
Testing a Single-Case Experimental Design to Study Dynamic Light Exposure in People with Dementia Living at Home

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Procedure
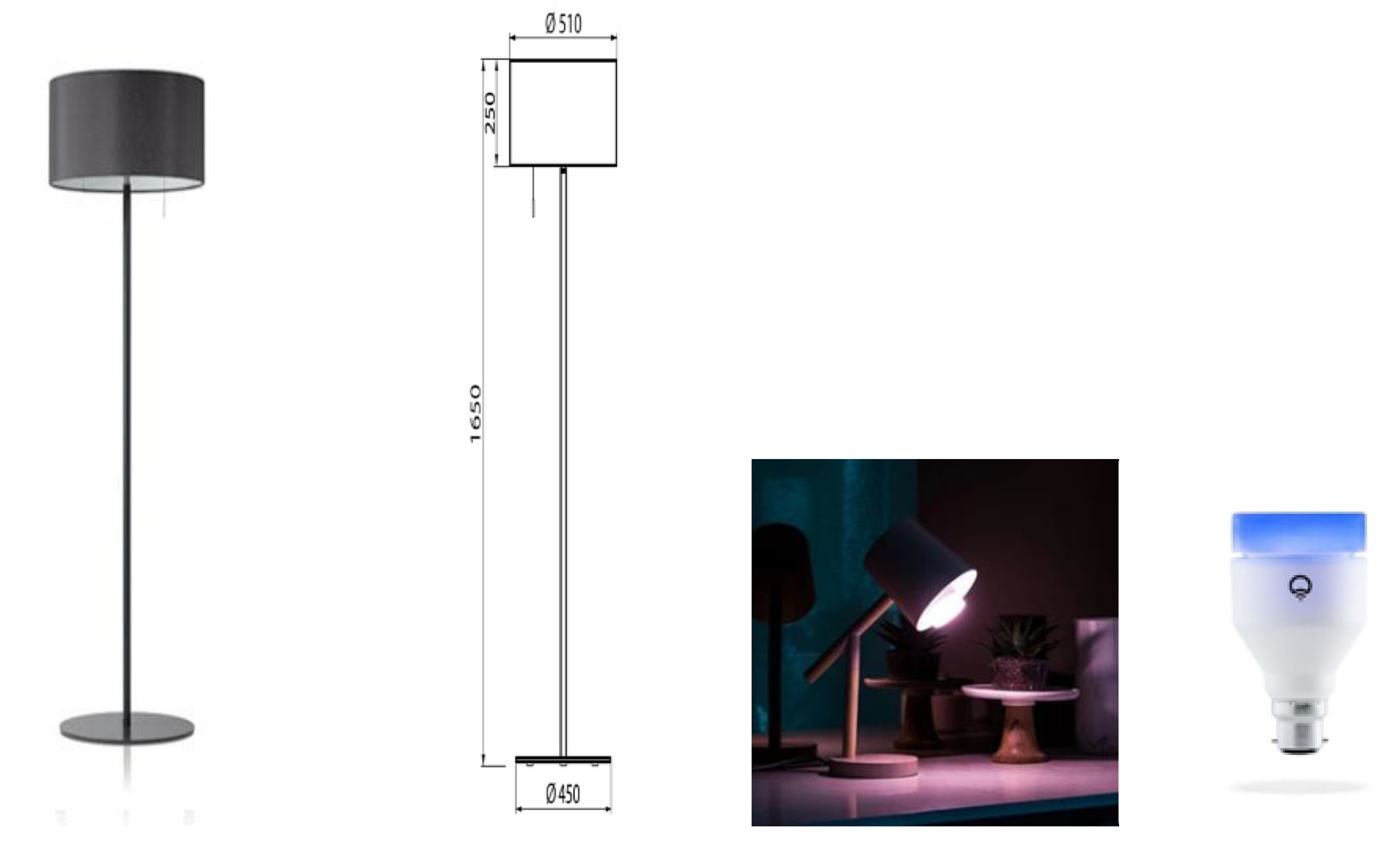
2.4. Lighting Intervention
2.5. Measurements
2.5.1. Baseline Light Measurements of the Home Situation Using a Spectrometer
2.5.2. Personal Light Measurements during the Day Using a Sensor Button
2.6. Statistical Analyses
2.6.1. Preparations
2.6.2. Randomization Tests
Randomization Test between Participants for the Spectrometer Data
Randomization Test within Participants for the Sensor Button Data
2.6.3. User Experiences
3. Results
3.1. Effectiveness of the Light Intervention
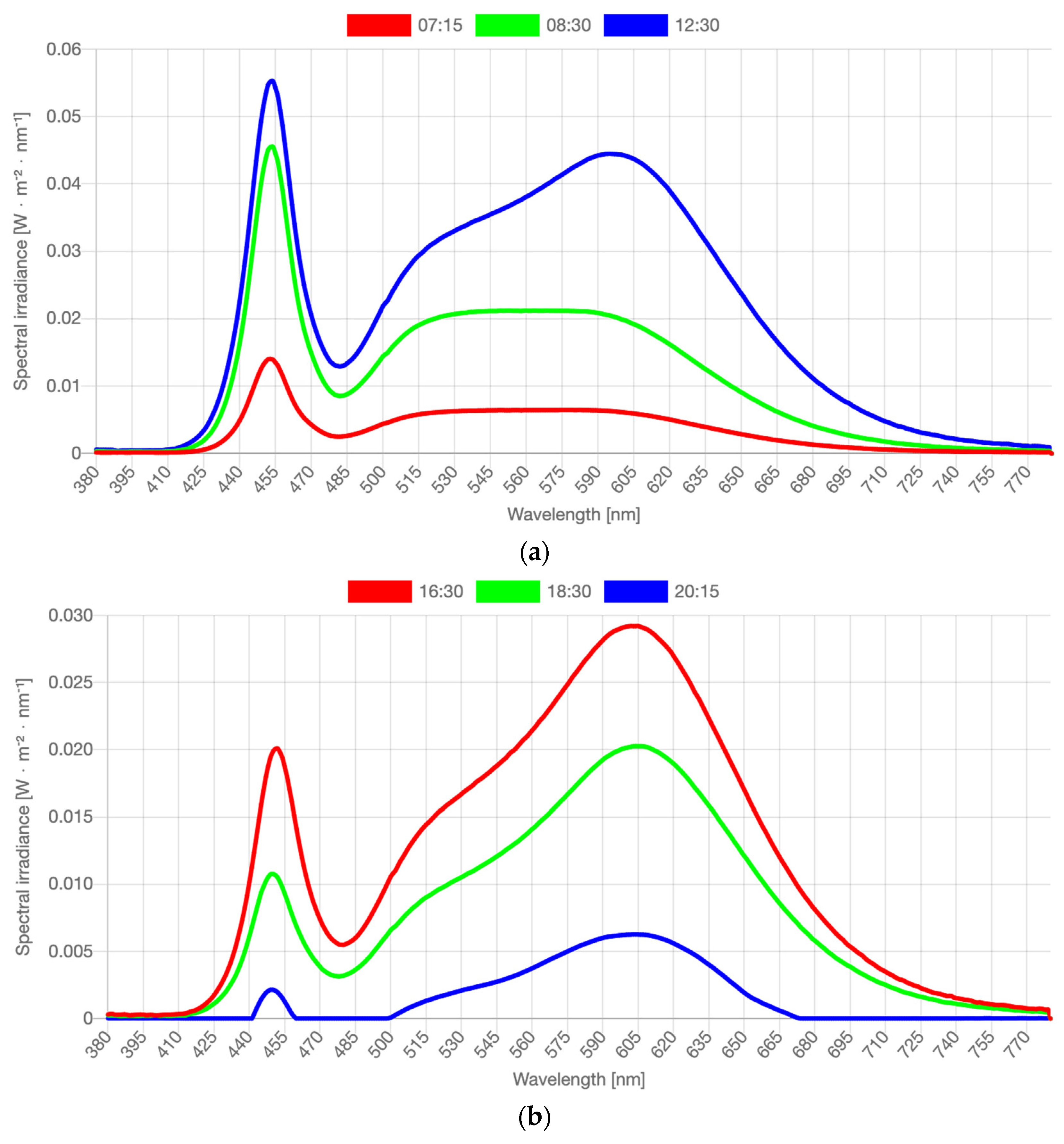
3.1.1. Spectrometer
3.1.2. Spectrometer Conclusion
3.1.3. Personal Light Exposure Measured with Wearable Sensors
3.1.4. Light Intensity (lx)
Light Intensity Conclusion
3.1.5. Randomization Test per Daypart
Daypart Differentiation Conclusion
3.1.6. Randomization Test of Seasonal Effects
3.1.7. Seasonal Effects Conclusion
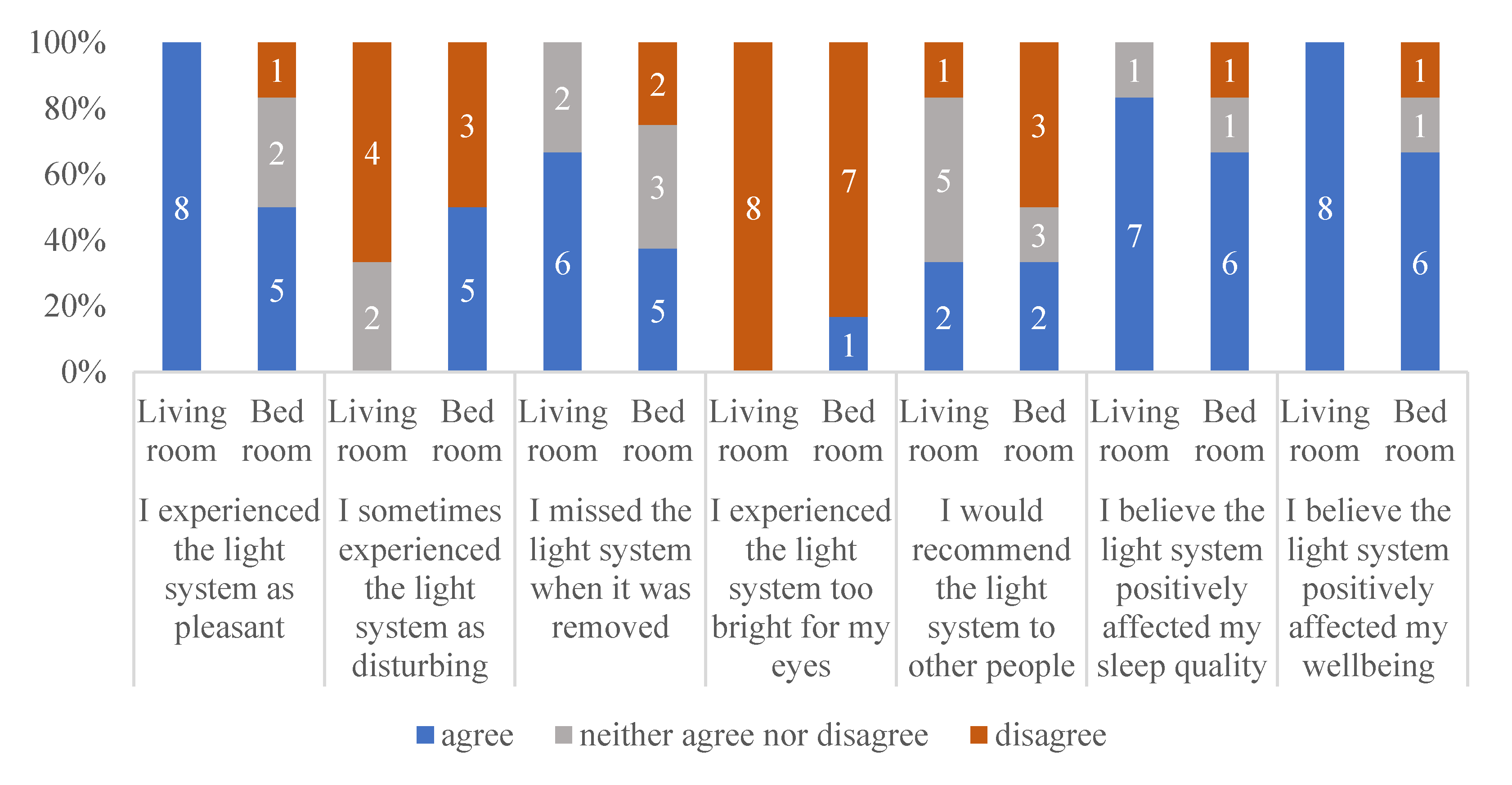
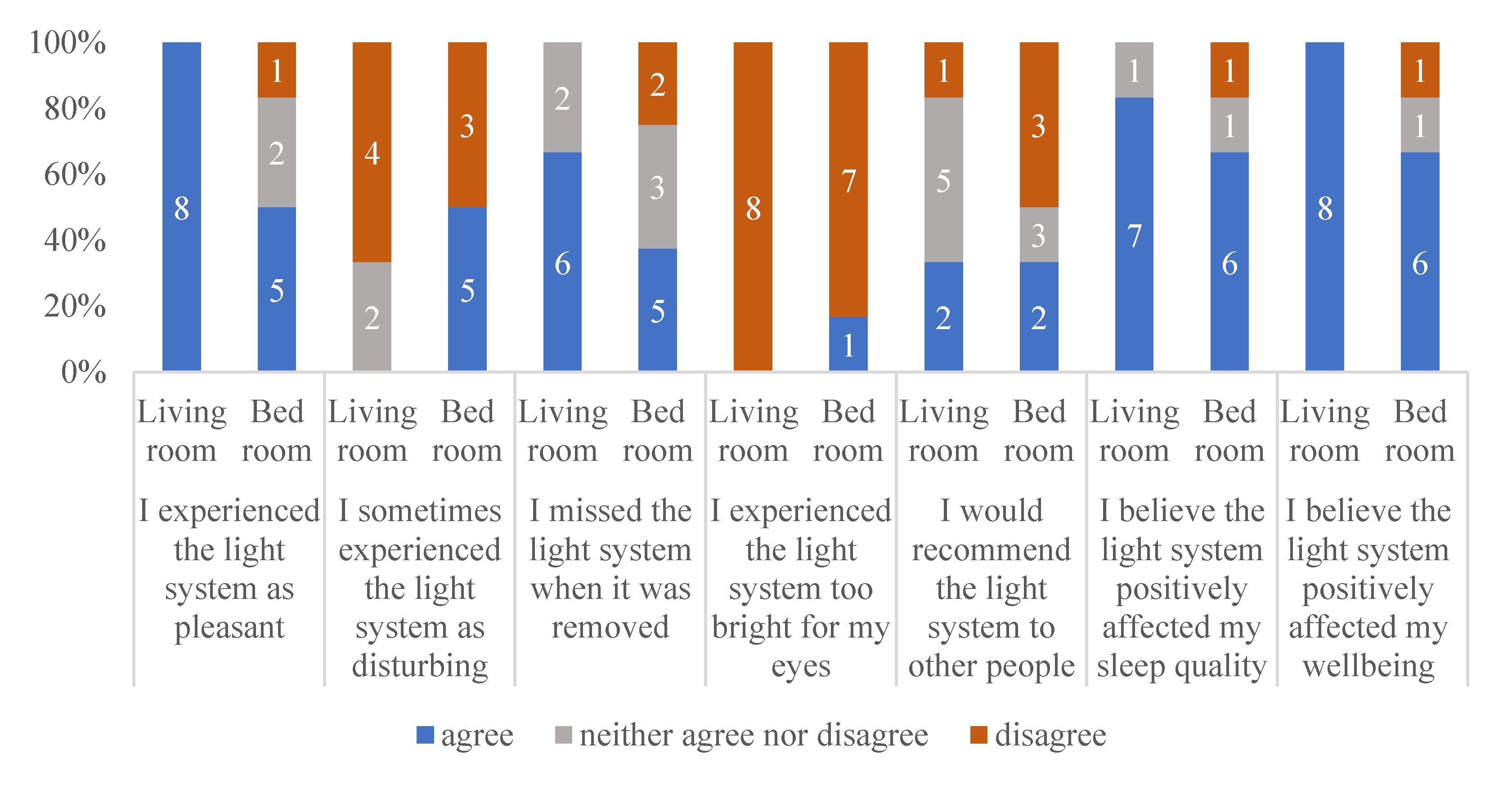
3.2. User Experiences
4. Discussion
4.1. Reflection on the Results
4.2. Reflection on the Used Design
4.3. Lessons Learned
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Figueiro, M.G. Light, sleep and circadian rhythms in older adults with Alzheimer’s disease and related dementias. Neurodegener. Dis. Manag. 2017, 7, 119–145. [Google Scholar] [CrossRef] [Green Version]
- Boyce, P.R. Lighting for the elderly. Technol. Disabil. 2003, 15, 165–180. [Google Scholar] [CrossRef]
- Shikder, S.; Mourshed, M.; Price, A. Therapeutic lighting design for the elderly: A review. Perspect. Public Health 2012, 132, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Wahl, S.; Engelhardt, M.; Schaupp, P.; Lappe, C.; Ivanov, I.V. The inner clock: Blue light sets the human rhythm. J. Biophotonics 2019, 12, e201900102. [Google Scholar] [CrossRef] [PubMed]
- Abbott, A. Restless nights, listless days. Nature 2008, 245, 896–898. [Google Scholar] [CrossRef] [PubMed]
