
Association of Posture, Gait, and Auditory Functioning with Cognitive Status in a Cohort of Community-Dwelling Older Adults



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Cognitive Testing
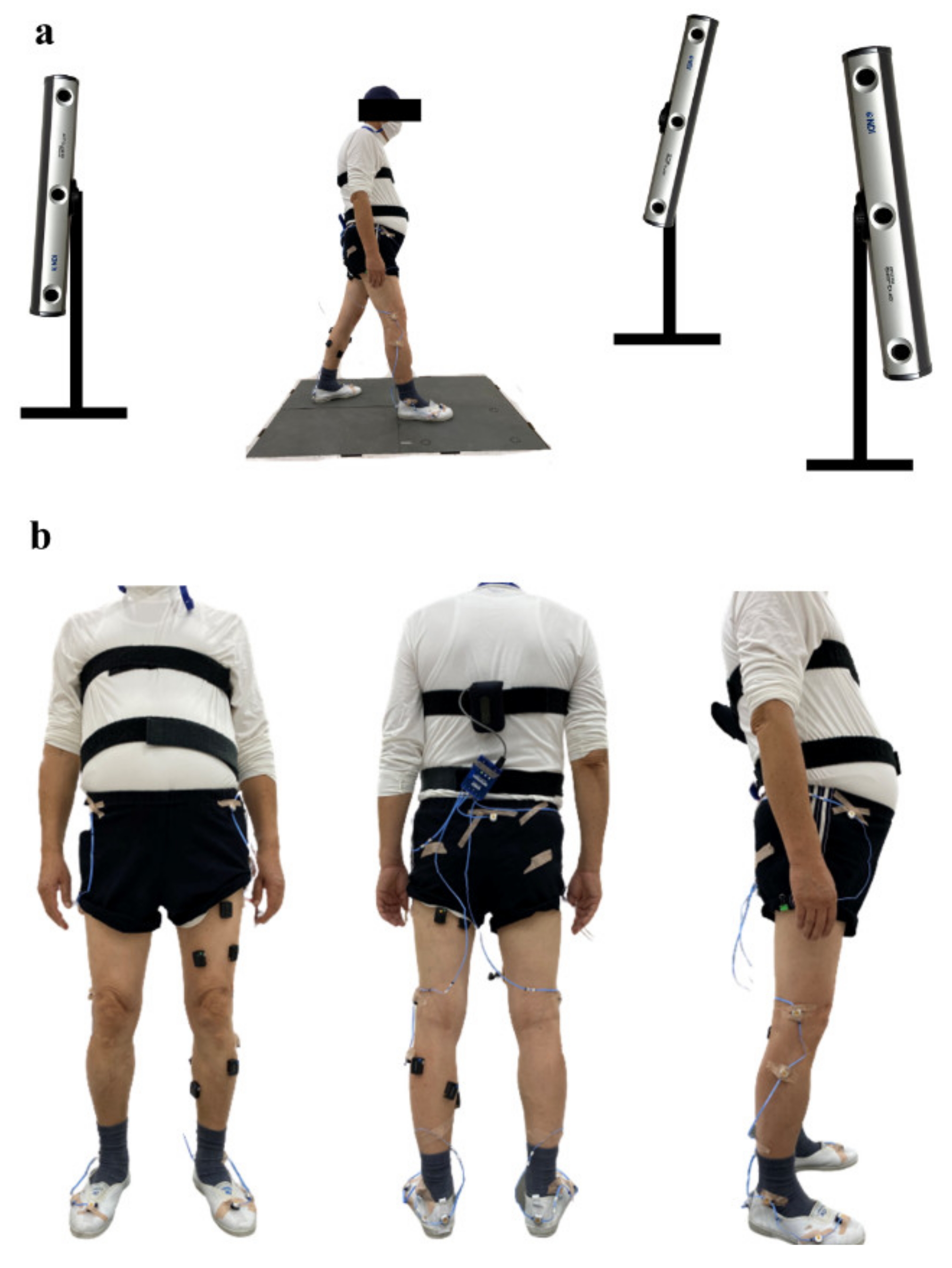
2.3. Level Walking
2.4. Audiological Exam
- 1.
