergometer Exercise with a Whole-Body Neuromuscular Electrical Stimulation Device" Applied Sciences 11, no. 24: 12048. https://doi.org/10.3390/app112412048
APA StyleOchiai, K., Tamura, Y., Terashima, M., Tsurumi, T., & Yasu, T. (2021). Microcirculatory and Metabolic Responses during Voluntary Cycle Ergometer Exercise with a Whole-Body Neuromuscular Electrical Stimulation Device. Applied Sciences, 11(24), 12048. https://doi.org/10.3390/app112412048