- Riemersma, R.F. Light and melatonin: Effect on sleep, mood and cognition in demented elderly. Neurobiol. Aging 2004, 25, 194. [Google Scholar] [CrossRef]
- Harper, D.G.; Volicer, L.; Stopa, E.G.; McKee, A.C.; Gitta, M.; Satlin, A. Disturbance of endogenous circadian rhythm in aging and Alzheimer disease. Am. J. Geriatr. Psychiatry 2005, 13, 359–368. [Google Scholar] [CrossRef] [PubMed]
- Hatfield, C.F.; Herbert, J.; van Someren, E.J.W.; Hodges, J.R.; Hastings, M.H. Disrupted daily activity/rest cycles in relation to daily cortisol rhythms of home-dwelling patients with early Alzheimer’s dementia. Brain 2004, 127, 1061–1074. [Google Scholar] [CrossRef] [Green Version]
- Bantry White, E.; Montgomery, P. Supporting people with dementia to walkabout safely outdoors: Development of a structured model of assessment. Health Soc. Care Community 2016, 24, 73–484. [Google Scholar] [CrossRef]
- Skene, D.J.; Swaab, D.F. Melatonin rhythmicity: Effect of age and Alzheimer’s disease. Exp. Gerontol. 2003, 38, 199–206. [Google Scholar] [CrossRef]
- Goudriaan, I.; van Boekel, L.C.; Verbiest, M.; van Hoof, J.; Luijkx, K.G. Dementia Enlightened?! A Systematic Literature Review of the Influence of Indoor Environmental Light on the Health of Older Persons with Dementia in Long-Term Care Facilities. Clin. Interv. Aging 2021, 16, 909–937. [Google Scholar] [CrossRef]
- Hanford, N.; Figueiro, M. Light therapy and Alzheimer’s disease and related dementia: Past, present, and future. J. Alzheimer Dis. 2013, 33, 913–922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, J.; Abaraogu, U.O.; Ellis, G. A systematic review of the physical activity levels of acutely ill older adults in Hospital At Home settings: An under-researched field. Eur. Geriatr. Med. 2020, 12, 227–238. [Google Scholar] [CrossRef] [PubMed]
- White, M.D.; Ancoli-Israel, S.; Wilson, R.R. Senior living environments: Evidence-based lighting design strategies. HERD Health Environ. Res. Des. J. 2013, 7, 60–78. [Google Scholar] [CrossRef]
- Aarts, M.P.J.; Stapel, J.C.; Schoutens, T.A.M.C.; van Hoof, J. Exploring the impact of natural light exposure on sleep of healthy older adults: A field study. J. Daylighting 2018, 5, 4–20. [Google Scholar] [CrossRef] [Green Version]