- PTA R and L = 0.5, 1, and 2 kHz Average Pure Tone Audiometry score for the right (R) and left (L) ears.
- 2.
- SRT = Average Speech Recognition Threshold of both ears.
- 3.
- WRS = Average Word Recognition Score of both ears.
- 4.
- WRS error = Total number of errors on the word recognition test.
- 5.
- SRS = Average Sentence Recognition Score of both ears.
- 6.
- SRS error = Total number of errors on the sentence recognition test.
2.5. Balance Function Testing
2.6. Exclusion
- 1.
- Inadequate level walking data (disturbed digital signal obtained from position markers), 3 participants.
- 2.
- Reported tinnitus, hearing aid or ear injury, 8 participants.
- 3.
- Gait velocity of more than 2 standard deviations (SD) higher than the average, one participant.
2.7. Statistical Analysis
2.7.1. Comparative Analysis
2.7.2. Predictive Ability Assessment
2.7.3. Logistic Regression Model Design
3. Results
3.1. Comparive Analysis
3.1.1. Demographics
3.1.2. Cognitive Function
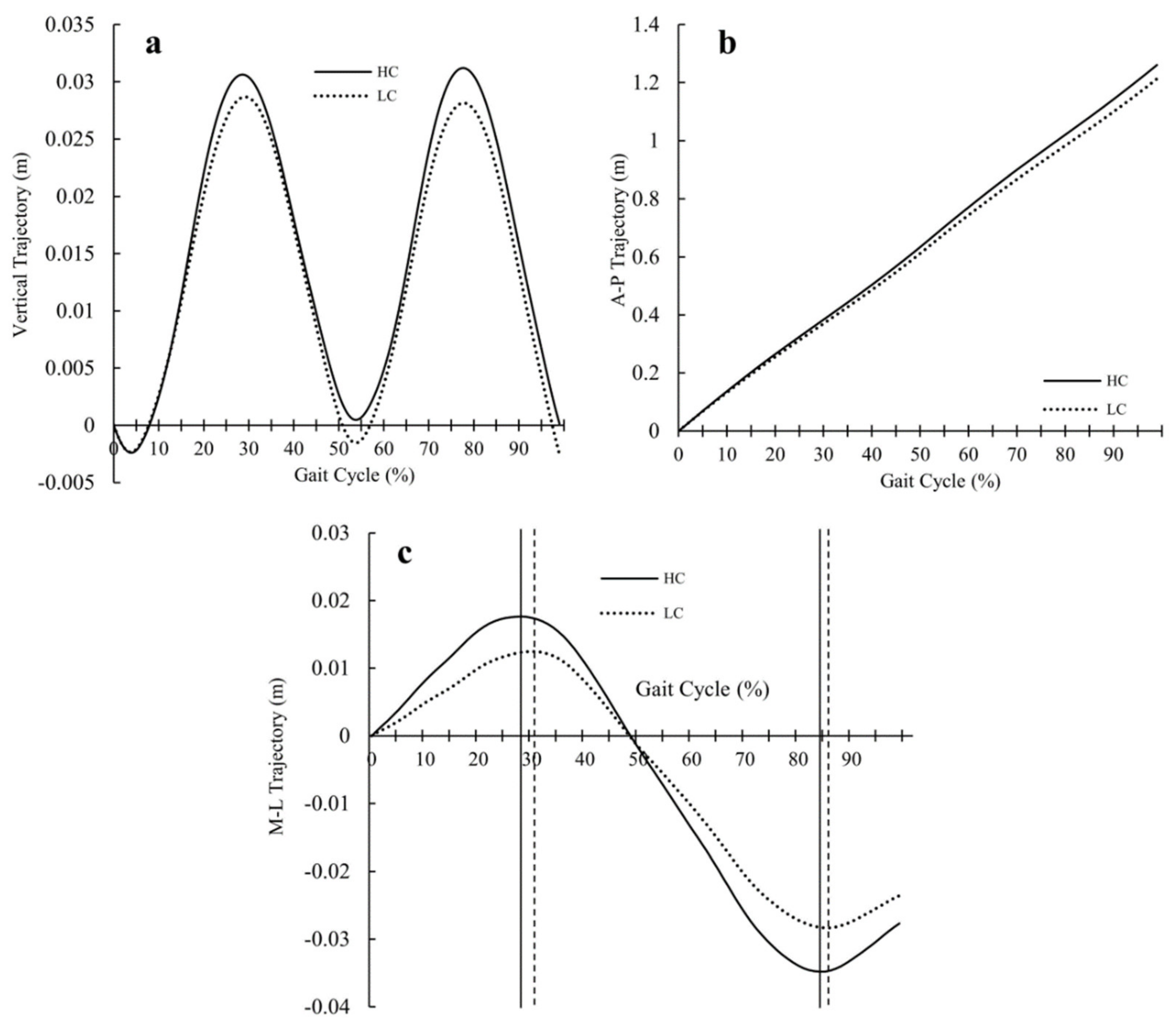
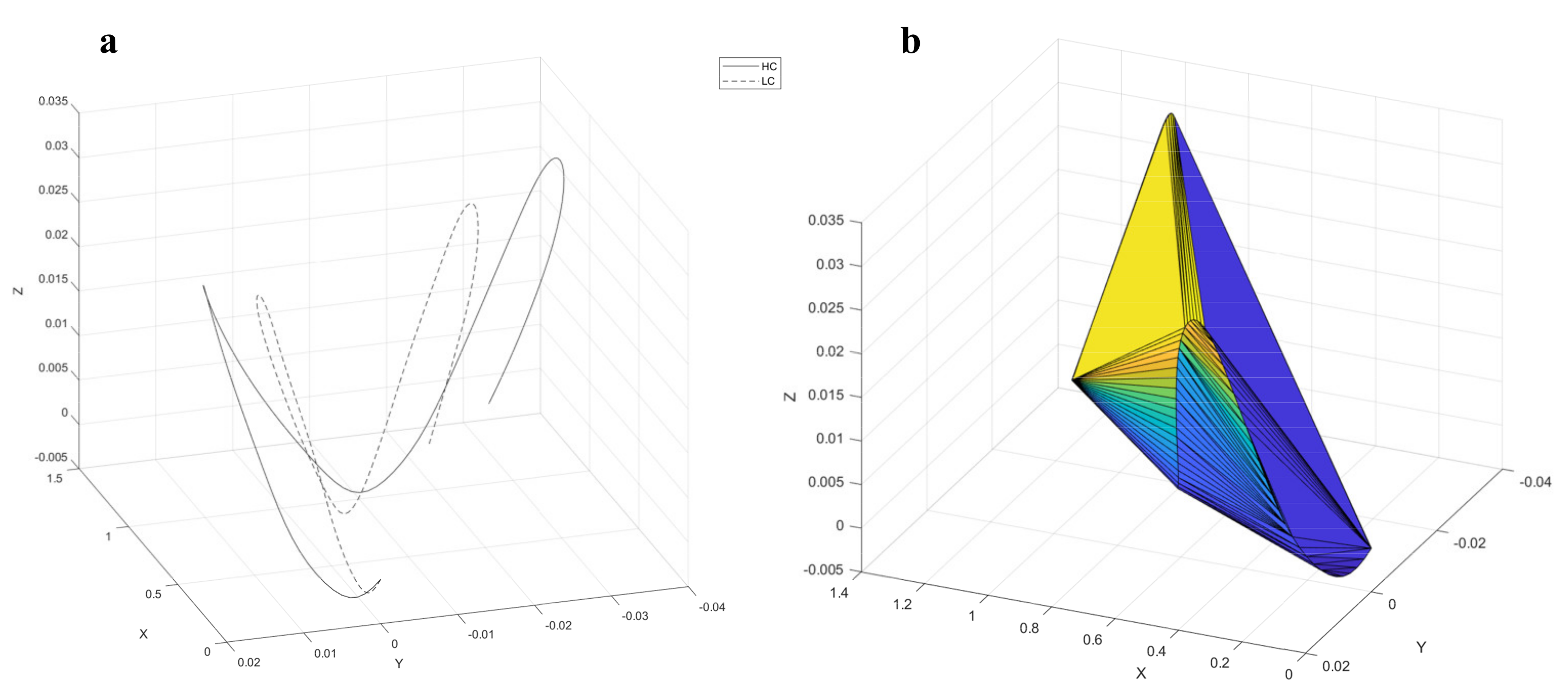
3.1.3. Level Walking
3.1.4. Audiological Function
3.1.5. Balance Function
3.2. Predictive Ablity and Logistic Regression Model Design
- (1)
- Age = 0.712 (CI 95% 0.579~0.844)
- (2)
- SLS = 0.711 (CI 95% 0.569~0.853)
- (3)
- PSI = 0.725 (CI 95% 0.577~0.873)
- (4)
- APSI = 0.705 (CI 95% 0.555~0.856)
- (5)
- SRS error = 0.732 (CI 95% 0.585~0.879)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). WHO Dementia. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 20 November 2020).
- Ewers, M.; Sperling, R.A.; Klunk, W.E.; Weiner, M.W.; Hampel, H. Neuroimaging markers for the prediction and early diagnosis of Alzheimer’s disease dementia. Trends Neurosci. 2011, 34, 430–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Querbes, O.; Aubry, F.; Pariente, J.; Lotterie, J.-A.; Demonet, J.-F.; Duret, V.; Puel, M.; Berry, I.; Fort, J.-C.; Celsis, P.; et al. Early diagnosis of Alzheimer’s disease using cortical thickness: Impact of cognitive reserve. Brain 2009, 132, 2036–2047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsolaki, M. Clinical workout for the early detection of cognitive decline and dementia. Eur. J. Clin. Nutr. 2014, 68, 1186–1191. [Google Scholar] [CrossRef] [PubMed]