- Kompier, M.E.; Smolders, K.C.H.J.; de Kort, Y.A.W. Abrupt light transitions in illuminance and correlated colour temperature result in different temporal dynamics and interindividual variability for sensation, comfort and alertness. PLoS ONE 2021, 16, e0243259. [Google Scholar] [CrossRef] [PubMed]
- Kompier, M.E.; Smolders, K.C.H.J.; de Kort, Y.A.W. A systematic literature review on the rationale for and effects of dynamic light scenarios. Build Environ. 2020, 186, 107326. [Google Scholar] [CrossRef]
- Figueiro, M.G.; Hamner, R.; Higgins, P.; Hornick, T.; Rea, M.S. Field measurements of light exposures and circadian disruption in two populations of older adults. J. Alzheimer Dis. 2012, 31, 711–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blume, C.; Garbazza, C.; Spitschan, M. Effects of light on human circadian rhythms, sleep and mood. Somnologie 2019, 23, 147–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fontana Gasio, P.; Kräuchi, K.; Cajochen, C.; van Someren, E.J.W.; Amrhein, I.; Pache, M.; Savaskan, E.; Wirz-Justice, A. Dawn-dusk simulation light therapy of disturbed circadian rest-activity cycles in demented elderly. Exp. Gerontol. 2003, 38, 207–216. [Google Scholar] [CrossRef]
- Figueiro, M.G.; Hunter, C.M.; Higgins, P.; Hornick, T.; Jones, G.E.; Plitnick, B.; Brons, J.; Rea, M.S. Tailored Lighting Intervention for Persons with Dementia and Caregivers Living at Home. Sleep Health 2015, 1, 322–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figueiro, M.G.; Plitnick, B.; Rea, M.S. A self-luminous light table for persons with Alzheimer’s disease. Light. Res. Technol. 2016, 48, 253–259. [Google Scholar] [CrossRef] [Green Version]
- Riemersma-van Der Lek, R.F.; Swaab, D.F.; Twisk, J.; Hol, E.M.; Hoogendijk, W.J.; Van Someren, E.J. Effect of bright light and melatonin on cognitive and noncognitive function in elderly residents of group care facilities: A randomized controlled trial. JAMA 2008, 299, 2642–2655. [Google Scholar] [CrossRef] [PubMed]
- Lieverse, R.; Van Someren, E.J.; Nielen, M.M.; Uitdehaag, B.M.; Smit, J.H.; Hoogendijk, W.J. Bright light treatment in elderly patients with nonseasonal major depressive disorder: A randomized placebo-controlled trial. Arch. Gen. Psychiatry 2011, 68, 61–70. [Google Scholar] [CrossRef]
- Van Hoof, J.; Aarts, M.P.; Rense, C.G.; Schoutens, A.M. Ambient bright light in dementia: Effects on behaviour and circadian rhythmicity. Build. Environ. 2009, 44, 146–155. [Google Scholar] [CrossRef]
- Gul, S. Chromo therapy—An Effective Treatment Option or Just a Myth? Critical Analysis on the Effectiveness of Chromo therapy. Am. Res. J. Pharm. 2015, 1, 62–70. [Google Scholar]
- Nioi, A.; Roe, J.; Gow, A.; McNair, D.; Spinall, P. Seasonal Differences in Light Exposure and the Associations With Health and Well-Being in Older Adults: An Exploratory Study. HERD Health Environ. Res. Des. J. 2017, 10, 64–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sloane, P.D.; Figueiro, M.; Garg, S.; Cohen, L.W.; Reed, D.; Williams, C.S.; Preisser, J.; Zimmerman, S. Effect of home-based light treatment on persons with dementia and their caregivers. Light. Res. Technol. 2015, 47, 161–176. [Google Scholar] [CrossRef] [PubMed]
- Kinnunen, K.M.; Vikhanova, A.; Livingston, G. The management of sleep disorders in dementia: An update. Curr. Opin. Psychiatry 2017, 30, 491–497. [Google Scholar] [CrossRef]
- Peeters, S.T.; Smolders, K.C.; de Kort, Y.A. What you set is (not) what you get: How a light intervention in the field translates to personal light exposure. Build. Environ. 2020, 185, 107288. [Google Scholar] [CrossRef]
- Dallery, J.; Cassidy, R.N.; Raiff, B.R. Single-case experimental designs to evaluate novel technology-based health interventions. J. Med. Internet Res. 2013, 15, e22. [Google Scholar] [CrossRef] [PubMed]
- Krasny-Pacini, A.; Evans, J. Single-case experimental designs to assess intervention effectiveness in rehabilitation: A practical guide. Ann. Phys. Rehabil. Med. 2018, 61, 164–179. [Google Scholar] [CrossRef]
- Smith, J.D. Single-case experimental designs: A systematic review of published research and current standards. Psychol. Methods 2012, 17, 510–550. [Google Scholar] [CrossRef] [Green Version]