- McGrath, R.; Robinson-Lane, S.G.; Clark, B.C.; Suhr, J.A.; Giordani, B.J.; Vincent, B.M. Self-Reported Dementia-Related Diagnosis Underestimates the Prevalence of Older Americans Living with Possible Dementia. J. Alzheimer’s Dis. 2021, 82, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Albers, M.W.; Gilmore, G.C.; Kaye, J.; Murphy, C.; Wingfield, A.; Bennett, D.A.; Boxer, A.L.; Buchman, A.S.; Cruickshanks, K.J.; Devanand, D.P.; et al. At the interface of sensory and motor dysfunctions and Alzheimer’s disease. Alzheimer’s Dement. 2015, 11, 70–98. [Google Scholar] [CrossRef] [Green Version]
- Deal, J.A.; Betz, J.; Yaffe, K.; Harris, T.; Purchase-Helzner, E.; Satterfield, S.; Pratt, S.; Govil, N.; Simonsick, E.M.; Lin, F.R.; et al. Hearing Impairment and Incident Dementia and Cognitive Decline in Older Adults: The Health ABC Study. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2016, 72, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Paik, J.-S.; Ha, M.; Jung, Y.H.; Kim, G.-H.; Han, K.-D.; Kim, H.-S.; Lim, D.H.; Na, K.-S. Low vision and the risk of dementia: A nationwide population-based cohort study. Sci. Rep. 2020, 10, 9109. [Google Scholar] [CrossRef]
- Yamada, Y.; Denkinger, M.D.; Onder, G.; Henrard, J.-C.; van der Roest, H.G.; Finne-Soveri, H.; Richter, T.; Vlachova, M.; Bernabei, R.; Topinkova, E. Dual Sensory Impairment and Cognitive Decline: The Results From the Shelter Study. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2016, 71, 117–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maharani, A.; Dawes, P.; Nazroo, J.; Tampubolon, G.; Pendleton, N. Visual and hearing impairments are associated with cognitive decline in older people. Age Ageing 2018, 47, 575–581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taniguchi, Y.; Yoshida, H.; Fujiwara, Y.; Motohashi, Y.; Shinkai, S. A Prospective Study of Gait Performance and Subsequent Cognitive Decline in a General Population of Older Japanese. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2012, 67, 796–803. [Google Scholar] [CrossRef] [Green Version]
- Verghese, J.; Wang, C.; Lipton, R.B.; Holtzer, R.; Xue, X. Quantitative gait dysfunction and risk of cognitive decline and dementia. J. Neurol. Neurosurg. Psychiatry 2007, 78, 929–935. [Google Scholar] [CrossRef] [PubMed]
- Doi, T.; Makizako, H.; Tsutsumimoto, K.; Hotta, R.; Nakakubo, S.; Makino, K.; Suzuki, T.; Shimada, H. Combined effects of mild cognitive impairment and slow gait on risk of dementia. Exp. Gerontol. 2018, 110, 146–150. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.C.S.; Marshall, C.R.; Weil, R.S.; Bamiou, D.-E.; Hardy, C.J.D.; Warren, J.D. Hearing and dementia: From ears to brain. Brain 2021, 144, 391–401. [Google Scholar] [CrossRef]
- Diamond, A. Executive Functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dorfman, M.; Herman, T.; Brozgol, M.; Shema, S.; Weiss, A.; Hausdorff, J.M.; Mirelman, A. Dual-Task Training on a Treadmill to Improve Gait and Cognitive Function in Elderly Idiopathic Fallers. J. Neurol. Phys. Ther. 2014, 38, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.; Park, J.S.; Yu, K.H.; Lee, B.C. A Reliability, Validity, and Normative Study of the Korean-Montreal Cognitive Assessment(K-MoCA) as an Instrument for Screening of Vascular Cognitive Impairment(VCI). Korean J. Clin. Psychol. 2009, 28, 549–562. [Google Scholar] [CrossRef]
- Bidabadi, S.S.; Murray, I.; Lee, G.Y.F. Validation of foot pitch angle estimation using inertial measurement unit against marker-based optical 3D motion capture system. Biomed. Eng. Lett. 2018, 8, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Lin, F.R.; Yaffe, K.; Xia, J.; Xue, Q.