- Sekiguchi, H.; Iritani, S.; Fujita, K. Bright light therapy for sleep disturbance in dementia is most effective for mild to moderate Alzheimer’s type dementia: A case series. Psychogeriatrics 2017, 5, 275–281. [Google Scholar] [CrossRef]
- Rasquin, S.M.C.; Willems, C.; De Vlieger, S.; Geers, R.P.J.; Soede, M. The Use of Technical Devices to Support Outdoor Mobility of Dementia Patients. Technol. Disabil. 2007, 19, 113–120. [Google Scholar] [CrossRef]
- Hein, A.; Krüger, F.; Bader, S.; Eschholz, P.; Kirste, T. Challenges of Collecting Empirical Sensor Data From People with Dementia in a Field Study. In Proceedings of the 2017 IEEE International Conference on Pervasive Computing and Communications Workshops (PerCom Workshops), Kona, HI, USA, 13–17 March 2017; pp. 22–25. [Google Scholar] [CrossRef]
- Corrà, M.F.; Warmerdam, E.; Vila-Chã, N.; Maetzler, W.L.; Maia, L. Wearable Health Technology to Quantify the Functional Impact of Peripheral Neuropathy on Mobility in Parkinson’s Disease: A Systematic Review. Sensors 2020, 20, 6627. [Google Scholar] [CrossRef]
- Bonci, T.; Keogh, A.; Del Din, S.; Scott, K.C.; Mazzà, C. An Objective Methodology for the Selection of a Device for Continuous Mobility Assessment. Sensors 2020, 20, 6509. [Google Scholar] [CrossRef] [PubMed]
- Kieboom, R.; Bongers, I.; Mark, R.; Snaphaan, L. Protocol: Innovate Dementia 2.0: A user-driven living lab for assistive technology to support people living at home with dementia. JMIR Res. Protoc. 2018, 8, e10952. [Google Scholar] [CrossRef]
- World Medical Association Declaration of Helsinki. Ethical Principles for Medical Research Involving Human Subjects; Bulletin of the World Health Organization; World Health Organization: Geneva, Switzerland, 2001; Volume 79, pp. 373–374. [CrossRef] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- CIE; International Commission on Illumination. CIE Position Statement on Non-Visual Effects of Light—Recommending Proper Light at the Proper Time. Available online: https://cie.co.at/files/CIE%20Position%20Statement%20-%20Proper%20Light%20at%20the%20Proper%20Time%20(2019)_0.pdf (accessed on 17 October 2021).
- Open Science Framework OSF Home Page. Available online: https://osf.io/5au6g/?view_only=5083989abe0f424487c8f4529afcf10b (accessed on 17 October 2021). [CrossRef]
- Spitschan, M. Luox: Platform for Calculating Quantities Related to Light and Lighting [Software]. Available online: https://luox.app/ (accessed on 17 October 2021).
- Spitschan, M.; Mead, J.; Roos, C.; Lowis, C.; Griffiths, B.; Mucur, P.; Herf, M. Luox: Novel Validated Open-Access and Open-Source Web Platform for Calculating and Sharing Physiologically Relevant Quantities for Light and Lighting. Available online: https://wellcomeopenresearch.org (accessed on 17 October 2021). [CrossRef]
- Bouwmeester, S.; Jongerling, J. Power of a randomization test in a single case multiple baseline AB design. PLoS ONE 2020, 15, e0228355. [Google Scholar] [CrossRef] [PubMed]
- Onghena, P.; Edgington, E.S. Customization of pain treatments: Single-case design and analysis. Clin. J. Pain 2005, 21, 56–72. [Google Scholar] [CrossRef]
- Aarts, M.; Duijnhoven, J.; Aries, M.; Rosemann, A.L.P. Performance of personally worn dosimeters to study non-image forming effects of light: Assessment methods. Build. Environ. 2017, 117, 60–72. [Google Scholar] [CrossRef]
- Koninklijk Nederlands Meteorologisch Instituut (KNMI). Available online: https://weerstatistieken.nl/eindhoven/2019/oktober (accessed on 16 June 2021).
- Huang, S.S.; Wang, W.F.; Liao, Y.C. Severity and prevalence of behavioral and psychological symptoms among patients of different dementia stages in Taiwan. Arc. Clin. Psychiatry 2017, 44, 89–93. [Google Scholar] [CrossRef] [Green Version]
- Van Den Kieboom, R.C.; Bongers, I.M.; Mark, R.E.; Snaphaan, L.J. User-Driven Living Lab for Assistive Technology to Support People Living at Home with Dementia: Protocol for Developing Co-Creation-Based Innovations. JMIR Res. Protoc. 2019, 8, e10952. [Google Scholar] [CrossRef] [PubMed]
- Astell, A.; Ellis, M.; Bernardi, L.; Alm, N.; Dye, R.; Gowans, G. Using a touch screen computer to support relationships between people with dementia and caregivers. Interact. Comput. 2010, 22, 267–275. [Google Scholar] [CrossRef]
- Meiland, F.; Innes, A.; Mountain, G. Technologies to Support Community-Dwelling Persons With Dementia: A Position Paper on Issues Regarding Development, Usability, Effectiveness and Cost-Effectiveness, Deployment, and Ethics. JMIR Rehabil. Assist. Technol. 2017, 4, e6376. [Google Scholar] [CrossRef]
- Koskinen, I.; Zimmerman, J. Design Research Through Practice. In Computer Graphics; Elsevier Science Ltd.: Waltham, MA, USA, 2018. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender | Participants | Caregivers |
| Male | 6 | 3 |
| Female | 5 | 8 |
| Dementia type | ||
| Alzheimer’s | 8 | |
| Lewy body | 2 | |
| Frontotemporal | 1 | |
| Relationship with participant | ||
| Spouse | 8 | |
| Daughter (in-law) | 3 | |
| Mean age (SD) | 78.1 (8.56) | 68.2 (11.59) |
| Mean MMSE score (SD) | 24.55 (2.3) |
| Phase | Description | CCT | Task Lighting (Ehorizontal at Lap Level) | Personal Exposure (Evertical at Eye Level) | ||||
|---|---|---|---|---|---|---|---|---|
| From | To | Intensity | Color | Illuminance (lx) | EDImel (lx) | Illuminance (lx) | EDImel (lx) | |
| 7:00 a.m. | 7:30 a.m. | Fast increase | Cool white | 6000 K | 0–1000 | 0–1100 | 0–350 | 0–370 |
| 7:30 a.m. | 9:30 a.m. | Slow increase | Regular white | 6000–4000 K | 1000–2600 | 1100–2300 | 350–850 | 370–770 |
| 9:30 a.m. | 3:30 p.m. | Stable | Regular white | 4000 K | 2600 | 2300 | 850 | 770 |