-L.; Harris, T.B.; Purchase-Helzner, E.; Satterfield, S.; Ayonayon, H.N.; Ferrucci, L.; Simonsick, E.M.; et al. Hearing Loss and Cognitive Decline in Older Adults. JAMA Intern. Med. 2013, 173, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Wang, J.; Wei, J. AVC: Selecting discriminative features on basis of AUC by maximizing variable complementarity. BMC Bioinform. 2017, 18 (Suppl. 3), 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mandrekar, J.N. Receiver Operating Characteristic Curve in Diagnostic Test Assessment. J. Thorac. Oncol. 2010, 5, 1315–1316. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.W.; Park, J.H.; Kim, M.-H.; Kim, M.D.; Kim, B.-J.; Kim, S.-K.; Kim, J.L.; Moon, S.W.; Bae, J.N.; Woo, J.I.; et al. A Nationwide Survey on the Prevalence of Dementia and Mild Cognitive Impairment in South Korea. J. Alzheimer’s Dis. 2011, 23, 281–291. [Google Scholar] [CrossRef] [Green Version]
- Van Der Flier, W.M. Epidemiology and risk factors of dementia. J. Neurol. Neurosurg. Psychiatry 2005, 76 (Suppl. 5), v2–v7. [Google Scholar] [CrossRef] [Green Version]
- Meyer, G.; Ayalon, M. Biomechanical aspects of dynamic stability. Eur. Rev. Aging Phys. Act. 2006, 3, 29–33. [Google Scholar] [CrossRef] [Green Version]
- Perry, J.; Burnfield, J.M. Phases of Gait in Gait Analysis: Normal And Pathological Function, 1st ed.; SLACK Inc.: Thorofare, NJ, USA, 1992; pp. 9–16. [Google Scholar]
- Kido, T.; Tabara, Y.; Igase, M.; Ochi, N.; Uetani, E.; Nagai, T.; Yamamoto, M.; Taguchi, K.; Miki, T.; Kohara, K. Postural Instability Is Associated with Brain Atrophy and Cognitive Impairment in the Elderly: The J-SHIPP Study. Dement. Geriatr. Cogn. Disord. 2010, 29, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Wang, W.; Wang, H.; Sun, Y. Sentence comprehension in patients with dementia of the Alzheimer’s type. PeerJ 2019, 7, e8181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.K.; Sung, J.E.; Jeong, J.H. Effects of syntactic complexity on sentence comprehension in persons with mild cognitive impairment and dementia of Alzheimer’s type. Commun. Sci. Disord. 2012, 17, 338–355. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Score (/Max) | ALL (n = 57) | HC (n = 39) | LC (n = 18) | p-Value * |
|---|---|---|---|---|
| MEAN (SD) | MEAN (SD) | MEAN (SD) | ||
| Age (years) | 74.42 (4.56) | 73.46 (4.51) | 76.5 (4.04) | 0.01 * |
| Height (cm) | 166.96 (5.53) | 167.15 (5.91) | 166.56 (4.73) | 0.708 |
| Weight (kg) | 67.34 (8.42) | 67.4 (8.8) | 67.19 (7.76) | 0.932 |
| Education (years) | 13.07 (3.41) | 13.1 (3.35) | 13.0 (3.63) | 0.917 |
| Score (/Max) | HC (n = 39) | LC (n = 18) | p-Value * |
|---|---|---|---|
| MEAN (SD) | MEAN (SD) | ||
| MoCA score (/30) | 23.3 (2.7) | 17.44 (3.4) | <0.001 * |
| Visuospatial executive function (/5) | 4.13 (1.0) | 2.39 (0.9) | <0.001 * |
| Naming (/3) | 2.89 (0.3) | 2.67 (0.5) | 0.035 * |
| Attention (/6) | 5.28 (0.76) | 4.44 (1.1) | 0.005 * |
| Language (/3) | 2.36 (0.67) | 1.44 (1.15) | 0.003 * |
| Abstraction (/2) | 1.02 (0.81) | 0.56 (0.51) | 0.038 * |
| Delayed recall (/5) | 1.79 (1.28) | 0.56 (0.78) | 0.001 * |
| Orientation (/6) | 5.82 (2.72) | 5.39 (3.4) | 0.055 |
| Variable | HC (n = 39) | LC (n = 18) | p-Value * |
|---|---|---|---|
| MEAN (SD) | MEAN (SD) | ||
| LR (%) | 10.55 (1.13) | 11.44 (1.49) | 0.016 * |
| MS (%) | 21.16 (2.51) | 19.67 (2.67) | 0.217 |
| TS (%) | 18.34 (2.84) | 18.91 (2.64) | 0.693 |
| PS (%) | 11.05 (1.13) | 11.77 (1.06) | 0.065 |
| SLS (%) | 39.5 (1.25) | 38.6 (1.30) | 0.014 * |
| DLS (%) | 21.61 (2.04) | 23.2 (2.29) | 0.011 * |
| SW (%) | 38.88 (1.32) | 38.21 (1.28) | 0.250 |
| COM volume (cm3) | 442.07 (193.08) | 344.37 (168.10) | 0.039 * |
| Variable | HC (n = 39) | LC (n = 18) | p-Value * |
|---|---|---|---|
| MEAN (SD) | MEAN (SD) | ||
| PTA R | 23.5 (10.05) | 26.4 (10.50) | 0.290 |
| PTA L | 23.38 (10.84) | 32.3 (19.32) | 0.075 |
| SRT | 19.23 (8.61) | 25 (13.26) | 0.221 |
| WRS | 76.99 (12.14) | 71.61 (13.07) | 0.140 |
| WRS error | 11.05 (5.02) | 14.33 (6.62) | 0.223 |
| SRS | 98.27 (1.94) | 95.2 (4.85) | 0.063 |
| SRS error | 1.38 (1.55) | 4 (3.91) | 0.049 * |
| Variable | HC (n = 39) | LC (n = 18) | p-Value * |