| 3:30 p.m. | 5:30 p.m. | Slow dimming | Warm white | 4000–3000 K | 2600–1300 | 1700–700 | 850–430 | 580–250 |
| 5:30 p.m. | 7:30 p.m. | Very slow dimming | Warm white | 3000 K | 1300–650 | 800–300 | 430–220 | 270–100 |
| 7:30 p.m. | 9:00 p.m. | Very slow dimming | Very warm white | 2500–2250 K | 350–0 | 115–0 | 115–0 | 40–0 |
| Illuminance (in lx) | CCT (in lxK) | EDImel (in lx) | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Kitchen | Bedroom | Living Room | Kitchen | Bedroom | Living Room | Kitchen | Bedroom | Living Room | ||||||||||
| A1 | B1 | A1 | B1 | A1 | B1 | A1 | B1 | A1 | B1 | A1 | B1 | A1 | B1 | A1 | B1 | A1 | B1 | |
| pp1 | 41 | 777 | 41 | 194 | 16 | 540 | 5924 | 4465 | 4516 | 6704 | 3820 | 3152 | 40 | 556 | 32 | 195 | 27 | 263 |
| pp2 | 195 | 818 | 24 | 919 | 3000 | 3550 | 3603 | 3909 | 4444 | 4456 | 4122 | 4104 | 121 | 520 | 19 | 659 | 2131 | 2496 |
| pp3 | 847 | 724 | 3 | 2030 | 23 | 324 | 3149 | 3115 | 1600 | 6214 | 3507 | 4178 | 444 | 378 | 2 | 1829 | 18 | 192 |
| pp4 | 48 | 1280 | 26 | 1320 | 50 | 2140 | 5029 | 4180 | 4057 | 4620 | 4300 | 4218 | 41 | 853 | 18 | 964 | 36 | 1413 |
| pp5 | 48 | 577 | 2 | 2720 | 5 | 1300 | 3270 | 3884 | 1600 | 3424 | 2582 | 4181 | 28 | 371 | 0 | 1377 | 1 | 854 |
| pp7 | 114 | 710 | 47 | 766 | 82 | 575 | 5085 | 4337 | 4782 | 3498 | 4874 | 4247 | 95 | 489 | 38 | 430 | 69 | 390 |
| pp8 | 43 | 982 | 53 | 2120 | 110 | 1360 | 2894 | 4115 | 5368 | 3521 | 4086 | 4193 | 20 | 634 | 47 | 1165 | 72 | 892 |
| pp9 | 37 | 745 | 15 | 2170 | 87 | 761 | 4386 | 4246 | 4814 | 3459 | 5653 | 4386 | 25 | 558 | 13 | 1172 | 81 | 528 |
| pp10 | 11 | 972 | 20 | 766 | 95 | 1210 | 3786 | 4140 | 4690 | 3465 | 5629 | 4453 | 7 | 631 | 16 | 416 | 77 | 860 |
| pp11 | 133 | 528 | 3 | 105 | 35 | 548 | 4388 | 3621 | 1600 | 3357 | 6018 | 3350 | 102 | 319 | 3 | 56 | 34 | 299 |
| pp12 | 8 | 584 | 11 | 1000 | 5 | 140 | 2661 | 3853 | 2429 | 3417 | 3594 | 2983 | 54 | 321 | 1 | 54 | 20 | 248 |
| MeanDif | 674 | 1261 | 813 | −28 | 567 | −431 | 356 | 653 | 599 | |||||||||
| Sig. | <0.001 | <0.001 | 0.03 | 0.532 | 0.169 | 0.88 | 0.002 | 0.004 | <0.001 | |||||||||
| A1 | B1 | A2 | B2 | B1–A1 | A2–B1 | B2–A2 | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Participant 1 | Mean | Md | p2 | Md | p | Md | p | |||
| pp1 | 1.40 | 1.21 | 1.35 | −0.20 | 0.022 * | 0.14 | 0.031 * | |||
| pp2 | 2.29 | 1.84 | 1.50 | −0.45 | 0.007 * | −0.34 | 0.989 | |||
| pp3 | 1.78 | 1.63 | 1.70 | 1.87 | −0.15 | 0.763 | 0.08 | 0.742 | 0.17 | 0.074 * |
| pp4 | 1.79 | 1.79 | 1.58 | 1.82 | 0.00 | 0.481 | −0.21 | 0.035 * | 0.24 | 0.041 * |
| pp5 | 1.80 | 1.67 | 1.63 | 1.61 | −0.13 | 0.853 | −0.04 | 0.339 | −0.02 | 0.551 |
| pp7 | 1.96 | 1.92 | 1.65 | 2.07 | −0.04 | 0.678 | −0.27 | 0.008 * | 0.41 | 0.001 * |
| pp8 | 1.54 | 1.83 | 1.72 | 1.84 | 0.29 | 0.003 * | −0.12 | 0.127 | 0.12 | 0.152 |
| pp9 | 1.44 | 1.55 | 1.65 | 1.77 | 0.11 | 0.151 | 0.11 | 0.816 | 0.12 | 0.161 |
| pp10 | 1.49 | 1.52 | 1.58 | 1.74 | 0.02 | 0.368 | 0.07 | 0.795 | 0.16 | 0.044 * |
| pp11 | 2.28 | 2.35 | 0.07 | 0.247 | ||||||
| pp12 | 1.68 | 1.85 | 1.77 | 2.20 | 0.17 | 0.068 * | −0.08 | 0.268 | 0.43 | 0.002 |
| Overall Effects | ||||||||||
| Mean difference 3 | 0.039 | −0.111 | 0.142 | |||||||
| Cohen’s d 3 | 0.135 | 0.355 | 0.376 | |||||||
| Sum p | 3.612 | 3.159 | 2.046 | |||||||
| Overall p | 0.152 | 0.02 | <0.001 | |||||||
| A1 | B1 | A2 | B2 | B1–A1 | A2–B1 | B2–A2 | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Participant 1 | Mean | Md | p2 | Md | p | Md | p | |||