|---|---|---|---|
| MEAN (SD) | MEAN (SD) | ||
| PSI | 0.68 (0.37) | 1.16 (0.86) | 0.006 * |
| APSI | 0.54 (0.36) | 0.86 (0.64) | 0.012 * |
| MLSI | 0.27 (0.15) | 0.59 (0.62) | 0.017 * |
| PV | β | S.E. | p-Value | OR | 95% CI of OR | AUC (95% CI) | ||
|---|---|---|---|---|---|---|---|---|
| Model 1 | SLS adjusted | −0.582 | 0.289 | 4.068 | 0.044 * | 0.559 | 0.317 to 0.984 | 0.832 (0.725~0.938) |
| PSI < 0.75 | −1.708 | 0.747 | 5.227 | 0.022 * | 0.181 | 0.042 to 0.784 | ||
| SRS error | 0.348 | 0.172 | 4.098 | 0.043 * | 1.416 | 1.011 to 1.983 | ||
| Constant | 1.71 | 1.199 | 0.02 | 0.887 | 1.186 | |||
| Model 2 | SLS adjusted | −0.584 | 0.290 | 4.048 | 0.044 * | 0.557 | 0.315 to 0.985 | 0.840 (0.735~0.946) |
| PSI < 0.75 | −1.59 | 0.765 | 4.321 | 0.038 * | 0.204 | 0.045 to 0.913 | ||
| SRS error | 0.322 | 0.176 | 3.347 | 0.067 | 1.380 | 0.977 to 1.948 | ||
| Age adjusted | 0.061 | 0.079 | 0.603 | 0.438 | 1.063 | 0.911 to 1.242 | ||
| Constant | −0.327 | 1.366 | 0.057 | 0.811 | 0.721 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kostic, E.; Kwak, K.; Kim, D. Association of Posture, Gait, and Auditory Functioning with Cognitive Status in a Cohort of Community-Dwelling Older Adults. Appl. Sci. 2021, 11, 9970. https://doi.org/10.3390/app11219970
Kostic E, Kwak K, Kim D. Association of Posture, Gait, and Auditory Functioning with Cognitive Status in a Cohort of Community-Dwelling Older Adults. Applied Sciences. 2021; 11(21):9970. https://doi.org/10.3390/app11219970
Chicago/Turabian StyleKostic, Emilija, Kiyoung Kwak, and Dongwook Kim. 2021. "Association of Posture, Gait, and Auditory Functioning with Cognitive Status in a Cohort of Community-Dwelling Older Adults" Applied Sciences 11, no. 21: 9970. https://doi.org/10.3390/app11219970
APA StyleKostic, E., Kwak, K., & Kim, D. (2021). Association of Posture, Gait, and Auditory Functioning with Cognitive Status in a Cohort of Community-Dwelling Older Adults. Applied Sciences, 11(21), 9970. https://doi.org/10.3390/app11219970