| pp1 | 3896 | 3208 | 3460 | −687.93 | 0.01 * | 251.97 | 0.131 | |||
| pp2 | 4512 | 4215 | 4300 | −297.42 | 0.01 * | 85.29 | 0.244 | |||
| pp3 | 3779 | 3687 | 3324 | 3566 | −91.78 | 0.608 | −362.91 | 0.03 | 241.96 | 0.059 * |
| pp4 | 4137 | 4259 | 3845 | 4179 | 121.77 | 0.274 | −413.24 | 0.06 * | 333.86 | 0.119 |
| pp5 | 4522 | 4249 | 3814 | 4069 | −273.02 | 0.899 | −435.08 | 0.01 | 254.69 | 0.096 |
| pp7 | 4325 | 3898 | 3688 | 3880 | −426.61 | 0.986 | −210.23 | 0.06 * | 191.60 | 0.061 * |
| pp8 | 4010 | 3844 | 4358 | 4609 | −165.99 | 0.806 | 514.08 | 0.99 | 250.51 | 0.187 |
| pp9 | 3410 | 3847 | 3801 | 4370 | 437.29 | 0.01 | −45.60 | 0.4 | 568.33 | 0.003 |
| pp10 | 4060 | 3859 | 3918 | 4249 | −201.08 | 0.759 | 58.74 | 0.59 | 331.45 | 0.111 |
| pp11 | 3676 | 4006 | 330.16 | 0.058 | ||||||
| pp12 | 3496 | 4115 | 4149 | 4319 | 619.53 | 0.007 * | 33.55 | 0.53 | 170.52 | 0.179 |
| Overall effects | ||||||||||
| Mean difference 3 | 39 | −184 | 268 | |||||||
| Cohen’s d 3 | 0.065 | 0.350 | 0.469 | |||||||
| Sum p | 4.41 | 2.68 | 1.19 | |||||||
| Overall p | 0.458 | 0.01 * | <0.001 * | |||||||
| Morning | Afternoon | Evening | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Md 1 | Sum_p | p | Md | Sum_p | p | Md | Sum_p | p | |
| Illuminance | |||||||||
| B1–A1 | 0.04 | 3.664 | 0.170 | 0.04 | 3.838 | 0.225 | 0.03 | 4.068 | 0.312 |
| B1–A2 | 0.11 | 4.532 | 0.307 | 0.20 | 2.952 | 0.012 * | 0.16 | 3.288 | 0.082 |
| B2–A2 | 0.04 | 4.106 | 0.166 | 0.18 | 2.231 | 0.001 * | 0.29 | 0.949 | <0.001 * |
| CCT | |||||||||
| B1–A1 | 257.66 | 3.181 | 0.065 | −75.4 | 5.024 | 0.724 | −43.88 | 4.496 | 0.498 |
| B1–A2 | 160.08 | 3.945 | 0.126 | 191.62 | 2.739 | 0.006 * | 218.61 | 2.661 | 0.016 * |
| B2–A2 | 68.99 | 3.529 | 0.054 | 125.61 | 3.461 | 0.046 * | 708.14 | 0.350 | <0.001 * |
| Summer–Fall | Winter–Spring | |||||
|---|---|---|---|---|---|---|
| Md 1 | Sum_p | p | Md | Sum_p | p | |
| Illuminance | ||||||
| B1–A1 | −0.05 | 2.276 | 0.904 | 0.23 | 0.861 | 0.004 * |
| B1–A2 | 0.18 | 1.129 | 0.003 * | 0.10 | 1.981 | 0.487 |
| B2–A2 | 0.10 | 1.683 | 0.031 * | 0.18 | 0.398 | 0.001 * |
| CCT | ||||||
| B1–A1 | −107.15 | 2.823 | 0.920 | 203.98 | 1.592 | 0.082 |
| B1–A2 | 401.14 | 0.178 | <0.001 * | −122.24 | 2.541 | 0.819 |
| B2–A2 | 226.56 | 0.725 | <0.001 * | 330.20 | 0.433 | <0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Lieshout-van Dal, E.; Snaphaan, L.; Bouwmeester, S.; de Kort, Y.; Bongers, I. Testing a Single-Case Experimental Design to Study Dynamic Light Exposure in People with Dementia Living at Home. Appl. Sci. 2021, 11, 10221. https://doi.org/10.3390/app112110221
van Lieshout-van Dal E, Snaphaan L, Bouwmeester S, de Kort Y, Bongers I. Testing a Single-Case Experimental Design to Study Dynamic Light Exposure in People with Dementia Living at Home. Applied Sciences. 2021; 11(21):10221. https://doi.org/10.3390/app112110221
Chicago/Turabian Stylevan Lieshout-van Dal, Ellen, Liselore Snaphaan, Samantha Bouwmeester, Yvonne de Kort, and Inge Bongers. 2021. "Testing a Single-Case Experimental Design to Study Dynamic Light Exposure in People with Dementia Living at Home" Applied Sciences 11, no. 21: 10221. https://doi.org/10.3390/app112110221
APA Stylevan Lieshout-van Dal, E., Snaphaan, L., Bouwmeester, S., de Kort, Y., & Bongers, I. (2021). Testing a Single-Case Experimental Design to Study Dynamic Light Exposure in People with Dementia Living at Home. Applied Sciences, 11(21), 10221. https://doi.org/10.3390/app112110221